EFFECTIVENESS OF ACUPUNCTURE FOR THE TREATMENT OF CHRONIC DAILY HEADACHE: A SHAM-CONTROLLED CLINICAL TRIAL
AYSESOZEN1, MUSTAFAYILMAZ1, H. RIFATKOYUNCUOGLU2, VEDATALIYUREKLI2, ERTUGRULUZAR2, SULEYMANKUTLUHAN2 1Mugla University Faculty of Medicine, Department of Neurology, Mugla, Turkey - 2Suleyman Demirel University Faculty of Medicine, Department of Neurology, Isparta, Turkey
[L’agopuntura nel trattamento della cefalea cronica quotidiana]
Introduction
Headache is one of the most common health problems(1). Recurrent headaches occur in up to 80%
of the adult population(2). If headache is not related to
another medical condition, and lasts for at least 15 days per month for a minimum of 3 months, it is called “chronic daily headache” (CDH). CDH can cause significant disruption in daily life and a con-siderable amount of pain(3). Many people endure the
pain of CDH until they are treated with some drug. The treatment may minimize, or control, the pain or eradicate it completely. In addition, drug treatment may cause even more headaches, so patients should limit the using of pain medication for CDH(4).
Because drug treatments are only partially effective, and can have side effects for people suffering from
headaches, an alternative treatment is needed for managing CDH(5).
Acupuncture has been used in traditional Chinese medicine for thousands of years and is accepted as a viable alternative for treating headache(6). There are traditional and scientific
expla-nations that explain its possible mechanism of action. Many clinicians have turned to alternative therapies when conventional therapies have not enough, exact-ly(7). Today acupuncture has been used to treat many
diseases such as rheumatic diseases, cancer, dysmen-orrhea, stroke, migraine, insomnia, and tinnitus(8-10).
In the last decades, acupuncture has increasingly been used for the treatment of chronic pain. It was mentioned that acupuncture may be used to provide sustained relief from headaches.
ABSTRACT
Objectives: Acupuncture is a traditional method for the treatment of many pain conditions, but the effectiveness of
acupunc-ture remains controversial on chronic daily headache (CDH). We evaluated the efficacy of real acupuncacupunc-ture (RA) at CDH compared with sham acupuncture (SA).
Method: The patients with CDH were selected from a Neurology Department of University Hospital. A total of 56 patients
with CDH were randomly assigned to two treatment groups. RA (n=34) and SA (n=22) groups were enrolled. The acupuncture treatment was terminated after 3 months.
Results: We found significant differences when compared visual analog scale (VAS) scores after first and third month of
treat-ment in RA and SA groups (p=0.007, p=0.021, respectively). The headache intensity was lower in RA group than SA group. The fre-quency of headache decreased in both groups. There was significant difference between the RA and SA groups for mean monthly number of headaches after first and third month of treatment (p=0.001, p=0.002, respectively). The effectiveness of acupuncture treatment was 69% in the RA group and 29% in the SA group.
Conclusion: Our study confirmed that both the acupuncture and SA might be a beneficial and effective treatment for the CDH.
However, the real acupuncture induced more effect on modulating intensity and duration of headache than in sham acupuncture.
Key words: Chronic daily headache, real acupuncture, sham acupuncture.
While acupuncture is commonly used to treat headache; acupuncture’s effects are contradictory in literature.
Some studies indicate that acupuncture is effective, but other trials report no effect(11-13). We
undertook a general overview of the more common-ly used acupuncture routines for the treatment of CDH. Most studies have focused mainly on the effectiveness of acupuncture for headache without using SA. The aim of the study was to investigate the efficacy and tolerability of RA and SA treat-ments in patients with CDH over three months.
Material and method Setting
The local ethics committee of Suleyman Demirel University approved the study. We conduct-ed this study according to monocenter, single-blind randomized control. We applied the guidelines of the International Headache Society for conducting clini-cal trials involving patients with CDH(14). Patients
with CDH selected for this study were treated in the Neurology Department of Suleyman Demirel University Hospital, Isparta, Turkey.
Subjects
All participants were informed about the study and written informed consent was obtained. After the local ethical committee approval, we included as subjects people who met the following criteria: headache not related to another medical condition 15 days or more every month for at least three months; age 18-60 years. We excluded patients who had headache due to organic disorders including cere-brovascular disease; tumor; severe depression; psy-chosis; irregular hypertension; anemia; bleeding dis-orders; and liver, kidney or thyroid disease. The clas-sification of headache was based on ICHD-II(14).
We performed a Beck Depression Inventory (BDI) on all the patients to investigate psychological comorbidity. BDI is a 21-item, self-report rating inventory that measures characteristic attitudes and symptoms of depression. Scores from 24 to 63 indi-cate severe depression.
We excluded patients with severe depression. Our research period lasted 17 weeks for each patient. In total, 56 patients with CDH were randomly divid-ed into two groups: real acupuncture (RA) group (n=34) and sham acupuncture (SA) (n=34) group. A
4-week baseline period was followed by randomiza-tion. We selected the acupuncture points for the first group according to traditional Chinese acupuncture and for second group, anywhere outside of these points. We used acupuncture needles for both groups. Sterile, disposable, steel needles with length of 0.13x0.32 mm (Wujiang Jia Chan, Wujiang City, China) were used.
Intervention
RA and SA has been defined in World Health Organization (WHO) Guidelines for Clinical Research on Acupuncture(15). The needles were
inserted at acupuncture points (depth 3-10 mm, LI4, DU-16, GV-24, GB-14, UB-2, SJ-23, SJ-22) for RA. A maximum of 15 points was used; the needles were left in place for 20 minutes for RA and SA groups. SA was performed with the needles inserted away from acupoints(16). During the SA treatment, the same
points were used for standardization for SA group. During the first two weeks, acupuncture was per-formed for 20 minutes each day, 5 days per week. Thus, a total of 400 minutes of acupuncture were given over 5 weeks. Then, the acupuncture treatment was performed for three months.
After the first month and at the end of the study, patients were asked to report their current pain, mean monthly number of headaches, pain intensity, dura-tion of headache, nausea, analgesic usage and response to analgesic, and side effects following treatment. The pain intensity was measured by visual analog scale (VAS) scores.
The treatments were provided by licensed acupuncturists (HRK) with seven years experience, using a standardized protocol for traditional Chinese acupuncture. If patients were in severe pain, then naproxene sodium or paracetamol tablets were pro-posed as saving drugs. The primary outcome was VAS scores for pain reduction during one and three months after the acupuncture period(17). VAS scores
for pain ranged from 0 (no pain) to 10 (worst pain ever). We noted any adverse effects of the treatments and leaving the application during the trial period.
The control of the third month after treatment, to determine patient satisfaction according to pre-treatment situation, improved in the moment were asked how many of the complaints.
Statistical Analysis
sta-tistical package SPSS-15 for Windows. An indepen-dent sample T-test, paired samples tests and a Wilcoxon signet test were used for comparing cate-gorical and scaled variables. p < 0.05 was accepted as the level of statistical significance.
Results
Demographic characteristics of baseline in patients who received RA or SA have been described in Table 1. Acupuncture treatments were performed in 34 patients for the RA group (23 patients with chronic migraine and 11 patients with chronic ten-sion-type headache) and in 22 patients for the SA group (11 with chronic migraine and 11 with chronic tension-type headache) (Table 2, Table 3). We found significant differences between of the RA group and the SA group in the mean VAS scores during the 1-month and 3-1-month period after treatment (p=0.007,
p=0.021, respectively) (Table 4). Moreover, the frequency of headache attacks during the periods 1 month and 3 months after treat-ment was significantly less in both the RA and SA groups than before treatment (p=0.001, p=0.002), respectively.
The intensity of headache was significantly lower in RA group than SA group after treatmentt (p<0.005) (Table 4). The headache intensity decreased in both group, however it was lower in RA group than SA group. In addition, we found signifi-cant differences between the RA and the SA with respect to the analgesic response to the presence of nausea and the pain duration after treatment. The duration of headache was significantly decreased in RA group than SA group (p<0.001).
The duration of pain decreased in 27 patients (79%) in the RA group. However 9 patients (40%) reported a reduction in nausea and 7 patients (31%)
RA group (n=34) (mean±SD) SA group(n=22) (mean±SD) p values Age 43.71±8.9 41.3±9.8 0.260 Gender 31F/3M 21F/1M -Disease duration 14.4±7.1 12.5±11.2 0.130 VAS scores 9.3±1.3 9.2±0.9 0.856 Monthly headache frequency 22.8±7.2 22.3±7.5 0.786
Table 1: Demographic characteristics of baseline in
patients who received RA or SA. F: female, M: male VAS: visual analog scala
RA group SA group p values
VAS (before
treat-ment) 6.98 6.91 >0.05 VAS (1. month) 3.93 5.18 >0.05 VAS (3. month) 3.15 5.05 >0.05 Headache Frequency (pretreatment) 21.96 19.73 >0.05 Headache frequency (1. month) 4.78* 12.64 0.013 Monthly headache frequency (3. month) 4.78* 13.64 0.000
Table 2: Comparing of outcome measures after first and
thirth month of treatment in patients with chronic migrai-ne of RA and SA groups.
*p<0.05 the comparing of results of RA group and SA group with chronic migraine
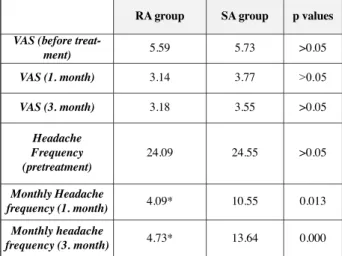
RA group SA group p values
VAS (before
treat-ment) 5.59 5.73 >0.05 VAS (1. month) 3.14 3.77 >0.05 VAS (3. month) 3.18 3.55 >0.05 Headache Frequency (pretreatment) 24.09 24.55 >0.05 Monthly Headache frequency (1. month) 4.09* 10.55 0.013 Monthly headache frequency (3. month) 4.73* 13.64 0.000
Table 3: Comparing of outcome measures after first and
thirth month of treatment in patients with chronic ten-sion-type headache of RA and SA groups.
*p<0.05 the comparing of results of RA group and SA group with chronic tension-type headache
RA group (n=34) (mean±SD) SA group (n=22) (mean±SD) p values VAS (1. month) 5.5±3.0* 7.4±2.1 0.007 VAS (3. month) 5.9±3.1* 7.6±2.2 0.02 Monthly headache frequency (1. month) 4.6±2.7** 11.5±8.8 0.001 Monthly headache frequency (3. month) 4.8±3.8# 11.1±8.4 0.002
Table 4: Comparison of VAS scores and monthly
heada-che frequency in RA and SA groups after first and thirth month of treatment.
RA: real acupuncture; SA: sham acupuncture; VAS: visual ana-log scale
reported an increased analgesic response in the SA group. Nine patients (40%) in the SA group reported decreases in the duration of pain. The nausea decreased in 26 patients (79%) and the analgesic response increased in 20 patients (%58) in the RA group. The analgesic response compared to baseline in patients in the SA group was not statistically sig-nificant (Table 5). Only 2 patients developed syn-cope and 26 experienced minimal bleeding. One patient experienced subcutaneous hematoma and 18 patients reported needle-site pain. The treatment suc-ceeded meanly 69% in the RA group, 43% in the SA group.
Discussion
In the present study, we, first, demonstrated dif-ferences between the RA group and the SA group in the VAS scores in the 1-month and 3-months-after-treatment period. The RA was found more effective than the SA in treatment of CDH. Secondly, we observed some beneficial effects in the SA group. The frequency of headache, VAS scores and pain duration were significantly lower than before treat-ment comparing with after treattreat-ment periods in both groups. The effectiveness of RA on frequency of headache was observed better than SA. In addition, the intensity of headache was more decreased in RA group than SA group. Many of the studies showed the benefits of acupuncture on headache, previously. Some of them found that RA was not better than SA, while others found RA to be more effective.
Acupuncture may be effective in treating headaches, involving skin penetration on the skin at classical points in the study. The needles are inserted to give pressure near of the nonacupuncture points but with-out any real analgesic effects in SA.
In a study, it was reported that SA leads to anal-gesic effect in 40-50% patients who have pain(18).
Hansen et al. showed that RA decreased the duration and frequency of headache in patients with CDH(19).
In another study, it was found a significant decrease in VAS scores after SA in headache. It was mentioned that SA also was very effective in reliev-ing headache(20). Vickers et al. reported that RA is
more effective than SA(21). In another study,
acupunc-ture was found more effective in reducing headache intensity than sham in tension-type headache, but the result was not found in migraine. We determined acupuncture more effective for reducing headache intensity in chronic tension-type headache and chronic migraine.
It was reported that acupuncture reduced pain with nausea and vomiting. In addition, it showed that decreased use of analgesic after acupuncture treat-ment. The stimulation of adrenal cortisol may play a role in the treatment(22). In addition, it was reported
that the using different acupuncture points of the head produced different effects on the body(23). The
content and duration of treatments for headache may vary. The potential psychological effects of acupunc-ture on pain alleviation have been attributed to the physiological effect mechanism. The current study found a significantly increased analgesic response(24).
Twenty patients (59%) in the RA group experienced an increased analgesic response. In addition nausea and pain duration significantly decreased after treat-ment. Twenty-six patients (76%) reported less nausea and twenty-seven patients (79%) reported a decreased duration of pain in the RA group. However, in the SA group, 9 patients (40%) reported reduced nausea and pain duration, and 7 patients (31%), increased analgesic response.
A previous study examined the effectiveness of acupuncture in the treatment of migraines and recur-rent headaches. It found that patients with headache and migraine experienced significantly more relief from RA than from SA(25). The possible effect of
acupuncture may be to restore the balance of energy in the body through the use of needles that are insert-ed into specific points or energy channels by stimu-lating biochemical processes such as the release of endorphins into the limbic structures, subcortical areas, and brain(26).
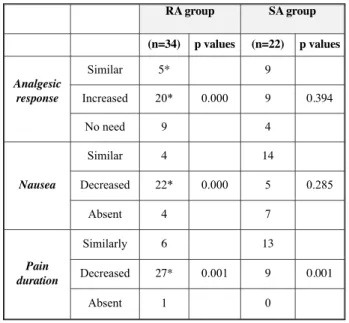
RA group SA group (n=34) p values (n=22) p values Analgesic response Similar 5* 9 Increased 20* 0.000 9 0.394 No need 9 4 Nausea Similar 4 14 Decreased 22* 0.000 5 0.285 Absent 4 7 Pain duration Similarly 6 13 Decreased 27* 0.001 9 0.001 Absent 1 0
Table 5: Comparison of analgesic response the presence
of nausea and pain duration after treatment.
*p<0.05 the comparing of pretreatment and after treatment results in RA group and SA group
However, this does not explain conclusively why acupuncture is efficacious in treating so many different diseases.
In this research, we also examined the side effects of acupuncture. It was reported that the inci-dence of “feeling of faintness or nausea (actually not as serious as syncope)” is 0.8%, and there were 4 fainting in 34,407 treatments (0.01%). The incidence of syncope in this study (2 in 56 subjects, 3.5%) seems to be quite high. In addition, the incidence of minimal bleeding after acupuncture was reported to be 2.6%, but, in this study, it was 26 in 56 subjects (46%). Pain or ache in the punctured region after treatment was reported to be 0.1%, while, in this study, it occurred in 18 of 56 subjects (32%)(27,28).
The difference may depend on race or sex character that including patients were 92% female.
Acupuncture is a safe therapy with low risk of adverse effects in management of chronic conditions such as CDH. Unfortunately, we could not examine gender-related responses to the treatments because most of the patients (93%) were women.
Our study confirmed that acupuncture is a ben-eficial and effective treatment in relieving CDH. The use of acupuncture for reducing CDH during attacks can reduce the need for drug therapies and it is valu-able option for patients suffering from CDH. Our study confirmed that both of the acupuncture and SA may be a beneficial and effective treatment for the CDH. But the acupuncture has more effects on relieving headache and decreasing intensity and duration of headache.
References
1) Kristoffersen Es, Grande Rb, Aaseth K et al. Management Of Primary Chronic Headache İn The General Population: The Akershus Study of Chronic Headache. J Headache Pain. 2012; 13(2): 113-20. 2) Castillo J, Muñoz P, Guitera V, et al. Epidemiology of
chronic daily headache in the general population. Headache 1999; 39: 190.
3) Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004; 24 Suppl 1: 9-160.
4) Hagen K, Linde M, Steiner TJ et al. Risk factors for medication-overuse headache: an 11-year follow-up study. The Nord-Trøndelag Health Studies. Pain. 2012; 153(1): 56-61.
5) Sun-Edelstein C, Mauskop A. Complementary and alternative approaches to the treatment of tension-type headache. Curr Pain Headache Rep. 2012; 16(6): 539-44.
6) Mauskop A. Nonmedication, alternative, and comple-mentary treatments for migraine. Continuum (Minneap
Minn). 2012; 18(4): 796-806.
7) Risberg T, Kaasa S, Wist E et al. Why are cancer patients using non-proven complementary therapies? A cross-sectional multicentre study in Norway. Eur J Cancer 1997; 33: 575.
8) Burstein HJ, Gelber S, Guadagnoli E et al. Use of alter-native medicine by women with early-stage breast can-cer. N Engl J Med 1999; 340: 1733.
9) Amezaga Urruela M, Suarez-Almazor Me. Acupuncture İn The Treatment of Rheumatic Diseases. Curr Rheumatol Rep. 2012; 14(6): 589-97.
10) Hansen PE, Hansen JH, Bentzen O. Acupuncture thera-py of chronic unilateral tinnitus. A double-blind cross-over study. Ugeskr Laeger. 1981; 26; 143(44): 2888-90. 11) Hopton A, MacPherson H. Acupuncture for chronic pain: is acupuncture more than an effective placebo? A systematic review of pooled data from meta-analyses. Pain Pract. 2010; 10(2): 94-102.
12) Endres HG, Böwing G, Diener HC et al. Acupuncture for tension-type headache: a multicentre, sham-con-trolled, patient-and observer-blinded, randomised trial. J Headache Pain. 2007; 8(5): 306-14.
13) Melchart D, Streng A, Hoppe A et al. The acupuncture randomised trial (ART) for tension-type headache-details of the treatment. Acupunct Med. 2005; 23(4): 157-65.
14) Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia. 2004; 24 Suppl 1: 9-160.
15) WHO Guidelines for clinical research on acupuncture, Series no. 15 Manila: Regional Publications Western Pacific 1995: 1-62.
16) Baust W, Sturtzbecher KH. Management of migraine using acupuncture in a double-blind study. Die Medizinische Welt 1978; 29: 669-73.
17) Scott J, Huskisson EC. Vertical or horizontal visual analogue scales. Ann Rheum Dis 1979; 38: 560. 18) Manias P, Tagaris G, Karageorgiou K. Acupuncture in
headache: a critical review. Clin J Pain. 2000; 16(4): 334-9.
19) Hansen K. Attitudes to evidence in acupuncture: an interview study. Med Health Care Philos. 2012; 15(3): 279-85.
20) Dowson DI, Lewith GT, Machin D. The effects of acu-puncture versus placebo in the treatment of headache. Pain. 1985; 21(1): 35-42.
21) Vickers AJ, Cronin AM, Maschino AC et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444-53.
22) Schiapparelli P, Allais G, Castagnoli Gabellari I et al. Non-pharmacological approach to migraine prophyla-xis: part II. Neurol Sci. 2010;31 Suppl 1:S137-9. 23) Kaptchuk T. Acupuncture: theory, efficacy and practice.
Ann Intern Med. 2002; 374–83.
24) Andersson S, Lundeberg T. Acupuncture--from empiri-cism to science: functional background to acupuncture effects in pain and disease. Med Hypotheses. 1995; 45(3): 271-81.
25) Endres HG, Böwing G, Diener HC et al. Acupuncture for tension-type headache: a multicentre, sham-con-trolled, patient-and observer-blinded, randomised trial. J Headache Pain. 2007; 8(5): 306-14.
26) Amezaga Urruela M, Suarez-Almazor ME. Acupuncture in the treatment of rheumatic diseases. Curr Rheumatol Rep. 2012; 14(6): 589-97.
27) Yamashita H. Incidence of Adverse Reactions Associated with Acupuncture. J Altern Complement Med. 2000; 6(4): 345-50.
28) MacPherson H. The York acupuncture safety study: prospective survey of 34000 treatments by traditional acupuncturists. BMJ 2001; 323: 486-7.
_______
Request reprints from: MUSTAFAYILMAZ, MD, Department of Neurology Mugla University Medical School, 48000, Mugla