Małgorzata Malinowska-Zaprzałka
1, Marzena Wojewódzka-Żelezniakowicz
2,
Jerzy R. Ładny
2, Ewa Chabielska
3The Influence of Chronic and Short-Term Treatment
with Angiotensin-Converting Enzyme Inhibitor
on Hemodynamics During Induction
of General Anesthesia in Patients Undergoing
Maxillofacial Surgery*
Wpływ inhibitora – konwertazy angiotensyny stosowanego
w przewlekłej i krótkotrwałej terapii na wybrane wskaźniki
hemodynamiczne podczas wprowadzenia do znieczulenia ogólnego
pacjentów poddanych zabiegom naprawczym po urazach twarzoczaszki
1 Department of Anaesthesiology and Intensive Care, Medical University of Bialystok, Poland 2 Department of Emergency and Disaster Medicine, Medical University of Bialystok, Poland 3 Biopharmacy Department, Medical University of Bialystok, Poland
Abstract
Background. There is still no agreement whether antihypertensive treatment with ACE-I should be continued until the day of surgery because of risk of perioperative hypotension. Moreover, non-treated hypertension is also a major risk of complications during anesthesia, especially ischaemic episodes.
Objectives. The aim of the study was to compare short-term versus chronic treatment effects of ACE-I enalapril on some hemodynamic (blood pressure and heart rate) parameters during the induction of general anesthesia.
Material and Methods. The authors compared systolic and diastolic blood pressure as well as heart rate during induction in three groups of patients (n = 152) scheduled for maxillofacial trauma surgery. Group A (n = 48) was chronically treated with ACE-I enalapril, group B (n = 54) received short term treatment. Group C (50) consisted of normotensive patients.
Results. The authors have determined that short-term (3–4 doses) treatment of patients with moderate hyper-tension not previously treated with enalapril allows the successful reduction of high systolic and diastolic blood pressures (SBP) – from 174 ± 18 to 148 ± 13 mm Hg and DBP from 112 ± 11 to 83 ± 14 mm Hg – until the day of surgery and induces lower values of systolic blood pressure (SBP) during the induction period of general anesthesia than does chronic treatment. The authors also confirmed the mild hypotensive effect of induction of anesthesia in patients chronically (for at least 6 months) treated with enalapril.
Conclusions. These findings suggest that interruption of treatment before anesthesia is not necessary in hyper-tensive chronic ACE-I treated patients. Short-term treatment with ACE-I in hyperhyper-tensive patients allows the suc-cessful reduction of high blood pressure and improves the level of safety during induction of anesthesia for maxil-lofacial trauma surgery (Adv Clin Exp Med 2010, 19, 3, 329–336).
Key words: general anesthesia, ACE-I, hemodynamic response.
Streszczenie
Wprowadzenie. Wiele kontrowersji budzi kontynuowanie leczenia nadciśnienia tętniczego inhibitorami konwer-tazy angiotensyny (ACE-I) do dnia zabiegu chirurgicznego z uwagi na niebezpieczeństwo okołooperacyjnego
spad-Adv Clin Exp Med 2010, 19, 3, 329–336 ISSN 1230-025X
oRIGINAl PAPERS
© Copyright by Wroclaw Medical University
ku ciśnienia tętniczego. Nieleczone nadciśnienie tętnicze stanowi natomiast poważne ryzyko powikłań podczas znieczulenia ogólnego, co może prowadzić do epizodów niedokrwienia mięśnia sercowego.
Cel pracy. Porównanie wpływu enalaprylu stosowanego w przewlekłej i krótkotrwałej terapii na niektóre wskaźniki hemodynamiczne (ciśnienie tętnicze i czynność serca) podczas wprowadzenia do znieczulenia ogólnego.
Materiał i metody. Badaniami objęto 152 pacjentów poddanych zabiegom naprawczym po urazach twarzoczaszki. oceniano wartości skurczowego i rozkurczowego ciśnienia tętniczego oraz częstość akcji serca w trzech grupach chorych podczas wprowadzenia do znieczulenia. Grupę A (n = 48) stanowili pacjenci z przewlekle leczonym nadci-śnieniem, grupę B (n = 54) chorzy leczeni krótkotrwale (3–4 dawki), a grupę kontrolną (n = 50) stanowili pacjenci z prawidłowym ciśnieniem tętniczym.
Wyniki. Wykazano, że krótkotrwałe leczenie enalaprylem umiarkowanego nadciśnienia tętniczego pozwala sku-tecznie obniżyć zarówno skurczowe (174 ± 18 vs 148 ± 13 mm Hg), jak i rozkurczowe (112 ± 11 vs 83 ± 14 mm Hg) ciśnienie tętnicze oraz wywołuje niższe wartości ciśnienia podczas wprowadzenia do znieczulenia niż w grupie chorych leczonych przewlekle. Potwierdzono także umiarkowane działanie hipotensyjne ACE-I podczas wprowa-dzenia do znieczulenia ogólnego w grupie pacjentów leczonych przewlekle.
Wnioski. Wyniki sugerują, że przerwanie leczenia ACE-I pacjentów z nadciśnieniem nie jest konieczne przed zabiegiem chirurgicznym naprawczym po urazach twarzoczaszki. Już krótkotrwałe przygotowanie tymi lekami pacjentów z umiarkowanym nadciśnieniem pozwala obniżyć jego wartości w dniu zabiegu chirurgicznego i pod-czas znieczulenia do zabiegów naprawczych po urazach twarzopod-czaszki, poprawiając bezpieczeństwo pacjenta (Adv Clin Exp Med 2010, 19, 3, 329–336).
Słowa kluczowe: znieczulenie ogólne, ACE-I, odpowiedźhemodynamiczna.
Hypertension in patients undergoing anesthesia and surgery is considered to be a major risk deter-minant of complications during anesthesia and the post-anesthetic period. Among the complications, myocardial ischemia and stroke are mentioned more than others. Although the magnitude of the risk remains controversial [1], it is always a warning for the anesthesiologist. It has often been concluded that hypertensive patients should rather undergo surgery with well-controlled blood pressure [2]. Therefore, to avoid undesired events during anesthesia in such patients, efforts have been made to provide such con-trol in as smooth a manner as possible.
General anesthesia interferes with many car-diovascular regulating systems [3]. First, most inhaled and intravenous anesthetics are known to dull sympathetic reflexes which, in patients with limited cardiovascular reserve, may lead to myo-cardial depression [4]. Secondly there are data that general anesthesia may increase the release of arginin-vasopressin (AVP) and the formation of angiotensin II [3]. Inhalation anesthesia and surgi-cal stress themselves have widely been shown to the activate renin-angiotensin system (RAS) [5–7].
Many authors have focused on the preanesthetic status of patients. Routinely, antihypertensive treat-ment is continued until the day of surgery. It is sug-gested, that this treatment, influencing the anesthe-sia, minimizes the hypertensive response to intuba-tion [7]. Nowadays, the opinion is rising suggesting the discontinuation of such treatment as a method for avoiding hypotensive episodes in hypertensive patients [8–10]. This is of great importance especial-ly when angiotensin – converting enzyme inhibitors (ACE-I) are concerned. As this group of drugs is the most widely used in the treatment of hypertension [11], the authors can also expect an increasing
num-ber of ACE-I-treated patients in the operation room [12]. However, some authors warn of profound hypotension in patients treated with enalapril or captopril occurring during induction of anesthesia [4, 6, 13], and there are no data comparing the effect of new ACE-I during induction.
There is very little data concerning the influ-ence of ACE-I given as a short-term mode during the induction period of anesthesia [3, 5, 13] and the results are controversial. It has even stated that short-term blockade of RAS might provide peri-operative organ protection and improve circula-tory conditions [15]. To our knowledge, there is no data comparing the effect of short-term versus chronic treatment with enalapril, one of the most frequently used ACE-I, on hemodynamic changes occurring during induction of anesthesia.
Therefore, the aim of the study was to com-pare short-term versus chronic treatment effects of enalapril on some hemodynamic (blood pressure and heart rate) parameters during the induction of general anesthesia.
Material and Methods
Patients and Treatment
val-ues of systolic blood pressure (SBP) > 160 mm Hg and diastolic blood pressure (DBP) < 110 mm Hg. In this group 5 mg enalapril was introduced on the day of admission (morning and evening) and con-tinued until the morning of surgery. All hyperten-sive patients were classified as ASA 2 (risk assess-ment American Society of Anesthesiologists). Group C consisted of 50 normotensive patients with ASA 1. All patients were admitted to the hos-pital two days before surgery and did not present any concomitant diseases.
on the morning of surgery, patients were pre-medicated with oral midazolam (7.5 mg) one hour before. Anesthesia was induced with etomidate (0.3 mg/kg) while the patient breathed 100% oxy-gen by mask. After loss of eyelid reflex chlorsuc-cinilocholin (1.5 mg/kg) was injected and after 1 minute the trachea was intubated. Before induc-tion, each patient received 500 ml of Ringer solution. Anesthesia was maintained throughout with a mix-ture of 66% nitrous oxide and 33% oxygen, supple-mented by sevoflurane < 1.5% inspirated concentra-tion and vecuronium for muscle relaxaconcentra-tion (0.1 mg/ kg). Fentanyl was also given in a dose of 2 ug/kg.
Hemodynamic Parameters
Measurement
Blood pressure (SBP, DBP) and heart rate (HR) were measured at admission (Ta), after treat-ment (Tt), while the baseline was measured after
premedication (T0). The other measurements were taken 2 minutes after induction (T1), 1 min-ute after intubation (T2) and 3 minmin-utes after intu-bation (T3). Blood pressure was monitored with a non-invasive automatic method using a Dameca anesthetic monitor (Denmark). Episodes of hypotension were defined as SBP < 100 mm Hg, DBP < 50 mm Hg, or a decrease of > 30% preinduc-tion (baseline) values. These episodes were treated routinely with administration of fluids. The study was approved by the local Bioethical Committee of the Medical University of Bialystok.
Statistical Analysis
Values were compared using Student’s unpaired t-test and changes over time were com-pared with ANoVA and the Kruskall-Wallis test, as well as Dunn’s multiple comparison test. Frequency of hypotensive episodes was measured with a Fisher test. Data was expressed as a mean (SD) and p < 0.05 was considered the level of sta-tistical significance.
Results
The three groups of patients were similar with regard to demographic characteristics but in group B the values of systolic and diastolic pressures (Ta) were higher (p < 0.01) (Tab. 1).
Table 1. Clinical characteristics of patient on admission
Tabela 1. Kliniczna charakterystyka pacjentów przy przyjęciu
Group (Grupa)
A B C
Number (liczba) 48 54 50
Age – years (Wiek – lata) 44 ± 7 40 ± 4 39 ± 7
Weight – kg
(Masa ciała – kg) 82 ± 7 89 ± 10 78 ± 9
Sex, n – male/n – -female
(Płeć, n – mężczyźni/n – kobiety) 28/10 32/8 38/12 SBp – mm Hg
(Ciśnienie skurczowe – mm Hg) 154 ± 15 174 ± 18** 138 ± 12 DBP – mm Hg
(Ciśnienie rozkurczowe – mm Hg) 86 ± 14 112 ± 11** 83 ± 11 HR – beats/min
(Częstość akcji serca – uderzeń/min) 78 ± 10 84 ± 7 74 ± 8
n – number/liczba pacjentów, SBP – systolic blood pressure, DBP – diastolic blood pressure,
Enalapril introduced after admission reduced (p
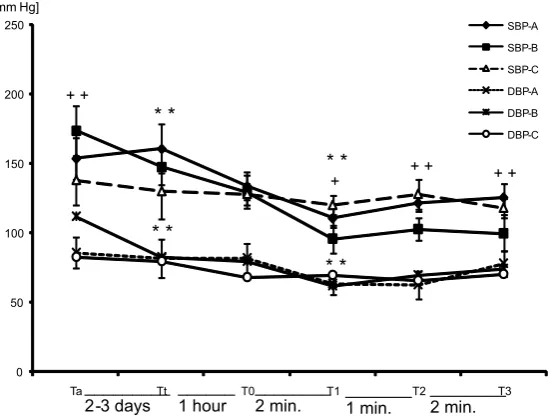
< 0.01) SBP and DBP (Tt) in group B after four doses (Fig. 1). on the day of surgery after premedication was given there were no differences in the baseline values (T0) of SBP, DBP (Fig. 1) and HR (Fig. 2). In group A, the induction of anesthesia (T1) was associ-ated with a decrease of SBP from 134 ± 10 to 111 ± 7 mm Hg (p < 0.05). Similar changes were observed in B group (from 130 ± 7 to 96 ± 16 mm Hg; p < 0,05). In control groups no significant changes were noted. DBP lowered after induction in all examined groups (Fig. 1). laryngoscopy and intubation (T2) induced changes in HR in both hypertensive groups (p < 0.01) (Fig. 2). The values of SBP in group B in times T2–T3 remained lower than the values in group A just as in the control group (Fig. 1).
Comparing the number of hypotensive epi-sodes in all groups the authors noticed that in group A three patients exhibited a decrease of SBP after induction of more than 30% from baseline values, while in group B there were 4 such patients (Tab. 2). Two hypotensive episodes were noted in patients from the control group. Also the number of patients with lower DBP did not differ significantly. All the patients responded well to fluid treatment and there was no need to use other medicaments.
Discussion
This study demonstrated that short-term (3–4 doses) ACE inhibition with enalapril allows the successful reduction of high systolic and diastolic blood pressures until the day of surgery, and gen-erates lower SBP during the induction period of anesthesia than chronic treatment. The authors also confirmed that induction of anesthesia may cause a marked decrease in systolic and diastolic blood pressures in chronically treated patients. Heart rate increase after intubation was compa-rable in both examined hypertensive groups and did not depend on the type of treatment.
In general anesthesia there are two points most dangerous of all: induction with intubation and the end of anesthesia with extubation. Generally one can expect slight hypotension after induc-tion and tachycardia after intubainduc-tion, however, under some clinical circumstances these responses may become exaggerated and therefore danger-ous. Most clinical investigators are in agreement that untreated hypertension may cause danger-ous cardiovascular effects during the induction of general anesthesia [16]. These effects include myocardial ischaemia caused by tachycardia with
0 50 100 150 200 250
Ta Tt T0 T1 T2 T3
[mm Hg]
SBP-A SBP-B SBP-C DBP-A DBP-B DBP-C
_________
2 -3 days ______ 1 hour ________2 min. _______1 min. ________2 min. + +
* *
* *
* *
+ + + +
* *
+
Fig. 1. Changes in SBP and DBP in patients during induction of anesthesia pointing to hypotension after propofol. Data show value (mean (SD)) at the time of admission (Ta), after treatment (Tt), baseline values before induction of anesthesia (T0), 2 minutes after induction of anesthesia (T1), 1 minute after intubation (T2), 3 minutes after intuba-tion (T3); A – patientschronically treated with ACE-I, B – patients received short term treatment of ACE-I, C – nor-motensive patients.
*p < 0.05; **p < 0.01; ++ – B vs A; ** – vs previous time
Ryc. 1. Zmiany wartości ciśnienia tętniczego skurczowego i rozkurczowego podczas wprowadzenia do znieczulenia ogólnego wskazujące na spadek ciśnienia tętniczego po podaniu propofolu. Dane ukazują wartości (średnie (SD)) przy przyjęciu pacjenta (Ta), po leczeniu (Tt), wartość wyjściową, przed wprowadzeniem do znieczulenia (T0), 2 minuty po wprowadzeniu do znieczulenia (T1), 1 minutę po intubacji (T2), 3 minuty po intubacji (T3); A – pacjenci otrzymujący ACE-I przewlekle, B – chorzy leczeni krótkotrwale, C – pacjenci z prawidłowym ciśnieniem tętniczym.
hypertension after laryngoscopy. The problem is of greater importance in emergency patients or in those with trauma, who have to be operated on as soon as possible. Therefore, many pharma-cological attempts have been made to attenuate these undesired changes. These attempts include strong premedication, supplementation of narcot-ics, i.v. lignocaine and beta-adrenoceptor blocking drugs. one of them, a very new clinical practice, is short-term (2–4 doses) or even acute application of ACE-I, 1–2 days before surgery, in patients with non treated hypertension [3].
In our study patients with mild uncontrolled hypertension on admission scheduled for maxillo-facial trauma surgery after enalapril treatment (Tt) presented decreased SBP and DBP values. on the day of surgery these values were comparable to those of patients who had been chronically treated, as well as to healthy ones (T0).
There is data indicating that strong hypoten-sion can occur after the first dose of ACE-I [14]. In the present study we did not observe this strong hypotensive effect. It must be mentioned, that we used relatively low, although effective doses of the drug. It should be stressed, however, that the values of SBP in the short-term treated group were signifi-cantly lower in all checked terms during the study,
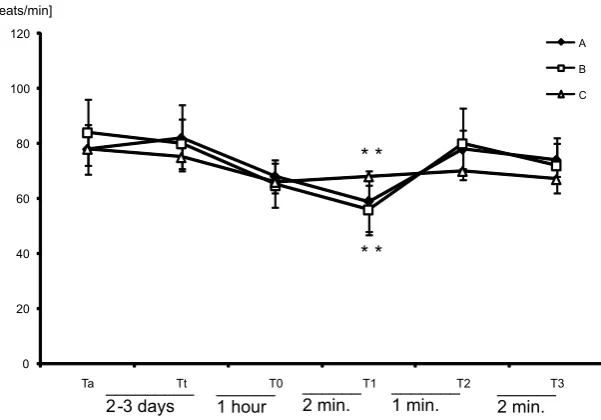
Fig. 2. Changes in HR in patients during induction of anesthesia pointing to bradycardia after propofol. Data show value (mean (SD)) at time of admission (Ta), after treatment (Tt), baseline values before induction of anesthesia (T0), 2 minutes after induction of anesthesia (T1), 1 minute after intubation (T2), 3 minutes after intubation (T3); A – patientschronically treated with ACE-I, B – patients received short term treatment of ACE-I, C – normotensive patients.
**p < 0.01
Ryc. 2. Zmiany w czynności serca u pacjentów podczas wprowadzenia do znieczulenia ogólnego wskazujące na bra-dykardię po podaniu propofolu. Dane ukazują wartości (średnie (SD)) przy przyjęciu pacjenta (Ta), po leczeniu (Tt), wartość wyjściową, przed wprowadzeniem do znieczulenia (T0), 2 minuty po wprowadzeniu do znieczulenia (T1), 1 minutę po intubacji (T2), 3 minuty po intubacji (T3); A – pacjenci otrzymujący ACE-I przewlekle, B – chorzy lecze-ni krótkotrwale, C – pacjenci z prawidłowym ciślecze-nielecze-niem tętlecze-niczym.
**p < 0,01
0 20 40 60 80 100 120
Ta Tt T0 T1 T2 T3
[beats/min]
A
B
C
______ 1 hour _________
2 -3 days ______2 min. _______1 min. ______2 min.
* * * *
Table 2. Patients with hypotensive episodes and the low-est DBP value.
Tabela 2. Pacjenci z epizodami hipotensji i najmniejszymi wartościami rozkurczowego ciśnienia tętniczego
Group
(Grupa) Patients with hypotensive epi-sodes
(Pacjenci z epizo-dami hipotensji)
Patients with the lowest value of DBP (Pacjenci
z najmniejszymi wartościami ciśnienia rozkur-czowego)
A
(n = 48) 3 4
B
(n = 54) 4 2
C
(n = 50) 2 2
but much more stable than in chronically treated patients. We have chosen the following end-points to assess cardiovascular stability: SBP after induc-tion of anesthesia of < 90 mm Hg, SBP after lar-yngoscopy and intubation more than 20% of base-line values and HR after intubation exceeding 100 beats/min. our data is in agreement with some other authors who point to cardiovascular stability after short-term and acute treatment with ACE-I [4, 17, 18]. It has also been shown that the ACE-I perindopril significantly reduces blood pressure values more after one day of treatment than other antihypertensive drugs (bisoprolol, verapamil, can-desartan) [19]. The strong effect of ACE inhibition is not surprising, because it has been demonstrat-ed [11], that even after temporary interruption of chronic ACE-I treatment, persistent inhibition of angiotensin-converting enzyme in tissues could be present despite the usual plasma-converting enzyme activity (19). Furthermore, there is data showing that this type of antihypertensive treat-ment demands lower doses of anesthetics for induction to reach the successful level of anesthe-sia, without impairing hemodynamics [4].
It is suggested that continuing ACE-I therapy until the day of surgery can attenuate the hemo-dynamic effect of anesthesia induction [10, 13, 21]. Coriat et al. have shown that the hypotensive response to induction of anesthesia is more pro-nounced in patients receiving enalapril than capto-pril [2]. However, in animals there is evidence that the type of ACE-I does not affect peri-operative hemodynamic changes [3]. Furthermore, it has been demonstrated that hypotensive episodes occur more frequently while using angiotensin II receptor type-1 antagonists rather than ACE-I [22]. Although the authors did not compare the effects of different drugs, the authors have confirmed a statistically sig-nificant decrease of SBP and DBP after induction in both hypertensive groups treated with enalapril.
The mild hypotensive response to induction found in own patients did not demand aggres-sive treatment (for example ephedrine) on top of fluid administration. The reason for only a mild hypotensive response may have been the design of the study: the anesthetic given for induction was etomidate, which is known to reduce the hemo-dynamic response to induction, whether hypoten-sive or hypertenhypoten-sive [12, 22, 23]. own earlier study
has shown, that another anesthetic, propofol, may induce hypotension during induction in chroni-cally enalapril-treated hypertensive patients [24]. one more reason could be the choice of patients: we examined only those with mild hypertension (DBP < 110 mm Hg) and without any other con-comitant diseases, while groups in other studies consisted of more severely ill patients i.e. with cor-onary artery disease, congestive heart failure, or diabetes mellitus [4]. There is always a greater risk of hypotension when a patient is treated with more than one drug. It has shown recently, that chronic diuretic treatment in hypertensive patients treated with ACE-I may produce profound hypotenion during anesthesia [25].
own patients seemed to be successfully pre-pared for anesthesia with an antihypertensive drug. laryngoscopy and intubation did not signif-icantly influence blood pressure parameters in the study; the increase of HR was comparable in both the short-term and the chronically treated groups (Fig. 2). Some authors have shown that tachycar-dia is considered to be dangerous over 110 beats per minute [26], but the values in our examined patients did not exceed 100 beats/min.
The fact that the authors compared quite a small group of patients undergoing a specific surgery and treated with one ACE-I may be limi-tation of this study. own findings may not fit aver-age surgical patients thus further studies are need-ed comparing different groups of patients, kinds of surgery and anesthetics.
In conclusion, short-term treatment with ACE-I in hypertensive patients undergoing max-illofacial trauma surgery successfully reduces high blood pressure until the day of surgery and induces lower values of SBP during the induc-tion period of anesthesia than in the chronically treated group. The authors would suggest that this short treatment in patients with mild hyperten-sion on admishyperten-sion who are scheduled for delayed emergency surgical procedure (i.e., two days maxi-mum) may improve their clinical status and level of safety during anesthesia. own study confirmed only mild hypotensive effect of induction of anes-thesia in patients chronically treated with ACE-I, and therefore the authors would suggest not to interrupt the treatment before surgery to avoid profound hypotension during induction.
References
[1] Sear JW, Jewkes C, Tellez J-C, Foex P: Does the choice of antihypertensive therapy influence haemodynamic responses to induction, laryngoscopy and intubation? Br J Anaest 1994, 73, 303–308.
[2] Coriat P, Richer C, Douraki T: Influence of chronic angiotensin-converting enzyme inhibition on anesthetic induction. Anesthesiology 1994, 81, 299–307.
[4] Licker M, Neidhart P, Lustenberger S: long-term angiotensin-converting enzyme inhibitor treatment attenu-ates adrenergic responsiveness without altering hemodynamic control in patients undergoing cardiac surgery. Anesthesiology 1996, 84, 789–800.
[5] Colson P: Angiotensin-converting enzyme inhibitors in cardiovascular anesthesia. J Cardiothor Vasc Anesth 1993, 7, 734–742.
[6] Ullman J: Vasopressin and angiotensin II in blood pressure control during isoflurane anesthesia in rats. Acta Anesthesiol Scand 1999, 43, 860–865.
[7] Ullman JE, Hjelmqvist H, Rundgren M, Leksell LG: Hemodynamic effects of vasopressin antagonism and angio-tensin I converting enzyme inhibition during halothane anesthesia in sheep. Acta Anesthesiol Scand 1992, 36, 132–137.
[8] Varon J, Marik PE: Perioperative hypertension management. Vasc Health Risk Manag 2008, 4, 615–627.
[9] Wallner T, Preis C, Mayer N: Cardiac medication in the perioperative period. Acta Anesthesiol Scand 1997, 111, 22–28.
[10] Comfere T, Sprung J, Kumar MM, Draper M, Wilson DP, Williams BA, Danielson DR, Liedl L, Warner DO:
Angiotensin system inhibitore in a general surgical population. Anesth Analg 2005, 100, 636–644.
[11] Eyraud D, Mouren S, Teugels K, Bertrand M, Coriat P: Treating anesthesia-induced hypotension by angio-tensin II in patients chronically treated with angioangio-tensin-converting enzyme inhibitors. Anesth Analg 1998, 86, 259–263.
[12] Kwella N, Kasperczyk J, Araszkiewicz A, Koroll: The influence of chronic treatment with angiotensin convert-ing enzyme inhibitors on blood pressure parameters durconvert-ing general anesthesia in laryngological surgery. Nowiny lekarskie 2000, 69, 251–259.
[13] Behnia R, Molteni A, Igić R: Angiotensin-converting enzyme inhibitors: mechanisms of action and implications in anesthesia practice. Curr Pharm Des 2003, 9, 763–776.
[14] Mangano DT: Cardiovascular morbidity association with surgery: perspectives and new findings.Ann Card Anaesth 1998, 1, 5–40.
[15] Licker M, Mortel DR: Inhibitors of the rennin angiotensin system: implications for the anaesthesiologist. Curr opin Anaesthesiol 1998, 11, 321–326.
[16] Colson P, Ribstein J, Mimran A, Grolleau D, Chaptal PA, Roquefeuil B: Effect of angiotensin-converting enzyme inhibition on blood pressure and renal function during open heart surgery. Anesthesiology 1990, 72, 23–27.
[17] Yates AP, Hunter DN: Anesthesia and angiotensin-converting enzyme inhibitors. The effect of enalapril on peri-operative cardiovascular stability. Anaesthesia 1988, 43, 935–938.
[18] Adamska-Dyniewska H, Ptaszyński W: Blood pressure variability and smoothness index after 6 antihypertensive drugs. Arterial Hypertens 2000, 4, 181–186.
[19] Falkenhahn M, Gohlke P, Paul M, Stoll M, Unger T: The renin-angiotensin system in the heart and vascular wall: new therapeutic aspects J Cardiovasc Pharmacol 1994, 24, S6–13.
[20] Colson P, Saussine M, Seguin JR: Hemodynamic effects of anesthesia in patients chronically treated with angio-tensin-converting enzyme inhibitors. Anesth Analg 1992, 74, 805–808.
[21] Brabant SM, Bertrand M, Eyraud D, Darmon PL, Coriat P: The hemodynamic effects of anesthetic induction in vascular surgical patients chronically treated with angiotensin II receptor antagonists. Anesth Analg 1999, 89, 1388–1392.
[22] Bendel S, Ruokonen E, Pölönen P, Uusaro A: Propofol causes more hypotension than etomidate in patients with severe aortic stenosis: a double-blind, randomized study comparing propofol and etomidate. Acta Anaesthesiol Scand 2007, 51, 284–289.
[23] Reich DL, Hossain S, Krol M, Baez B, Patel P, Bernstein A, Bodian CA: Predictors of hypotension after induc-tion of general anesthesia. Anesth Analg 2005, 10, 622–628.
[24] Malinowska-Zaprzałka M, Wojewódzka M, Dryl D, Grabowska SZ, Chabielska E: Hemodynamic effect of propofol in enalapril-treated hypertensive patients during induction of general anesthesia. Pharmacol Rep 2005, 57, 675–678.
[25] Kheterpal S, Khodaparast O, Shanks A, OReilly M, Tremper KK: Chronic angiotensin-converting enzyme inhibitor or angiotensin receptor blocker therapy combined with diuretic therapy is associated with increased episodes of hypotension in noncardiac surgery. J Cardiothorac Vasc Anesth 2008, 22, 180–186.
[26] Slogoff S, Keats AS: Randomized trial of primary anesthetic agents on outcome of coronary artery bypass opera-tions. Anesthesiology 1989, 70, 179–188.
Address for correspondence:
Małgorzata Malinowska-Zaprzałka Biopharmacy Department
Medical University of Bialystok Mickiewicza 2C
15-222 Białystok Poland
E-mail: [email protected]
Conflict of interest: None declared Received: 27.01.2010