639
SCOTT DAVID MARTIN • THOMAS S. THORNHILL
causes of shoulder pain. Final diagnosis may require repeated office examinations and correlation of diagnostic tests with symptoms and response to selective injections. Improve-ments in diagnostic tests, such as magnetic resonance imaging (MRI), computed tomography (CT)-arthrography, ultrasonography, and electromyography (EMG), have facili-tated early diagnosis of shoulder pain and have provided a better understanding of shoulder pathology.
This chapter provides practical guidelines for the diag-nosis and treatment of painful shoulder disorders that may be encountered in a rheumatology or general practice. A detailed analysis of shoulder problems and information on the treatment of major trauma are beyond the scope of this chapter and have been addressed by other authors.
ANATOMY AND FUNCTION
Because of its complexity, an understanding of the structural and functional anatomy of the shoulder is required for the clinician who is treating shoulder pain. The shoulder joint is the most mobile joint of the body, although mobility is gained at the sacrifice of stability. Only 25% of the humeral head surface has contact with the glenoid at any time. The labrum increases the contact area of the articular surface and confers stability to the joint.6 Lesions of the labrum may
result from instability, and the type of lesion may indicate the type of instability. Labral tears also may be a source of pain from internal derangement of the shoulder.7 Joint
sta-bility is provided by a thin capsule and by the glenohumeral ligaments, which are thickenings of the capsule anteriorly, posteriorly, and inferiorly.6 Anterior stability is
predomi-nantly conferred by the anterior band of the inferior gleno-humeral ligament.
The rotator cuff provides dynamic stability of the joint. It is composed of four musculotendinous units: the supraspi-natus, infraspisupraspi-natus, and teres minor posteriorly, and the subscapularis anteriorly. The shoulder consists of three joints: the acromioclavicular (AC), sternoclavicular, and glenohumeral joints, and two gliding planes—the scapulo-thoracic and subacromial surfaces.
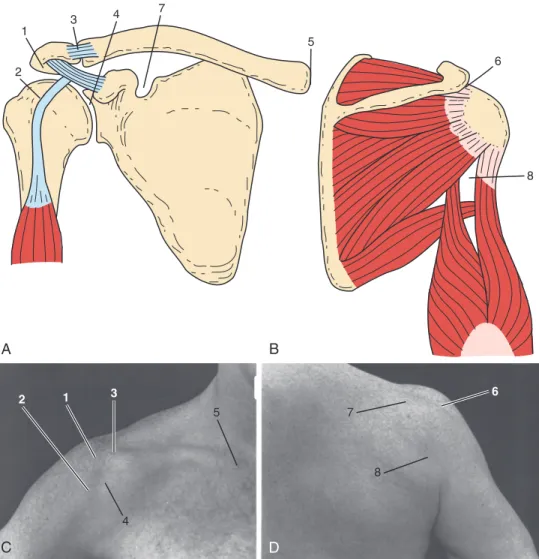
Figure 46-1 shows the musculoskeletal and topographic localization of pain associated with common shoulder dis-orders. Figure 46-2 shows the relationship of the three pos-terior rotator cuff muscles coursing anpos-teriorly underneath the acromion to insert on the greater tuberosity. The sub-scapularis, the only anterior rotator cuff muscle, inserts on the lesser tuberosity. By understanding the relationship between the rotator cuff and the subacromial region, bounded inferiorly by the humeral head and superiorly by the undersurface of the acromion, the clinician can visualize the problems of impingement syndrome and can accurately KEY POINTS
Comprehension of functional anatomy allows diagnosis of most causes of shoulder pain on clinical examination. History and clinical examination aided by ancillary tests will usually guide application of the most appropriate treatment for shoulder pain.
The differential diagnosis of shoulder pain includes not only common local disorders (e.g., of tendon and adjacent structures) but should also include consideration of etiologies arising from distant anatomic sites arising by referred pain-mediated pathways.
A variety of specific diagnostic tests can greatly aid in diagnosis of shoulder pain.
Most causes of shoulder pain can be treated with a structured physical therapy program. Successful treatment programs understand potential surgical candidates including those who fail conservative treatment.
Systemic arthroopathies can occasionally present with shoulder disease and often involve the shoulder over time. Early assessment in such patients is essential.
Shoulder pain is one of the most common musculoskeletal complaints that may arise from diverse causes. Accurate diagnosis of shoulder pain is made difficult by the unique anatomy and position of the shoulder, which serves as a link between the upper extremity and the thorax. One of the most complex and mobile joints of the body, the shoulder is traversed by muscle, tendon, and bone, and is surrounded by major neurovascular structures, all of which may serve as potential sources of local and referred pain.
Determining the source of shoulder pain is essential in recommending the proper method of treatment. The exam-ining physician must be able to differentiate the occurrence of shoulder pain caused by intrinsic, or local factors, and extrinsic, or remote factors, or a combination of the two. Intrinsic factors originate from the shoulder girdle and include glenohumeral and periarticular disorders, whereas extrinsic factors occur outside of the shoulder girdle with secondary referral of pain to the shoulder (Table 46-1). Examples of extrinsic factors include left shoulder pain as the initial presentation of coronary artery disease; hepatic, gallbladder, and splenic disease also may initially manifest as shoulder pain.
Accurate evaluation, diagnosis, and treatment require a thorough understanding of shoulder anatomy, including pain referral patterns. A complete and systematic physical examination is crucial for an accurate diagnosis. During the initial evaluation, care must be taken to discern all possible
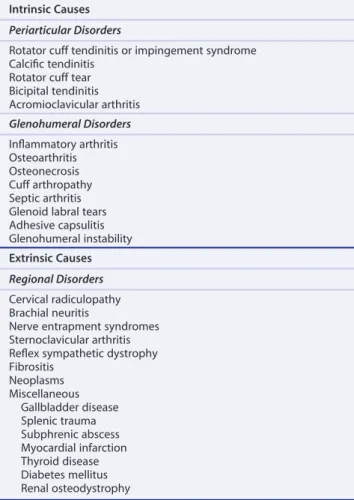
Table 46-1 Common Causes of Shoulder Pain Intrinsic Causes
Periarticular Disorders
Rotator cuff tendinitis or impingement syndrome Calcific tendinitis
Rotator cuff tear Bicipital tendinitis Acromioclavicular arthritis Glenohumeral Disorders Inflammatory arthritis Osteoarthritis Osteonecrosis Cuff arthropathy Septic arthritis Glenoid labral tears Adhesive capsulitis Glenohumeral instability Extrinsic Causes Regional Disorders Cervical radiculopathy Brachial neuritis
Nerve entrapment syndromes Sternoclavicular arthritis Reflex sympathetic dystrophy Fibrositis Neoplasms Miscellaneous Gallbladder disease Splenic trauma Subphrenic abscess Myocardial infarction Thyroid disease Diabetes mellitus Renal osteodystrophy
inject this space. Knowledge of the route of the tendon of the long head of the biceps through the bicipital groove and onto the superior aspect of the glenoid helps in understand-ing bicipital tendinitis. Before attemptunderstand-ing to diagnose and treat shoulder pain, the clinician should review in detail one of the many sources describing the structural and functional relationships of the shoulder girdle.2,3
DIAGNOSIS
Clinical Evaluation of the Shoulder
Accurate diagnosis and successful treatment of a shoulder disorder begin with a thorough history and physical exami-nation. Most of the information needed to make a correct diagnosis can be elicited with basic clinical skills, rather than by relying on expensive and highly technologic inves-tigative aids. Diagnostic tests should be used only to confirm an established diagnosis or to assist in cases with a challeng-ing presentation.
History
In establishing a diagnosis, it is important to consider the patient’s age and chief complaint. The differential diagnosis of shoulder pain in a 70-year-old sedentary individual is entirely different from that in a 20-year-old pitcher. Did the pain occur slowly over time or suddenly with a particular
event? Gradual onset of pain over the anterolateral or deltoid region that is increased with forward elevation of the shoulder and nocturnal pain suggest impingement with rotator cuff tendinopathy. The presence of significant weak-ness with pain on overhead activities suggests impingement with rotator cuff tear. Pain and weakness may also be noted with reaching behind the back with the shoulder in exten-sion and external rotation, as when reaching into the back seat of a car. Initiating factors relative to the onset of symp-toms should be elicited, and any history of shoulder pain or trauma should be carefully documented.
Pain intensity, character, location, and periodicity and aggravating or alleviating factors should be assessed. Pain should be graded on a visual analog scale of 0 to 10, with 0 indicating no pain, and 10 indicating the worst pain the patient has ever experienced. Another indication of the severity of pain is disruption of sleep. The patient should be asked whether the pain prevents sleep or awakens the patient, and whether the patient can lie on the affected shoulder. Is the pain sharp or dull? Sharp, burning pain over the top of the shoulder indicates a neurogenic origin, whereas a dull, aching pain over the lateral deltoid suggests rotator cuff pathology with impingement. Location or dis-tribution of the pain should be identified. Is it local around the shoulder girdle, or does the pain radiate down the arm? Is concomitant sensory loss or weakness present? Periodicity of the pain as constant or intermittent should be deter-mined, as should factors that aggravate or alleviate the pain. Pain caused by rotator cuff tendinopathy usually is exacer-bated by repetitive activities that involve the elbow away from the side of the body.
Any history of neck pain should be considered, along with history of radicular pain. Radicular-type pain fre-quently extends below the elbow and is associated with sensory loss and weakness. Pain located in the paracervical region may indicate a cervical origin, or it can be localized to the trapezius. Trapezial pain often is associated with shoulder pain and results from the patient trying to favor the shoulder. Assuming a military brace position may produce fatiguing, spasm, and trigger points of the trapezius.
Any pertinent medical history, such as a history of malig-nancy, should be considered. Neurologic, visceral, and vas-cular disease can produce referred pain to the shoulder and should always be considered, especially in a patient with a painless range of motion.
Physical Examination
Proper physical examination of the shoulder includes close inspection of the shoulder girdle from the front and back. The evaluation is started by standing behind the patient, who has both shoulders exposed. The normal shoulder is always inspected and compared with the injured shoulder. Examination can be performed with the patient in the sitting or standing position. Contour and symmetry are observed and compared between shoulders, and any atrophy or asymmetry in shoulder position or level is assessed. Spi-natus muscle atrophy may result from disuse, chronic cuff tear, or suprascapular or brachial neuropathy.8 If scapular
winging is evident, the patient should be asked to do a wall push-up, which accentuates winging.
Figure 46-1 Musculoskeletal (A and B) and topographic (C and D) areas localizing pain and tenderness associated with specific shoulder problems. 1, Subacromial space (rotator cuff tendinitis/impingement syndrome, calcific tendinitis, rotator cuff tear). 2, Bicipital groove (bicipital tendinitis, biceps tendon subluxation and tear). 3, Acromioclavicular joint. 4, Anterior glenohumeral joint (glenohumeral arthritis, osteonecrosis, glenoid labrum tears, adhesive capsulitis). 5, Sternoclavicular joint. 6, Posterior edge of acromion (rotator cuff tendinitis, calcific tendinitis, rotator cuff tear). 7, Suprascapular notch (suprascapular nerve entrapment). 8, Quadrilateral space (axillary nerve entrapment). These areas of pain and tenderness frequently overlap.
A B C D 1 2 3 5 4 7 8 6 2 1 3 4 5 6 8
Figure 46-2 A, Superior view of the rotator cuff musculature as it courses anteriorly underneath the coracoacromial arch to insert on the greater tuberosity. B, Anterior view of the shoulder reveals the subscapularis, which is the only anterior rotator cuff muscle inserting on the lesser tuberosity. It internally rotates the humerus and provides dynamic anterior stability to the shoulder. (A and B, From the Ciba Collection of Medical Illustrations, Volume 8, Part I. Netter Illustration from www.netterimages.com ©Elsevier Inc. All rights reserved.)
Trapezoid ligament
Conoid ligament Coracoid process
Subscapularis tendon Supraspinatus tendon Infraspinatus tendon Teres minor tendon Clavicle Coracoclavicular ligament: Subscapularis muscle Supraspinatus muscle Supraspinatus muscle Acromion of scapula Coracoacromial ligament Spine of scapula Superior margin of scapula Infraspinatus muscle Coracoid process Clavicle Coracoacromial ligament Supraspinatus tendon Subscapularis tendon Greater tuberosity Lesser tuberosity Humerus
Bicipital tendon groove
A B
Acromioclavicular joint Acromion
while applying axial compression to the skull. Pain that radiates to the ipsilateral shoulder is considered a positive test result and indicates radiculopathy.
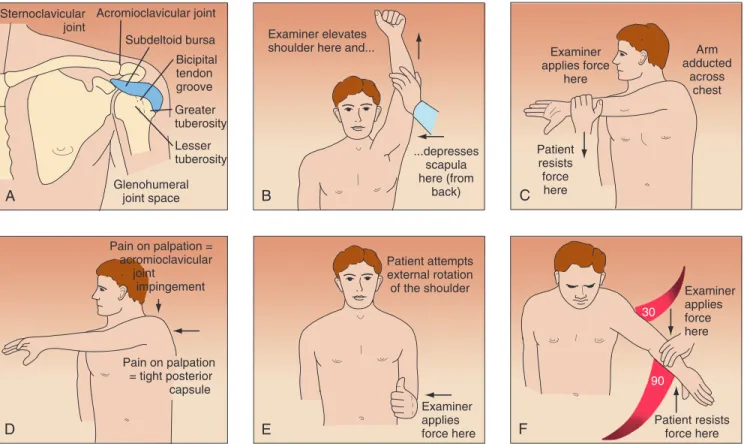
To elicit the impingement sign, the shoulder is elevated passively in forward flexion, while the scapula is depressed with the opposite hand, forcing the greater tuberosity against the anterior acromion and producing pain in cases of impingement (Figure 46-3B).9 This maneuver also may
be painful in conditions such as adhesive capsulitis, glenohumeral and acromioclavicular (AC) arthritis, gleno-humeral instability, and calcific tendinitis. A dynamic impingement test, the circumduction-adduction shoulder maneuver, also called the Clancy test, is 95% sensitive and 95% specific for diagnosing rotator cuff tendinopathy, including partial tears.10 The test is done with the patient
in the standing position and with the head turned to the contralateral shoulder. The affected shoulder is circum-ducted and adcircum-ducted across the body to shoulder level, while the elbow is kept in extension, the shoulder in inter-nal rotation, and the thumb pointing toward the floor Range of motion should be carefully recorded, along with
notation of any absence of rhythmic shoulder motion or excessive scapulothoracic motion that may compensate for the lack of glenohumeral motion. Internal rotation of the shoulder is checked by having the patient reach behind the back with the thumb while the examiner notices the verte-bral level. Loss of internal rotation is seen early with shoul-der pain and usually indicates some tightness of the posterior shoulder capsule. The biceps tendon; the coracoid, lesser, and greater tuberosities; and the posterior cuff are palpated, and any tenderness is gauged (Figure 46-3A). Tenderness on palpation of the long head of the biceps frequently is associated with rotator cuff tendinopathy and tenderness of the greater tuberosity. Any spasm or tenderness of the tra-pezius or levator scapulae may be associated with rotator cuff disease or cervical spine disease. Cervical range of motion and palpation of the paracervical muscles are carried out. Paracervical tenderness and limited range of motion of the neck may indicate cervical spondylosis or neurogenic disease. A Spurling test is done by flexing the neck laterally
Figure 46-3 A, Tenderness on palpation of trigger points may help localize the site of pathology. Tenderness on palpation of the long head of the biceps and greater tuberosity suggests impingement with possible cuff tendinopathy. B, To elicit the impingement sign, the shoulder is elevated in forward flexion while the scapula is depressed with the opposite hand, forcing the greater tuberosity and the rotator cuff against the anterior acromion and producing pain when impingement exists. Relief of pain after injection of local anesthetics (i.e., impingement test) provides additional evidence of subacromial pathology. C, The Clancy test is performed with the patient standing and with the head turned toward the contralateral shoulder. The affected shoulder is circumducted and adducted across the body to shoulder level, keeping the elbow in extension with the arm internally rotated with the thumb pointed toward the floor. In this position, the patient is asked to resist maximally as a uniform downward force is applied to the extended arm by the examiner. Production of pain or weakness localized to the anterior lateral portion of the shoulder is considered a positive test result. D, The test is performed by forward flexion of the arm at 90 degrees and subsequent cross-chest adduction of the arm. Pain localized to the acromioclavicular joint is considered a positive test result. E, The test is performed with the patient’s elbow flexed at 90 degrees and held at the patient’s side by the examiner. The patient is asked to attempt external rotation of the shoulder from a neutral position (0 degrees of adduction) as the examiner applies resistance to the forearm. Strength is compared with that of the contralateral arm. F, Abduction strength testing is performed with the patient’s shoulder in 30 degrees of forward flexion and 90 degrees of abduction and with the thumb pointed toward the floor. The patient is asked to resist as the examiner exerts a downward force on the abducted arm. Strength is compared with the contralateral shoulder. (From Martin TL, Martin SD: Rotator cuff tendinopathy, Hosp Med 12:23–31, 1998.)
Sternoclavicular
joint Acromioclavicular joint Subdeltoid bursa Greater tuberosity Lesser tuberosity Glenohumeral joint space Bicipital tendon groove A Examiner elevates shoulder here and...
...depresses scapula here (from back) B Examiner applies force here Examiner applies force here Examiner applies force here Patient resists force here Patient resists force here Patient attempts external rotation of the shoulder Arm adducted across chest C Pain on palpation = acromioclavicular joint impingement Pain on palpation = tight posterior capsule D E 30 90 F
tion should be done with the elbow at the side and sup-ported by the examiner; the patient is asked to attempt external rotation of the shoulder from a neutral position (0 degrees of adduction), while the examiner applies resistance (Figure 46-3E).15 Weakness in this position may suggest a
tear of the infraspinatus tendon. Abduction strength testing against resistance is done with the shoulder in 30 degrees of forward flexion and 90 degrees of abduction, and with the thumb pointed toward the floor (Figure 46-3F).16,17
Weak-ness in this position may suggest a tear of the supraspinatus tendon. A lift-off test should be performed with the shoul-der in internal rotation; the patient is asked to try to hold the hand away from the back. Inability to do so indicates a subscapularis tear.
If after a thorough physical examination impingement is suspected, an impingement test should be performed with injection of 5 mL of local anesthetic into the subacromial space.18,19 Before the test is performed, the patient is asked
to grade the pain during the impingement signs on a visual analog scale of 0 to 10, with 0 equal to no pain and 10 equal to the most severe pain the patient has ever experienced. The injection may be done anteriorly, laterally, or posteri-orly, depending on the physician’s preference. Ten minutes after injection of local anesthetic into the subacromial space, the patient should be re-examined and asked to regrade the pain on the same visual analog scale. A 50% or greater reduction in pain is thought to be a positive test result for impingement; otherwise, an alternative cause of shoulder pain should be sought, or inadequate placement of the anesthetic should be suspected. If the AC joint is thought to be contributing to the shoulder pain, 1 to 2 mL of local anesthetic should be injected into the joint, and the shoulder should be re-examined. When subacromial impingement and the AC joint are thought to be contribut-ing to shoulder pain, serial injections durcontribut-ing separate office visits may be needed to evaluate the shoulder while mini-mizing discomfort to the patient.12
In cases of suspected bicipital tendinitis, Speed’s test is performed by having the patient flex the shoulder and extend the elbow while a downward force is applied to the arm. The production of pain over the long head of the biceps is a positive test result and suggests bicipital tendinitis.
Upper extremity strength testing should be performed and compared with the contralateral side so that any atrophy is detected. Grip strength is checked, and the hands are examined carefully for evidence of intrinsic atrophy. The biceps (C5), triceps (C7), and brachioradialis (C6) reflexes are checked for symmetry and briskness.
Light touch sensory testing should be conducted, and the dermatomal distribution of any deficits that may suggest cervical radiculopathy should be identified. The cervical, supraclavicular, axillary, and epitrochlear regions should be palpated for enlarged lymph nodes, which may suggest malignancy.
Imaging
Radiographic Assessment
For nontraumatic painful shoulder evaluation, standard radiographic profiles are used. An impingement series resist maximally as a uniform downward force is applied to
the extended arm by the examiner. The test result is con-sidered positive if pain or weakness is elicited during the maneuver, with pain localized to the anterolateral aspect of the shoulder. A strong positive correlation of pain and weakness is noted with complete cuff tear.10
The sternoclavicular and AC joints should be observed for prominences and palpated for stability and tenderness. Many patients with impingement have tenderness on direct downward palpation of the AC joint owing to impingement on the cuff from undersurface osteophytes of the distal clavicle.2,8
AC joint tenderness may also result from primary AC joint arthrosis and should be differentiated by physical examination, including the cross-chest adduction test and O’Brien’s test.11 Radiographic evidence of AC joint
arthro-sis is common in patients older than 40 years, but this condition is not usually painful.12
The cross-chest adduction test or the horizontal adduc-tion test is performed by forward flexing the shoulder 90 degrees with subsequent cross-chest adduction of the arm (Figure 46-3D). Pain localized to the AC joint is considered a positive test result. If pain occurs posteriorly over the shoulder, a tight posterior capsule with impingement is sus-pected. O’Brien’s test is performed by forward flexing the arm 90 degrees and adducting the arm 10 degrees out of the sagittal plane of the body. The first part of the test is performed with the hand maximally pronated with the thumb pointed down. In this position, the patient is asked to resist as the examiner applies a downward force on the arm. If the test elicits pain, the patient is asked if the pain is on top of the shoulder or deep inside. Pain localized to the top of the shoulder indicates AC joint pain, and pain deep inside the shoulder indicates a superior labrum anterior posterior (SLAP) lesion. In the second part of the test, the patient is asked to supinate the hand maximally, while the examiner applies a downward force to the arm. If the patient notices significantly less pain, the test result is positive for a SLAP lesion. If the pain is unchanged and is located on top of the shoulder, the test result is positive for AC joint pathology.11
If the cause of AC joint tenderness is still in question, a lidocaine injection should be administered. The clinician should carefully avoid injecting the subacromial space by advancing the needle too far inferiorly through the AC joint; this can lead to false interpretation. Painful degenera-tive changes of the AC joint may exist concomitantly with subacromial impingement and should be evaluated thor-oughly when surgical treatment (i.e., distal clavicle exci-sion) is being considered.13
In patients with pain out of proportion to objective find-ings, other causes of shoulder pain should be sought, includ-ing calcific tendinitis, infection, reflex sympathetic dystrophy, and fracture. Patients with significant wasting of the supraspinatus and infraspinatus muscles and posterior shoulder pain, especially younger patients, may have supra-scapular neuropathy or brachial neuropathy (Parsonage-Turner syndrome).8,14
Patients with chronic cuff disease frequently have vari-able disuse atrophy of the supraspinatus and infraspinatus fossae; in cases of chronic massive cuff tears, atrophy and
diagnosis of non-neoplastic or noninfectious shoulder disease.
Scintigraphy may have a role in identifying patients with complete rotator cuff tears that proceed to cuff-tear arthrop-athy. This is an important distinction because patients with complete rotator cuff tears may do well, whereas those who develop progressive changes of cuff-tear arthropathy have progressive arthritis, pain, and significant functional impair-ment. Synovitis or calcium pyrophosphate deposition disease may be an important factor in the pathogenesis of cuff-tear arthropathy. In such cases, scintigraphy may show the increased blood flow and blood pooling associated with chronic synovitis.
Arthrography
Double-contrast arthrotomography (DCAT) can be used to evaluate problems of the rotator cuff, glenoid labrum, biceps tendon, and shoulder capsule.24-27Figure 46-5 shows normal
DCAT of the shoulder. Rotator cuff tears can be shown by single-contrast or double-contrast studies. Proponents of double-contrast arthrography believe that the extent of the tear, the preferred surgical approach, and the quality of the rotator cuff tissue are best determined by double-contrast studies.24-29 Arthrography without MRI or CT can be
mis-leading and may result in underestimation of the extent of a rotator cuff tear. Multidetector CT can enhance the accu-racy of diagnosing labral and rotator cuff tears, especially in patients for whom MRI is not possible (Figure 46-6).
Tears of the glenoid labrum without shoulder dislocation are sources of anterior shoulder pain in athletes.7 Glenoid
labrum tears (Figure 46-7), with or without associated gle-nohumeral subluxation, frequently can be identified by DCAT.27,28 Kneisl and colleagues30 described 55 patients
who underwent DCAT followed by diagnostic shoulder should be obtained, which includes anteroposterior views
with a 30-degree caudal tilt (Rockwood view), an outlet view (scapular Y with 10- to 15-degree caudal tilt), and an axillary view. Internal and external rotational views may be obtained if calcific tendinitis or instability is suspected. The Rockwood view can reveal any osteophytes off the anterior acromion and AC joint.20 In cases of traumatic injury, a
trauma series is obtained that includes a true anteroposterior view, a scapular Y view, and an axillary view. The axillary view is useful in assessing posterior or anterior subluxation of the humeral head. Additional views, such as the West Point view, which evaluates the glenoid for evidence of a bony Bankart lesion, or the Styker notch view, which assesses the humeral head for a Hill-Sachs lesion, may be obtained to assist evaluation if the diagnosis of instability is in doubt. Secondary impingement-type rotator cuff tendi-nitis may be caused by increased anterior translation with subluxation of the humeral head. In such cases, an axillary view or fluoroscopy can help show the subluxation.21,22
When AC joint pathology is suspected, a 10-degree, cephalic tilt view of the AC joint at 50% penetrance, as described by Zanca,23 should be obtained (Figure 46-4).
Stress views of the AC joint may be obtained by strapping 5 to 10 lb of weight to the patient’s forearms and determin-ing AC separation. Compardetermin-ing the coracoclavicular dis-tance of both shoulders may be helpful. When clinically indicated, cervical spine radiographs should be obtained to exclude cervical spondylosis as a cause of shoulder pain.
Scintigraphy
Tc 99m methyl diphosphonate (MDP) or gallium may be of diagnostic help in evaluating skeletal lesions around the shoulder joint. Bone scans generally are not helpful in the
Figure 46-4 Zanca view of the acromioclavicular joint is obtained with a 10-degree cephalic tilt and 50% penetrance. (From Rockwood CA Jr, Young DC: Disorders of the acromioclavicular joint. In Rockwood CA Jr, Matsen TA III, editors: The shoulder, Philadelphia, 1985, WB Saunders, pp 413–476.)
X-ray 10°
Figure 46-5 Normal double-contrast arthrography shows the inferior edge of the rotator cuff (RC) as it courses through the subacromial space to the greater tuberosity, the tendon of the long head of the biceps (BT), and the articular cartilage of the humeral head (AC).
BT
RC
bursography is not routinely used diagnostically, and, in our opinion, it is of little value in planning surgical procedures.
Computed Tomography
CT is helpful in evaluating the musculoskeletal system, and CT combined with contrast arthrography (CT-arthrography) has become a major diagnostic tool for the evaluation of glenoid labrum tears, loose bodies, and chondral lesions (Figure 46-9). Rafii and co-workers34 reported using
CT-arthrography in an evaluation of shoulder derangement. This study found 95% accuracy of CT-arthrography for investigating lesions of the labrum and articular surface.34
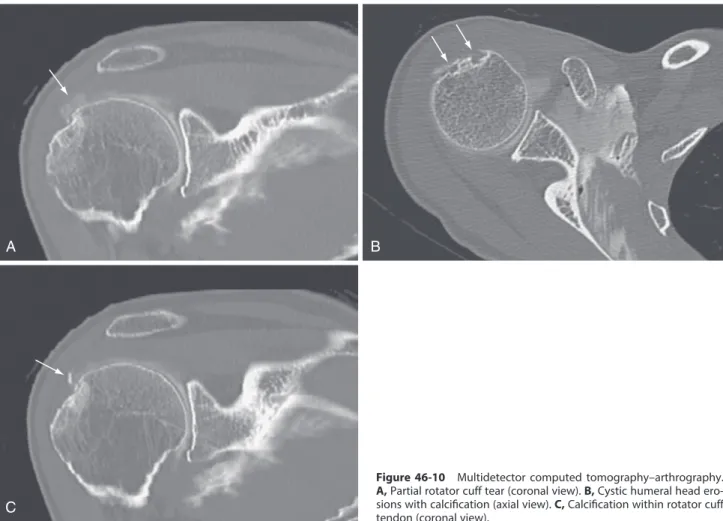
More recently, multidetector CT-arthrography scans have been used to evaluate partial cuff tears (Figure 46-10A), cystic lesions (Figure 46-10B), and calcific tendinopathy (Figure 46-10C).
Ultrasonography
Technologic improvements in ultrasound equipment have led to improved ultrasound study of the rotor cuff. The technique is noninvasive, is rapid, and involves no radiation exposure.30-32,35 The cuff is examined in the horizontal and
transverse planes with the arm in different positions to allow visualization of various areas of the cuff. These tech-niques generally provide visualization of the distal cuff, where most rotator cuff tears are located. Figure 46-11 shows normal and abnormal ultrasound images of the rotator cuff in longitudinal and transverse planes.
Several studies report high sensitivity and specificity for the diagnosis of a rotator cuff tear by ultrasound.32-35 The
specificity and sensitivity of the procedure are reported to be greater than 90% as determined by arthrographic and surgical correlations.34,35 This technique also has been used
for the postoperative evaluation of a rotator cuff repair and for evaluation of abnormalities of the biceps tendon.36-40
arthroscopy. DCAT predicted the arthroscopic findings in 76% of anterior labrum studies and 96% of posterior labrum studies. This test was 100% sensitive and 94% specific in diagnosing complete rotator cuff tears. Partial rotator cuff tears identified at arthroscopy were missed in 83% of patients undergoing DCAT. Investigators believed that DCAT was better in diagnosing intra-articular and cuff pathology in cases of instability than when pain alone was the presenting diagnosis.30
Shoulder arthrography can confirm a diagnosis of adhe-sive capsulitis by showing a contracted capsule with an obliterated axillary recess (Figure 46-8). The use of subacro-mial bursography has been beneficial in visualizing the outer surface of the rotator cuff and the subacromial space in cases of impingement.31,32 Fukuda and associates33 reported a
small series of younger patients (average age, 41.8 years) who underwent subacromial bursography after a negative glenohumeral arthrographic result. These patients showed pooling of contrast medium on the bursal side of a tear, which was confirmed at the time of surgery. Subacromial
Figure 46-6 Multidetector computed tomography revealing a superior labral tear of the shoulder.
Figure 46-7 Double-contrast arthrotomography shows a tear of the anterior-inferior portion of the glenoid labrum (arrow).
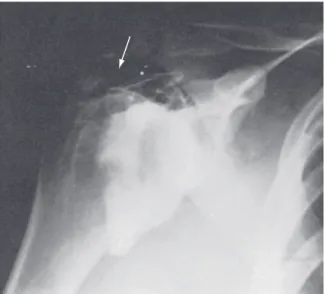
Figure 46-8 Double-contrast arthrography of a patient with calcific tendinitis (arrow) and adhesive capsulitis. Notice the contracted capsule with diminution of the synovial space and obliteration of the axillary recess.
better than the accuracy of other diagnostic modalities of the time. With technologic advances in fiberoptics, video output, and arthroscopic instrumentation, the use of arthros-copy to diagnose and treat shoulder problems exponentially increased to include procedures previously used only for open techniques.44
Compared with DCAT, arthroscopy is more accurate in the diagnosis of intra-articular lesions associated with a painful shoulder.30 An additional benefit is that arthroscopy
can be used to diagnose and treat shoulder problems of the glenohumeral joint and the subacromial region. With increased accuracy of MRI-arthrography in detecting partial cuff tears and labral lesions, diagnostic shoulder arthroscopy has become less common in the absence of clear indications and specific treatment plans. In combination with a detailed history and physical examination, and along with examina-tion under anesthesia, shoulder arthroscopy has been helpful in the diagnosis of chronic instability patterns of the gleno-humeral joint.44-47
The indications and usefulness of shoulder arthroscopy in the treatment of common pathologic conditions have continued to increase as the technology improves, and as understanding of the pathophysiology of shoulder problems grows. Shoulder arthroscopy has been used routinely to confirm and treat SLAP lesions, labral tears, partial cuff
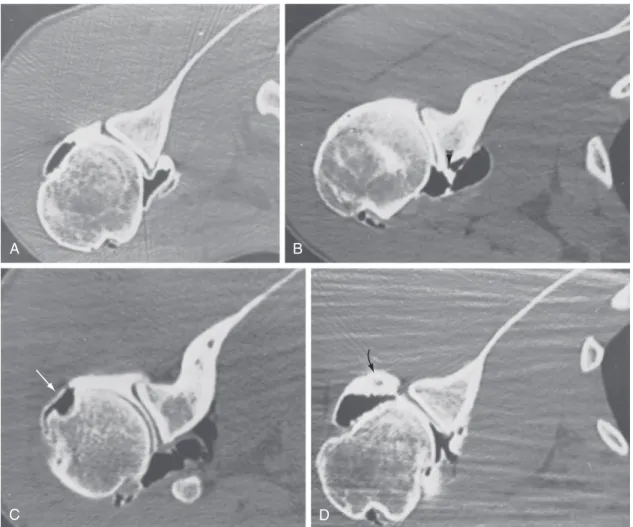
Figure 46-9 CT-arthrography of the shoulder. A, Normal findings. B, Tear of the anterior glenoid labrum. C, Large defect of the articular surface of the posterior portion of the humeral head (Hill-Sachs lesion) (arrow). D, Loose body in the posterior recess (arrow).
A B
C D
Gardelin and Perin41 reported ultrasound to be 96%
sen-sitive in determining rotator cuff and biceps tendon pathol-ogy. Mack and associates36 found ultrasound to be valuable
in evaluating postoperative patients with recurrent shoulder symptoms. In a prospective study, Hodler and colleagues39
compared ultrasound with MRI and arthrography in evalu-ating rotator cuff lesions in 24 shoulders. Ultrasound identi-fied 14 of 15 torn cuffs, MRI identiidenti-fied 10 of 15, and arthrography identified 15 of 15.39 Ultrasound identified 7
of 9 intact rotator cuffs, whereas MRI was accurate in 8 of 9 intact cuffs.39 Vestring and colleagues42 found ultrasound
to be as accurate as MRI in the diagnosis of humeral head defects and joint effusions, but inferior to MRI in the diag-nosis of labrum lesions, rotator cuff lesions, subacromial spurs, and synovial inflammatory disease. In the hands of an experienced sonographer, ultrasound may be the most cost-effective test for the initial evaluation of a rotator cuff injury, but most surgeons require CT-arthrography or MRI confirmation before beginning surgical exploration.36,39,41-43
Arthroscopy
The use of arthroscopy for the diagnosis of shoulder pathol-ogy increased in the 1980s, in part because of its accuracy, which was far greater than that of clinical examination and
to be as accurate as CT-arthrography in the diagnosis of abnormalities of the glenoid labrum.53
Characteristic MRI findings in rotator cuff tears include a hypointense gap within the supraspinatus muscle tendon complex on T1-weighted films, absence of a demonstrable supraspinatus tendon with narrowing of the subacromial space, and an increased signal within the supraspinatus tendon on T2-weighted images.54 Seeger and colleagues,55
reporting the results of 170 MRI studies, found that T1-weighted images were highly sensitive for identifying abnormalities within the supraspinatus tendon, but T2-weighted images were required to differentiate tendinitis from a small supraspinatus tendon tear. Large full-thickness tears could be identified, however, on T1-weighted and T2-weighted images. Figure 46-12 depicts common shoul-der pathology as seen by MRI. MRI is almost as sensitive as and is more specific than scintigraphy in the diagnosis of osteonecrosis and neoplastic lesions around the shoulder.
Electromyography and Nerve Conduction Velocity Studies
EMG and nerve conduction velocity studies can help dif-ferentiate shoulder pain from pain of neurogenic origin. They also may be beneficial in determining the localization of neurogenic pain to a particular cervical root, the brachial plexus, or a peripheral nerve.56,57
tears, refractory adhesive capsulitis, partial biceps tendon tears, and multidirectional instability. Other conditions that are routinely treated arthroscopically include rotator cuff tears, glenohumeral instability, AC joint pathology, loose bodies, sepsis, osteochondritis dissecans, synovitis, chondral lesions, subacromial impingement, and calcific tendinitis.7,13,44,47
Magnetic Resonance Imaging
MRI has been used to diagnose partial-thickness and full-thickness rotator cuff tears, biceps tendon tears, impinge-ment of the rotator cuff, synovitis, articular cartilage damage, and labral pathology associated with glenohumeral instability.48-50 In rheumatoid arthritis, MRI is reported to
be more sensitive than plain radiographs in determining soft tissue abnormalities and osseous abnormalities of the glenoid and humeral head.51
One of the most valuable diagnostic uses of MRI is in rotator cuff pathology. Morrison and Offstein52 studied 100
patients with chronic subacromial impingement syndrome using arthrography and MRI. MRI was 100% sensitive but only 88% specific in confirming arthrography-proven rotator cuff tears. Nelson and associates53 studied 21 patients with
shoulder pain and found MRI to be more accurate than CT-arthrography or ultrasound in identifying partial-thickness cuff tears. These investigators also reported MRI
A B
C
Figure 46-10 Multidetector computed tomography–arthrography. A, Partial rotator cuff tear (coronal view). B, Cystic humeral head ero-sions with calcification (axial view). C, Calcification within rotator cuff tendon (coronal view).
Potential Diagnostic Tests
Table 46-2 lists reimbursement and charges for various shoulder diagnostic tests based on 2011 Medicare fee sched-ules and 2011 charges at a single institution. The choice of a specific test depends on its sensitivity, specificity, and cost-benefit analysis. History and physical examination are the most important factors in establishing diagnosis of the painful shoulder. Plain radiographs (three views) should be the first radiographic tests performed. Although not as sen-sitive as the more sophisticated tests, plain radiographs can identify arthritic change, calcific tendinitis, established osteonecrosis, and most neoplasms.
If intra-articular pathology (e.g., labrum tear, capsular tear, loose body, chondral defect) is suspected, MRI-arthrography is preferable to CT-MRI-arthrography. In diagnos-ing acute rotator cuff tears in a younger patient, ultrasound is the most cost-effective test to confirm a clinical suspicion. In cases of impingement syndrome, MRI is sensitive, but it is difficult to differentiate tendinitis, partial tears, and small complete tears without MRI-arthrography. Orthopedic sur-geons prefer MRI-arthrography for verification of labral tears or partial rotator cuff tears. In the case of a suspected full-thickness rotator cuff tear, MRI is preferred to deter-mine the size of the tear, the amount of muscle atrophy and tendon retraction, and the quality of remaining tissue for repair.
Injection
Injection of local anesthetics and glucocorticoids is a useful technique for the diagnosis and treatment of shoulder pain.58
The physician must have a thorough understanding of the anatomy of the shoulder girdle and a presumptive diagnosis to direct the injection properly. Injection of referred pain areas may be misleading. In a patient with lateral arm pain secondary to deltoid bursal involvement from calcific ten-dinitis of the supraspinatus tendon, injection should be performed in the subacromial space, rather than in the area of referred pain in the deltoid muscle. It is often better to use a posterior or lateral subacromial approach when injecting a rotator cuff tendinitis in a patient with anterior impingement symptoms because it is easier to enter the subacromial region posteriorly or laterally, and this approach is less traumatic for contracted anterior structures.
The instillation of rapidly acting local anesthetics can be beneficial in determining the source of shoulder pain. Oblit-eration of pain by injection of a local anesthetic along the bicipital groove can confirm a diagnosis of bicipital tendi-nitis. The use of local anesthetics is less helpful when the subacromial space is injected because of its extensive com-munication with the rest of the shoulder girdle, but relief of symptoms by such an injection can exclude pain from con-ditions such as cervical radiculopathy or entrapment neuropathy.
Figure 46-11 A, Normal longitudinal view of rotator cuff by ultrasound shows the humeral head (1), the superior articular surface (2), the rotator cuff (3), the deltoid tendon (4), and tapering of the cuff to its insertion on the greater tuberosity (5). B, Transverse view of a normal intact rotator cuff covering the humeral head. C, Rotator cuff tear, showing a hypoechoic area (arrow) on a longitudinal view. D, Rotator cuff tear, showing hypoechoic area (arrows) on a transverse view.
A B C D 4 3 2 1 4 3 2 1 5
acromion, coracoacromial ligament, coracoid process, or AC joint on the rotator cuff as it passes beneath them during glenohumeral motion. The function of the posterior rotator cuff is to abduct and externally rotate the humerus. The cuff with the biceps tendon serves as a humeral head depressor to maintain the head centered within the glenoid fossa as the cuff and to use the deltoid to elevate the arm.59-61
Controversy continues, however, as to the exact cause of impingement, that is, whether it is a primary, intrinsic, degenerative event within the tendon with superior migration of the head on arm elevation and secondary
INTRINSIC FACTORS CAUSING
SHOULDER PAIN
Periarticular Disorders
Shoulder Impingement and Rotator Cuff Tendinopathy
One of the most common nontraumatic causes of shoulder pain is impingement with rotator cuff tendinopathy. In 1972, Neer9 described his results of 100 anatomic shoulder
dissections and coined the term impingement syndrome. Impingement may be defined as the encroachment of the
Figure 46-12 A, Magnetic resonance imaging (MRI) proton density–weighted coronal view shows the supraspinatus tendon as a black band (A) that has an increased signal as it nears insertion on the greater tuberosity (B). B, Similar view in a T2-weighted image shows increased signal as gray (arrow), indicating a partial-thickness tear or tendinitis. C, MRI proton density–weighted coronal view shows abrupt end of supraspinatus tendon as it courses right to left (A). From A to B is an area of increased signal followed by a short portion of tendon (B) inserting at the greater tuber-osity. D, Similar view in a T2-weighted image shows increased signal as white (fluid density), indicating fluid in the gap of a complete rotator cuff tear. E, MR arthrography shows a normal rotator cuff. F, MR arthrography shows a chronic cuff tear with retraction.
A B C D E F A B A B A B
on the affected extremity and is exacerbated by overhead activity. Tenderness on palpation may be elicited over the greater tuberosity and the long head of the biceps within the bicipital groove, indicating an associated biceps tendi-nitis. In cases with concomitant degenerative changes in the AC joint, tenderness may be noted on palpation over the AC joint, as an offending osteophyte impinges on the rotator cuff beneath.
The impingement sign as described by Neer9 (Figure
46-13) is useful in the diagnosis of rotator cuff tendinopathy. The patient often describes a catch as the arm is brought into the overhead position. The patient may be observed to raise the arm by abduction and external rotation to clear the greater tuberosity of the acromion, bypassing the painful area. A typical painful arc usually occurs between 70 degrees and 110 degrees of abduction. Neer9 also described an
impingement test that involves injection of lidocaine into the subacromial bursa. Relief of pain is a positive impinge-ment test result and usually indicates rotator cuff origin of the shoulder pain.
impingement on the acromion, or purely mechanical attri-tion of the tendon with primary impingement against the acromion. The mechanical impingement of the rotator cuff may be influenced by variations in the shape and slope of the acromion.62,63 The supraspinatus outlet may become
narrowed from proliferative spur formation of the acromion or degenerative changes in the AC joint. These changes, along with intrinsic degenerative changes of the rotator cuff, may lead to rotator cuff tear, but the exact pathogenesis remains controversial. Many studies have found a strong correlation between degenerative hypertrophic spur forma-tion, with its resulting narrowing of the supraspinatus outlet, and the presence of full-thickness cuff tears,9,19,64-71 but
clini-cal studies have failed to confirm whether hypertrophic changes in the coracoacromial arch are caused by the cuff lesions, or whether these changes themselves cause the lesions.
Neer9 developed a staging system for description of
impingement lesions of the shoulder. A stage I lesion involves edema and hemorrhage of the rotator cuff and is typically found in individuals younger than 25 years who are active in overhead athletics. The condition usually responds to conservative treatment that includes rest, anti-inflammatory medication, and physical therapy. Stage II lesions usually occur in the 30s or 40s and represent the biologic response of fibrosis and thickening of the tendon after repeated episodes of mechanical impingement over time. Lesions are treated conservatively, as in stage I, but attacks may recur. If symptoms persist despite adequate con-servative management for longer than 6 to 12 months, surgical intervention is warranted. Stage III lesions involve rotator cuff tears, biceps tendon rupture, and bone changes, and they rarely occur before age 40. Patients may present with pain, weakness, or supraspinatus atrophy, depending on the chronicity of the tear. Surgical treatment depends on the patient’s age, loss of function, weakness, and pain.
Patients usually present to the clinician with a complaint of pain that has failed to resolve after a variable period. Pain can be sudden and incapacitating in cases of traumatic cuff tears, or more commonly may manifest as a dull ache in cases of chronic impingement. Pain usually is located over the anterior and lateral aspects of the shoulder and may radiate into the lateral deltoid. It may worsen with sleeping
Table 46-2 Relative Costs of Shoulder Diagnostic Procedure in 2011
Procedure Initial Fee (USD) Technical Fee (USD) Interpretation Fee (USD)
Medicare B Fee Schedule
Initial office visit (30 min) 154.00
Plain radiography (3 views) 36.28 23.09
Arthrography 156.08 34.07
Ultrasonography 74.70 41.62
Magnetic resonance imaging 531.28 81.42
Computed tomography 233.06 66.77
Tomography 78.53 39.69
Institutional Charges
Initial office visit (30 min) 196.00
Plain radiography (3 views) 371.00 36.00
Arthrography 533.00 302.00
Ultrasonography 801.00 119.00
Magnetic resonance imaging 3831.00 350.00
Computed tomography 1860.00 203.00
USD, U.S. dollars.
Figure 46-13 The impingement sign is elicited by forced forward ele-vation of the arm. Pain results as the greater tuberosity impinges on the acromion. The examiner’s hand prevents scapular rotation. This maneu-ver may be positive in other periarticular disorders. (From Neer CS II: Impingement lesions, Clin Orthop Relat Res [173]:70, 1983.)
lesions, with many investigators reporting high success rates in treating impingement syndrome and rotator cuff tears.74-77
Reported results show good and excellent relief of symptoms in 71% to 87% of patients treated by the open surgical procedure.78-81
In 1985, Ellman45 described the technique of arthroscopic
subacromial decompression. His initial results46 and the
results of others are comparable with those of open surgical techniques.47,82 Arthroscopic subacromial decompression
has become a widely accepted treatment for refractory stage II and III impingement lesions. The procedure can be done as outpatient surgery, and because no deltoid is detached, as with the open technique, the procedure facilitates rehabili-tation and increases overall recovery rates.
Calcific Tendinitis
Calcific tendinitis is a painful condition around the rotator cuff that is associated with deposition of calcium salts, pri-marily hydroxyapatite.83-85 The cause of calcific tendinitis is
unknown. The commonly accepted cause is degeneration of the tendon, which leads to calcification through a dystro-phic process.85 A common clinicopathologic correlation is
seen in three distinct phases of the disease process: the precalcific or formative phase, which can be relatively pain-less; the calcific phase, which tends to be quiescent and may last months to years; and the resorptive or postcalcific phase, which tends to be painful, as calcium crystals are resorbed.83
Although it is more common in the right shoulder, at least a 6% incidence of bilaterality has been reported. Patients with bilateral shoulder involvement often have the syn-drome of calcific periarthritis, in which calcium hydroxy-apatite crystals are found at multiple sites.86 Patients usually
present with impingement-type pain in the affected shoul-der during overhead activity. The pain may seem to be out of proportion to any objective physical findings. The patient may describe difficulty sleeping on the shoulder and trouble falling asleep. Symptoms may last a few weeks or a few months.
The incidence of calcific tendinitis varies in the litera-ture among asymptomatic individuals from 2.7% to 20%. Most calcification occurs in the supraspinatus tendon, and 57% to 76.7% of patients are women. The average age of patients is 40 to 50 years.83,87
Codman1 pointed out the localization of calcification
within the tendon of the supraspinatus. He provided a detailed description of the symptoms and the natural history of this condition. In describing the phases of pain, spasm, limitation of motion, and atrophy, he noted the lack of cor-relation between symptoms and the size of the calcific deposit. According to Codman, the natural history includes degeneration of the supraspinatus tendon, calcification, and eventual rupture into the subacromial bursa. During the latter phase, pain and decreased motion can lead to adhe-sive capsulitis (see Figure 46-8).
Several factors may affect localization of calcium within the supraspinatus. Many patients have an early stage of impingement, which compresses the supraspinatus tendon on the anterior portion of the acromion.9,19 This
long-standing impingement may lead to local degeneration of tendon fibers. In patients without impingement, be normal or may reveal a hooked acromion. As the disease
progresses, sclerosis, cyst formation, and sclerosis of the anterior third of the acromion and the greater tuberosity may be observed. An anterior acromial traction spur may appear on the undersurface of the acromion lateral to the AC joint and represents contracture of the coracoacromial ligament. Late radiographic findings include narrowing of the acromiohumeral gap, superior subluxation of the humeral head in relation to the glenoid, and erosive changes in the anterior acromion.71 Arthrography, MRI, and
ultra-sound may be helpful in diagnosing a full-thickness tear of the rotator cuff in association with stage III disease. In some cases of chronic large rotator cuff tears, proximal migration of the humeral head leads to a pattern of degenerative arthritis termed cuff-tear arthropathy.
The choice of treatment and frequently its result are functions of the stage of the impingement and the response to pain. In stage I disease, in which little mechanical impingement occurs, most patients respond to rest. It is important to avoid immobilizing the shoulder for any period because contraction of the shoulder capsule and periarticu-lar structures can produce an adhesive capsulitis. After a period of rest, a progressive program of stretching and strengthening exercises generally restores the shoulder to normal function. Use of aspirin and other nonsteroidal anti-inflammatory drugs (NSAIDs) may shorten the symptom-atic period. Modalities such as ultrasound, neuroprobe, and transcutaneous electrical nerve stimulation generally are not helpful. Patients with stage I or II disease may have a dramatic response to local injection of glucocorticosteroids and local anesthetic agents. For stage II disease in which fibrosis and thickening occur anteriorly, it is frequently better to inject through a posterior approach. We prefer a combination of 3 mL of 1% lidocaine (Xylocaine), 3 mL of 0.5% bupivacaine, and 20 mg of triamcinolone. This injec-tion combines a short-acting anesthetic to help confirm the diagnosis, a longer-acting anesthetic for analgesic purposes, and a steroid preparation in a depot form.
An integrated program of occupational and physical therapy often precludes the need for surgery in patients with stage II disease. Job modification for individuals with impingement syndrome caused by overuse may alleviate symptoms. Businesses are becoming increasingly aware of the cost savings associated with proper job ergonomics.72,73
The initial rehabilitation in stage II impingement con-sists of cessation of repetitive overhand activity. Ice, NSAIDs, and local injections also may be beneficial. Initial physical therapy includes passive, active-assisted, and active range of motion combined with stretching and mobilization exercises to prevent contracture. As pain and inflammation subside, isometric or isotonic exercises are used to strengthen the rotator cuff musculature. Isokinetic training at variable speeds and in variable positions is instituted before the patient is returned to full activity. For patients with a job-related injury, it is crucial to review and modify job mechan-ics to prevent recurrent episodes that can cause further disability and may precipitate the need for surgery.72
Neer19 suggested that a patient with refractory stage II
disease may respond to division of the coracoacromial liga-ment and bursectomy of the subacromial bursa. Open ante-rior acromioplasty as described by Neer has become accepted
and cellularity of the tendon, along with changes in the collagen fibers of the tendon that occur with aging.
Loss of motion with subsequent capsular tightness, par-ticularly in the posterior capsule, may lead to cephalad migration of the humeral head, with subsequent impinge-ment of the cuff under the coracoacromial arch.96
Rehabili-tation exercises stress regaining a normal range of motion. To achieve full, painless motion, the normal relationship of glenohumeral to scapulothoracic motion must be achieved.16,17,97
Diagnosis
History. Patients with nontraumatic tears of the rotator cuff report symptoms of chronic impingement. Loss of motion and a feeling of stiffness are often noted with extremes of motion, along with difficulty during activities of daily living, such as combing the hair, hooking a bra strap, putting on a shirt or coat, and reaching into the back pocket. In chronic cases of cuff tendinopathy, loss of motion usually occurs. Limitation of internal rotation occurs ini-tially, is caused by posterior capsular contracture, and is often associated with posterior shoulder pain with adduc-tion of the ipsilateral shoulder. Further shoulder impinge-ment occurs with forward flexion because of superior migration of the humeral head against the anterior inferior acromion. This upward translation is analogous to the action of a yo-yo climbing on a string.96,98 Over time, loss
of forward flexion, abduction, and external rotation occurs with passive and active motion of the shoulder.
Imaging. In acute cases, a history of trauma, such as a fall onto the affected shoulder, may be reported. In cases involving an anterior shoulder dislocation with sub-sequent profound weakness of the rotator cuff, a large cuff tear or a greater tuberosity avulsion should be suspected, in addition to axillary nerve palsy. In younger patients, traumatic failure of the cuff under tensile overload may result in cuff failure caused by forced adduction of the affected shoulder or active abduction against resistance, and this may occur with traumatic dislocation. Repetitive tensile overload also can result in partial rotator cuff tears in an overhead athlete.
Plain radiographs are used in initial evaluation of impingement-type shoulder pain with cuff tendinopathy. An impingement series should be ordered, including an anteroposterior radiograph with a 30-degree cephalic tilt (Rockwood view), which can reveal osteophytes of the anterior os acromion and AC joint; a scapular Y view with a 10-degree cephalic tilt (supraspinatus outlet view), which can evaluate the type of acromion and reveal anterior and AC osteophytes; and an axillary view, which can evaluate the acromion for possible os acromionale. Calcific deposits within the rotator cuff tendon can be viewed best with rotational anteroposterior radiographs. Cuff arthropathy should be suspected if the acromial-humeral distance is less than 7 mm, or with the presence of cyst formation within the greater tuberosity, humeral head osteopenia, sclerosis around the greater tuberosity, or humeral head collapse. In advanced stages of cuff arthropathy, complete loss of gleno-humeral joint space may be seen with superior migration and abutment of the humeral head against the undersurface of the acromion.59
localization of calcium within the supraspinatus may be related to the blood supply of the rotator cuff, which nor-mally is derived from an anastomotic network of vessels from the greater tuberosity or from the bellies of the short rotator muscles.84 The watershed of these sources is just
medial to the tendinous attachment of the supraspinatus.88
Rathburn and Macnab89 referred to this watershed as the
critical zone and pointed out that during abduction this area was rendered ischemic.
Treatment of calcific tendinitis depends on the clinical presentation and the presence of associated impingement. Patients can have an acute inflammatory reaction that may resemble gout. The acute inflammation can be treated with local glucocorticoid injection, NSAIDs, or both. Ultra-sound may be beneficial. If impingement is associated, treat-ment depends on the stage at presentation. The radiographic appearance of the calcification can direct and perhaps predict the response to therapy. In the resorptive state, deposits appear floccular, suggesting that the process is in the phase of repair, and that a conservative program is indicated.
Patients with discrete calcification and perhaps associ-ated adhesive capsulitis (see Figure 46-8) may be at a stable phase, in which calcium produces a mechanical block and is unlikely to be resorbed. For these patients, mechanical removal of calcific deposits and correction of associated pathologic lesions may be necessary.90-92 Percutaneous
dis-ruption of calcified areas may be performed using a needle directed by fluoroscopy. This technique allows lavage and injection, but does not treat associated impingement. Sub-acromial arthroscopy allows mechanical débridement of calcific deposits under direct visualization. This technique can be combined with arthroscopic removal of the inflamed bursa and decompression of associated impingement. Improved results have been noted with complete removal of calcific deposits.93 In many cases of refractory calcific
tendinitis associated with impingement, open or arthro-scopic acromioplasty, subacromial bursectomy, and decom-pression are indicated.
Rotator Cuff Tear
Pathophysiology
Spontaneous tear of the rotator cuff in an otherwise normal individual is rare.19 It can occur in patients with rheumatoid
arthritis or systemic lupus erythematosus as part of the pathologic process with invasion from underlying pannus. Metabolic conditions such as renal osteodystrophy and agents such as glucocorticoids occasionally are associated with cuff tears. Most patients report a traumatic episode, such as falling on an outstretched arm or lifting a heavy object. The usual presenting symptoms are pain and weak-ness of abduction and external rotation. Crepitus and even a palpable defect may be associated. Long-standing tears generally are associated with atrophy of the supraspinatus and infraspinatus muscles. It may be difficult to differentiate a painful tendinitis from a partial-thickness or a small full-thickness cuff tear.
Controversy continues about the exact cause of cuff ten-dinopathy.88,92,94,95 Most likely, the pathophysiology involves
injection into the cuff tendon is to be avoided. If the patient fails to improve after 3 months of conservative treatment, or does not continue to improve after three sequential injec-tions, surgical options should be discussed.
The mainstay of conservative therapy is exercise. Reha-bilitation stresses pain relief with exercises aimed at restor-ing shoulder motion and strengthenrestor-ing remainrestor-ing cuff muscles, deltoid, and scapular stabilizers. Therapy can be divided into three phases. The goals of the initial phase of therapy are to relieve pain and restore shoulder motion. Motion therapy includes pendulum exercises, passive motion with use of a wand with assistance of the uninvolved shoulder, an overhead pulley system, and posterior capsular stretching. The arc of motion is gradually increased and is guided by the patient’s discomfort to avoid painful impinge-ment arcs.
The second phase of therapy is entered after the patient has return of motion and little discomfort with overhead activity. Emphasis is placed on strengthening the remaining rotator cuff musculature and deltoid and periscapular muscles. Strengthening with elastic surgical tubing provides variable degrees of resistance, depending on the size of the tubing. Initial strengthening is performed out of the impingement arc (70 to 120 degrees of shoulder flexion). The goal of this phase is to strengthen the shoulder to prevent dynamic proximal humeral migration with impingement during active shoulder elevation.59,61 Normal
shoulder kinematics relies on combined and synchronous glenohumeral flexion and scapular rotation.60,92 In addition
to strengthening the cuff and deltoid, the scapular rotators, including the trapezius and the serratus anterior muscles, are emphasized.107
After the patient has successfully completed phase two of the rehabilitation program with minimal symptoms and good shoulder function, the final phase is entered. Phase three is characterized by a gradual return to normal over-head activities, including work and sporting activities. This part of the rehabilitation program should be tailored to the individual patient’s needs and the demands placed on the shoulder.
Surgical Treatment. A Cochrane review of the effec-tiveness of surgery for rotator cuff disease failed to reach any firm conclusions about the effectiveness or safety of rotator cuff surgery.108
Severity and duration of pain are the primary indications for surgical intervention in a rotator cuff tear. Other factors important in surgical decision making include shoulder dominance, activity level, physiologic age, acuteness of the tear, degree of tear, loss of function, amount of tendon retraction, and fatty atrophy of the remaining cuff musculature.
A systematic review of indications for rotator cuff surgery found that earlier surgical intervention may be needed for patients with cuff tears with weakness and significant func-tional disability. In addition, older chronologic age did not portend a worse outcome; however, pending workman’s compensation claims, it did negatively affect treatment results.109
Acute Tears. Acute tears of the rotator cuff can be treated with conservative measures of periscapular and cuff strengthening along with capsular stretching to restore “gold standard” for diagnosing full-thickness and
partial-thickness rotator cuff tears, with greater than 90% sensitiv-ity and specificsensitiv-ity.33,99 Currently, arthrography with CT or
MRI is routinely used to diagnose rotator cuff pathology, including full-thickness and partial-thickness tears.
Ultrasonography has been accurate in the diagnosis of full-thickness rotator cuff tears.39,100-103 Ultrasonography
offers the advantages of being inexpensive and noninvasive, but disadvantages include unproven effectiveness in deter-mining subacromial impingement, capsular and labral abnormalities, and partial cuff tears. The procedure and its results are technician dependent. Ultrasonography may have a useful role in determining the postoperative integrity of the cuff repair.38
MRI has been invaluable in evaluating rotator cuff tears. Sensitivity and specificity of MRI for diagnosing full-thickness cuff tears are 100% and 95%.104 Through the use
of gadolinium or saline, partial tears that are otherwise dif-ficult to detect with conventional imaging can be detected. Diagnosing cuff tears with MRI usually is based on dis-continuity of the tendon on T1-weighted images and con-sistency with fluid signal on T2-weighted images. Ancillary findings include fluid in the subacromial space on T2-weighted images, loss of the subacromial fat plane on T1-weighted images, and proliferative spur formation of the acromion or AC joint. Large, chronic cuff tears also may be associated with cephalad migration of the humeral head and fatty atrophy of the spinatus muscle. Periarticular soft tissues, including the capsulolabral complex and the biceps tendon, as well as the rotator cuff can be thoroughly exam-ined. The degree of tear and tendon retraction and evidence of muscle atrophy can be evaluated, all of which are crucial in preoperative planning for possible cuff repair.
Treatment
Nonsurgical Treatment. Codman and Akerson64
rec-ommended early operative repair for acute full-thickness rotator cuff tears and reported the first documented repair in 1911. McLaughlin66 recommended early repair in cases
of grossly displaced tuberosity fractures or massive tears. Several other clinical studies have supported the concept that a full-thickness tear does not preclude good shoulder function. DePalma105 reported that 90% of patients
with rotator cuff tears responded to conservative measures, such as rest, analgesics, anti-inflammatory agents, and physiotherapy.
The reported percentage of patients responding to non-surgical treatment in the literature varies from 33% to 90%.3,18,106 Conservative treatment includes pain control
with NSAIDs, ultrasound, heat before shoulder stretching and exercise, and ice after overhead activity. Deep massage therapy is employed to reduce trigger point tenderness within the trapezius, levator scapulae, and periscapular muscles. Patients on long-term anti-inflammatory medica-tions are monitored periodically for evidence of gastrointes-tinal bleeding and for hepatic or renal toxicity. Opiate-based drugs are used only in the acute setting, such as after a fall, or in the perioperative period.
Steroid and local anesthetic injections are used when the patient has significant pain that prohibits rehabilitation.