www.journalofoptometry.org
ORIGINAL
ARTICLE
Visual
function
and
color
vision
in
adults
with
Attention-Deficit/Hyperactivity
Disorder
Soyeon
Kim
a,
Samantha
Chen
a,
Rosemary
Tannock
a,b,∗aDepartmentofAppliedPsychology&HumanDevelopment,UniversityofToronto,Toronto,Canada bNeurosciences&MentalHealthResearchProgram,HospitalforSickChildren,Toronto,Canada
Received1April2013;accepted3July2013 Availableonline16August2013
KEYWORDS Visualfunction; AdultswithADHD; Colorvision; ADHD
Abstract
Purpose:Colorvision andself-reportedvisual functionineverydaylifeinyoungadultswith Attention-Deficit/HyperactivityDisorder(ADHD)wereinvestigated.
Method: Participantswere 30youngadultswithADHDand30 controlsmatched forageand gender.TheyweretestedindividuallyandcompletedtheVisualActivitiesQuestionnaire(VAQ), Farnsworth-Munsell100HueTest(FMT)andAQuickTestofCognitiveSpeed(AQT).
Results:TheADHDgroupreportedsignificantlymoreproblemsin4of8areasontheVAQ:depth perception,peripheralvision,visualsearchandvisualprocessingspeed.FurtheranalysesofVAQ itemsrevealedthattheADHDgroupendorsedmorevisualproblemsassociatedwithdrivingthan controls.ColorperceptiondifficultiesontheFMTwererestrictedtothebluespectruminthe ADHD group.FMTand AQTresults revealed slowerprocessing ofvisualstimuliinthe ADHD group.
Conclusion:Acomprehensiveinvestigationofmechanismsunderlyingvisualfunctionandcolor visioninadultswithADHDiswarranted,alongwiththepotentialimpactofthesevisualproblems ondrivingperformance.
© 2013Spanish GeneralCouncil ofOptometry. Publishedby ElsevierEspaña, S.L.All rights reserved.
PALABRASCLAVE Funciónvisual; AdultosconTDAH; Visióndecolor; TDAH
Funciónvisualyvisióndecolorenadultoscontrastornodedéficitdeatencióncon hiperactividad
Resumen
Objetivo:Seinvestigólavisióndecolorylafunciónvisualenlavidacotidianaauto-reportada delosjóvenesadultoscontrastornodedéficitdeatenciónconhiperactividad(TDAH).
∗Corresponding author at: Human Development & Applied Psychology (Room 9-288), The Ontario Institute for Studies in
Educa-tion/UniversityofToronto,252BloorStreetWest,Toronto,Ontario,CanadaM5S1V6.Tel.:+14169780924;fax:+14169264713.
E-mailaddress:[email protected](R.Tannock).
1888-4296/$–seefrontmatter©2013SpanishGeneralCouncilofOptometry.PublishedbyElsevierEspaña,S.L.Allrightsreserved. http://dx.doi.org/10.1016/j.optom.2013.07.001
VisualfunctioninADHD 23 Método: Participaron30jóvenesadultosconTDAHy30controlesequiparadosporedadysexo. Fueron evaluados individualmente, debiendo completar el ‘‘Vision Activities Questionnaire (VAQ)-CuestionariodeActividadesVisuales,lapruebade100tonalidadesdeFarnsworth-Munsell (FMT)yunapruebarápidadevelocidadcognitiva(AQT).
Resultados: Elgrupo deTDAH reportóunaproporción superior de problemasen 4de las8 áreas delVAQ:percepcióndeprofundidad,visión periférica,búsquedavisualyvelocidadde procesamientovisual.LosanálisisadicionalesdelascuestionesdelVAQrevelaronqueelgrupo deTDAHreflejómásproblemasvisualesasociadosalaconducciónqueelgrupodecontrol.Las dificultadesdepercepcióndelcolorenlapruebaFMTserestringieronalespectrodelazulen elgrupodeTDAH.LosresultadosdeFMTyAQTrevelaronunprocesamientomáslentodelos estímulosvisualesenelgrupodeTDAH.
Conclusión: Estágarantizadaunaampliainvestigaciónsobrelosmecanismossubyacentesdela funciónvisualylavisióndecolorconTDAH,juntoconelimpactopotencialdeestosproblemas visualessobrelaconducción.
©2013Spanish GeneralCouncilofOptometry.Publicado porElsevierEspaña,S.L.Todoslos derechosreservados.
Introduction
Attention-Deficit/Hyperactivity Disorder (ADHD) is one of themostfrequentlydiagnosedchildhoodpsychiatric disor-ders,withworldwideprevalenceratesestimatedat5.3%.1
Alongitudinalstudyshowsthatapproximately65%of chil-drenwithADHDcontinuetoshowsymptomsinadulthood.2,3
WhileadultswithahistoryofADHDmaynotmeetthefull criteria of symptoms listed in the DSM-IV, they continue to exhibit clinically significant symptoms.4 These
contin-ued symptoms are costly to society and the individual.5
For example, ADHD individuals were found to engage in higherriskydrivingbehaviorsandhave morefrequent car crashes.6---10
Current theories posit that executive function deficits accountforpooroutcomesinADHDincludingdriving prob-lems.By contrast, we investigate anovel hypothesis that poor visual function might contribute to some of the negative outcomes. A review of the literature revealed several reports of ophthalmological problems in children with ADHD (see Table 1). For example, numerous studies reportasignificantlyhigherincidenceofADHDamong chil-dren with convergence insufficiency.11---13 The ADHD trait
was also found to be common in children with intermit-tentexotropia.14Variousvisualfunctionandocularfeatures
includingvisualacuity,strabismusandocularmotility,near pointofconvergenceandnearpointofaccommodationwere alsotestedinchildrenwithADHD.15Theauthorsreportthat
children withADHD hada higher frequency of ocular and visual abnormalities,suggesting an early alterationof the developmentof neuralandvasculartissuesincentral ner-vous system. Although Grönlund et al.15 found no effect
of stimulantmedication onvisual function, anotherstudy reported that stimulant treatment seemed to improved visualfieldandbestcorrecteddistancevisualacuityin chil-drenwithADHD.16
Not only have ophthalmological abnormalities been reported among individuals with ADHD, but also so have color perception deficiencies (see Table 2). Specifically, children with ADHD score poorly on clinical tests of blue
colorperception,butnotred-green.17,18Furthermore,
chil-drenwithADHDshowpoorergameperformanceinavirtual environmentwhenimportanton-screeninformationis dis-played predominantly in blue-yellow colors compared to red-green colors.19 Several studies show decreased speed
in color processing in ADHD population.20,21 Notably, the
‘‘retinaldopaminergic’’ hypothesis of color vision22
spec-ulates that a deficiency in central nervous system (CNS) dopamineinADHDmayinduceahypo-dopaminergictonein theretina,whichinturnwouldhavedeleteriouseffectson short-wavelength(‘‘blue’’)cones.Blueconesarevery sen-sitivetodopamine(aswellasotherneurochemicalagents) andrelativelyscarceinnumber,sothatthepurportedlow dopaminergictoneinADHD23 mayaffectblue-yellowcolor
perception.
Numerous studies have reported possible visual defi-ciency including color perception in children with ADHD. However, it is unknown whether adults with ADHD also manifest problems in color vision or whether any visual problemshaveanyfunctionalimpactintheireverydaylife. Accordingly,theaimsofthispreliminarystudywereto inves-tigatevisualfunctionineverydayactivitiesandcolorvision in adults with ADHD. Based on the retinal dopaminergic hypothesis,we hypothesizedthatadultswithADHDwould showaspecificcolordiscriminationproblemwithblue col-ors.
Materials
and
methods
Participants
Thirtyyoungadultswithapreviouslyconfirmeddiagnosisof ADHD(meanageof27years;47%male)andthirtyhealthy controls(meanageof 25years;50%male) participatedin thestudy.ParticipantswithADHDwererecruitedfromtwo sources:astudentpopulationregisteredwithalocal univer-sity’s accessibilities services, which requires documented evidenceofaconfirmeddiagnosis,andanationaladvocacy group for ADHD. In addition to the previously confirmed
S.
Ki
m
et
al.
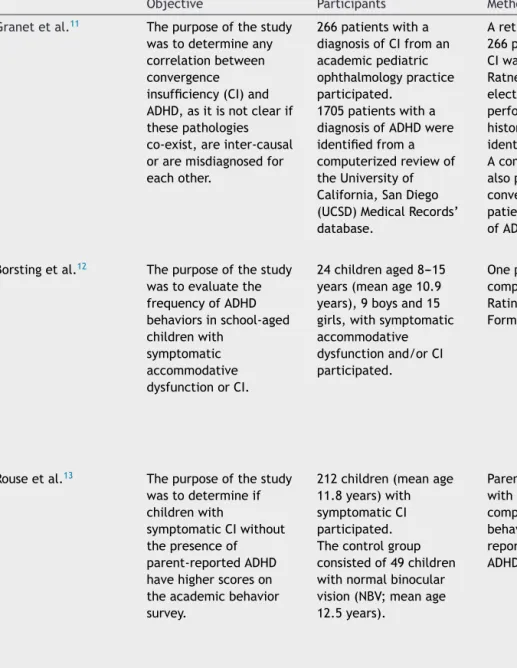
Table1 LiteraturesummaryonvisualfunctioninADHD.
Objective Participants Method Results Conclusions
Granetetal.11 Thepurposeofthestudy
wastodetermineany
correlationbetween convergence insufficiency(CI)and ADHD,asitisnotclearif thesepathologies co-exist,areinter-causal oraremisdiagnosedfor eachother. 266patientswitha diagnosisofCIfroman academicpediatric ophthalmologypractice participated. 1705patientswitha
diagnosisofADHDwere
identifiedfroma
computerizedreviewof
theUniversityof California,SanDiego (UCSD)MedicalRecords’ database.
Aretrospectivereviewofthe 266patientswithadiagnosisof
CIwasobtainedfromtheUCSD
RatnerChildren’sEyeCenter’s electronicdatabasewas performed.Patientswith historyofADHDwere identified.
Acomputerizedreviewwas
alsoperformedlookingatthe converseincidenceofCIin patientscarryingthediagnosis
ofADHD.
Fromthe266chartsof patientswithCI,26 patients(9.8%)hada historyofADHD.Ofthe
patientswithADHDand
CI,20(76.9%)wereon
medicationforADHDat
thetimeofdiagnosisfor CI.
Thereviewofcomputer
recordsshoweda15.9%
incidence(28patients outof1705)ofCIinthe
ADHDpopulation.
Theauthorsreporta three-foldgreater incidenceofADHD amongpatientswithCI
whencomparedwith
incidenceofADHDinthe generalUSpopulation (1.8---3.3%).Theyalso noteaseeming three-foldgreater incidenceofCIinthe ADHDpopulation.
Borstingetal.12 Thepurposeofthestudy
wastoevaluatethe
frequencyofADHD behaviorsinschool-aged childrenwith symptomatic accommodative dysfunctionorCI. 24childrenaged8---15
years(meanage10.9
years),9boysand15 girls,withsymptomatic accommodative dysfunctionand/orCI participated.
Oneparentofeachchild
completedtheConnorsParent
RatingScale-RevisedShort
Form(CPRS-R:S).
OntheCPRS-R:S,
cognitive
problem/inattention, hyperactivity,andADHD indexweresignificantly differentfromnormative values.
Theresultsfromthis preliminarystudy suggest thatschool-aged childrenwith symptomatic accommodative dysfunctionorCIhavea higherfrequencyof ADHD-likebehaviorsas measuredbythe CPRS-R:S.
Rouseetal.13 Thepurposeofthestudy
wastodetermineif childrenwith
symptomaticCIwithout
thepresenceof
parent-reportedADHD
havehigherscoreson
theacademicbehavior
survey.
212children(meanage
11.8years)with
symptomaticCI
participated. Thecontrolgroup consistedof49children withnormalbinocular vision(NBV;meanage 12.5years).
Parents/guardiansofchildren withsymptomaticCIorNBV
completedtheacademic
behaviorsurvey(ABS)and reportedwhetherthechildhad ADHD.
16%oftheCIgroupand 6%oftheNBVgroup
wereclassifiedasADHD
byparentalreport.Total ABSscorefor
symptomaticCIwith parentreportofADHD groupwassignificantly higherthanthe symptomaticCIwith parentreportofno
ADHDgroupandtheNBV
group.
ChildrenwithCIwith parentreportofno
ADHDscored
significantlyhigheron
theABSwhencompared
V isual function in ADHD 25
Grönlundetal.15 Thepurposeofthestudy
wastoinvestigatevisual functionandocular featuresinchildrenwith
ADHDandestablish
whethertreatmentwith
stimulantsisreflectedin functioningofthevisual system.
42childrenand
adolescentswithADHD
aged6.3---17.6years (meanage12years),37 boysand5girls,who werebeingtreatedwith stimulantsparticipated.
Childrenhadbeenon
medicationsforamean
periodof19.5months. Thecontrolgroup consistedof50school children(meanageof 11.9years),44boysand 6girls.
Ophthalmologictestswerefirst
performedwithoutmedication:
-Visualacuity(VA) -Strabismusandocular motility(heterotropia) -Stereoacuity
-Nearpointofconvergence (NPC)
-Newpointofaccommodation
Afterwardsthechildrenwere giventheirregulardrugs.After atleast60min,alltestswere
performedinthesameorder
withmedication.Inaddition, thefollowingtestswere performed:
-Refractionundercyclopegia -Assessmentofocular dimensions
-Examinationofanterior segment,media,andocular fundus
-Photographyoftheocular fundusforquantitativedigital imageanalysis
-Historytakingofvisual perception
76%ofchildrenwith
ADHDhad
ophthalmologicfindings
includingsubnormalVA, strabismus,reduced stereovision,absentor
subnormalNPC,
refractiveerrors,small opticdiscsand/orsigns ofcognitivevisual problems.
Thechildrenhadan increasedproportionof heterophoriaandpoorer performanceonvisual
acuityandconvergence
testswithout,butnot with,stimulantswhen comparedwithcontrols.
ChildrenwithADHDhad
ahigherfrequencyof ocularandvisual abnormalities.
Treatmentwith
stimulantscausedno significantdifferencein visualfunction.They presentedsubtle
morphologicalchanges
oftheopticnerveand retinalvasculature, indicatinganearly disturbanceofthe
developmentofneural
andvasculartissuesin theCNS.
S. Ki m et al. Table1(Continued)
Objective Participants Method Results Conclusions
Martinetal.16 Thepurposeofthisstudy
wastoevaluatevisual functioninchildrenwith ADHD,tocorrelatethese datawiththe
morphologyoftheoptic nerve,andtofindoutif
andhowpsychostimulant
medicationaffectsvisual functions.
18childrenaged6---17
years(meanage11.9
years),16boysand2 girls,diagnosedwith
ADHDandtreatedwith
stimulantsparticipated.
Childrenhadbeenon
medicationforamean periodof14.7months.
ADHDdiagnoseswere
determinedaccordingto DSM-IVcriteriabyone physicianinallpatients. Thecontrolgroup consistedof24children aged7---18years(mean age11.7years),15boys and9girls.
Bothgroupsunderwentan
ophthalmologicalexamination includingbestcorrected distancevisualacuity(BCVA), visualfieldexamination,and fundusphotography.
TheADHDchildrendidnottake medicationonthemorningof theinitialexamination.Two hourslater,thechildrenwere giventheirregulardrugdoses
andtheexaminationswere
repeated.Thecontrolgroup wasexaminedtwice,atthe sametimeintervalsasthe
ADHDgroup.
Visualacuityincreased significantlyintheADHD groupaftertreatment.
Thedifferencebetween
thetwoVFexaminations wassignificantlylarger
intheADHDcompared
withthecontrolgroup.
SignificantlymoreADHD
subjectshadsubnormal
VFresultswithout
stimulants,compared
withcontrols,butwith stimulantsthe
differencewasnolonger significant.
ChildrenwithADHD
showedbetterVAandVF
resultswiththanwithout psychostimulant
medication.
Chungetal.14 Thepurposeofthestudy
wastoinvestigatethe
symptomsofADHDas reportedbyparentsin childrenwith intermittentexotropia [X(T)]andtodetermine whetherstrabismus
surgeryforX(T)affects
ADHDsymptoms.
51childrenundergoing musclesurgeryforX(T) aged3---9years(mean age5.96years),22boys and29girls,
participated.Allpatients hadeitherdivergence excessorbasictype X(T).
Oneparentofeachchild
completedtheADHDrating
scaleIV(ADHDRS-IV) assessment,basedonthe
DSM-IVhomeversion,
consecutivelybeforeandone yearaftersurgery(symmetric lateralrectusrecessionon botheyes).
8(15.7%)ofthe51 patientsdemonstrated
theADHDtrait.ADHD
RS-IVscoresfollowing strabismussurgery significantlydecreased inpatientswiththe ADHDtrait,whilethey didnotdifferinpatients withouttheADHDtrait. 7ofthe8patientswith theADHDtraitshowed improvementintheir ADHDRS-IVscoresafter surgery.
TheADHDtraitwas
relativelycommonin childrenwithX(T),and theparent-reported
symptomsofthe
childrenwiththeADHD traitimprovedafter strabismussurgery.
V isual function in ADHD 27
Table2 LiteraturesummaryoncolorvisioninADHD.
Objective Participants Method Results Conclusions
Tannocketal.20 Thepurposeofthe
studywasto investigaterapid
automatizednaming
(RAN)andeffectsof stimulantmedication inschool-agechildren
withADHDwithand
withoutconcurrent readingdisorder(RD)
67childrenwithADHD, 21withADHD+RD,and 27healthycomparison childrenparticipated.All
childrenwerebetween7
and12yearsofage,80% ofwhichweremale. Inasecondstudy,a subgroup(n=47)ofthe
totalADHDsample
participatedinanacute medicationtrial,35 belongingtotheADHD group,12tothe
ADHD+RDgroup.
Thethreegroupswere
comparedon:colornaming
speed,letternamingspeed,
phonologicdecoding,and
arithmeticcomputation. Inthemedicationtrial,the subgroupofchildren
completedseveralacademic
andcognitivemeasuresaswell asthreeoftheRANTests: Colors,Letters,andDigits. Eachchildcompleteda randomized,
placebo-controlled,cross-over trialwiththreesingledoses (10,15,20mg)of
methylphenidate.Theactive
medicationandplacebowere
administeredinadouble-blind
mannereachmorningduringa
1-weekperiod.Testingunder double-blindconditions
commencedabout1hafter
ingestionofmedicationand lastedfor2h.
BothADHDgroupswere
significantlyslowerincolor namingthancontrols,butdid notdifferfromoneanother, showingevidenceofan associationbetweendeficitsin
colornamingandADHDthat
couldnotbeattributedtothe comorbiditywithRD.
Methylphenidateselectively
improvedcolor-namingspeed
buthadnoeffectonthespeed ofnaminglettersordigits.
Thefindingsofcolor
namingimpairmentsin
ADHDchallengethe
currentassumptionthat
namingspeeddeficits
arespecifictoRDand alsoprovidesome supportforthe purportedprocessing differencesunderlying colornamingandletter
naming,ofwhich
color-namingspeedis improvedbystimulant medication.
Lawrenceetal.21 Thepurposeofthe
studywastocompare
children’s performanceonboth neuropsychological andreal-life measuresof executivefunction andprocessingspeed.
44boysaged6---12years (meanage9.7years),22 withadiagnosisofADHD and22controls, participated.
Participantscompletedthe StroopColor---WordTestand WisconsinCardSortingTask
(WCST),whichwereselected
asneuropsychological measures,aswellasroute tasksinavideogameandat thezoo,whichwereusedto indexreal-lifemeasures.
Therewerenogroup
differencesinexecutive functionontheStrooporzoo tasks,buttheADHDgroup exhibiteddeficitsin
set-shiftingasassessedbythe WCST(preservativeerrorsand
responses)andvideogameplay
(fewerchallengescompleted.
TheADHDgroupwas
significantlyslowerincolor namingontheStroop,andalso tookmoretrialsontheWCST tocompletesortingcards accordingtothefirstcategory ofcolor.
Thereisgrowing evidenceofcolornaming andcolorprocessing deficitsinchildren, adolescents,andadults
S. Ki m et al. Table2(Continued)
Objective Participants Method Results Conclusions
Banaschewskietal.17 Thepurposeofthe
studywasto investigatecolor perceptionin childrenwithADHD, aswellasthe relationshipbetween colorperceptionand
performanceona
conventional neuropsychological task(StroopTask) thatrequiresspeeded namingofcolored stimuli.
27childrenaged 8.0---13.0years, consistingof14children
withADHDand13
controls,participated.
Colordiscriminationabilitywas investigatedusingthe
Farnsworth-Munsell100Hue Test(FMT).Colorvision abnormalitiesandaptitude weredeterminedbytheability ofthechildtoplacethecolor capsinorderofhue.
Childrencompletedthe
Stroop-Color---WordTask.
Namingtimeanderrorswere
recordedforthreesubtests separately:Stroop-Word, Stroop-Color,and
Stroop-Color/Word.A
nominationscorewas
calculatedintermsofthe differenceinreactiontimesof readingofcolorwordsand colornaming.
ChildrenwithADHDwere
slowerinnamingthecolorsof stimulionboththeColorand Color---Wordconditionsofthe Stroop,butdidnotdifferin
namingspeedontheWord
condition,norinStroop interference.Thisdeficitwas accountedforsimilarlyby blue-yellowandred-green discriminationabilities.
Thesefindingsindicate subtleproblemsinthe
blue-yellowmechanism
andchangesinretinal dopaminergic
mechanismsinchildren
withADHD.However,
performancedeficitson
Stroopcolornaming seemnottobefully attributabletocolor visionimpairment.
Roessneretal.18 Thepurposeofthe
studyistoexamine colorperceptionin
ADHDandChronicTic
Disorders(CTD)to clarifywhichfactor
(ADHDversusCTD)
influencescolorvision parametersespecially inthecaseofthe comorbidityof ADHD+CTD. 69childrenaged 8.0---12.6years,14with adiagnosisofADHD,22 withCTD,19with ADHD+CTD,14healthy controls.
Colordiscriminationabilitywas investigatedusingthe
Farnsworth-Munsell100Hue Test(FMT).Colorvision abnormalitiesandaptitude weredeterminedbytheability ofthechildtoplacethecolor capsinorderofhue.
Participantsalsocompleted theStroop-Color---WordTask.
Namingtimeanderrorswere
recordedforthreesubtests separately:Stroop-Word, Stroop-Color,and Stroop-Color/Word.
Colorperceptiondeficits,as
indexedbytheFMT,were
foundforbothmainfactors
(ADHDandCTD),butthere
werenointeractioneffects.A preponderanceofdeficitson
theblue-yellowcomparedto
thered-greenaxiswas
detectedforADHD.
IntheStrooptaskonlythe
‘pure’ADHDgroupshowed
impairmentsininterference controlandotherparameters ofStroopperformance. Nosignificantcorrelations
betweenanyFMTvariableand
colornamingintheStrooptask
werefound.
Basiccolorperception deficitsinbothADHD andCTDcouldbefound, andthesedeficitsare additiveinthecaseof comorbidity
(ADHD+CTD).
Performancedeficitson
theStrooptaskwere presentonlyinthe
‘pure’ADHDgroup.
Hence,thelattermaybe
compensatedinthe
comorbidgroupbygood
prefrontalcapabilitiesof
CTD.Theinfluenceof
colorperceptiondeficits onStrooptask
performancemightbe
V isual function in ADHD 29
SilvaandFrère19 Thepurposeofthe
studywastoexamine
blue-yellowcolor discriminationin ADHDindividuals usingavirtual environmentthatis capableof quantifyingthe influenceof red-greenversus blue-yellowcolor stimulionparticipant performance. 40volunteersaged 15---25years,17menand 23women,consistingof
20non-ADHDvolunteers
and20volunteerswith
ADHDparticipated.
Aninteractivecomputergame
basedonvirtualrealitywas developedtoevaluatethe performanceoftheplayers. Withinthegame,theplayer mustfindandinterprethints scatteredindifferent
scenarios.Inoneversion,hints
andinformationboardswere
paintedusingredandgreen colors.Inthesecondversion, theseobjectswerepainted usingblueandyellowcolors.
TheADHDgroupandcontrol
groupweredividedinto subgroupswhichplayedeither thered-greenversionorthe yellow-blueversion.Thetime spenttocompleteeachtaskof
thegamewasmeasured.
Useofblue/yellowinsteadof green/redcolorsdecreasedthe gameperformanceofall participants.However,a greaterdecreasein
performancecouldbeobserved
withADHDparticipantswhere tasks,thatrequireattention, weremostaffected.
Colorsaffectthe performanceoftasks thatsimulatedaily activitiesrequiring attentionintheADHD population.
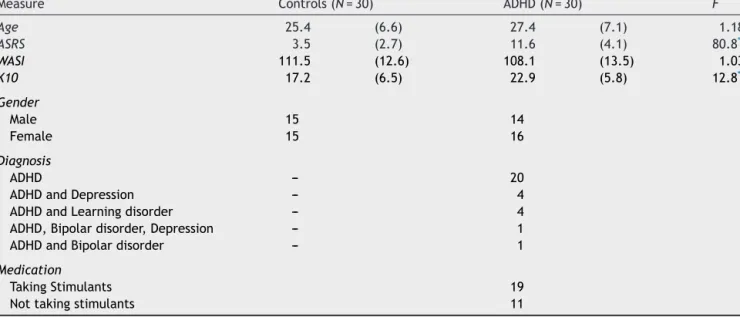
Table3 DemographicandclinicalcharacteristicsofparticipantswithADHDandcontrols.
Measure Controls(N=30) ADHD(N=30) F
Age 25.4 (6.6) 27.4 (7.1) 1.18 ASRS 3.5 (2.7) 11.6 (4.1) 80.8** WASI 111.5 (12.6) 108.1 (13.5) 1.03 K10 17.2 (6.5) 22.9 (5.8) 12.8* Gender Male 15 14 Female 15 16 Diagnosis ADHD --- 20
ADHDandDepression --- 4
ADHDandLearningdisorder --- 4
ADHD,Bipolardisorder,Depression --- 1
ADHDandBipolardisorder --- 1
Medication
TakingStimulants 19
Nottakingstimulants 11
Note.Standarddeviationsappearinparenthesesbesidemeans. * p≤0.05.
**p≤0.001.
diagnosisofADHD,currentsymptomsofADHDwerechecked using the Adult ADHD Self-Report Scale (ASRS24).
Partici-pantswereaskedtoreportanycomorbiddisorders.Control participants were recruited through the same local uni-versity and community advertisements. Participants were excludediftheyhadbelowaverageintellectualfunctioning (below80in WASI-II),anyknowngeneticvision problems, impaired visual acuity as measured by the Snellen eye chart(despitecorrectedvision),orcurrenttreatmentofa severe psychiatricdisorder other than ADHD. Participants withADHD who were being treated with stimulant medi-cation (n=19; 63%) wererequested to stop anystimulant medicationforatleast12hpriortothestudy(Table3).
Materialsandmethod
ThestudywasapprovedbytheInstitutionalResearchEthics Boardandallparticipantsprovidedwritten informed con-sentpriortothetesting.
Adult ADHD Self-Report Scale (ASRSv1.124): The ASRS
wasadministered to assess current ADHD symptoms. The ASRSisaninstrumentconsistingofeighteenquestionsbased onthecriteriausedfordiagnosingADHDintheDSM-IV-TR. Scoresforeachitemwereaddedtocalculateatotalscore. TheASRSisareliableandvalidscaleforevaluatingADHDin adults.25 Ithashighinternalconsistency(Cronbach’salpha
0.88and0.89,forbothpatientandrater-administered ver-sions, respectively) and high concurrent validity withthe rater-administeredADHDRatingScale.
WechslerAbbreviatedScaleofIntelligenceII(WASI-II26):
ScoresfromboththeVocabularyandMatrixReasoningtasks weresummedtogiveanestimatedIQscore.
KesslerPsychologicalDistressScale(K1027):TheK-10was
usedtoexaminerecentemotionaldistress.TheK10isa 10-itemquestionnaire based on questions about anxiety and
depressivesymptomsthatapersonhasexperiencedinthe mostrecent4-weekperiod.Scoresforeachitemwereadded tocalculateaglobalmeasureofdistress.
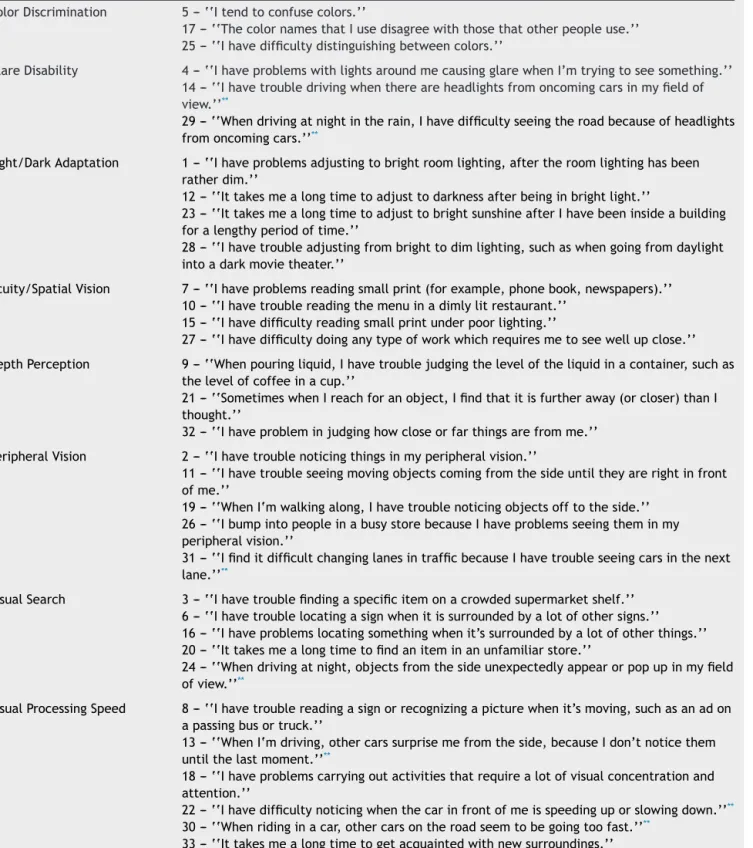
Visual Activities Questionnaire (VAQ28): The VAQ was
conducted to assess perceived visual function in ordinary activities. The VAQ is a self-report questionnaire consist-ing of 33 items thatare behaviourally basedin that they refertoactualvisualactivitiesandtasks.These33itemsfall intoeightareasthatareknowntobeimportantincarrying outvisual activities:Colordiscrimination,Glaredisability, Light/Darkadaptation,Acuity/Spatialvision,Depth percep-tion,Peripheralvision,Visualsearch,andVisualprocessing speed. For the purpose of this study,items pertainingto driving were extracted fromthe various categories to be examined separately in a post hoc analysis.The items of eachcategoryarelistedinTable4.Participantsresponded by selecting one of the following options: never, rarely, sometimes,oftenandalways,whichwerecodedfrom1to5, respectively.Thesumscoreforeachsubscalewasusedfor analysis;thesumscoreofallitemspertainingtodrivingwere alsocomputedandanalyzed.TheVAQisareliableandvalid scaleforevaluatingvisualdifficulties.28Itisconsideredtobe
anefficientmeasureforcurrentvisualfunctionindisorders such as glaucoma29 and cataracts, and for self-perceived
visualdifficultiesrelatedtoadverseoutcomessuchasa vehi-clecrashorafall.28Inaddition,scoresoncertainsubscales
suchasperipheralvisionhavebeenassociatedwithgreater visualfieldloss.30
ColorVisionScreeningInventory(CVSI31):A10-item
self-report behavioral inventory was used toassess perceived color vision ability. This brief screening inventory is a behaviourally validated instrument that can classify indi-vidualsbasedontheircolorvisionperception.Participants respondedbyselectingoneofthefollowingoptions:never, seldom, occasionally, frequently and always, which were coded from 1 to 5, respectively. The established cut-off
VisualfunctioninADHD 31 valueis17.Sevenoutof10questionsaskiftheparticipant
have difficulty discriminating between certaincolors (i.e. betweenredandbrown),andtheotheritemsinquirescolor namingdifficultyingeneral.
Farnsworth-Munsell 100 Hue Test (FMT32): The FMT
was used to provide an objective assessment of color
discriminationability.TheFMTisawidelyusedcolorvision testthatrequiresparticipantstosequencecolorreference caps in order of incremental hue variation spanning the visiblespectrum.Theerrorscoresreflectthenumberof mis-placements.Errorscoreswerecomputedseparatelyforthe blue,yellow,red,andgreenspectra.Totaltimetocomplete
Table4 ItemsofVisualActivitiesQuestionnairepercategories. ColorDiscrimination 5---‘‘Itendtoconfusecolors.’’
17---‘‘ThecolornamesthatIusedisagreewiththosethatotherpeopleuse.’’ 25---‘‘Ihavedifficultydistinguishingbetweencolors.’’
GlareDisability 4--- ‘‘IhaveproblemswithlightsaroundmecausingglarewhenI’mtryingtoseesomething.’’ 14---‘‘Ihavetroubledrivingwhenthereareheadlightsfromoncomingcarsinmyfieldof view.’’**
29---‘‘Whendrivingatnightintherain,Ihavedifficultyseeingtheroadbecauseofheadlights fromoncomingcars.’’**
Light/DarkAdaptation 1---‘‘Ihaveproblemsadjustingtobrightroomlighting,aftertheroomlightinghasbeen ratherdim.’’
12---‘‘Ittakesmealongtimetoadjusttodarknessafterbeinginbrightlight.’’
23---‘‘IttakesmealongtimetoadjusttobrightsunshineafterIhavebeeninsideabuilding foralengthyperiodoftime.’’
28---‘‘Ihavetroubleadjustingfrombrighttodimlighting,suchaswhengoingfromdaylight intoadarkmovietheater.’’
Acuity/SpatialVision 7---‘‘Ihaveproblemsreadingsmallprint(forexample,phonebook,newspapers).’’ 10---‘‘Ihavetroublereadingthemenuinadimlylitrestaurant.’’
15---‘‘Ihavedifficultyreadingsmallprintunderpoorlighting.’’
27---‘‘Ihavedifficultydoinganytypeofworkwhichrequiresmetoseewellupclose.’’ DepthPerception 9---‘‘Whenpouringliquid,Ihavetroublejudgingtheleveloftheliquidinacontainer,suchas
thelevelofcoffeeinacup.’’
21---‘‘SometimeswhenIreachforanobject,Ifindthatitisfurtheraway(orcloser)thanI thought.’’
32--- ‘‘Ihaveprobleminjudginghowcloseorfarthingsarefromme.’’ PeripheralVision 2---‘‘Ihavetroublenoticingthingsinmyperipheralvision.’’
11---‘‘Ihavetroubleseeingmovingobjectscomingfromthesideuntiltheyarerightinfront ofme.’’
19---‘‘WhenI‘mwalkingalong,Ihavetroublenoticingobjectsofftotheside.’’ 26---‘‘IbumpintopeopleinabusystorebecauseIhaveproblemsseeingtheminmy peripheralvision.’’
31---‘‘IfinditdifficultchanginglanesintrafficbecauseIhavetroubleseeingcarsinthenext lane.’’**
VisualSearch 3---‘‘Ihavetroublefindingaspecificitemonacrowdedsupermarketshelf.’’ 6---‘‘Ihavetroublelocatingasignwhenitissurroundedbyalotofothersigns.’’ 16---‘‘Ihaveproblemslocatingsomethingwhenit’ssurroundedbyalotofotherthings.’’ 20---‘‘Ittakesmealongtimetofindaniteminanunfamiliarstore.’’
24---‘‘Whendrivingatnight,objectsfromthesideunexpectedlyappearorpopupinmyfield ofview.’’**
VisualProcessingSpeed 8---‘‘Ihavetroublereadingasignorrecognizingapicturewhenit’smoving,suchasanadon apassingbusortruck.’’
13---‘‘WhenI‘mdriving,othercarssurprisemefromtheside,becauseIdon’tnoticethem untilthelastmoment.’’**
18---‘‘Ihaveproblemscarryingoutactivitiesthatrequirealotofvisualconcentrationand attention.’’
22---‘‘Ihavedifficultynoticingwhenthecarinfrontofmeisspeedinguporslowingdown.’’**
30---‘‘Whenridinginacar,othercarsontheroadseemtobegoingtoofast.’’**
33---‘‘Ittakesmealongtimetogetacquaintedwithnewsurroundings.’’ ** VAQitemspertainingtovisionanddriving.
theFMTwasalsorecordedtoprovideanindexofthespeed or efficiency of color discrimination. All testing was per-formed understandard light conditions in the sameroom andatthesameplace.Theilluminancewasmaintainedat D65daylight,6500K.
A Quick Test of Cognitive Speed (AQT33): The AQT, a
variantofrapidautomatizednaming,wasusedtomeasure speededcolorprocessing.Otherthanspeedednaming abil-ity,AQTisusedtomeasurerapidcognitiveshiftsbetween visual stimuli and working memory. The AQT consists of threemaintasks,eachcomprisedofthreesubtests.InTask A, participants were first required to name color (color-naming: black, yellow, red, and blue), followed by form (form-naming:circle,line,triangle,andsquare),andlastly, acolor---formcombinationinwhichparticipantsnamedthe color followed by the form (i.e. blue circle). In Task B, theparticipanthastonamecolor,number(number-naming: numbers 1---9), and a color---number combination. In Task C, participants are required to name color, letter, and a color---letter combination. Each subtest is presented on a singlepagewith8rowscomprisedof5items.Participants areinstructed to name all 40 items as fast and as accu-ratelyastheycan.Namingtimeanderrorswererecorded and combined across each task to give six overall varia-bles:color-naming,form/number/letter-naming,andcolor andform/number/letter-namingintermsofbotherrorand speed.AQT has shown high test-retest reliability(r=0.91 to 0.95) and discriminates individuals with ADHD from controls.33
Results
Demographics
Thetwogroupsdidnotdifferinage,sex,IQ(seeTable3). The visual acuity (corrected eye sight) measured with a Snellen chart were within normal range (20/20) in both groupsanddidnotdiffersignificantlybetweenthegroups. Asexpected,ADHDparticipantsreportedsignificantlymore symptoms on the ASRS than the comparison group [F(1, 58)=80.8,p<001],aswellashigheremotionaldistressas measuredusingtheK10[F(1,58)=12.8,p<001].Nosex dif-ferencesamongvariablesbetweenthegroupswerefound.
Visualfunctioning
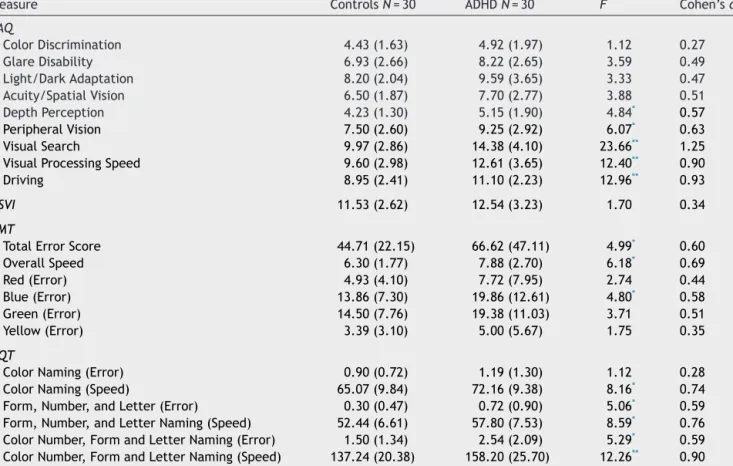
IndividualswithADHDreportedmorevisualdifficultiesthan thecomparisongroupontheVAQ(groupmeansandstandard deviations of scores on the various subscales are shown in Table 5). A one-way multivariate analysis of variance (MANOVA)wasconductedtodeterminetheeffectofgroup (ADHDparticipantsversushealthycontrols)onself-reported VAQitems.Significantgroupdifferenceswerefoundonthe VAQ, Wilks’s =0.629, F(9, 51)=3.34, p=0.0028, multi-variate 2 based onWilks’s =0.37. Analysis of variance (ANOVA) was conducted on the eight subcategories to followupthesignificantresult.Specifically,theADHDgroup reported more problems in depth perception (M=5.15, 95% CI [4.57, 5.74]) than the control group (M=4.23, 95% CI [3.64, 4.83]), p=0.032. Also, the ADHD partici-pants(M=9.25,95%CI[8.25,10.24])hadsignificantlymore
visual difficulty with peripheral vision than healthy con-trols(M=7.50,95%CI[6.50,8.51]),p=0.017.Inaddition, individuals with ADHD (M=14.38, 95% CI [13.11, 15.65]) self-reportedmoreproblemsinvisualsearchthanthe com-parisongroup(M=9.97,95%CI[8.67,11.26]),p<001.Lastly, theADHDgroup(M=12.61,95%CI[11.41,13.81])endorsed significantly more difficulties with VAQ items related to visualprocessingspeedthancontrols(M=9.60,95%CI[8.38, 10.82]),p<0.001.PosthocanalysisoftheVAQitemsrelated todrivingrevealedasignificantmaineffectof‘group’, indi-catingthatparticipantswithADHD(M=11.10,95%CI[10.26, 11.93]) reportedmore visual problemswhen driving com-paredtocontrols(M=8.95,95%CI[8.10,9.80]),p<0.001.
Colorvision
Aone-wayMANOVAyieldednomaineffectofgrouponthe fourcolordiscriminationerrorscores,Wilks’s=0.908,F(4, 52)=1.32,p=0.27(seeTable5).Totestforapriori hypoth-esis of blue-color perception problems, we proceeded to perform one-wayANOVAs for each color spectrum on the FMTerror scores.IndividualswithADHD(M=19.86,95%CI [16.01,23.72])committedmoreerrorsonlywhen discrimi-natingbluespectrumcolorsandnotinothercolorssuchas redorgreencomparedtonormalcontrols(M=13.86,95%CI [9.94,17.78]),p=0.033. Analysisof thetimetocomplete the FMT also revealed slower color discrimination in the ADHD group(M=7.88,95% CI[6.76,8.99]) relativetothe comparisongroup(M=6.30,95%CI[5.58,7.01]),p=0.016.
Visualperceptualspeed
Aone-wayMANOVAyieldedamaineffectgrouponAQT nam-ing time, Wilks’s=0.767, F(6, 53)=2.69, p=0.024. The multivariate2 basedonWilks’swas0.23.Resultsfrom follow-upANOVAtestsindicatedthatparticipantswithADHD weresignificantlyslowerinallthreenamingtasksthan con-trolgroup(seeTable5).Intermsofaccuracyscores,ADHD participantsmademoreerrorsthanthehealthycontrolsin form/number/letter-naming(alsoseeTable5).
Interrelationshipamongstvisualfunctioning,color vision,andADHDsymptoms
To determine whether ADHD symptoms were related to visual problems, Pearson correlations were calculated between the ASRS scores and those for the five VAQ subscales impaired in ADHD. Significant correlations were found between ASRS and peripheral vision [r(58)=0.320, p=0.013],visualsearch[r(58)=0.492,p<0.001],andvisual processing [r(58)=0.315, p=0.014]. Although there were no group differences in the CVSI, correlational analyses revealed a significant positive correlation betweenscores on the CVSI and those on the VAQ color discrimination scale for both groups: ADHD: r(27)=0.82, p<0.001; Con-trol:r(28)=0.78, p<0.001.Also,in the ADHDgroup, CVSI scores correlatedwithVAQdepthperception [r(27)=0.48, p=008]. Inthecontrol group,CVSIscores correlatedwith glare disability [r(28)=0.47, p=0.008] and acuity/spatial vision[r(28)=0.44,p=014].
VisualfunctioninADHD 33 Table5 VisionandcolorvisionquestionnaireandcolorvisiontestsANOVAresults.
Measure ControlsN=30 ADHDN=30 F Cohen’sd
VAQ ColorDiscrimination 4.43(1.63) 4.92(1.97) 1.12 0.27 GlareDisability 6.93(2.66) 8.22(2.65) 3.59 0.49 Light/DarkAdaptation 8.20(2.04) 9.59(3.65) 3.33 0.47 Acuity/SpatialVision 6.50(1.87) 7.70(2.77) 3.88 0.51 DepthPerception 4.23(1.30) 5.15(1.90) 4.84* 0.57 PeripheralVision 7.50(2.60) 9.25(2.92) 6.07* 0.63 VisualSearch 9.97(2.86) 14.38(4.10) 23.66** 1.25
VisualProcessingSpeed 9.60(2.98) 12.61(3.65) 12.40** 0.90
Driving 8.95(2.41) 11.10(2.23) 12.96** 0.93
CSVI 11.53(2.62) 12.54(3.23) 1.70 0.34
FMT
TotalErrorScore 44.71(22.15) 66.62(47.11) 4.99* 0.60
OverallSpeed 6.30(1.77) 7.88(2.70) 6.18* 0.69 Red(Error) 4.93(4.10) 7.72(7.95) 2.74 0.44 Blue(Error) 13.86(7.30) 19.86(12.61) 4.80* 0.58 Green(Error) 14.50(7.76) 19.38(11.03) 3.71 0.51 Yellow(Error) 3.39(3.10) 5.00(5.67) 1.75 0.35 AQT
ColorNaming(Error) 0.90(0.72) 1.19(1.30) 1.12 0.28
ColorNaming(Speed) 65.07(9.84) 72.16(9.38) 8.16* 0.74
Form,Number,andLetter(Error) 0.30(0.47) 0.72(0.90) 5.06* 0.59
Form,Number,andLetterNaming(Speed) 52.44(6.61) 57.80(7.53) 8.59* 0.76
ColorNumber,FormandLetterNaming(Error) 1.50(1.34) 2.54(2.09) 5.29* 0.59
ColorNumber,FormandLetterNaming(Speed) 137.24(20.38) 158.20(25.70) 12.26** 0.90
VAQ=VisualActivitiesQuestionnaire;CVSI=ColorVisionScreeningInventory;FMT=Farnsworth-Munsell100Hue;MRM=Mollon-Reffin Minimalist;AQT=AQuickTestofCognitiveSpeed.
Note.Standarddeviationsappearinparenthesesbesidemeans. * p≤0.05
** p≤0.001.
Discussion
Thisstudy providesthefirstevidenceofcolorvision prob-lemsandfunctionalvisualimpairmentsinadultswithADHD. Specifically,youngadultswithADHDexhibitedsignificantly morevisualdifficulties,asindicated byself-report onfour outofeightareasineverydayvisualactivities.Moreover,the ADHDgroupreportedmorevisualdifficultieswhendriving. Alsoadults with ADHD exhibitedspecific problems in dis-criminatingcolorsalongthebluespectrum,asindicatedby theirperformanceontheFMT,aswellaslessefficientcolor discriminationandoverallvisualprocessing,asindexedby thelongertimetakentocompletetheFMTandAQTscores, respectively.
In our study, ADHD individuals reported that they perceived significantly more difficulties compared to the controlgroupinthefollowingareasontheVAQ:depth per-ception,peripheralvision,visualsearch,visualprocessing, and items related to driving. Also, in the ADHD group self-ratingofADHDsymptomsontheASRScorrelated signif-icantlywithVAQsubscalessuchasperipheralvision,visual search andvisual processingspeed, suggesting that these visualdifficultiesmayberelatedtobehavioralsymptomsof inattention.However,thoseVAQitemspertainingtovisual
difficulties associated with driving did not correlate with ASRSscores. Previous studies have reported driving prob-lemsincludingriskydrivingbehaviorandvehiclecollisions inadultswithADHD.6,7OurfindingsontheVAQ, whichare
basedonself-reportedproblemsinvisualfunctionin every-daylife,suggest thatvisualproblemsreportedinprevious studies may have functional consequences in real world activitiesincludingdriving.Consideringthatvisual percep-tionis knownto beone of the most importantfactors in driving,ourfindingswarrantsfurtherinvestigationto delin-eateunderlyingmechanismsofvisualdifficultiesinADHDas wellasthelinkbetweenvision,attentionanddriving.34,35
Intermsofcolorperception,ourfindingofimpairedFMT performanceforthebluespectruminadultswithADHD,isin linewithfindingsfrompreviousstudiesusingtheFMTwith childrenwith ADHD17,18 (see Table 1).Notably,no
impair-mentswerefoundfor theredorgreenspectra,suggesting thatthedifficultywithbluecannotsimplybeattributable toproblems withsustainedattention: thelatterwouldbe expectedtohaveanimpactonFMTperformanceacrossall of the colors.But howare we to accountfor the finding thatthehuediscriminationproblemswererestrictedtothe bluespectrumanddidnotinclude problemswiththe yel-low spectrum? According to opponent color theory,36 the
blue and yellow visual system may be coupled and show similaroutcomeinvisualfunctions. However,analternate modelofcolorvision,Dual-ProcessTheory37 proposedthat
thevisualsystemiscomprisedoftwostages.Thefirststage canbeconsideredasthereceptorstage,where thethree retinalphotoreceptors(S,MandLcones)traducephysical stimuliintoneuralsignals.Inthesecond stage,theneural signalsfromconesarecombinedtocreate twochromatic mechanisms:L---M and S---(L+M). The S---(L+M) mechanism combinespositiveinputsfromSconesandnegativeinputs fromthe sum of L and M conesignals which lead toour perceptionof blueandyellow.Notably,deficiency in cen-tralnervoussystem(CNS)dopamineinADHDmayinducea hypo-dopaminergictoneintheretina,whichinturnwould havedeleteriouseffectsonshort-wavelengthcones. There-fore,wemayspeculatethatthisdopaminergiceffectmay have an impactonS-cones inthe receptor stage,leaving yellowperception, which is a product of LM conesin the receptorlevelintact.Anotherpossibility,albeitspeculation, isthattheobserved‘blue-colorproblem’inADHDreflects an alteration in an opsin/vitamin-A-based photopigment, calledmelanopsin,whichismaximallysensitivetobluelight andlinkedwithregulation ofcircadianrhythms:38,39
circa-diansystemsareimpairedinADHD.40
Furthermore,highcorrelationsbetweenCVSIscoreand several categories in VAQ imply possible impact of color visionindailyvisualactivities.Likewise,evidenceofacolor perceptiondeficit is important giventhe extensiveuse of colorindailylifeandtheuseofcolorstimuliinmanyofthe standardneuropsychologicaltestsusedintheassessmentfor ADHD(e.g.color---wordStrooptest,WisconsinCardSorting Task).Forexample,onepreviousstudyreportedan intrigu-ingrelationshipbetweenperformanceontheWisconsinCard Sorting Task (number of trials tocomplete the first cate-gory,whichiscolor)andcolor namingontheStroop.Both tasksinvolve a high proportionof blue stimuli.21 Findings
forcolorvisionwerenotcompletelyconsistentinthisstudy. Forinstance,self-reportssuchastheCVSIandthecolor dis-criminationvariableontheVAQdidnotindicateanygroup differencesinperceived colorvisionwhiletheFMTresults showedsignificantgroupdifferencesonthebluespectrum. Thisseeminglyinconsistentfindingwithself-reported ques-tionnairessuggeststhatcolorperceptiondeficiencymaybe specifictobluecolors,assuggestedbytheretinal dopami-nergichypothesis.
Finally,wefoundthattheADHDpopulationwere signif-icantlyslower in naming speed than the control group in allsubscalesoftheAQT:colornaming,form/number/letter naming and color---form/color---number/color---letter nam-ing. Individuals withADHD were also generallyslower on thecolordiscriminationtask(FMT)thanthecontrolgroup. Furthermore,ADHDindividualscommittedmoreerrorsthan controlsexceptforthecolornamingsubscale.Thisfinding issomewhatinconsistent withprevious studiesthat found differencesincolornaming speed.17,20 Oneimportant
fac-tortoconsiderwhenevaluatingthefindingsfromtheAQT is that the AQT differs significantly from the Stroop test inthat theAQT tasksmeasure generalcognitive and per-ceptualprocessingspeed41 whereastheStroopcolor---word
test is believed tobea classic executive functiontest. A study using regional cerebral blood flow has shown that during color---form naming task, brain activation in the
parietalareaisincreasedandactivationsinfronto-temporal regionsaredecreased,whichindicatesthatthecolor---form test may requiremore perceptual processing than execu-tive functions.42 Along with slower naming speed in FMT,
thisfurtherreinforcestheideathatindividualswithADHD experiencedifficultiesinvisualprocessingefficiency.
Thereare several limitations in thispreliminary study. Firstofall,thesamplesizeisrelativelysmallandinvolvesa largeproportionofcollegestudentswhichmakesitdifficult to generalize the results to the entire ADHD adult popu-lation.We acknowledge that thispreliminary study needs to be replicated with a larger, clinical sample for find-ingstobegeneralizabletotheADHDpopulation.However, based on the effect sizes on the visual and color vision measures of this study that range frommedium to large, the sample providedsufficient statisticalpower todetect groupdifferences.43Secondly,ADHDdiagnosisinthisstudy
wasdeterminedbypreviousdocumentationofdiagnosisand comorbiditieswereself-reportedbytheparticipantsinstead of a comprehensive diagnosticprocedure. Another limita-tionisthatvisualfunctionproblemsindailylifeweremainly analyzed with a self-report measure which might entail information bias. Subsequent studies should use a more objectivemeasureofvisualfunctionproblems ineveryday life. In addition, the limitation of using the FMT is that itrequires theparticipanttoarrangethecapsinthebest colororder(i.e.fromyellowishgreentoturquoisegreen). This process involves both accurate movement execution and sustainedattention, whichare knowntobeimpaired in ADHD. Future studies might want togive greater con-sideration to the choice of color perception tests and to incorporateotherapproachestodisaggregatevisual atten-tion andcolor vision. Perhaps display basedtests suchas Color Assessment and Diagnosis (CADs) should be used in futurestudiestoinvestigatingRGandYBchromatic sensi-tivitymoreaccurately.
Notwithstandingthestudylimitations,thisstudy repre-sentsthefirstattempttoinvestigatetheperceiveddifficulty in dailyvisual activities,andtotest whethera previously reportedprobleminbluecolorperceptioninchildrenwith ADHD also manifests in adults with ADHD. Its interdisci-plinaryinnovationliesinitsapplicationofawell-established measureofcolorvision(FMT)alongwithalessusedmeasure ofvisualfunctioningtotestanovelhypothesis(retinal dopa-minergichypothesis22)inaprevalentpsychiatriccondition
(ADHD),which isnot traditionallylinkedwithvisual prob-lems. Ourfindingshighlight the need for furtherresearch onthecomplexinteractionsbetweenattention,color per-ception,andvisualfunctioningandunderlyingexplanatory mechanisms. Moreover,our findings indicatethe need for optometrists,psychiatrists,andother cliniciansto investi-gatevisualfunctionintheassessmentofyoungadultswith ADHD.TheVAQappearstobeapsychometricallysound mea-surethatmayserveasausefulclinicaltoolforinvestigating self-reportedvisualfunctionindailylife.
Conflicts
of
interest
DrTannockhasservedasaconsultantforEliLillyandPurdue Pharmaceuticals in thepast 3 years,andPearson-Cogmed providessoftwarelicenceswithoutcostforherresearchon
VisualfunctioninADHD 35 workingmemorytraininginADHDcollegestudents;neither
MsKimnorMsChenhaveanyconflictsofinterest.
Acknowledgements
Special thanks to Heidi Bernhardt, the president and nationaldirectoroftheCenterforADHDAwareness,Canada (CADDAC)forherhelpinrecruitingADHDparticipants.Also weappreciateourresearchassistantsHamedDarandPalm Soontornsittipongfortheirhelpindatacollection.Thisstudy wasfundedinpartbytheCanadaResearchChairsprogram (RT)andGraduateFunding(SK).
References
1.PolanczykG,JensenP.Epidemiologicconsiderationsin atten-tiondeficithyperactivitydisorder:areviewandupdate.Child AdolescPsychiatrClinNAm.2008;17:245---260.
2.Barkley RA, Fischer M, Smallish L, Fletcher K. The persis-tenceofAttention-Deficit/Hyperactivity Disorder intoyoung adulthoodasafunctionofreportingsourceanddefinitionof disorder.JAbnormPsychol.2002;111:279---289.
3.FaraoneSV,BiedermanJ,MickE.Theage-dependentdecline ofattentiondeficithyperactivitydisorder:ameta-analysisof follow-upstudies.PsycholMed.2006;36:159---165.
4.RamtekkarUP,ReiersenAM,TodorovAA,ToddRD.Sexandage differencesinAttention-Deficit/HyperactivityDisorder symp-tomsanddiagnoses:implicationsforDSM-VandICD-11.JAm AcadChildAdolescPsychiatry.2010;49:217---228.
5.Pelham WE, Foster EM, Robb JA. The economic impact of Attention-Deficit/HyperactivityDisorderinchildrenand ado-lescents.JPediatrPsychol.2007;32:711---727.
6.RosenbloomT,WultzB.Thirty-dayself-reportedriskydriving behaviors ofADHD and non-ADHD drivers. Accid AnalPrev. 2011;43:128---133.
7.Cox DJ, Madaan V, Cox BS. Adult Attention-Deficit/Hyperactivity Disorder and driving: why and how tomanageit.CurrPsychiatryRep.2011;13:345---350. 8.Reimer B, Mehler B, D’Ambrosio LA, Fried R. The impact
of distractions on young adult drivers with Attention Deficit Hyperactivity Disorder (ADHD). Accid Anal Prev. 2010;42:842---851.
9.RichardsTL,DeffenbacherJL,RosénLA,BarkleyRA,Rodricks T.DrivingangeranddrivingbehaviorinadultswithADHD.J AttenDisord.2006;10:54---64.
10.RichardsT,DeffenbacherJ,RosénL.Drivingangerandother driving-relatedbehaviorsinhighandlowADHDsymptom col-legestudents.JAttenDisord.2002;6:25---38.
11.GranetDB,GomiCF,VenturaR,Miller-ScholteA.The relation-shipbetweenconvergenceinsufficiencyandADHD.Strabismus. 2005;13:163---168.
12.Borsting E, Rouse M, Chu R. Measuring ADHD behaviors in children with symptomatic accommodative dysfunction or convergence insufficiency: a preliminary study. Optometry. 2005;76:588---592.
13.RouseM,Borsting E,MitchellGL,etal. Academicbehaviors inchildrenwithconvergenceinsufficiency withandwithout parent-reportedADHD.OptomVisSci.2009;86:1169---1177. 14.ChungSA,ChangYH,RhiuS,LewH,LeeJB.Parent-reported
symptomsofAttentionDeficitHyperactivityDisorderin chil-drenwithintermittentexotropiabeforeandafterstrabismus surgery.YonseiMedJ.2012;53:806---811.
15.GrönlundMA,AringE,LandgrenM,HellströmA.Visualfunction andocularfeaturesinchildrenandadolescentswithAttention
DeficitHyperactivityDisorder,withandwithouttreatmentwith stimulants.Eye.2007;21:494---502.
16.MartinL,AringE,LandgrenM,HellströmA,GrönlundMA.Visual fieldsinchildrenwithAttention-Deficit/HyperactivityDisorder beforeandaftertreatmentwithstimulants.ActaOphthalmol. 2008;86:259---264.
17.BanaschewskiT,RuppertS,TannockR,etal.Colourperception inADHD.JChildPsycholPsychiatry.2006;47:568---572. 18.RoessnerV,BanaschewskiT,Fillmer-OtteA,etal.Colour
per-ceptiondeficitsinco-existingAttention-Deficit/Hyperactivity Disorder and chronic tic disorders. J Neural Transm. 2008;115:235---239.
19.SilvaAP,FrèreAF.Virtualenvironmenttoquantify the influ-enceofcolourstimuliontheperformanceoftasksrequiring attention.BiomedEngOnline.2011;10:74.
20.Tannock R, Martinussen R, Frijters J. Naming speed per-formanceand stimulant effects indicate effortful, semantic processingdeficitsinAttention-Deficit/HyperactivityDisorder. JAbnormChildPsychol.2000;28:237---252.
21.Lawrence V, Houghton S, Douglas G, Durkin K, Whiting K, Tannock R. Executive function and ADHD: a comparison of children’sperformanceduringneuropsychologicaltestingand real-worldactivities.JAttenDisord.2004;7:137---149. 22.TannockR,BanaschewskiT,GoldD.Colournamingdeficitsand
Attention-Deficit/HyperactivityDisorder:aretinal dopaminer-gichypothesis.BehavBrainFunct.2006;2:4.
23.SagvoldenT,JohansenEB,AaseH,RussellVA.Adynamic devel-opmental theory of Attention-Deficit/Hyperactivity Disorder (ADHD) predominantly hyperactive/impulsive and combined subtypes.BehavBrainSciJun.2005;28:397---419.
24.AdlerLA,SpencerT,FaraoneSV,etal.ValidityofpilotAdult ADHDSelf-ReportScale(ASRS)torateadultADHDsymptoms. AnnClinPsychiatry.2006;18:145---148.
25.HinesJL,KingTS,CurryWJ.TheAdultADHDSelf-ReportScale forscreeningforAdultAttentionDeficit-HyperactivityDisorder (ADHD).JAmBoardFamMed.2012;25:847---853.
26.WechslerD.WechslerAbbreviatedScaleofIntelligence--- sec-ondeditionmanual.Bloomington,MN:Pearson;2011. 27.KesslerRC,AndrewsG,ColpeLJ,etal.Shortscreeningscales
tomonitorpopulationprevalencesandtrendsinnon-specific psychologicaldistress.PsycholMed.2002;32:959---976. 28.SloaneM,BallK,OwsleyC,BruniJ,RoenkerD.TheVisual
Activ-ities Questionnaire: developing an instrument for assessing problems ineverydayvisual tasks.Tech DigNoninvasAssess VisSys.1992;1:26---29.
29.JanzNK,MuschDC,GillespieBW,WrenPA,NiziolLM, Collabo-rativeInitialGlaucomaTreatmentStudy(CIGTS)Investigators. Evaluating clinical change and visual function concerns in driversandnondriverswithglaucoma.InvestOphthalmolVis Sci.2009;50:1718---1725.
30.Janz NK,Wren PA,Lichter PR,et al. The Collaborative Ini-tialGlaucomaTreatmentStudy:interimqualityoflifefindings afterinitialmedicalorsurgicaltreatmentofglaucoma. Oph-thalmology.2001;108:1954---1965.
31.CorenS,HakstianAR.Colourvisionscreeningwithouttheuseof technicalequipment:scaledevelopmentandcross-validation. PercepPsychophys.1988;43:115---120.
32.Farnsworth D. The Farnsworth-Munsell 100-Hue test. Balti-more:MunsellColourCompany;1957.
33.WiigEH,NielsenNP.Aquicktestofcognitivespeedfor compar-ingprocessingspeedtodifferentiateadultpsychiatricreferrals with and without Attention-Deficit/Hyperactivity Disorders. PrimCareCompanionCNSDisord.2012;14:2.
34.Taylor JF. Vision and driving. Ophthalmic Physiol Opt. 1987;7:187---189.
35.Owsley C, Stalvey BT, Wells J, Sloane ME, McGwin Jr G. Visualriskfactorsforcrashinvolvementinolderdriverswith cataract.ArchOphthalmol.2001;119:881---887.
36.HeringE.Outlinesofatheoryofthelightsense.Cambridge, MA:HarvardUniversityPress;1964.
37.HurvichLM,JamesonD.Anopponentprocesstheoryofcolor vision.PsycholRev.1957;64:384---404.
38.Hankins MW,Peirson SN,FosterRG. Melanopsin:anexciting photopigment.TrendsNeurosci.2008;31:27---36.
39.Bailes HJ, Lucas RJ. Human melanopsin forms a pigment maximallysensitivetobluelight(max≈479nm)supporting activationofG(q/11)andG(i/o)signallingcascades.ProcBiol Sci.2013;3;280:20122987.
40.ImerajL,Sonuga-BarkeE,AntropI,etal.Alteredcircadian pro-filesinAttention-Deficit/HyperactivityDisorder:anintegrative
reviewandtheoreticalframeworkforfuturestudies.Neurosci BiobehavRevSep.2012;36:1897---1919.
41.Andersson M, Wiig EH, Minthon L, Londos E. A quick test forcognitivespeed:ameasureofcognitivespeedin demen-tia with Lewy bodies. Am J Alzheimers Dis Other Demen. 2007;22:313---318.
42.WiigEH,NielsenNP,MinthonL,McPeekD,SaidK,Warkentin S.Parietal lobe activationin rapid,automatized namingby adults.PerceptMotSkills.2002;94:1230---1244.
43.Cohen J. Statistical power analysis for the behavioral sci-ences. 2nded.Hillsdale,NJ:LawrenceEarlbaumAssociates; 1988.