This appendix has been provided by the authors to give readers additional information about their work.
Supplement to: Kaske EA, Cramer SW, Pena Pino I, et al. Injuries from less-lethal weapons during the George Floyd protests in Minneapolis. N Engl J Med. DOI: 10.1056/NEJMc2032052
Methods 2
Study Design and Participants 2
Data Collection 2 Definitions 2 Statistical Analysis 2 Results 2 Demographics 2 Injury Severity 3
Figure S1. Spatial distribution of projectile injuries to anatomic regions 4 Figure S2. Pediatric patient with a compound, depressed skull fracture 5 Figure S3. Patient with ruptured globe and closed fracture of right orbit 6 Figure S4. Open wound from a rubber bullet to the lower extremity. 7
Table S1. Demographics and clinical characteristics 8
Table S2. Injury Inventory 9
Table S3. Surgery Inventory 10
Methods
Study Design and Participants
This retrospective study included two cohorts of patients from M Heath Fairview and Hennepin County Medical Center (Minneapolis, MN) with local IRB approval. All patients (adult, pediatric) received medical evaluation during the period May 26 to June 15, 2020 at Primary Care Clinics, Urgent Care, and the Emergency Department with ICD10 codes S00-T59 or patients with “riot” or “rubber bullet” or “tear gas” or “protest” or “projectile” in patient notes comprised the inclusion criteria. We excluded patients who (1) did not sustain injury or (2) if injuries did not relate to the protests. This analysis excluded injuries not related to less-lethal weapons or officer violence. Injury Severity Score (ISS) served as our primary outcome. To report injuries, we followed the STROBE (Strengthening the Reporting of Observation Studies in Epidemiology) guidelines.
Data Collection
Structured Query Language (SQL) was used to screen ICD billing codes and keywords in the electronic medical record (EMR). Two researchers then independently reviewed each patient's EMR and determined if they met inclusion/exclusion criteria. Research Electronic Data Capture (REDCap) generated patient demographics, injury inventories, medical history, COVID-19 status, and radiographic results.
Definitions
The Abbreviated Injury Scale (AIS), Injury Severity Score (ISS), and Ocular Trauma Score (OTS) was used to classify the severity of trauma.1–3 ISS scores range from 3-75 and minor trauma is <9,
moderate trauma is 9-15, and major trauma is >15. Traumatic Brain Injury (TBI) was defined by the evaluating provider at the time of diagnosis and identified by study researchers in the medical record problem list. Distance from the protest was calculated using the patient home address listed in the electronic medical record and the Minneapolis, MN third precinct address.
Statistical Analysis
We computed descriptive statistics as percentages and means, and we used nonparametric statistics where appropriate. All statistics were performed with R software.4
Results
Demographics
Of the 6626 medical records identified during the initial search, 89 met the study inclusion and exclusion criteria. The median age was 28 years. Forty-seven (52.0%) of patients were male, 39 (43.8%) were female, and 3 (3.4%) identified as neither male nor female gender. Forty-seven (52.8%) patients were non-Hispanic white, 25 (28.1%) were non-Hispanic black, 6 (6.7%) were Hispanic, 5 (5.6%) were American Indian/Alaskan Native, and 6 (6.7%) patients were of unknown or another race and ethnicity. The median distance of residence was 5.2 km from the third precinct, and 87.6% lived within 25.0 km.
Thirty of 89 (33.7%) patients were evaluated for alcohol ingestion, and 8 of 30 (26.7%) were determined to be intoxicated
Injury Severity
The ISS was on average 4.76 (standard deviation (SD) = 4.83) with 77 (86.5%) mild injuries, 8 (9.0%) moderate injuries, and 4 (4.5%) severe injuries. Approximately half of the patients had a known exposure to tear gas (44 [49.4%]). Average ISS for patients only exposed to tear gas was 1.36 (SD = 1.65), which is equivalent to very minor trauma. Those suffering kinetic impact projectile injury were higher ISS 6.18 (SD = 5.16)
Figure S1. Spatial distribution of projectile injuries to anatomic regions
We defined anatomic areas of interests as: head, face, and neck; thorax and abdomen; upper extremities; and the lower extremities. We tabulated the number of strikes to each anatomic region from kinetic impact projectiles across our sample of 89 patients. Matlab was used to generate a colormap to depict the frequency of strikes. Anatomic regions were colored using the specific colors assigned by Matlab. Absolute strike counts were 37, 20, 15, and 14 to the head, face, and neck; thorax and abdomen; upper extremities; and the lower extremities, respectively.
Figure S2. Pediatric patient with a compound, depressed skull fracture
Patient was a bystander; rubber bullet caused a scalp laceration (a) and a compound, depressed skull fracture of the frontal bone. (b) Coronal, (c) sagittal, (d)(e) axial views demonstrate depressed skull fracture (solid arrow) complicated by pneumocephalus (double arrow) and extra-axial hemorrhage (open arrow). Patient underwent surgical elevation of the depressed skull fracture and removal of cranial fragments. Patient was discharged three days after surgery.
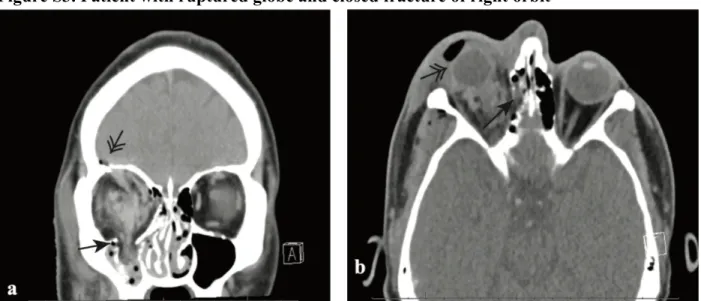
Figure S3. Patient with ruptured globe and closed fracture of right orbit
Tear gas canister caused a loss of consciousness, (a) coronal image demonstrates orbital blowout fracture with extraocular muscle entrapment (closed arrow) and orbital roof fracture with pneumocephalus (double arrow), (b) axial image demonstrates medial orbital wall fracture (closed arrow) and right globe rupture and retinal detachment (double arrow). They underwent multiple surgeries, however, vision in the right eye is permanently impaired and the patient is now legally blind in the right eye.
Figure S4. Open wound from a rubber bullet to the lower extremity.
Rubber bullet preceded cellulitis of the leg 1 week after rubber bullet injury. The patient recovered after intravenous antibiotic treatment, and surgical debridement was not performed.
Table S1. Demographics and clinical characteristics Patients (n = 89) Age, years Median 28 Range 15-77 <18 4 (4.5%) 18-30 51 (57.3%) 30-50 26 (29.2%) >50 7 (7.9%) Gender Female 39 (43.8%) Male 47 (52.8%) Other 3 (3.4%)
Race and Ethnicity
Non-Hispanic White 47 (52.8%)
Non-Hispanic Black 25 (28.1%)
Hispanic 6 (6.7%)
American Indian/Alaskan Native 5 (5.6%)
Unknown or Other 6 (6.7%)
Location
Emergency Department 69 (77.5%)
Urgent Care 7 (7.9%)
Primary Care Clinics 13 (14.6%)
Distance from Residence to Protest, km
Median 4.93 Range 0.4-2475 <5 47 (52.8%) 0-25 31 (34.8%) 25-100 7 (7.9%) >1000 6 (6.7%) Employed Yes 44 (49.4%) No 24 (27.0%) Unknown 21 (23.6%) Intoxicated Positive Test 8 (9.0%) Negative Test 22 (24.7%) Not Tested 59 (66.3%) COVID Test Tested, Positive 1 (1.1%) Tested, Negative 23 (25.5%) Not Tested 65 (73%)
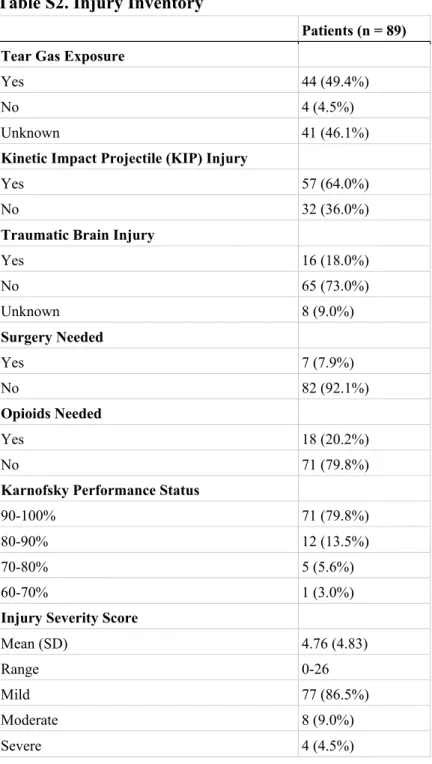
Table S2. Injury Inventory
Patients (n = 89) Tear Gas Exposure
Yes 44 (49.4%)
No 4 (4.5%)
Unknown 41 (46.1%)
Kinetic Impact Projectile (KIP) Injury
Yes 57 (64.0%)
No 32 (36.0%)
Traumatic Brain Injury
Yes 16 (18.0%) No 65 (73.0%) Unknown 8 (9.0%) Surgery Needed Yes 7 (7.9%) No 82 (92.1%) Opioids Needed Yes 18 (20.2%) No 71 (79.8%)
Karnofsky Performance Status
90-100% 71 (79.8%)
80-90% 12 (13.5%)
70-80% 5 (5.6%)
60-70% 1 (3.0%)
Injury Severity Score
Mean (SD) 4.76 (4.83)
Range 0-26
Mild 77 (86.5%)
Moderate 8 (9.0%)
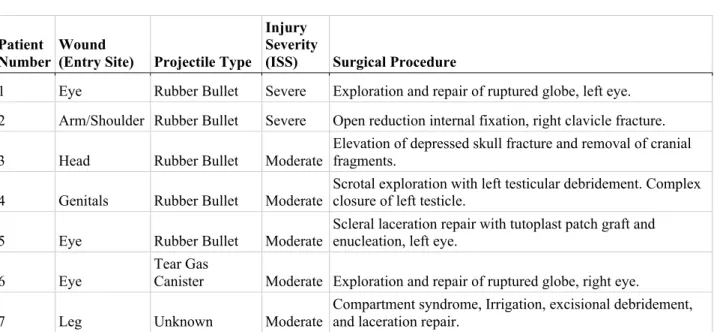
Table S3. Surgery Inventory
Patient Number
Wound
(Entry Site) Projectile Type
Injury Severity
(ISS) Surgical Procedure
1 Eye Rubber Bullet Severe Exploration and repair of ruptured globe, left eye.
2 Arm/Shoulder Rubber Bullet Severe Open reduction internal fixation, right clavicle fracture.
3 Head Rubber Bullet Moderate Elevation of depressed skull fracture and removal of cranial fragments.
4 Genitals Rubber Bullet Moderate Scrotal exploration with left testicular debridement. Complex closure of left testicle.
5 Eye Rubber Bullet Moderate
Scleral laceration repair with tutoplast patch graft and enucleation, left eye.
6 Eye
Tear Gas
Canister Moderate Exploration and repair of ruptured globe, right eye.
Supplemental References
1. Stevenson M, Segui-Gomez M, Lescohier I, Di Scala C, McDonald-Smith G. An overview of the injury severity score and the new injury severity score. Inj Prev 2001;7(1):10–3. 2. Palmer CS, Gabbe BJ, Cameron PA. Defining major trauma using the 2008 Abbreviated
Injury Scale. Injury 2016;47(1):109–15.
3. Scott R. The Ocular Trauma Score. Community Eye Health 2015;28(91):44–5. 4. R Core Team. R: A Language and Environment for Statistical Computing [Internet].