Original Article
Chest pain centers contribute to decrease in acute
cardiac complications and better short-term
prognosis for patients with AMI
Wenbin Lu1, Ziwei Zhang2, Jiandong Ding1, Qiming Dai1, Yu Wang1, Lijuan Chen1, Genshan Ma1
1Department of Cardiology, Zhongda Hospital, Affiliated to Southeast University, Nanjing, China; 2Division of Endo-crinology, The Drum Tower Hospital, Affiliated to Nanjing University, Nanjing, China
Received January 3, 2018; Accepted June 7, 2018; Epub August 15, 2018; Published August 30, 2018
Abstract: Background: Acute myocardial infarction (AMI), especially ST elevation myocardial infarction (STEMI), not only increases risk for cardiovascular complications and mortality but also leads to decreased quality of life. Re-cently, the creation of Chest Pain Centers (CPCs) in China has ensured that AMI patients are diagnosed and treated in a timely fashion. This present study aimed to compare different patterns of acute cardiac complications and short-term prognosis in STEMI patients treated in the CPC. Methods: Prior to creation of the CPC, 53 STEMI patients were selected and carefully examined (January 2014-December 2014). Baseline clinical data were also included in the evaluation. After creation of the CPC, another 52 STEMI patients were enrolled (January 2015-December 2015). All patients received formal AMI treatment to ameliorate symptoms and preserve the structure and function of the heart according to AMI guidelines for China (2014-2016). Acute cardiac complications, within 7 days, for these STE-MI patients were compared. The groups were also compared in terms of short-term prognosis (at 90 days) using a Kaplan-Meier estimator. Cox proportional-hazard models were further used to analyze association of the prognosis and effects of CPC after adjusting for confounding factors (diabetes, cerebral infarction, hypertension, smoking, hy-perlipidemia, and renal insufficiency). Results: The first medical contact to oral medication load time (FMC2M) was significantly lower in patients after creation of the CPC compared with STEMI patients before the CPC was created (p < 0.001). First medical contact of patients to balloon opening time (FMC2B) was also significantly decreased in STEMI patients after creation of the CPC (p < 0.001). Acute cardiac complications, within 7 days, were significantly lower in these STEMI patients after creation of the CPC (p < 0.001). In addition, these STEMI patients also showed decreased cardiovascular events in the next 90 days after creation of the CPC. Univariate Kaplan-Meier analysis further revealed significant differences between the two groups (p < 0.001). Conclusions: The Chest Pain Center produced lower incidence of cardiac complications and better prognosis for STEMI patients. Effective, efficient, and timely treatment under the influence of a CPC may greatly explain the causality.
Keywords: Myocardial infarction, chest pain center, percutaneous coronary intervention
Introduction
Chest pains are the subjective feelings of sharp or dull pains, including pressure, shortness of breath, and often accompanied by anxiety or fear. Chest pains are one of the most common symptoms for an emergency activation. One cross-sectional study in Beijing showed that chest pain patients accounted for approxima- tely 4.7% of emergency patients [1]. A total of 13,740 chest pain patients were followed up for 1 year in the British General Practitioner Study Database. Results showed that ischemic
difficulty of early recognition and timely treat-ment of AMI. In recent years, diagnosis and treatment of myocard-ial infarction, especially acute ST-segment Elevation Myocardial Infarc- tion (STEMI), has progressed under the back-drop of established guidelines for AMI and influ-ence of the creation of CPCs. This present study aimed to compare and analyze different pat-terns of acute cardiac complications and short-term prognoses in STEMI patients treated in the CPC.
Materials and methods
Study population
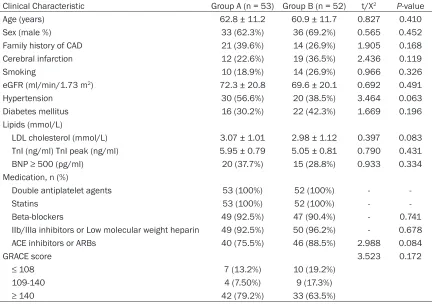
[image:2.612.90.527.86.390.2]All enrolled patients were STEMI patients. All patients were admitted to the Cardiac Center of Zhongda Hospital, Affiliated with Southeast University, and received formal AMI treatment, including percutaneous coronary intervention (PCI), to ameliorate symptoms and preserve the structure and function of the heart according to Table 1. Baseline characteristics
Clinical Characteristic Group A (n = 53) Group B (n = 52) t/X2 P-value
Age (years) 62.8 ± 11.2 60.9 ± 11.7 0.827 0.410 Sex (male %) 33 (62.3%) 36 (69.2%) 0.565 0.452 Family history of CAD 21 (39.6%) 14 (26.9%) 1.905 0.168 Cerebral infarction 12 (22.6%) 19 (36.5%) 2.436 0.119 Smoking 10 (18.9%) 14 (26.9%) 0.966 0.326 eGFR (ml/min/1.73 m2) 72.3 ± 20.8 69.6 ± 20.1 0.692 0.491
Hypertension 30 (56.6%) 20 (38.5%) 3.464 0.063 Diabetes mellitus 16 (30.2%) 22 (42.3%) 1.669 0.196 Lipids (mmol/L)
LDL cholesterol (mmol/L) 3.07 ± 1.01 2.98 ± 1.12 0.397 0.083 TnI (ng/ml) TnI peak (ng/ml) 5.95 ± 0.79 5.05 ± 0.81 0.790 0.431 BNP ≥ 500 (pg/ml) 20 (37.7%) 15 (28.8%) 0.933 0.334 Medication, n (%)
Double antiplatelet agents 53 (100%) 52 (100%) - Statins 53 (100%) 52 (100%) - Beta-blockers 49 (92.5%) 47 (90.4%) - 0.741 IIb/IIIa inhibitors or Low molecular weight heparin 49 (92.5%) 50 (96.2%) - 0.678 ACE inhibitors or ARBs 40 (75.5%) 46 (88.5%) 2.988 0.084
GRACE score 3.523 0.172
≤ 108 7 (13.2%) 10 (19.2%) 109-140 4 (7.50%) 9 (17.3%) ≥ 140 42 (79.2%) 33 (63.5%)
Baseline Clinical Characteristics of STEMI patients. Group A, STEMI patients selected before the creation of a CPC; Group B, STEMI patients selected after the creation of a CPC. Values are mean ± SD, or n (%). ACEI: angiotensin-converting enzyme inhibi-tors; CAD: Coronary artery disease; BNP: B-natriuretic peptide; TnI Troponin I; eGFR: estimated glomerular filtration rate; LDL: low-density lipoprotein; ARB: angiotensin II receptor antagonists; GRACE: The Global Registry of Acute Coronary Events.
Table 2. Comparison of number of related offending vessel lesions
Group N Offending vessel lesions (%) Number of vessels involved (lesions ≥ 50%) LM LAD LCX RA One Two Three Group A 53 7 (13.2%) 15 (28.3%) 13 (24.5%) 18 (34.0%) 23 (43.4%) 16 (30.2%) 14 (26.4%) Group B 52 5 (936%) 20 (38.5%) 12 (23.1%) 15 (28.8%) 20 (38.5%) 20 (38.5%) 12 (23.1%)
t/x2 - 1.351 0.798
P Value - 0.717 0.671
[image:2.612.88.524.466.545.2]AMI guidelines for China (2014-2015). Prior to creation of a CPC, 53 STEMI patients were selected and carefully examined (Group A). In addition, 52 STEMI patients were enrolled after creation of the CPC (Group B). Clinical data in terms of comorbidities, cardiovascular or cere-brovascular disease history, smoking history, blood pressure, cholesterol, estimated glomer-ular filtration rate (eGFR), left ventricglomer-ular ejec-tion fracejec-tion (LVEF), drugs taken, and GRACE scores were mostly acquired from hospital medical records. This study was approved by the local Ethics Committee and performed in accordance with the Declaration of Helsinki.
Definitions of STEMI
For patients having ST elevation myocardial infarction (STEMI), at least two of the following criteria had to be met in addition to ST segment elevation in 2 or more contiguous leads (Cut-off point: ≥ 0.1 mv) [6, 7]: typical symptoms or typi-cal signs of AMI including angina equivalents (severe substernal chest pain, chest tightness or severe precordial discomfort with cold sweat, and an impending sense of doom) and an increased level of biomarkers specific for myo-cardial injury, especially Troponin I (TnI ≥ 0.04 ng/mL). Subjects with any of the following exclusion criteria were not allowed: ≥ 80 years old or < 18 years old, severe liver or kidney dis-eases, glomerular filtration rate (GFR) of < 30 ml/(min∙1.73 m2) or Child-Turcotte-Pugh (CTP) score ≥ 6, coagulation disorders associat- ed with significant bleeding, intake of syste- mic immunosuppressive agents, occurrence of other serious disorders during the study period, and life expectancy of less than 6 months.
Definitions of primary end points
Primary end points of the study included inci-dence of acute myocardial infarction
complica-tions in the acute phase (within 1 week) and incidence of cardiovascular events in the short-term (90-days). Myocardial infarction compli- cations were defin-ed as follows: arrhythmia (including atrial fibrillation, ventricular tachycar-dia, ventricular fibrillation, ≥ II° atrioventricular block), acute left ventricle failure, aneurysm, papillary muscle dysfunction or rupture (con-firmed by color Doppler), ventricular wall rup-ture, and subsequent sudden cardiac death. Adverse cardiovascular events were defined as heart failure, re-admission, target vessel revas-cularization, stent thrombosis, recurrent myo-cardial infarction, non-hemorrhagic stroke, and ischemic or vascular thrombosis-related deaths. All criteria were in accordance with Academic Research Consortium criteria [8, 9].
Statistical analysis
Data management and statistical analysis were performed with Statistical Package for Social Sciences software (SPSS version 19.0 for Windows, SPSS Inc.). Data are expressed as mean ± standard deviation or as median and interquartile range when necessary. Categori- cal variables were compared using X2 test or Fisher’s exact test. For continuous data, group comparisons were performed using an unpair- ed t test or Mann-Whitney U-test. Log-rank Mantel-Cox tests and Kaplan-Meier survival curves were used to compare event-free sur-vival. Results were considered statistically sig-nificant if the two-sided p-value was ≤ 0.05. Results
Baseline characteristics for the two groups
Clinical characteristics of STEMI patients in the two groups are summarized in Table 1. There were no significant differences between the groups in terms of age, sex, smoking history, diabetes mellitus, hypertension, or other chron-ic diseases. Risk factors in AMI patients after creation of the CPC, such as cholesterol, GRACE scores, and clinical medication, seem to have been reduced. However, there were still no significant differences revealed. The culprit vessel and number of diseased blood vessels of these STEMI patients are shown in Table 2.
Time of first medical contact to balloon open-ing in the two groups
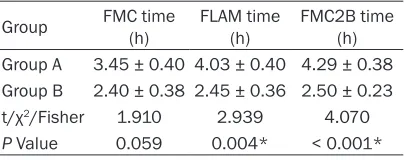
[image:3.612.91.293.84.164.2]The amount of time required to treat patients with acute myocardial infarction is expected Table 3. Door-to-balloon times for each group
Group FMC time (h) FLAM time (h) FMC2B time (h) Group A 3.45 ± 0.40 4.03 ± 0.40 4.29 ± 0.38 Group B 2.40 ± 0.38 2.45 ± 0.36 2.50 ± 0.23 t/χ2/Fisher 1.910 2.939 4.070
P Value 0.059 0.004* < 0.001*
to be less under the establishment of ch- est pain center. This study found that the fir- st medical contact time in group B (STEMI patients enrolled after creation of the CPC) was shorter than in Group A (STEMI pati- ents enrolled before creation of the CPC), thou- gh there were no significant differences bet- ween the groups (FMC, 2.40 ± 0.38 vs. 3.45 ± 0.40, p = 0.059). However, both the first time of oral loading doses of antiplatelet ag- ents (FLAM, 2.45 ± 0.36 vs. 4.03 ± 0.40, p = 0.004) and first medical contact to balloon opening time (FMC2B, 2.50 ± 0.23 vs. 4.29 ± 0.38, p < 0.001) were signifcantly shorter in group B than in group A (Table 3).
7-day incidence of acute cardiac complications
The establishment of a chest pain center is to ensure that AMI patients receive medical treat-ment as quickly as possible. Therefore, cardiac complications at the time of the acute phase is expected to be less than those prior to the inception of the CPC. This study defined acute myocardial infarction complications as follows: cardiac death due to papillary muscle dysfunc-tion or the rupture of the ventricular wall as con-firmed by color Doppler, ventricular aneurysm,
acute heart failure, and arrhythmia (including atrial fibrillation, ventricular and supraventricu-lar tachycardia, ventricusupraventricu-lar fibrillation, ≥ II° atrioventricular block). It was found that inci-dence of complications in STEMI patients was significantly lower in group B than in group A (28.8% vs. 60.4%, t = 10.55, p < 0.001). Speci- fic complications are listed in Table 4.
Comparison of cardiovascular events between the two groups
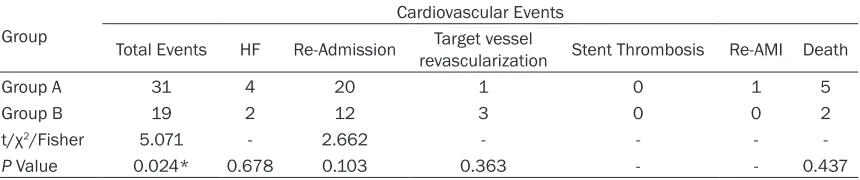
[image:4.612.91.524.86.164.2]Retrospective analysis of major cardiovas- cular events in the 90 days after an AMI (- heart failure, readmission, target vessel revas-cularization, stent thrombosis, recurrent myo-cardial infarction, non-hemorrhagic stroke, and ischemic or vascular thrombosis-relat- ed deaths) showed significant differences between the groups (36.5% vs. 58.5%, χ2 = 5.071 p = 0.024). Incidence of adverse ev- ents in group B (19 cases) was significant- ly lower than in group A (31 cases), after es- tablishment of the Chest Pain Center. There were only 2 patients that suffered from is- chemic or vascular-related deaths after cre-ation of the CPC, compared to 5 patients in group A. There were 12 patients readmitt- Table 4. Acute cardiac complications within the first 7 days
Group Acute cardiac complications
Total complications Cardiac death Ventricular aneurysm Acute heart failure Arrhythmia
Group A 32 3 3 11 15
Group B 15 1 2 5 7
t/x2/Fisher 1.55 - - 2.522 3.490
P Value < 0.001* 0.618 1.0 0.112 0.062
Group A, STEMI patients selected before the creation of a CPC; Group B, STEMI patients selected after the creation of a CPC; Arrhythmia (including atrial fibrillation, ventricular and supraventricular tachycardia, ventricular fibrillation, ≥ 2nd degree
atrioven-tricular block). *P ≤ 0.05 vs. the control group.
Table 5. Cardiovascular events between the two groups
Group
Cardiovascular Events
Total Events HF Re-Admission revascularizationTarget vessel Stent Thrombosis Re-AMI Death
Group A 31 4 20 1 0 1 5
Group B 19 2 12 3 0 0 2
t/χ2/Fisher 5.071 - 2.662 - - -
-P Value 0.024* 0.678 0.103 0.363 - - 0.437
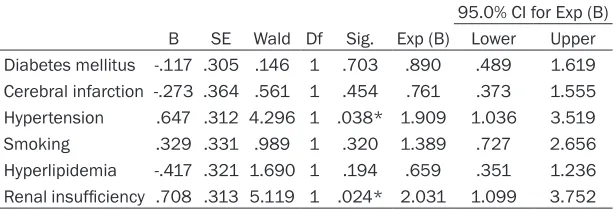
[image:4.612.92.522.233.323.2]ed for various reasons in group B compared to 20 patients in group A (Table 5). Statisti- cally significant differences between the two groups were further shown in the Kaplan-Meier suvival curves (41.5% vs. 63.5%; log-rank test χ2 = 4.24, p = 0.039) (Figure 1A). Multivariate regression analysis was further applied after adjusting for diabetes mellitus, cerebral in- farction, hypertension, smoking, hyperlipiemia, and renal insufficiency. Results indicated that STEMI patients in group B had less adverse cardiovascular outcomes (X2 = 20.625, p = 0.004). Survival function at the mean of covariates is shown in Figure 1B. Further- more, results showed that renal insufficiency (HR: 2.031, 95% CI: 1.099-3.752, p = 0.024) and hypertension (HR: 1.909, 95% CI: 1.036-3.519, p = 0.038) were associated with
[image:5.612.88.522.75.246.2]occur-therapeutic straegy [10]. Chest Pain Centers have been created to exclusively treat chest pain patients. The symptoms of chest pain may be sharp, dull, burning, aching, and stabbing or they may be a tight, squeezing, or crushing sensation. Acute myocardial infarction (heart attack) is a more severe discomfort accom-panied by crushing sub-sternal pain. AMI is an acute and urgent inflammatory disease charac-terized by the rupture of arterial plaques and interruption of blood supply to the myocardium. This present study demonstrated that the foun-dation of a Chinese Chest Pain Center signifi-cantly lowered incidence of acute cardiac complications in the first week. Furthermore, cardiac events significantly decreased in the following 3 months after creation of the Chest Table 6. Multivariate regression analysis of 90-day survival functions
95.0% CI for Exp (B) B SE Wald Df Sig. Exp (B) Lower Upper Diabetes mellitus -.117 .305 .146 1 .703 .890 .489 1.619 Cerebral infarction -.273 .364 .561 1 .454 .761 .373 1.555 Hypertension .647 .312 4.296 1 .038* 1.909 1.036 3.519 Smoking .329 .331 .989 1 .320 1.389 .727 2.656 Hyperlipidemia -.417 .321 1.690 1 .194 .659 .351 1.236 Renal insufficiency .708 .313 5.119 1 .024* 2.031 1.099 3.752
[image:5.612.90.397.320.425.2]Multivariate regression analysis of 90-day survival functions of the mean covariates after adjusting for confounding factors in STEMI patients in the equation are shown. B: Partial regression coefficient; SE: Standard error of partial regression coefficient; Wald: test of the significance between the total partial regression coefficient and zero,when v = 1, W = (B/ SE)2; Exp (B): relative risk (RR value). *P ≤ 0.05 vs. the control group.
Figure 1. Univariate Kaplan-Meier and multivariate regression analysis. A. Survival functions in two groups of STEMI patients before (blue line) and after (red line) the creation of a CPC. B. Multivariate regression analysis after adjust-ing for confoundadjust-ing factors in STEMI patients.
rence of adverse cardio-vasclarevents (Table 6). Discussion
Pain Center (patients in group B). These results indicate that the quick reactions of a Chest Pain Center, especially in preparation of the cardiac catheterization lab, play a very active role in the diagnosis and treatment of AMI patients, including re-canalization of acutely occluded vessels in STEMI patients.
It should be noted there are still many other possible critical factors that could have contrib-uted to a decrease in cardiac complications and adverse cardiovascular events. This study further analyzed first medical contact time, oral dose loading time of antiplatelet agents, and balloon time in the two groups. This study is the first to show that loading of antiplatelet agents (aspirin 300 mg and ticagrelor 180 mg) was very timely in STEM patients, after creation of Chest Pain Center, in comparison to that be- fore. Most AMI patients received a loading of antiplatelet agents only after admittance to the Emergency Department and confirmation by ECG and cardiac enzymes of AMI. It should be noted that most STEMI patients in group B received a loading dose of antiplatelet agents just after first medical contact with Emergency Medical Services (EMS) providers within the allotted 120 minutes of transport time. In addi-tion, these patients were directly transferred to the Cardiac Catheter Lab for emergency coro-nary angiographies instead of being admitted to the Emergency Department. This specifica- lly contributed to decreased door-to-balloon times. Thus, these various time-saving proce-dures greatly reduced the extent of cardiomyo-cyte deaths and myocardial necrosis.
These results also partially confirm the ideal reported by Steven M. et al. [30], stating that Chest Pain Centers aim to provide care that is safe, effective, efficient, timely, and patient-centered. Translation of these aims into clinical practice for STEMI patients ensures the timely transfer of STEMI patients to PCI-capable cen-ters [11, 12]. According to ACC/AHA/SCAI gui- delines that are focused on primary percutane-ous coronary intervention for patients with STEMI [13-15], Emergency Medical Services and integrated PCI networks are critical for these patients regarding door-to-balloon times of less than 90 minutes and transport to PCI-capable centers of less than 120 minutes. In fact, there remains a great discrepancy bet- ween clinical reality and recommendations of the guidelines, particularly in developing
coun-tries [16, 17]. However, according to this pres-ent study, the Chest Pain Cpres-enter contributed to reduction of this discrepancy and greatly reduced door-to-balloon times.
Diabetes mellitus, cerebral infarction, hyper-tension, smoking, hyperlipidemia, and renal insufficiency are all risk factors for cardiova- scular disease, contributing to reverse remod-eling in AMI patients [18, 19]. This study found that renal insufficiency and hypertension are associated with occurrence of adverse car- diovascular events, indicating that long-term chronic inflammatory lesions accompanied by higher oxidative stress and increased ROS plays an important adversarial role in cardio-vascular events in AMI patients. However, this retrospective study had the limitations of a small sample. Prospective, multi-center, large sample studies are urgently needed. On the other hand, the construction of China’s Chest Pain Center was arrived late by 2013 and the current number of CPCs is less than one hun-dred compared to thousands of PCI-capable centers in America [20]. Meanwhile, growth of PCI-capable centers has not been uniform in relation to prevalence of AMI or distance between PCI-capable facilities [21]. Thus, more chest pain centers are urgently needed to lower incidence of acute cardiac complications and adverse cardiac events.
Conclusions
This retrospective study found that establish-ment of the Chest Pain Center contributed to lower incidence of acute cardiac complications and decreased adverse cardiovascular out-comes, suggesting better prognosis for STEMI patients treated in the Chest Pain Center. In addition, this study concludes that renal insuf-ficiency and hypertension can affect the prog-nosis of these STEMI patients, indicating that early, effective, efficient, and timely interven-tion is necessary. However, whether the current model of the Chest Pain Center can further optimize and enrich the prognosis of STEMI patients while serving as a standard therapeu-tic strategy for AMI should be further studied. Acknowledgements
Technology Department of Jiangsu Province-Social Development and Standardized Diagno- sis and Treatment of Key Diseases Project (No. BE2016785).
Disclosure of conflict of interest
None.
Address correspondence to: Genshan Ma, Wenbin Lu and Jiandong Ding, Department of Cardiology, Zhongda Hospital, Affiliated to Southeast Universi- ty, 89# Dingjiaqiao Road, Nanjing 210009, China. Tel: +86-02583262595; E-mail: [email protected] (GSM); Tel: +86-13605185175; E-mail: [email protected] (WBL); Tel: +86-1395163- 4029; E-mail: [email protected] (JDD)
References
[1] Ma CP, Wang X, Wang QS, Liu XL, He XN, Nie SP. A modified HEART risk score in chest pain patients with suspected non-ST-segment ele-vation acute coronary syndrome. J Geriatr Car-diol 2016; 13: 64-9.
[2] Ishak M, Ali D, Fokkert MJ, Slingerland RJ, Dik-keschei B, Tolsma RT, Lichtveld RA, Bruins W, Boomars R, Bruheim K, van Eenennaam F, Timmers L, Voskuil M, Doevendans PA, Mo-sterd A, Hoes AW, ten Berg JM, van‘t Hof AW; FAMOUS TRIAGE Study Group. Fast assess-ment and manageassess-ment of chest pain without ST-elevation in the pre-hospital gateway: ratio-nale and design. Eur Heart J Acute Cardiovasc Care 2015; 4: 129-36.
[3] Wächter C, Markus B, Schieffer B. Cardiac causes of chest pain. Internist (Berl) 2017; 58: 8-21.
[4] Kohlhauer M, Berdeaux A, Ghaleh B, Tissier R. Therapeutic hypothermia to protect the heart against acute myocardial infarction. Arch Car-diovascular Dis 2016; 109: 716-722.
[5] Dind A, Allahwala U, Asrress KN, Jolly SS, Bhin-di R. Contemporary management of ST-eleva-tion myocardial infarcST-eleva-tion. Heart Lung Circ 2017; 26: 114-121.
[6] Swenne CA. Improved STEMI diagnosis by se-rial ECG analysis. J Electrocardiol 2015; 48: 99-100.
[7] Rowland-Fisher A, Smith S, Laudenbach A, Reardon R. Diagnosis of acute coronary occlu-sion in patients with non-STEMI by point-of-care echocardiography with speckle tracking. Am J Emerg Med 2016; 34: 1914, e3-6. [8] Bijuklic K, Schwencke C, Schofer J. Long-term
major adverse cardiac and cerebrovascular events (MACCE) rate: comparison of retrograde and antegrade recanalization of chronic total
coronary occlusions. Wien Klin Wochenschr 2017; 129: 243-250.
[9] Kalra PR, Greenlaw N, Ferrari R, Ford I, Tardif JC, Tendera M, Reid CM, Danchin N, Stepinska J, Steg PG, Fox KM. Hemoglobin and change in hemoglobin status predict mortality, cardio-vascular events and bleeding in stable coro-nary artery disease. Am J Med 2017; 130: 720-730.
[10] Köhnlein T. Chest pain in the emergency de-partment: differential diagnosis and diagnos-tic strategy. Internist (Berl) 2017; 58: 3-7. [11] Langabeer JR 2nd, Smith DT,
Cardenas-Turan-zas M, Leonard BL, Segrest W, Krell C, Owan T, Eisenhauer MD, Gerard D. Impact of a rural regional myocardial infarction system of care in Wyoming. J Am Heart Assoc 2016; 5. pii: e003392.
[12] Jacobs AK, Antman EM, Faxon DP, Gregory T, Solis P. Development of systems of care for ST-elevation myocardial infarction patients: ex-ecutive summary. Circulation 2007; 116: 217-30.
[13] Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Ting HH, O’Gara PT, Kushner FG, Ascheim DD, Brindis RG, Casey DE Jr, Chung MK, de Lemos JA, Diercks DB, Fang JC, Franklin BA, Granger CB, Krumholz HM, Linderbaum JA, Morrow DA, Newby LK, Ornato JP, Ou N, Radford MJ, Tamis-Holland JE, Tommaso CL, Tracy CM, Woo YJ, Zhao DX. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary interven-tion for patients with ST-elevainterven-tion myocardial infarction: an update of the 2011 ACCF/AHA/ SCAI guidelinefor percutaneous coronary inter-vention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol 2016; 67: 1235-50.
[14] Caporale R, Geraci G, Gulizia MM, Borzi M, Co-livicchi F, Menozzi A, Musumeci G, Scherillo M, Ledda A, Tarantini G, Gerometta P, Casolo G, Formigli D, Romeo F, Di Bartolomeo R. ANMCO/ SIC/SICI-GISE/SICCH consensus document: clinical approach to pharmacological pretreat-ment for patients undergoing myocardial re-vascularization. G Ital Cardiol (Rome) 2016; 17: 462-90.
2014 ESC/EACTS guidelines on myocardial re-vascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Associa-tion for Cardio-Thoracic Surgery (EACTS) Devel-oped with the special contribution of the Euro-pean Association of Percutaneous Cardiovas- cular Interventions (EAPCI). Eur Heart J 2014; 35: 2541-619.
[16] Task Force Members1, Montalescot G, Sech-tem U, Achenbach S, Andreotti F, Arden C, Bu-daj A, Bugiardini R, Crea F, Cuisset T, Di Mario C, Ferreira JR, Gersh BJ, Gitt AK, Hulot JS, Marx N, Opie LH, Pfisterer M, Prescott E, Ruschitzka F, Sabaté M, Senior R, Taggart DP, van der Wall EE, Vrints CJ; ESC Committee for Practice Guidelines, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Dea-ton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancel-lotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Ten-dera M, Torbicki A, Wijns W, Windecker S; Doc-ument Reviewers, Knuuti J, Valgimigli M, Bue-no H, Claeys MJ, Donner-Banzhoff N, Erol C, Frank H, Funck-Brentano C, Gaemperli O, Gon-zalez-Juanatey JR, Hamilos M, Hasdai D, Hus-ted S, James SK, Kervinen K, Kolh P, Kris-tensen SD, Lancellotti P, Maggioni AP, Piepoli MF, Pries AR, Romeo F, Rydén L, Simoons ML, Sirnes PA, Steg PG, Timmis A, Wijns W, Winde-cker S, Yildirir A, Zamorano JL. 2013 ESC guidelines on the management of stable coro-nary artery disease: the task force on the man-agement of stable coronary artery disease of the European Society of Cardiology. Eur Heart J 2013; 34: 2949-3003.
[17] Helve S, Viikilä J, Laine M, Lilleberg J, Tierala I, Nieminen T. Trends in treatment delays for pa-tients with acute ST-elevation myocardial in-farction treated withprimary percutaneous coronary intervention. BMC Cardiovasc Disord 2014; 14: 115.
[18] Bradley SM, Carey EP, Michael Ho P. US growth in PCI care--less than ideal, but is the ideal less? J Am Heart Assoc 2013; 19; 2: e000552. [19] Noor Hassim I, Norazman MR, Diana M,
Khairul Hazdi Y, Rosnah I. Cardiovascular risk assessment between urban and rural popula-tion in Malaysia. Med J Malaysia 2016; 71: 331-337.
[20] Harumi Higuchi Dos Santos M, Sharma A, Sun JL, Pieper K, McMurray JJ, Holman RR, Lopes RD. International variation in outcomes among people with cardiovascular disease or cardio-vascular risk factors and impaired glucose tol-erance: insights from the NAVIGATOR trial. J Am Heart Assoc 2017; 13; 6. pii: e003892. [21] Concannon TW, Nelson J, Kent DM, Griffith JL.