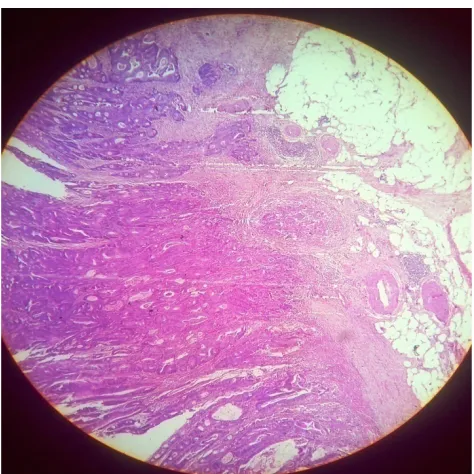
Synchronous Adenocarcinoma of Caecum and Sigmoid Colon: A Case Report
Full text
Figure

Related documents
The state child protection agency agreed to a DNR order if the hospital ethics committee approves it.. The patient’s mother and father are adamantly opposed to a DNR order or
Cholesteryl ester transfer protein inhibition, high-density lipoprotein raising, and progression of coronary atherosclerosis: insights from ILLUSTRATE (Investigation of Lipid
In Wave 1 data from the Intellectual Disability Supplement to the Irish Longitudinal Study on Ageing (IDS-TILDA) (2011), the reported prevalence of PPI use was 21.7%, and 44% of
Kaunselor di Unit Pembangunan Pelajar perlu melibatkan diri dalam pelaksanaan kaunseling kelompok secara menyeluruh agar kebolehan dan pengalaman mereka dapat digunakan secara
ICT, induction chemotherapy; CCRT, concurrent chemoradiotherapy; MRI, magnetic resonance imaging; IPTW, inverse probability of treatment weighting; ICTOS, Induction
hensive coupled climate model IPSL CM4, we simulate the Greenland ice sheet (GrIS) during the Eemian interglaciation with the three-dimensional ice sheet model SICOPOLIS.. The Eemian
It decreases the size of prolactin secreting pituitary tumors, and has been used with varying degrees of success in the treatment of menstrual disorders, premenstrual syndrome
Note: If you are connecting your display station to a 5294 Control Unit, you may be setting up the workstations (display stations and printers) before the workstation controller
