2016 Vol 83 No 9 S Afr Pharm J
41
Introduction
The development of antibiotics in the 1940’s was a significant breakthrough in public health.1 Antibiotics transformed health
care by dramatically reducing morbidity and mortality due to infectious diseases and have allowed for major advancements in medicine such as surgery and organ transplants to be made possible.1 On the contrary, the widespread use and overuse
of these agents, has resulted in the development of resistant organisms.1,2 As early as 1945, Sir Alexander Fleming, the discoverer
of penicillin, foresaw this phenomenon and famously cautioned that the rampant overuse of penicillin would cause an epidemic of drug resistant organisms3:
“The microbes are educated to resist penicillin and a host of penicillin-fast organisms is bred out … In such cases the thoughtless person playing with penicillin is morally responsible for the death of the man who finally succumbs to infection with the penicillin-resistant organism. I hope this evil can be averted.”
Globally, antimicrobial resistance is now considered a major threat to public health and without urgent coordinated action by many stakeholders, the world is headed for a post-antibiotic era, in which common easily treatable infections can once again kill.4,5
This situation is compounded by the rapid decline in discovery and development of new antibiotics.5 Although the lull in drug
discovery has been eased to some extent in recent years, new products are mostly targeting gram-positive organisms. However it is the emergence of resistant strains of gram-negatives which currently poses a greater threat to human life, with very few antibiotics that can combat them in the development pipe-line.5,6
The antimicrobial resistance (AMR) landscape
Mechanisms of antimicrobial resistance
Antimicrobials are agents that kill or inhibit the growth of microorganisms and encompass antibiotics, antifungals, and antivirals.2 Antimicrobial resistance (AMR) develops when
microorganisms adapt and grow in the presence of antimicrobials, rendering treatment with an antimicrobial drug ineffective.2,6
The factors leading to AMR are complex and multifactorial.7
Essentially, resistance occurs due to a natural evolutionary process which equips the microorganisms with mechanisms with which to counteract the effects of the antimicrobials.7 Antimicrobial
resistance can happen, for example, when a microorganism produces an enzyme that destroys the drug directly (e.g. β-lactamases which degrade β-lactam antimicrobials).7 It can
also occur through a genetic mutation of the pathogen, resulting in alteration of bacterial enzymes (e.g. mutated DNA-gyrases that resist quinolone binding) or changes in membrane permeability to antimicrobials (caused by efflux pumps) or protection of the target by DNA-binding proteins (known as Qnr).7 Development of
resistance in a single microorganism or location can unpredictably and rapidly spread through various mechanisms, for example, through the exchange of genetic material between resistant and susceptible microorganisms (horizontal gene transfer) or through transmission in human and animal populations via food, water and the environment.2,4
Prevalence of AMR
One of the cornerstones of the management of infectious diseases, and the basics of public health, is surveillance of drug-resistant infections and antimicrobial consumption.8 Availability
Appropriate use of antimicrobials:
An ongoing and coordinated effort
Hannelie (JC) Meyer, MSc(Med) Pharmacy, PhD (Pharmacy), Associate Professor; Mncengeli Sibanda, BPharm (Hons), MBA, MPharmDepartment of Pharmacy, Faculty of Health Sciences, Sefako Makgatho Health Sciences University
Correspondence to: Hannelie Meyer, e-mail: [email protected]
Keywords: rational antibiotic use, antimicrobial stewardship, antimicrobial (antibiotic) resistance
Abstract
The world is on the brink of a post antibiotic era and antibiotic resistance is no longer a prediction for the future; it is happening right now, across the world, and has the potential to put public health efforts into disarray. Despite the wealth of programmes and information, South Africa is not exempt from the threat of increasing antimicrobial resistance. An overview of the persisting issue of antimicrobial resistance, the current trends in antimicrobial stewardship and strategies for rational antibiotic use is provided. Specific emphasis is placed on the role of the pharmacist in containing antimicrobial resistance across the different practice settings, and working in collaboration with other healthcare professionals.
2016 Vol 83 No 9 S Afr Pharm J
42
of surveillance data is a critical requirement for action.6,8 However,
surveillance data worldwide is poor and improvement has been recommended.6,8 According to the latest data available, there has
been an increase in antibiotic consumption, driven by irrational prescribing and growing economies particularly in low and middle income countries, to such an extent that global consumption increased by 36% in the period between 2000 and 2010.6,9,10
Worldwide, AMR is increasing in prevalence resulting in infections that are difficult and expensive to treat. Currently, a number of common infections such as urinary tract infections, diarrhoea, gonorrhoea, tuberculosis, and other respiratory diseases are becoming more difficult to treat.4,6 Subsequently, terms like
‘super-bugs’, multi-drug resistant (MDR), extensively drug-resistant (XDR), methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant enterococci (VRE), pan-vancomycin-resistant bacteria, New Delhi Metallo-beta-lactamase-1 (NDM-1), Klebsiella pneumoniae
carbapenemase (KPC) and second-line therapy, feature increasingly and prominently in our medical diction.2,4,6
In 2014 an estimated 450 000 new cases of tuberculosis (TB) were reported in South Africa, with 1.8% of new cases and 6.7% of previously treated cases estimated to have MDR-TB.11 Recent
surveillance data from the Centre for Disease Dynamics, Economics and Policy’s (CDDEP) online interactive tool, ResistanceMap, paint an even more dire picture of the AMR landscape.12 In
2014 Escherichia coli resistance to fluoroquinolones was 28%, methicillin-resistant Staphylococcus aureus (MRSA) was 31% and
Klebsiella pneumoniae resistance against carbapenems showed an
increasing rate from 2% in 2013 to 4% in 2014.12,13
Irrational antibiotic use is not only limited to human use but also in agriculture.6,9,14 An estimated 80% of all antibiotics used globally
are used for the purpose of animal health, for growth promotion in feed animals, or for agriculture and aquaculture to prevent or treat infection.13,14 These practices are posing a significant public health
threat, contributing to drug-resistant pathogens.9,14 Estimated
antimicrobial consumption in livestock in 2010, is projected to rise by 67% by 2030, and nearly double in Brazil, Russia, India, China, and South Africa.9,12
South Africa evidently is using a large amount of antibiotics in food-producing animals, including a number of antibiotics that have been banned for use in other countries.15,16 Evidence
has shown that when required to treat or prevent infection, the practice of treating the entire herd instead of the infected animal, or administering antibiotics for extended periods of time using sub-therapeutic concentrations, is prevalent.6,15 This is further
compounded by the use of antibiotics for growth promoters without veterinary prescriptions and the lack of controls in the sale of antibiotics to farmers by veterinarians.6,15
Consequences of AMR
Antimicrobial resistance threatens to reverse the gains of antimicrobials in advancing modern medicine.16 While the real
magnitude of the problem is unknown, and the methods for measuring economic impact of resistance are not well elucidated, the monetary cost of treating antibiotic resistant infections
globally is estimated to be several billions of dollars per year.6,15
Worldwide, it is estimated that 10 million deaths per year, and 2% to 3.5% reduction in global gross domestic product by 2050, will be a direct result of the current trends in AMR.8
In a clinical setting, infections caused by resistant microorganisms may require more toxic therapy that can lead to adverse outcomes. In addition, in-hospital mortality rates and extended hospital stays will increase as a result of AMR.4 This is coupled with an up to
two-fold increase in hospital-acquired infections and costs for patients with resistant versus susceptible infection, due to infections which are more difficult and more expensive to treat.4,6
The societal and economic impacts of AMR are myriad.4 For the
patient, some drug resistant micro-organisms require physical isolation from society in order to minimise transmission which may result in loss of work and family time.4,17 Furthermore, the patient
may incur costs for extra visits to the doctor and lengthened hospitalisation, possible second-line treatments, laboratory tests and other diagnostic costs.4
Lastly,AMR has the potential to cause calamitous effects on international travel and trade resulting from the cross-border transmission of resistant infections.2
Strategies to combat antimicrobial resistance
Global action plan on antimicrobial resistance
Several regional and global resolutions have called for action on specific health aspects related to AMR.2,4,18 In 2008, the Global
Antibiotic Resistance Partnership (GARP) was established to help developing countries build capacity and establish policies to deal with the growing problem of AMR.19 Following a World Health
Assembly resolution in 2015, a global action plan on AMR was developed for adoption by member states, to produce national strategic plans to combat AMR.18 The overall goal of the action
plan is to ensure, for as long as possible, continuity of the ability to treat and prevent infectious diseases with effective and safe medicines that are quality-assured, used in a responsible way, and accessible to all who need them.18 To achieve this overall goal, the
following five main strategic objectives were set out18:
• Improve awareness and understanding of antimicrobial resistance through effective communication, education and training
• Strengthen the knowledge and evidence base through surveillance and research
• Reduce the incidence of infection through effective sanitation, hygiene and infection prevention measures
• Optimise the use of antimicrobial medicines in human and animal health
2016 Vol 83 No 9 S Afr Pharm J
43
The global action plan provides the framework for national action plans to combat AMR.18 For each of the objectives, key actions are
stipulated to combat AMR, which should be taken by the various actors involved, using an incremental approach over the next 5–10 years.18 Antibiotic resistance is covered in great detail,
however, reference is made to existing action plans for viral, parasitic and bacterial diseases, including HIV/AIDS, malaria and tuberculosis.18 Special emphasis is placed on strengthening of
already existing principles of antimicrobial stewardship.18
South African Antimicrobial Resistance National Strategy Framework, 2014–2024
In South Africa, GARP conducted a situation analysis of antibiotic use and resistance.19 This situational analysis highlighted the
emergence of ‘super-bugs’ and the need for action to contain AMR.20 Subsequently, the South African Antibiotic Stewardship
Programme (SAASP) was established under the auspices of the Federation of Infectious Diseases Societies of Southern Africa (FIDSSA), comprising of members from the private and public sector, to strengthen antibiotic stewardship and education in South Africa.20,21
In 2014, the National Department of Health in South Africa, published the Antimicrobial Resistance (AMR) National Strategy Framework, 2014–2024, in response to the preceding WHO global strategy for containment of AMR and advocacy by SAASP.13,21
This strategy defines South Africa’s approach to manage AMR, limit further increases in resistant microbial infections, and improve patient outcomes.13 The vision is “to ensure the
appropriate use of antimicrobials by healthcare professionals in all health establishments in South Africa to conserve the efficacy of antimicrobials for the optimal management of infections in
human and animal health.”13 South Africa’s national AMR strategy
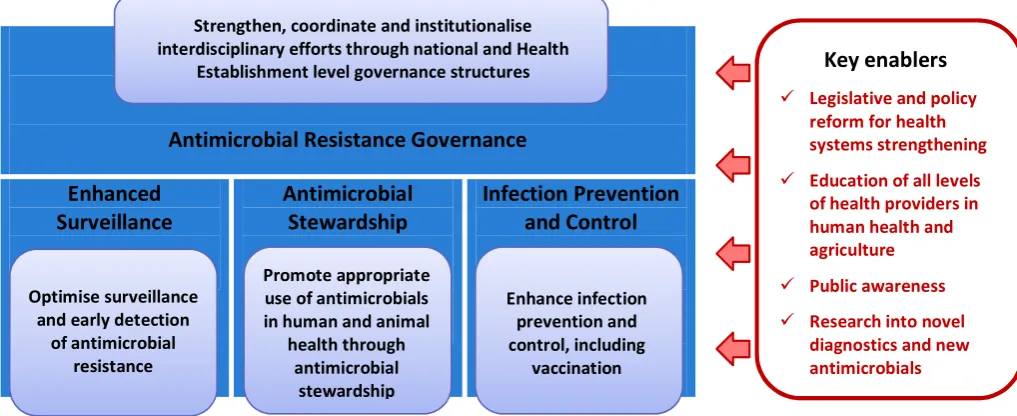
framework consists of four building blocks with strategic objectives that are reinforced by four key enablers (Figure 1).13,20
The strategic framework emphasises a governance model which is supported by relevant laws in order to ensure success of each objective and enabler, and to allow for oversight, monitoring and evaluation.13,20 The antimicrobial governance model is enabled
through a multidisciplinary inter-sectorial ministerial advisory committee comprising of key stakeholders on AMR.13,20 Prior to
the promulgation of the strategic framework for the AMR national strategy and the corresponding implementation plan, there was no single national guideline to address antimicrobial resistance, although the objectives and enablers were promoted in one form or another in various documents.13,14,17 For example, the Essential
Medicines List (EML) and Standard Treatment Guidelines (STGs) recommend principles for the use of antimicrobials at different levels of the South African healthcare system.14 The National Core
Standards for health establishments in South Africa endorse AMS and infection control and prevention interventions at the different facility levels.20
Antimicrobial stewardship in South Africa
Antimicrobial stewardship (AMS) is defined as a multidisciplinary, systematic approach to optimising the appropriate use of all antimicrobials to improve patient outcomes and limit the emergence of resistant pathogens whilst ensuring patient safety.18,24 Antimicrobial stewardship programmes in South
Africa as well as other countries have shown to be successful in promoting rational antibiotic use, improve patient outcomes and reduce adverse consequences of antibiotic use, including antibiotic resistance, toxicity and unnecessary costs.22-24
Despite not having an outright mandate from the National Department of Health, the South African Antibiotic Stewardship Programme (SAASP) provides leadership, advocacy, and strengthening of antibiotic stewardship, in the public and private sectors in South Africa.22 They have published treatment guidelines
on antibiotic prescribing, offer courses and educational materials on antimicrobial stewardship and an antibiotic prescription chart is available for use on its website.22
Antimicrobial Resistance Governance
Enhanced
Surveillance
Antimicrobial
Stewardship
Infection Prevention
and Control
Figure 1.
Strategic framework for the antimicrobial resistance national strategy
13,20The strategic framework emphasises a governance model which is supported by relevant laws in
order to ensure success of each objective and enabler, and to allow for oversight, monitoring and
evaluation.
13,20The antimicrobial governance model is enabled through a multidisciplinary
inter-sectorial ministerial advisory committee comprising of key stakeholders on AMR.
13,20Prior to the
promulgation of the strategic framework for the AMR national strategy and the corresponding
implementation plan, there was no single national guideline to address antimicrobial resistance,
although the objectives and enablers were promoted in one form or another in various
documents.
7,13,14For example, the Essential Medicines List (EML) and Standard Treatment Guidelines
(STGs) recommend principles for the use of antimicrobials at different levels of the South African
healthcare system.
14The National Core Standards for health establishments in South Africa endorse
AMS and infection control and prevention interventions at the different facility levels.
20Antimicrobial stewardship in South Africa
Antimicrobial stewardship (AMS) is defined as a multidisciplinary, systematic approach to optimising
the appropriate use of all antimicrobials to improve patient outcomes and limit the emergence of
resistant pathogens whilst ensuring patient safety.
18,24Antimicrobial stewardship programmes in
South Africa as well as other countries have shown to be successful in promoting rational antibiotic
use, improve patient outcomes and reduce adverse consequences of antibiotic use, including
antibiotic resistance, toxicity and unnecessary costs.
22-24Despite not having an outright mandate from the National Department of Health, the South African
Antibiotic Stewardship Programme (SAASP) provides leadership, advocacy, and strengthening of
antibiotic stewardship, in the public and private sectors in South Africa.
22They have published
treatment guidelines on antibiotic prescribing, offer courses and educational materials on
antimicrobial stewardship and an antibiotic prescription chart is available for use on its website.
22The National Department of Health recently prepared a draft Practical Guide to Antimicrobial
Stewardship in South Africa.
23This guide is intended to act as a blueprint for all healthcare
professionals in the public and private sector, to enact AMS in line with the Strategic Framework and
Strengthen, coordinate and institutionaliseinterdisciplinary efforts through national and Health Establishment level governance structures
Promote appropriate use of antimicrobials in human and animal
health through antimicrobial
stewardship
Enhance infection prevention and control, including
vaccination Optimise surveillance
and early detection of antimicrobial
resistance
Key enablers
Legislative and policyreform for health systems strengthening Education of all levels
of health providers in human health and agriculture Public awareness Research into novel
diagnostics and new antimicrobials
2016 Vol 83 No 9 S Afr Pharm J
44
The National Department of Health recently prepared a draft Practical Guide to Antimicrobial Stewardship in South Africa.23
This guide is intended to act as a blueprint for all healthcare professionals in the public and private sector, to enforce AMS in line with the Strategic Framework and Implementation Plan, at all levels of care.23 The document further aims to be a practical,
step-by-step or ‘how to’ guide, addressing the four pillars of the Strategic Framework.23 With the practical approach taken in the
guide, much broader AMR programme activities and interventions are specified, compared to what is stipulated for AMS in the National Core Standards.23 A useful monitoring and evaluation
framework for AMS implementation is offered for each level of the health system.23
Central to the theme of AMS is the need to develop a collaborative practice between clinicians, pharmacy staff, microbiologists, laboratorians and infection control specialists in order to provide the best outcome for the patient, reduce healthcare costs and curb the emergence of infections and drug resistant organisms.22,25,26
Pharmacists’ role in combatting antimicrobial
resistance
One of the main drivers of AMR is the widespread and inappropriate use of antimicrobials.6 Pharmacists are the custodians of medicines
and are mandated to meet the healthcare needs of the population through the supply of safe, effective and quality medicines and providing of pharmaceutical care by taking responsibility for the outcomes of therapy.25 They have an important role to play
in the community in that they often serve either as the first port-of-call for the patient in the healthcare-seeking chain, as well as a last contact when medicines are dispensed.25,27 In this gateway
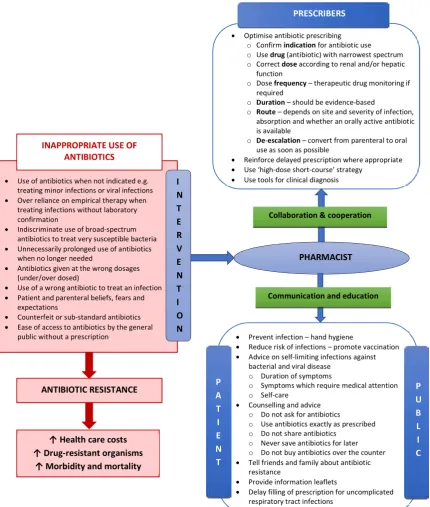
function, pharmacists have opportunities to providing information to the general public as well as clinicians in judicious antibiotic use and thus preventing unnecessary antibiotic use, which is strongly associated with increased resistance.27,28 Figure 2 illustrates the
role the pharmacist can play in response to the inappropriate use of antibiotics specifically.24,27,28-32
In 2008, the International Pharmaceutical Federation (FIP) published a pioneering statement of policy control of antimicrobial medicines resistance.28 Similarly, the South African Pharmacy
Council’s Good Pharmacy Practice (GPP) aims to strive for quality pharmaceutical services for all the people of South Africa.29
Although not explicitly to be used in relation to antimicrobials, the rules in the GPP serve as minimum standards with which the pharmacist can fulfil their role in antimicrobial stewardship.29,30
Lately, there have also been updated recommendations released by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA) to complement current antimicrobial stewardship strategies.31,32
The minimum roles of the pharmacist in encouraging judicious use of antimicrobials and minimising antimicrobial resistance in the different practice settings are cross-cutting across most sectors of pharmacy. Table I shows examples of the specific roles pharmacists can play in AMR in line with the building blocks of the national strategy framework for AMR in South Africa.13,18,20,22,23,27-35
The goal of these efforts is always to improve health outcomes for the patient, i.e. reduced morbidity and mortality, minimise hospital-acquired infections, limit the emergence of drug-resistant organisms and lower healthcare costs.13,20
Hospital pharmacist
In the clinical environment, pharmacists may play an oversight role amongst healthcare professionals by formulating and monitoring adherence to standard treatment guidelines, including rational antibiotic prescribing by clinicians.25,26 The pharmacist and the
nurse can actively collaborate in AMS programmes in the ward, acute and outpatient setting, to optimise antimicrobial use and combat AMR.26 Ideally, doctors should be part of such an
integrated team. 26
As a core member of a multi-disciplinary antibiotic stewardship committee, the pharmacist can also provide appropriate guidelines regarding empiric and prophylactic use of antibiotics through the use of evidence-based medicine principles.27,28,29 These include
antibiotic cycling, de-escalation therapy, dose optimisation and/ or parenteral to oral conversion when applicable.24,28,32-34 The
hospital pharmacist through collaboration with the laboratory services, can ensure the availability of rapid diagnostic testing such as accurate point of care tests to guide clinicians on the most appropriate use of antibiotics.30
The hospital setting is ideal for prospective audit and feedback after two or three days of treatment in order to ensure the right drug is prescribed at the right time for the right diagnosis.33 This is
more so for targeted antibiotics such as those that treat emerging drug-resistant bacterial infections.24,33,34
These activities require professional diligence through continuing education programmes of prescribers and dispensers as well as prospective monitoring and evaluation to avoid irrational prescribing.21
Community pharmacist
The community pharmacist has a vantage point in being able to directly initiate therapy.29 The pharmacist in this instance
may recommend alternative treatment for minor infections and reassure patients of the inappropriateness of antibiotics for viral infections.25 The community pharmacist must exercise due
diligence in upholding the law and not permit the over-the-counter sale of antibiotics.25 In instances when an antibiotic is
indicated, the pharmacist can then advise the patient to complete the course and warn of possible side-effects or interactions in order to aid adherence.25 Technologies such as electronic measurement
devices can be used to improve adherence to antibiotic therapy.30
The community pharmacist can teach community members to dispose of any unused medicines appropriately.25 The community
pharmacist has a further role to play in promoting preventative measures of limiting infection such as good hygiene and vaccination campaigns.29
Academic pharmacist
2016 Vol 83 No 9 S Afr Pharm J
45
providers on the rational use of medicines and AMS.26,35 Although
AMS training is included in the undergraduate pharmacy curriculum, a recent study amongst final year pharmacy students reported significant differences between the eight universities in the country, with 90% of students indicating that they would like more training on AMS.35 Central to their role in AMS, academic
pharmacists can also develop curricula for continuing professional development in this field so as to improve current and future performance of all health practitioners as well as veterinarians.23
Academic pharmacists are in the ideal position to contribute towards collection and interpretation of surveillance data and conduct research, in collaboration with other members of the healthcare team.23,33,34
Industrial and wholesale pharmacist
In their role in AMS, manufacturing pharmacists have an obligation to ensure the manufacture of safe, efficacious and good quality medicines.27,29 In addition, they should proactively seek to
promote innovation and research on new antimicrobials as well as ensure the steady production of essential antimicrobials to meet supply.29 Pharmacists practising in a wholesale environment can
ensure that only authorised channels of distribution are used to supply the medicines to hospital and community pharmacies in order to minimise the availability of counterfeit and substandard medicines, and the rerouting of essential antimicrobials to non-approved clients.28
7
Figure 2. Inappropriate antibiotic use and the role of the pharmacist24,27-32
In 2008, the International Pharmaceuticals Federation (FIP) published a pioneering statement of policy control of antimicrobial medicines resistance.28 Similarly, the South African Pharmacy Council’s Good Pharmacy Practice (GPP) aims to strive for quality pharmaceutical services for all the
Optimise antibiotic prescribing
o Confirm indication for antibiotic use o Use drug (antibiotic) with narrowest spectrum o Correct dose according to renal and/or hepatic
function
o Dose frequency – therapeutic drug monitoring if required
o Duration – should be evidence-based
o Route – depends on site and severity of infection, absorption and whether an orally active antibiotic is available
o De-escalation – convert from parenteral to oral use as soon as possible
Reinforce delayed prescription where appropriate Use ‘high-dose short-course’ strategy
Use tools for clinical diagnosis PRESCRIBERS
Collaboration & cooperation
Communication and education PHARMACIST
Prevent infection – hand hygiene
Reduce risk of infections – promote vaccination Advice on self-limiting infections against
bacterial and viral disease o Duration of symptoms
o Symptoms which require medical attention o Self-care
Counselling and advice o Do not ask for antibiotics
o Use antibiotics exactly as prescribed o Do not share antibiotics
o Never save antibiotics for later o Do not buy antibiotics over the counter
Tell friends and family about antibiotic
resistance
Provide information leaflets
Delay filling of prescription for uncomplicated
respiratory tract infections
P A T I E N T
P U B L I C ANTIBIOTIC RESISTANCE
↑ Health care costs ↑ Drug-resistant organisms
↑ Morbidity and mortality
Use of antibiotics when not indicated e.g.
treating minor infections or viral infections
Over reliance on empirical therapy when
treating infections without laboratory confirmation
Indiscriminate use of broad-spectrum antibiotics to treat very susceptible bacteria
Unnecessarily prolonged use of antibiotics
when no longer needed
Antibiotics given at the wrong dosages
(under/over dosed)
Use of a wrong antibiotic to treat an infection Patient and parenteral beliefs, fears and
expectations
Counterfeit or sub-standard antibiotics Ease of access to antibiotics by the general
public without a prescription
INAPPROPRIATE USE OF ANTIBIOTICS
I N T E R V E N T I O N
2016 Vol 83 No 9 S Afr Pharm J
46
Table I. The role of the pharmacist in containing antimicrobial resistance18,22,23,25,27-35
H
ospital pharmacist
Enhanced surveillance Antimicrobial stewardship Infection prevention and control
• Monitor patient outcomes and provide information about incidence and prevalence of AMR
• Identify patients at risk of AMR • Post-prescribing audits to monitor
antimicrobial consumption
• Clinical pharmacists to conduct therapeutic drug monitoring (TDM) in collaboration with laboratory services in order to minimise adverse drug reactions
• Strengthen pharmacovigilance systems and adverse drug reaction reporting
• Minimise pharmacy stock-outs to ensure that patient treatment is not interrupted • Prospective monitoring and evaluation of
prescribing habits and compliance to EML, STGs and antibiotic prescribing guidelines
• Establish and enforce the prescribing on antibiotic prescription charts
• Ward rounds to ensure dose optimisation based on patient characteristics and antibiotic susceptibility testing
• Monitoring of antibiotics use: surgical prophylaxis duration; de-escalation and reassessment of treatment need, hang time • Ensure access to EML, STGs and national
antibiotic prescribing guidelines • Develop hospital formulary with limited
number of antibiotics in order to restrict the number and type of antimicrobials used • Pre-authorisation for certain antibiotics, to
ensure necessary oversight for appropriate use • Timeous feedback and interventions to modify
irrational prescribing
• Promote use of algorithms to guide prescribers based on clinical signs and symptoms
• Key member of the hospital infection prevention and control committee • Ensure availability of cleaning agents and
personal protective equipment for hospital staff
• Encourage the use of single-dose packages of sterile drug products rather than multiple-dose containers
• Enhance and encourage hand hygiene in the hospital setting in order to minimise transmission of hospital-acquired infections • Offer continuous training on hand hygiene • Educate and promote vaccination against viral
and bacterial diseases
Communit
y pharmacist
• Prescription review and feedback recommendations in order to track AMR • Prescription review and collection of data on
antimicrobial sales, prescriptions and use to monitor antimicrobial consumption • Prescription review and feedback in order to
give oversight on rational antimicrobial use • Measure success of programmes
• Primary care drug therapy permit holders to prescribe and dispense antibiotics according to EML and STGs using the antimicrobial prescription chart
• Monitor antibiotic prescribing for self-limiting conditions
• Ensure antibiotic prescribed is justified and correct (see Figure 2)
• Delayed antibiotic prescriptions where appropriate
• Education and information leaflets for patients on AMR
• Implement vaccination uptake programmes to reduce the incidence of bacterial and viral infections
• Promote hand hygiene in the community • Increase community awareness on infectious
diseases, their causes and how to prevent them including general infection and prevention measures
Ac
ademic pharmacist
• Conduct proactive research in collaboration with microbiologists which will serve as an early warning system for the emergence and spread of new forms of resistance
• Conducting qualitative research mapping the consumption of antimicrobial medicine through the regular collection of data on sales, prescriptions and use in single or multiple centres
• Development and incorporation of AMS into undergraduate and postgraduate curriculum • Ensure all undergraduate and postgraduate
students participate in AMS ward rounds • Support continuous professional development
in AMS e.g. antimicrobial prescribing course on the antimicrobial prescription chart
• Computerised clinical decision support to guide clinicians on the best choice of antimicrobial agent
• Clinical trials that incorporate AMS in their design
• Assist with pharmacokinetics and
pharmacodynamics to ensure most effective antimicrobial agent is used
• Implementation research
• Develop public education programmes on AMR
• Contribute towards and participate in training programmes in collaboration with other heathcare professionals on infection prevention and control
• Support continuous professional development in infection prevention and control and vaccination e.g. by developing online training materials on infection prevention and control and vaccination
• Participate in campaigns to enhance vaccine uptake for bacterial and viral diseases
Industrial pharmacist
• Collection of data on antimicrobial sales to track antimicrobial consumption
• Manufacture safe, efficacious and good quality medicines
• Promote innovation and research on new antimicrobials
• Ensure steady production of essential antimicrobials to meet supply
• Production and marketing agreements for a
needs-based number of treatments per year • Conduct nationwide health awareness campaigns that promote the appropriate use of antimicrobials and the growing threat of AMR
Regula
tor
y / health sy
st
ems
• Setup and implement national surveillance framework and development of indicators for AMR
• Collate national antibiotic consumption data at all healthcare levels (private and public) • Overseeing role on medicines and diagnostics
to ensure good quality medicines and diagnostic assays
• Minimise substandard and counterfeit antimicrobials in order to ensure good quality medicines
• Formulate and implement antimicrobial prescription charts for use at all health levels in the public and private sector
• Participate in expert committees formulating national EML and STGs
• Regulating contacts with pharmaceutical representatives to limit undue influence on prescribers
• Develop tools to assist with clinical diagnoses in out-patient setting
• Multi-disciplinary collaboration to develop and implement educational and behavioural interventions for appropriate prescribing
• Active and passive surveillance for hospital-acquired infections, outbreaks and control • Programmes to ensure environmental safety i.e.
2016 Vol 83 No 9 S Afr Pharm J
47
Regulatory and health system pharmacist
Pharmacists can participate in the development of national policy, laws and guidelines which will promote appropriate use of antimicrobials and the implementation of such policies where they exist.22,23 In particular, they can collaborate with
health-professional societies and associations to develop and facilitate the implementation of educational and behavioural interventions that will assist in rational antimicrobial use.23
Furthermore, they can ensure legislation, which prevents dispensing without prescription, is enforced and that the antibiotics registered for use are safe, efficacious and of a good quality.25 Moreover, such pharmacists can enable an environment
that ensures that there is minimum influence on prescribing and dispensing by the pharmaceutical industry.22,27
Conclusion
Antimicrobial resistance is a major threat to public health. A post-antibiotic era is fast approaching, calling for an urgent and coordinated action by all stakeholders. South Africa’s AMR strategy framework with its four building blocks (AMR governance, enhanced surveillance, AMS, infection prevention and control) and strategic enablers, aims to ensure the appropriate use of antimicrobials by all healthcare professionals and in all health establishments. The framework provides an opportunity for pharmacists across all practice settings to get involved, collaborate and play a role in this important endeavour. Antimicrobial stewardship specifically has the potential of combating the threat of dwindling antibiotic resources while advancing pharmaceutical care. Pharmacists from all sectors of practice should proactively uphold the principles of rational antimicrobial use and participate in AMS programmes, within the multi-disciplinary healthcare team, and at all levels of care. It is in the interest of public health that change, collaboration and cooperation start with all of us.
References
1. Aminov R. A brief history of the antibiotic era: lessons learned and challenges for the fu-ture. Frontiers in Microbiology. 2010;1(134):1-7. doi: 10.3389/fmicb.2010.00134. 2. World Health Organization (WHO). The evolving threat of antimicrobial resistance. Options
for action. 2012. Available from: http://www.who.int/patientsafety/implementation/amr/ publication/en/.
3. New York Times. Penicillin finder assays its future. 26 June 1945:21.
4. World Health Organization (WHO). Antimicrobial resistance global report on surveillance. 2014. Available from: http://www.who.int/whr/2006/en/.
5. O’Neill J. Securing new drugs for future generations: The pipeline of antibiotics. The Review on Antimicrobial Resistance. 2015. http://amr-review.org/Publications.
6. Laxminarayan R, Matsoso P, Pant S, et al. Access to effective antimicrobials: a worldwide challenge. Lancet. 2016;387:168–75.
7. Holmes AH, Moore LSP, Sundsfjord A, et al. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet. 2016;387:176–87.
8. O’Neill J. Tackling drug-resistant infections globally: Final report and recommendations. The review on antimicrobial resistance. May 2016. Available from: https://amr-review.org/. 9. Van Boeckel TP, Gandra S, Ashok A, et al. Global Antibiotic Consumption 2000 to 2010: An Analysis of National Pharmaceutical Sales Data. Lancet Infect Dis. 2014;3099(14):1–9. http://doi.org/10.1016/S1473-3099(14)70780-7.
10. Gelband H, Miller-Petrie M, Pant S, et al. The State of the World’s Antibiotics 2015. Wound Healing Southern Africa. 2015;8(2):30–34.
11. National Department of Health (NDoH). Antimicrobial Resistance. Background document. 2015. Available from: http://www.fidssa.co.za/Content/Documents/AMR_Background_ document_FINAL_March15.pdf.
12. Centre for Disease Dynamics, Economics & Policy (CDDEP). Resistance Map. Available from: http://resistancemap.cddep.org/index.php.
13. National Department of Health (NDoH). Antimicrobial Resistance National Strategy Framework, 2014–2024. 2014. Available from: http://www.mm3admin.co.za/documents/ docmanager/3C53E82B-24F2-49E1-B997-5A35803BE10A/00090160.pdf.
14. National Department of Health (NDoH). Antimicrobial Resistance. Background document. 2015. Available from: http://www.fidssa.co.za/Content/Documents/AMR_Background_ document_FINAL_March15.pdf.
15. Moyane JN, Jideani AIO, Aiyegoro OA. Antibiotics usage in food-producing animals in South Africa and impact on human: Antibiotic resistance. Afr J Microbiol. 2013;7(24):2990– 2997. DOI: 10.5897/AJMR2013.5631.
16. Eagar HA, Swan G, Van Vuuren M. Survey of antimicrobial usage in animals in South Africa with specific reference to food animals. J S Afr Vet Assoc. 2012;83(1):16. Doi: 10.4102/jsava. v83i1.16.
17. National Department of Health (NDoH). National Strategic Plan on HIV, STIs and TB, 2012-2016. 2011. Available from: http://www.gov.za/documents/national-strategic-plan-hiv-stis-and-tb-2012-2016.
18. World Health Organization (WHO). Global Action Plan on Antimicrobial Resistance. 2015. Available from: http://www.wpro.who.int/entity/drug_resistance/resources/global_ac-tion_plan_eng.pdf.
19. Winters C, Gelband H. The Global Antibiotic Resistance Partnership (GARP). 2011. S Afr Med J. 2011;101(8):556-57. Available from: http://www.cddep.org/publications/situation_anal-ysis_antibiotic_use_and_resistance_south_africa#sthash.6RI0oNo4.dpuf.
20. Mendelson M, Matsotso M. The South African Antimicrobial Resistance Strategy Frame-work. AMR Control. 2015;54–61.
21. Mendelson M. Role of antibiotic stewardship in extending the age of modern medicine. 2015. S Afr Med J. 2015;105(5):414–48.
22. South African Antibiotic Stewardship Programme (SAASP). Available from: http://www. fidssa.co.za/SAASP.
23. National Department of Health (NDoH). A Practical Guide to Antimicrobial Stewardship in South Africa. Draft version 1. 1. July 2016. Pretoria: Department of Health. Available from: http://www.health.gov.za/index.php/antimicrobial-resistance
24. Brink AJ, Messina AP, Feldman C, et al. Antimicrobial stewardship across 47 South African hospitals: an implementation study. Lancet Infect Dis. 2016;16(9):1017–1025.
25. World Health Organization (WHO) Regional Office for Europe. The role of pharmacist in encouraging prudent use of antibiotics and averting antimicrobial resistance: a review of policy and experience in Europe. 2014. Available from: http://apps.who.int/medicinedocs/ documents/s22244en/s22244en.pdf.
26. Schellack N, Pretorius R, Messina AP. ‘Esprit de corps’: Towards collaborative integration of pharmacists and nurses into antimicrobial stewardship programmes in South Africa. S Afr Med J. 2016;106(10):973–974. DOI:10.7196/SAMJ.2016.v106i10.11468.
27. International Pharmaceutical Federation (FIP). FIP Statement of Policy Control of Antimi-crobial Medicines Resistance (AMR). 2008. Available from: http://www.fip.org/www/up-loads/database_file.php?id=289&table_id.
28. Kotwani A, Wattal C, Joshi P, et al. Irrational use of antibiotics and role of the pharmacists: an insight from a qualitative study in New Delhi, India. J Clin Pharm Ther. 2012;37:308–12. 29. South African Pharmacy Council (SAPC). Good Pharmacy Practice in South Africa (GPP).
Fourth Edition. 2010. Arcadia. Pretoria: SAPC.
30. Brink AJ. Antimicrobial stewardship (AMS) in the outpatient setting. Pathchat. 2015. Edi-tion no. 26. Available from: https://www.ampath.co.za/wp-content/newupload/2015/05/ pathchat26-FINAL.pdf.
31. Barlam TF, Cosgrove SE, Abbo LM, et al. Implementing an Antibiotic Stewardship Program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin Infect Dis. 2016;15;62(10):e51–77.
32. Centre for Disease Control and Prevention (CDC). Core Elements of Hospital Antibiotic Stewardship Programs: Get Smart for Healthcare. 2016. Available from: http://www.cdc. gov/getsmart/healthcare/implementation/core-elements.html.
33. Boyles TH, Whitelaw A, Bamford C, et al. Antibiotic stewardship ward rounds and a dedi-cated prescription chart reduce antibiotic consumption and pharmacy costs without af-fecting inpatient mortality or re-admission rates. PLoS One. 2013;8(12):e79747. 34. Messina AP, van den Bergh D, Goff DA. Antimicrobial stewardship with pharmacist
inter-vention improves timeliness of antimicrobials across thirty-three hospitals in South Africa. Infect Dis Ther. 2015;4(1)5–14.