Signs of Prior Trachoma Infection among
Trichiasis Surgery Patients without
Trachomatous Scarring
Camille D. Mittendorf
Senior Honors Thesis Health Policy and Management University of North Carolina at Chapel Hill
Spring 2020
Readers:
Emily Gower, PhD
First Reader and Primary Honors Thesis Advisor Department of Epidemiology
Gillings School of Global Public Health University of North Carolina at Chapel Hill
Karl Umble, PhD, MPH Second Reader and Advisor
Abstract:
Objectives: We seek to determine if trichiasis surgery patients without visible conjunctival
scarring have other signs of prior trachoma. To do this, we will determine the proportion of eyes
in the study cohort with and without visible conjunctival scarring and will characterize and
compare the prevalence of other signs of trachoma that exist in these two groups.
Methods: This study analyzes data from participants’ baseline ocular examinations from the
MTSS trial. We characterize and compare the prevalence and severity of various eyelid
characteristics across a portion of the cohort. We will also cross-tabulate conjunctival scarring
with the five key other signs of trachoma for eyelids with and without conjunctival scarring.
Results: 5,002 people participated in the MTSS trial, and 2,444 eyes had TT in the late phase.
Among these, 51 eyes had no visible conjunctival scarring. Almost half the eyelids without
scarring had some indication of prior TT. The proportion of eyes with conjunctival scarring was
much higher for severe trichiasis than for eyes without conjunctival scarring. Eyes without
conjunctival scarring present with either no signs of Herbert’s Pits or pannus or the mildest
manifestation of both signs. Most eyes without conjunctival scarring do not present with corneal
scarring but approximately 20% of eyes have a corneal scar grade of at least 1. Both eyes with
conjunctival scarring and without conjunctival scarring reported similar proportions of eyes with
lower lid TT.
Discussion: The main finding of this study is that individuals without visible signs of
conjunctival scarring in the field have other signs of trachoma, indicating that their trichiasis is
trachomatous in nature. These eyes are thus eligible for TT surgery and should not be turned
away, and it is thus crucial to consider other signs of trachoma as markers for the disease. These
Background:
Trachoma is considered a neglected tropical disease and is the “leading infectious cause
of blindness” [1]. As of 2013, 1.2 million people were permanently blinded as a result of the
disease [2]. Numerous risk factors contribute its etiology: areas with endemic trachoma have
populations with low personal and community hygiene typically characterized by poverty,
overcrowding, close contact with active cases, poor sanitation facilities, and inadequate water
availability [1]. Young children are more likely to get this infection because of their close
proximity to others and poor facial cleanliness. However, the advanced stages of trachoma
typically occur in adulthood after people sustain repeated bouts of infections [1].
Trachoma is transmitted through the bacterium, Chlamydia trachomatous, which causes
an infection of the eye [1]. The bacteria is spread through three primary modes of transmission:
direct contact with ocular or nasal discharge from infected persons, exposure to contaminated
inanimate objects (i.e. towels or shawls), and indirect transmission through flies that carry the
bacteria after landing on infected faces [3]. Trachoma distinguishes itself from other eye
infections by its two major phases. The first phase of the disease is the inflammatory stage
wherein active infection and inflammation characterize the eyelid [8]. The inflammatory
response can vary, but when it is severe, it eventually leads to tarsal scarring. Cicatricial
trachoma, which is the second phase of the disease, is demarcated by a structural change in the
eyelid resulting from scarring that causes entropion and trichiasis. During this late phase,
inflammation and infection are less common [8].
To assess the signs of the disease, the 1987 WHO simplified grading scheme for
trachoma identified five signs to establish grading and diagnostic standardization [8]. The
purpose behind this grading scheme was to measure the impact and disease progression of
trachoma by determining the presence of:
Active trachoma, which is early onset, severe, and transmissible;
Cicatricial trachoma, where the disease is well established;
Corneal scarring, which provides a basis to estimate vision loss [8].
These five signs delineate these stages of the disease and include tarsal follicles, inflammatory
thickening, tarsal scarring, trichiasis, and corneal opacity. The first stage of the disease
progression and the grading scheme is trachomatous inflammation – follicular (TF), which is
characterized by the presence of five or more follicles in the upper tarsal conjunctiva [8].
Trachomatous inflammation – intense (TI) is the second stage of active trachoma and involves
inflammatory thickening of the tarsal conjunctiva that conceals more than half of the normal
deep tarsal vessels [8]. Trachomatous scarring (TS) is the third stage and is characterized by
scarring—visible white bands or lines—in the tarsal conjunctiva that exemplifies the late phase
of trachoma [8]. The fourth stage is trachomatous trichiasis (TT), which occurs when at least one
eyelash touches the eyeball as a result of the eyelid turning inwards [8]. TT is indicative of the
severe structural transformation that corresponds with the late phase of the disease. Lastly, the
simplified grading scheme assesses corneal opacity (CO) as a measure of visual impairment,
which is easily visible opacity that covers the pupil or where the pupil margin is blurred [8].
These four signs (TF, TI, TS, TT) are mutually exclusive and are graded as present or not present
Signs and Structural Change in the Cicatricial Phase
This study focuses on signs that appear in the late phase of trachoma. Active infection
creates an inflammatory response in the conjunctiva [1]. As it is easy to transmit the bacteria,
individuals in trachoma-endemic areas can get multiple reinfections, although infection is less
likely to occur in adults. In the cicatricial phase, repeated infections can lead to tarsal
conjunctival scarring in the underside of the eyelid, where white bands of scarring appear [1].
Eventually, this scarring causes a distortion of the eyelid wherein the eyelid turns inwards,
causing the eyelashes to point down towards the eye. When the eyelashes touch the eye, this
condition is known as TT and produces intense pain, globe discomfort, and visual impairment or
blindness [1]. Individuals cope with TT in two ways. The first is through eyelash epilation,
which is the self-management technique of plucking eyelashes to provide pain relief [5].
Although epilation can provide temporary relief, the more effective solution to treat trichiasis is
TT surgery [14]. An individual with one eyelash angled in such a way that it touches the eye
should be considered for this surgery.
Other Signs of Trachoma and TT Severity
Aside from conjunctival scarring and trichiasis, other signs of trachoma appear in
individuals that are also indicative of the disease. In this study, we will examine five of these
signs: Herbert’s pits, pannus, corneal scarring, lower eyelid trachomatous trichiasis, and prior
surgery.
Herbert’s pits are “corneal manifestations of trachoma” [9]. These are grayish, marginal
pits or depressions in the upper part of the cornea that form along the cornea’s perimeter [9].
by the “scleral, episcleral and corneal bundles which were destroyed due to the formation of the
trachomatous nodules” that did not grow back when the eye recovered from active trachoma
[12]. Herbert’s pits are unique signs of the disease.
Pannus is superficial corneal vascularization where the limbus and cornea become
vascularized due to the growth of blood vessels across the eye [10]. Researchers postulated that
pannus could form earlier in the trachomatous disease process than conjunctival scarring, stating
that the “late appearance of scars compared to pannus would indeed suggest that this mechanism
is entirely different from that of pannus formation or even the mechanism of Herbert’s pits” [11].
This presents the idea that these three signs are mutually exclusive from one another, and thus,
the manifestation of one does not necessarily affect the manifestation of another. In some
individuals, Herbert’s pits and pannus might be the only sign that they ever had trachoma in the
first place [9].
Corneal scarring is synonymous to corneal opacity and is a late sign of trachoma. It
typically occurs after the eyelashes have abraded the cornea and caused trauma to it. Corneal
scarring is measured by the extent to which the cornea is obscured by visible opacity. Lower
eyelid TT, a fourth sign of trachoma, occurs when the eyelashes of the lower lid mirror the
mechanism of upper lid TT and start to rotate inwards. Although this occurs more rarely, there
are only two types of lower lid TT, and one of them is trachomatous. Thus, this sign is a potential
marker that an eyelid with trichiasis does have TT. We also considered prior TT surgery as a sign
of trachoma because if an individual had surgery in the past, in at least one eye, this would
indicate that they had prior TT.
Although it is not viewed as a separate sign of trachoma, we believe it is important to
eye’s TT severity is an assessment not made in the field but by the study team. This variable is
determined by considering a combination of two factors: the number of eyelashes touching the
globe and the amount of epilation.
Global Strategy to Eradicate Trachoma
In 1996, the WHO Alliance for the Global Elimination of Trachoma by 2020 (GET 2020)
was formed to promote efforts to eliminate trachoma as a public health issue through the SAFE
strategy and global cooperation and collaboration [3]. The SAFE initiative is an effective
package approach to trachoma elimination where S stands for surgery for trachomatous
trichiasis; A is antibiotics to clear infection; F is facial cleanliness to prevent transmission; and E
is environmental improvement to address risk factors such as improving water and sanitation
conditions [3].
Currently, 2.5 million people need surgery to manage their TT [4] [6]. The “ultimate
intervention goal” or global target for eliminating trachoma includes bringing the prevalence of
TT in endemic areas to less than 0.2% in people aged 15 years and above or less than 1 case for
every 1000 individuals of any age in a district [3] [7]. Great strides were made by members of
the WHO alliance in the fifteen years following its inception [1], including great expansion in the
number of TT surgeries performed. The largest number of surgeries conducted occurred in 2016
[3]. Out of all TT surgeries that year, 71% were done in Ethiopia [3], which is the country with
the greatest burden of trachoma [1]. As of 2019, eight countries had successfully eliminated
trachoma as a public health problem, and five countries claimed meeting the prevalence targets
Problem
In current discussions around managing TT and assessing the TT backlog, some experts
believe that people with trichiasis should not get surgery if they do not present with visible
conjunctival scarring as assessed by field graders or they should not be included in the TT
backlog count. However, we believe an individual can still have TT even if they do not have
visible scarring because they could present with other visible signs trachoma, such as those
mentioned of above. Some research indicates that some of these signs could develop differently
from conjunctival scarring [11]. We postulate that in trachoma-endemic communities, among
individuals with trichiasis but without visible tarsal conjunctival scarring, their trichiasis is likely
trachomatous in nature, and this can be demonstrated by assessing them for other signs of prior
trachomatous infections.
To evaluate this hypothesis, there is a need to determine how common other signs of
trachoma are in patients with trichiasis who present without visible conjunctival scarring.
Concluding this would invalidate the proposed argument, which currently poses a risk to those
who seek surgery for TT but do not have visible conjunctival scarring in the field. If these
individuals are excluded from surgery, it is possible that a significant proportion of people would
be unjustifiably excluded from the TT backlog count and would not benefit from a surgery that
can provide pain relief and minimize their risk for blindness. Additionally, this proposed
argument could, in the long term, hinder a country from truly eliminating trachoma as a public
health problem by minimizing the magnitude of its trachoma backlog and enabling it to
prematurely claim attainment of the WHO ultimate intervention goal [3] [7]. Ultimately, this
impact could lead to a backsliding of the global progress that has already been made to eradicate
Research Aim
To address the proposed argument in the field, we seek to determine if trichiasis surgery
patients without visible conjunctival scarring have other signs of prior trachoma. We hope to
achieve this by determining the proportion of eyes in the study cohort with and without visible
conjunctival scarring. Secondly, we will characterize and compare the prevalence of other signs
of trachoma that exist in both groups.
Methods:
This cross-sectional study is an extension of the MTSS trial (Maximizing Trachomatous
Trichiasis Surgery Success trial), which is an ongoing randomized controlled trial in Ethiopia.
The MTSS trial is led by a consortium of researchers from the University of North Carolina at
Chapel Hill, Johns Hopkins School of Medicine, and Orbis International Ethiopia. The aim of
this larger study is to compare post-operative surgical outcomes across three TT surgeries.
Study population and Participant Recruitment
Recruitment for the MTSS trial spanned April 2017 to May 2019 during which 6,900
eyes were enrolled in the study. To recruit participants for the trial, the study was promoted in
two ways: community-based TT case finders and community announcements. After a brief
training on identifying TT cases, community-based case finders were asked to visit all the
households in their neighborhood to locate eligible individuals with TT. The identified
individuals were asked to assemble at a location in the community on the designated day of the
to make announcements in public places, such as assemblies and local markets, advertising the
details for community-based screening and the upcoming surgery day.
On surgery day (Day 0), a TT surgeon inspected all individuals presenting with suspected
TT. Individuals deemed eligible for TT surgery were transported to the surgical site, where
medical examiners inspected all cases for operable TT. All operable TT individuals met with a
study team member to confirm study eligibility, review the study requirements, and determine
the individual’s interest in participation. Eligibility criteria included having at least one eyelid
with trichiasis that did not have prior TT surgery, being at least eighteen years of age, and being
able to comply with the study requirements for the duration of the study. All eligible and willing
individuals met with a consent specialist to provide appropriate consent in the individual’s native
language. After consent and enrollment, each participant was randomly assigned to one of three
surgery protocols at the time of surgery and underwent a baseline ocular exam prior to surgery.
Data Collection and Data Sources
This study analyzes data from participants’ baseline ocular examinations. Although we
characterize the prevalence of various eyelid characteristics across the entire study cohort (n =
5,002 individuals), we specifically focus on baseline ocular examinations conducted from
August 2018 to April 2019 when the questionnaire included assessments for all of the signs of
trachoma under investigation. The exam was completed for both eyes on the same day as study
enrollment, prior to surgery, with the intended purpose of describing characteristics of both
eyelids, regardless if only one eye had surgery. Data were inputted into an electronic repository.
WHO validated grading schemes for trachoma. These data are found in the Clinical MTSS Trial
Dataset.
Statistical Analysis
Data from the baseline ocular exams were aggregated into an excel file, and we
performed all quantitative data analyses in RStudio. We divided the dataset into two phases, an
early study phase and a late study, where the cutoff date was August 15, 2018. Prior to this date,
the baseline ocular exam did not contain all questions relating to the variables under
investigation. In order to examine our hypothesis, we had to limit our analysis to the subset of
data where all variables for the signs of trachoma under investigation were collected.
After this initial step, we assessed the person-level characteristics (Table 1) and eye-level
characteristics (Table 2) to determine whether our subset was similar to the entire study cohort.
We provide the counts and proportions for both tables. Person-level characteristics concerned the
demographics of the study cohort, and eye-level characteristics examined specific trichiatic
and/or trachomatous characteristics that could differ between one eye and the other.
Additionally, for the eye-level characteristics, we divided each phase into two groups: eyes with
conjunctival scarring and eyes without conjunctival scarring. The purpose of this was to assess
differences in the prevalence of eyelid characteristics between both groups. This analysis also
enabled us to analyze any differences in the severity of eyelid characteristics between those with
and without conjunctival scarring.
Examining specific variables that were collected in the late phase of the study, the final
step of our analysis was to cross tabulate conjunctival scarring with the five key other signs of
signs that each eye presented with and then determining the total number of eyes that had zero or
more signs. Our goal was to understand how the prevalence of these unique signs of trachoma
differed between eyes with and without conjunctival scarring. We further cross tabulated
conjunctival scarring with trichiasis severity to explore their association.
Results:
Baseline Person-Level Characteristics
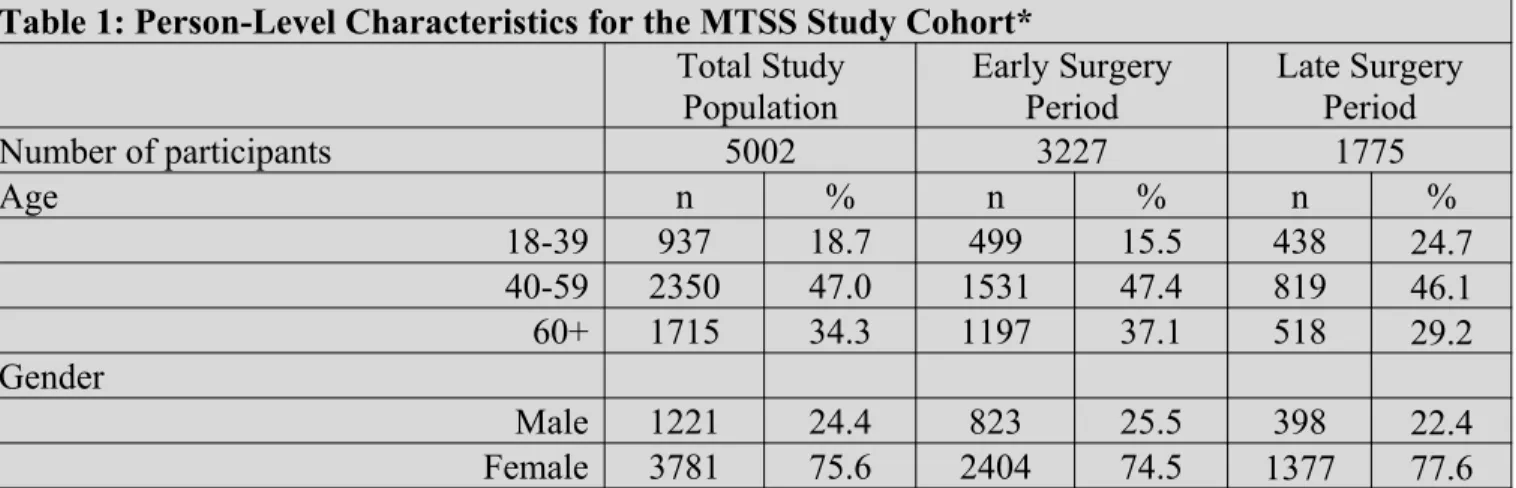
A total of 10,004 eyes (n = 5002 individuals) were included. Table 1 presents the
person-level characteristics across the early and late phase of the study, showing that approximately
three quarters of the study cohort was female for both phases, and most of the participants fell in
the 40-59 age group.
Table 1: Person-Level Characteristics for the MTSS Study Cohort*
Total Study Population
Early Surgery Period
Late Surgery Period
Number of participants 5002 3227 1775
Age n % n % n %
18-39 937 18.7 499 15.5 438 24.7
40-59 2350 47.0 1531 47.4 819 46.1
60+ 1715 34.3 1197 37.1 518 29.2
Gender
Male 1221 24.4 823 25.5 398 22.4
Female 3781 75.6 2404 74.5 1377 77.6
*All eyes from study cohort are included because these eligible participants have TT in at least one or both eyes.
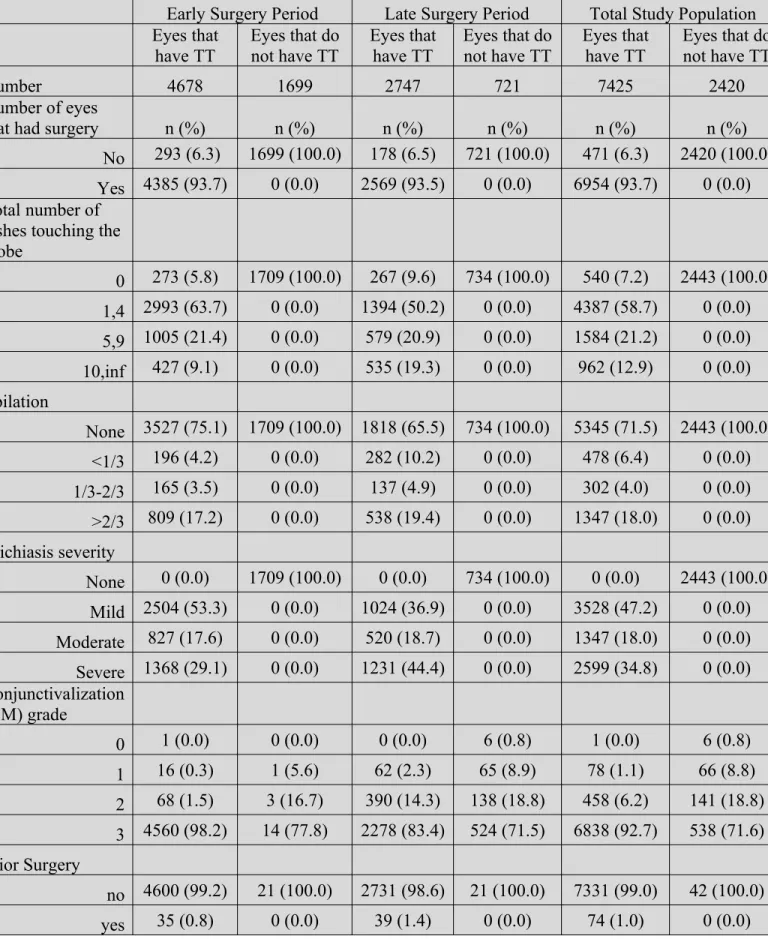
Baseline Prevalence for Eye-Level Characteristics Across the Early and Late Study Phases
Data for the early and late phase of the study are presented to determine whether there
was a difference in eyelid characteristics between both groups (Table 2 in appendix). The cohort
of eyes that were determined to have TT at baseline received surgery to correct for trachomatous
trichiasis.
Of the eyes with TT, a majority of them (n=4387, 58.7% of the combined total; n=2993,
63.7% of the early phase; n=1394, 50.2% of the late phase) had 1-4 lashes that were touching the
globe on the surgery visit day. A larger proportion of eyes had ten or more lashes touching the
globe in the late study period compared to the early study period (19.3% vs. 9.1%). All eyes
without TT did not have any lashes touching the globe.
In both the early and late study phases, the majority of people did not epilate (n=5345,
71.5% of the combined total; n=3527, 75.1% of the early phase; n=1818, 65.5% of the late
phase). A greater proportion of eyes in the late study period than the early study period (10.2%
vs. 4.2%) had eyes where 1/3 of the lashes or less were epilated.
Amongst eyes with TT, more eyes in the early phase of the study had mild trichiasis than
in the late phase (53.3% of eyes in the early phase vs. 36.9% of eyes in the late phase), where
most eyes had severe trichiasis (44.4% of eyes in the late phase vs. 29.1% of eyes in the early
phase). It is unclear why people in the early phase of the study present with milder forms of
trichiasis. One of the reasons could be that this group had milder conjunctival scarring, but we
cannot ascertain this because conjunctival scar data was not collected at the point of the study.
Conjunctivalization of the eyelid margin, which characterizes the extent to which the
eyelid margin has rotated inwards, tends to correlate with TT severity. In both phases of the
study, a large majority of eyes had the most severe grade for conjunctivalization (n=6838, 92.7%
of the combined total; n=4560, 98.2% of the early phase; n=2278, 83.4% of the late phase)
eyes without TT, a large proportion of eyes presented with the highest severity grade for
conjunctivalization, suggesting that they might be at an early stage of late trachoma.
Among eyes with TT, a relatively equal proportion of eyes had never had prior surgery
across both phases (n=7331, 99.0% of the combined total; n=4600, 99.2% of eyes form the early
phase; n=2731, 98.6% of eyes from the late phase). For the few eyes that did have prior surgery
(n=74, 1.0% of the combined total; n=35, 0.8% of eyes from the early phase; n=39, 1.4% of eyes
from the late phase), their other eye did not have prior surgery, which is why they were included
in the study. For eyes without TT, none had prior surgery (n=42, 100% of the combined total),
which means that they never had TT, even in the past.
In the early phase of the study for both the group with and without TT, there are no data
on conjunctival scarring because this data was not yet collected prior to the cutoff date (August
15, 2018). Looking at the data from the late phase, 61% of eyes with TT had severe conjunctival
scarring of the upper eyelid, and only 2% of eyes with TT had no easily visible conjunctival
scarring. This suggests that in this trachoma-endemic area, a minority of eyes present with
trichiasis without having any visible signs of scarring. The was also seen in eyes without TT
although a smaller proportion of eyes (34.8%) had severe conjunctival scarring of the upper
eyelid and the smallest proportion of eyes (12.7%) had no conjunctival scarring. This highlights
the possibility that even in eyes without TT, they might still have trachoma that has not yet
evolved to a point where trichiasis occurs.
Among eyes with TT, there is a discrepancy between the early and late phase of the study
in that 82% of eyes did not have any corneal scarring in the early phase, whereas only 22% of
eyes had no corneal scarring in the late phase of the study. In contrast, the largest proportion of
although there could be an association between TT severity and corneal scarring where the more
severe the trichiasis, the more likely corneal scarring will be present and/or severe. This would
posit that TT severity was lower in the early study group than the late study group. A similar
finding is observed in the group without TT. For those with reported data, most eyes had no
corneal scarring in the early phase whereas a larger proportion of eyes had a corneal scar grade
of 1 in the late phase. Alternatively, perhaps trauma from another disease mechanism caused the
corneal scarring. It is important to note that for the vast majority of eyes without TT, data was
not collected on their degree of corneal scarring perhaps because this was not collected after their
TT determination was made. Additionally, data on corneal scarring was a variable for which data
was collected after the start of the study. Thus, some eyes simply do not have any reported data.
For eyes with TT, impaired vision was very common (n=2945, 39.8% of the combined
total), followed by those with normal vision (n=2744, 37.1% of the combined total), then eyes
that were deemed blind (n=1704, 23.0% of the combined total). Among eyes without TT, most
eyes had normal visual acuity across both phases (n=1065, 44.1% of the combined total),
followed by impaired vision (n=879, 36.4% of the combined total), then blind eyes (n=470,
19.5% of the combined total). Since trichiasis leads to worsened visual acuity and a considerable
number of eyes without TT have impaired vision, a plausible explanation is that these eyes are at
an earlier stage of trachoma, had prior TT surgery, or other trauma or risk factors impacted their
vision.
Only 176 eyes (2.4%) had lower lid TT among eyes with TT, and 38 eyes (1.6%) had
lower lid TT among eyes without TT. Thus, it is possible for eyes to only present with lower lid
TT and not upper lid TT or to present with both upper and lower lid TT. Findings were
Data for the presence of Herbert’s pits was collected starting August 15, 2018, so only
eyes in the latter half of the study have reported data. For those with TT, 51% of eyes do not
have any sign of Herbert’s pits and 34% of eyes have 1 to 3 typical Herbert’s pits. Fewer eyes
have more extreme manifestations of Herbert’s pits. In the group of eyes without TT, signs of
Herbert’s pits are also observed, with 21% of eyes showing 1 to 3 typical Herbert’s pits.
However, Herbert’s pits were less common in eyes without TT.
Focusing on eyes with TT, 68% of eyes did not have pannus and 20% of eyes had
between 0 and 2 mm vessel extension. The proportion of those with pannus decreased as pannus
severity increased. Similarly, in eyes without TT, roughly 87% had no pannus, and 10% had
pannus extension between 0 and 2 mm.
Conjunctival Scarring and the Severity for Five Signs of Trachoma
Further examining the presence of other signs of trachoma in eyes with TT, we compared
the group with conjunctival scarring to the group without conjunctival scarring (Table 3 in
appendix). The “total number of signs” variable summarizes the number of eyes that present with
zero or more of the signs of trachoma under investigation after August 15, 2018. Separating eyes
into those with conjunctival scarring and those without, we can see the total number of signs that
eyes had at baseline although this measure does not reflect the severity of their presentations.
Across the group that presented with conjunctival scarring, 43% had one of the signs of trachoma
under investigation, and 30% of eyes had two signs. Only 9% of eyes had no other signs of
trachoma. Of those without conjunctival scarring, 59% of eyes presented with at least one other
sign of trachoma. This signifies that over half of these eyes have some indication of prior
nature and thus requires TT surgery. This affirms that other signs of trachoma could be present
even if the main marker, conjunctival scarring, is not. For both groups, the proportion of eyes
decreased as the number of total signs increased. In addition, neither group had eyes that
displayed all five signs of trachoma under investigation.
0 1 2 3 4 5
0% 20% 40% 60% 80% 100%
Total Number of Signs of Trachoma
No Conjunctival Scarring Yes Conjunctival Scarring
Total Number of Signs of Trachoma
P e rc e n ta g e o f St u d y C o h or t
Figure 1: Total Number of Signs of Trachoma between Eyes with Conjunctival Scarring and Eyes without Conjunctival Scarring
The proportion of eyes with conjunctival scarring decreases as the severity of Herbert’s
pits increases. On the other hand, eyes without conjunctival scarring present with either no signs
of Herbert’s pits (57%) or 1 to 3 typical characteristics of the sign (43%), which is the mildest
manifestation of the sign. No eyes without visible conjunctival scarring have a higher severity
grade for Herbert’s pits, suggesting that only milder forms of the sign will present in these eyes.
Despite only presenting in a milder form, eyes without conjunctival scarring that have visible
Herbert’s pits have evidence that their trichiasis is trachomatous in nature and consequently
None
1-3 typi
cal
>3, u pper
lunu lar n
ot in volve
d
Entir e up
per l unul
ar in volve
d
Corn ea e
ncirc led 0% 40% 80%
Herbert’s pits
No Conjunctival Scarring Yes Conjunctival Scarring
Herbert’s pits Grade
P e rc e n ta ge o f S tu d y C o h o rt
Figure 2: The Severity of Herbert’s Pits between Eyes with Conjunctival Scarring and Eyes without Conjunctival Scarring
Similarly, the proportion of eyes with conjunctival scarring decreases as the severity of
pannus increases. A larger proportion of eyes (72%) have no evidence of pannus, and only 19%
of eyes have pannus between 0 and 2 mm in size. Among eyes without conjunctival scarring,
86% do not present with any signs of pannus, and 12% show pannus between 0 and 2 mm. These
findings purport that pannus is rare in both groups but that a majority of eyes with pannus have a
milder form of it for both groups. Pannus also seems to occur in some eyes regardless of the
presence of conjunctival scarring, emphasizing that the trichiasis in some eyes without
0 mm extension >0 - <2.0 mm
extension 2.0- <4.0 mm extension 4.0 - <6.0 mm extension 6.0 mm or more extension 0%
20% 40% 60% 80% 100%
Pannus Extension
No Conjunctival Scarring Yes Conjunctival Scarring
Pannus Grade
P
e
rc
en
ta
g
e
o
f
St
u
d
y
C
o
h
o
rt
Figure 3: The Severity of Pannus between Eyes with Conjunctival Scarring and Eyes without Conjunctival Scarring
In terms of corneal scarring, most eyes with conjunctival scarring (60%) have a corneal
scar grade of 1, and the frequency of eyes drops considerably as the corneal scar grade increases.
However, 6% of eyes have a corneal scar grade of 4. For eyes without conjunctival scarring,
most eyes do not present with significant corneal scarring although approximately 25% of eyes
have a corneal scar grade of at least 1. Additionally, it is possible that those with less severe
corneal scarring have less severe trichiasis and less severe conjunctival scarring because the
0 1 2a 2b 2c 2d 3 4 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Corneal Scarring
No Conjunctival Scarring Yes Conjunctival Scarring
Corneal Scarring Grade
P e rc e n ta g e o f St u d y C o h o rt
Figure 4: The Severity of Corneal Scarring between Eyes with Conjunctival Scarring and Eyes without Conjunctival Scarring
Both eyes with conjunctival scarring and without conjunctival scarring reported similar
proportions of eyes with lower lid TT (Table 3; 4% in the group without conjunctival scarring vs.
3% in the group with conjunctival scarring). These strikingly similar findings between both
groups could suggest that lower lid TT has the same prevalence in eyes with and without
conjunctival scarring, signifying that lower lid TT—albeit rare—could be used as an indicator of
trichiasis that is trachomatous in nature, as it is part of the inflammatory trachoma disease
process.
Almost no one in both groups had prior surgery (Table 3; 0% of eyes without
conjunctival scarring vs. 1% of eyes with conjunctival scarring). As a result, prior surgery is
likely not an effective measure to use when considering the diagnosis of TT in eyes that did not
present with conjunctival scarring as so few individuals had prior surgery. These findings do
report that eyes with conjunctival scarring that did have prior surgery (n=27), and therefore had
suggest that the eyes in the group without conjunctival scarring had TT in the past that received
treatment. With such a small sample of eyes without conjunctival scarring, it cannot be inferred
whether prior surgery should be used as a marker to assess if their trichiasis is trachomatous. It is
important to mention that if these eyes did have prior surgery, this is evidence that they had TT
in the past that received treatment. Correspondingly, their trichiasis is likely trachomatous in
nature because it is possible for trichiasis to return even having had surgery because the
trachoma disease process is still impacting the eye [14].
Lastly, we also looked at differences in trichiasis severity in eyes with and without
conjunctival scarring. Almost two times the proportion of eyes without conjunctival scarring
presented with milder forms of trichiasis compared to the proportion of eyes with conjunctival
scarring. In contrast, the proportion of eyes with conjunctival scarring with severe trichiasis was
almost twice the proportion of eyes without conjunctival scarring. This proposes that eyes
without visible conjunctival scarring are at earlier stages of the disease where scarring is not yet
visible and the disease progression has not yet shown the same magnitude the structural
transformation that leads to more serious trichiasis.
None Mild Moderate Severe
0% 20% 40% 60% 80% 100%
Trichiasis Severity
No Conjunctival Scarring Yes Conjunctival Scarring
Trichiasis Severity Grade
Figure 5: Trichiasis Severity between Eyes with Conjunctival Scarring and Eyes without Conjunctival Scarring
Discussion:
Public Health and Policy Implications
The main implication of this study is that individuals without visible signs of conjunctival
scarring in the field have other signs of trachoma that suggest that their trichiasis is trachomatous
in nature, as evidenced by Herbert’s pits, pannus, corneal scarring, and lower lid TT in eyes
without visible scarring. This stresses that it is possible to have trichiasis that is trachomatous
without presenting with visible conjunctival scarring. It is thus imperative to consider other signs
of trachoma as markers for the disease in determining whether trichiasis is trachomatous.
Presenting with any number of these other signs in addition to trichiasis suggests that an
individual has TT, are eligible for TT surgery, and should not be turned away.
Refusing surgery to patients who present with these other signs of trachoma and no
visible conjunctival scarring compromises efforts to eliminate trachoma as a public health
problem. These individuals escape the scrutiny of meeting global intervention targets, such as
those stipulated under the SAFE strategy, and risk a country underreporting the number of TT
cases it seeks to treat. As a result, it jeopardizes the global efforts that have been made in
eliminating trachoma and a country’s programmatic decision-making in adequately addressing
the prevalence of TT in its borders.
Rather than turning people away from surgery for not presenting with conjunctival
scarring and reducing the magnitude of the problem, it is important to advocate for the continued
expansion of TT surgery. Governments in countries with trachoma should maintain or expand
enhancing screening procedures to screen for other signs of trachoma and ensure that those who
do not have scarring do not get excluded from surgery. In this way, surgery campaigns will be
more effective at catching all those with clinical TT who would have otherwise gone untreated
for trichiasis if their TT was only determined by the extent of their conjunctival scarring.
Ultimately, the goal behind this recommendation is to better strive for the WHO ultimate
intervention goal and continue the progress that has been made in eliminating trachoma.
Relationship Between Trichiasis Severity and Conjunctival Scarring
The nature of the relationship between trichiasis severity and conjunctival scarring is
predicated on the phase of the trachoma disease process. Per the findings, eyes without visible
conjunctival scarring presented with milder trichiasis. On the other hand, while some eyes with
visible conjunctival scarring presented more severe trichiasis, others were still mild. This
suggests that eyes without scarring may be at an early stage of the cicatricial phase of trachoma
because the scarring has only started the structural inward rotation of the eyelid. In contrast, eyes
with visible conjunctival scarring are further along in the cicatricial phase. Visibly worse
conjunctival scarring indicates greater structural change, which may be indicative of TT that has
progressed more. Consequently, these eyes with conjunctival scarring will more often have
severe trichiasis.
Context Constraints with Field Workers
A supporting argument for looking at other signs of trachoma when determining the
nature of the trichiasis is that field workers have an inherently harder time identifying the minor
not detect conjunctival scarring in the field even though it would be observed by specialized
experts in a clinical setting. Minor signs of conjunctival scarring might be too difficult or
obscured to observe in the field given the context and resource constraints that field workers
face. With many patients to address, field workers are limited by the time they can spend
assessing the signs of trachoma, increasing the risk of missing small or hidden indications of
scarring. Field workers are further limited by the tools at their disposal. Unlike expert clinicians
who can observe magnified images of the eye, field workers are less able to detect these signs
without the use of specialized equipment. Lastly, field workers do not receive the same training
that expert ophthalmologists have and thus may not have an acute skillset to perceive the
nuanced signs of conjunctival scarring. This reinforces the need to also consider the other signs
of trachoma in the field—not only conjunctival scarring—to confirm the trachomatous nature of
the trichiasis.
Limitations
The primary limitation of this study is that not all variables were collected from the start
of the MTSS trial. This forced us to exclude many individuals from the dataset and only consider
data after August 15, 2018, which was the first date where all variables for the other signs of
trachoma were collected and reported. For example, data on the conjunctival scar variable was
not collected until August 15, 2018. A ramification of this is that it restricted our sample size and
resulted in a low number of individuals that presented with eyes without conjunctival scarring in
the late phase of the study. This low sample size may impact the ability of the findings to be
Future Research
This study is significant because it supports the argument that other signs should be
evaluated alongside conjunctival scarring when determining whether trichiasis is trachomatous in
nature. Any eye with trichiasis that presents with any number of these signs of trachoma likely
has clinical TT. These signs—such as Herbert’s pits, pannus, and lower lid TT—should thus be
considered as markers for the disease, as they are part of the disease manifestation.
Although our findings show that eyes without conjunctival scarring presenting with these
other signs of trachoma have clinical TT, a fraction of eyes without conjunctival scarring (Table
3) presented with no other signs of trachoma. Additionally, for each of the other signs of
trachoma under investigation, a large proportion of eyes without conjunctival scarring still did
not present with the sign. In both of these cases, it would be paramount to research the signs of
trachoma that appear in the opposite eye, as it could provide evidence for the presence and state
of the disease process in an individual. It is possible that signs might not present themselves in
one eye but could be visible in the other. Exploring eyelid characteristics in the opposite eye
provides an opportunity to better grasp the various markers of trachoma and the nature of
trachoma.
Acknowledgements:
Completing this project would not have been possible without the assistance and support of the
following people:
Emily Gower, PhD, who provided me with incredible mentorship and guidance as I developed
trachoma research, and after I switched thesis topics, she was most willing to help me develop a
new research question and project.
Alison Singer, PhD, who provided me with invaluable support and assistance on framing the
data analysis for this project.
Karl Umble, PhD, MPH, who went above and beyond with being the best thesis program
coordinator and second reader. I am forever grateful for Dr. Umble and for his investment in the
success of my thesis experience and in my future.
References:
[1] “WHO Alliance for the Global Elimination of Blinding Trachoma by the Year 2020 Progress Report on Elimination of Trachoma, 2013.” Weekly Epidemiological Record, vol. 89, no. 39, Sept. 2014, pp. 421–28, https://www.who.int/wer/2013/wer8939.pdf.
[2] Pascolini, Donatella, and Silvio Paolo Mariotti. “Global Estimates of Visual Impairment: 2010.” British Journal of Ophthalmology, vol. 96, no. 5, May 2012, pp. 614–18, https://bjo-bmj-com.libproxy.lib.unc.edu/content/96/5/614.
[3] “WHO Alliance for the Global Elimination of Trachoma by 2020: Progress Report on Elimination of Trachoma, 2014–2016.” Weekly Epidemiological Record, vol. 92, no. 26, June 2017, pp. 359–368,
https://apps.who.int/iris/bitstream/handle/10665/255778/WER9226.pdf;jsessionid=61FA749D51 5EC0DE711083961D9B5E63?sequence=1.
[4] “WHO Alliance for the Global Elimination of Trachoma by 2020: Progress Report on Elimination of Trachoma, 2018.” Weekly Epidemiological Record, vol. 94, no. 29, July 2019, pp. 317–328, https://apps.who.int/iris/bitstream/handle/10665/325910/WER9429-en-fr.pdf? ua=1.
[5] International Coalition for Trachoma Control. Global Scientific Meeting on Trachomatous Trichiasis: Meeting Discussions, Conclusions & Suggested Research. International Coalition for Trachoma Control, 2012,
http://www.kcco.net/wp-content/uploads/2017/08/ictc_tt_surgery_report_2012_english.pdf. [6] “Key Trachoma Facts and Statistics.” International Coalition for Trachoma Control, International Coalition for Trachoma Control, 2019,
http://www.trachomacoalition.org/trachomastatistics.
[9] “Herbert's Peripheral Pits.” The British journal of ophthalmology vol. 15,7 (1931): 411-2. doi:10.1136/bjo.15.7.411
[10] ZSCHEILE, F.PAUL. “Herbert’s pits.” Arch Ophthalmol, vol. 73, no. 6, 1965, pp. 827–828, doi:https://doi.org/10.1001/archopht.1965.00970030829014.
[11] Dawson, C. R., et al. “Limbal Disease in Trachoma and Other Ocular Chlamydial Infections: Risk Factors for Corneal Vascularisation.” Eye, vol. 3, Mar. 1989, pp. 204–09, doi:doi:10.1038/eye.1989.29.
[12] Busacca, Archimede. “On the Structure of Herbert’s pits.” The British Journal of Opthalmology, vol. 19, no. 1, Jan. 1935, pp. 26–31,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC511760/pdf/brjopthal00801-0045.pdf.
Table 2: Eye-Level Characteristics for Study Cohort*
Early Surgery Period Late Surgery Period Total Study Population Eyes that
have TT Eyes that donot have TT Eyes thathave TT Eyes that donot have TT Eyes thathave TT Eyes that donot have TT
Number 4678 1699 2747 721 7425 2420
Number of eyes
that had surgery n (%) n (%) n (%) n (%) n (%) n (%)
No 293 (6.3) 1699 (100.0) 178 (6.5) 721 (100.0) 471 (6.3) 2420 (100.0) Yes 4385 (93.7) 0 (0.0) 2569 (93.5) 0 (0.0) 6954 (93.7) 0 (0.0) Total number of
lashes touching the globe
0 273 (5.8) 1709 (100.0) 267 (9.6) 734 (100.0) 540 (7.2) 2443 (100.0) 1,4 2993 (63.7) 0 (0.0) 1394 (50.2) 0 (0.0) 4387 (58.7) 0 (0.0) 5,9 1005 (21.4) 0 (0.0) 579 (20.9) 0 (0.0) 1584 (21.2) 0 (0.0) 10,inf 427 (9.1) 0 (0.0) 535 (19.3) 0 (0.0) 962 (12.9) 0 (0.0) Epilation
None 3527 (75.1) 1709 (100.0) 1818 (65.5) 734 (100.0) 5345 (71.5) 2443 (100.0) <1/3 196 (4.2) 0 (0.0) 282 (10.2) 0 (0.0) 478 (6.4) 0 (0.0) 1/3-2/3 165 (3.5) 0 (0.0) 137 (4.9) 0 (0.0) 302 (4.0) 0 (0.0) >2/3 809 (17.2) 0 (0.0) 538 (19.4) 0 (0.0) 1347 (18.0) 0 (0.0) Trichiasis severity
None 0 (0.0) 1709 (100.0) 0 (0.0) 734 (100.0) 0 (0.0) 2443 (100.0) Mild 2504 (53.3) 0 (0.0) 1024 (36.9) 0 (0.0) 3528 (47.2) 0 (0.0) Moderate 827 (17.6) 0 (0.0) 520 (18.7) 0 (0.0) 1347 (18.0) 0 (0.0) Severe 1368 (29.1) 0 (0.0) 1231 (44.4) 0 (0.0) 2599 (34.8) 0 (0.0) Conjunctivalization
(CM) grade
0 1 (0.0) 0 (0.0) 0 (0.0) 6 (0.8) 1 (0.0) 6 (0.8)
1 16 (0.3) 1 (5.6) 62 (2.3) 65 (8.9) 78 (1.1) 66 (8.8)
2 68 (1.5) 3 (16.7) 390 (14.3) 138 (18.8) 458 (6.2) 141 (18.8) 3 4560 (98.2) 14 (77.8) 2278 (83.4) 524 (71.5) 6838 (92.7) 538 (71.6) Prior Surgery
Conjunctival Scar Grade
No scarring -- -- 51 (2.1) 83 (12.7) 51 (2.1) 83 (12.7)
Mild -- -- 279 (11.4) 161 (24.7) 279 (11.4) 161 (24.7)
Moderate -- -- 618 (25.3) 182 (27.9) 618 (25.3) 182 (27.9)
Severe -- -- 1496 (61.2) 227 (34.8) 1496 (61.2) 227 (34.8)
Corneal Scar (CO) Grade
0 3825 (82.4) 15 (71.4) 617 (22.4) 293 (40.7) 4442 (60.0) 308 (41.6) 1 575 (12.4) 6 (28.6) 1618 (58.7) 386 (53.6) 2193 (29.6) 392 (52.9) 2a 86 (1.9) 0 (0.0) 201 (7.3) 17 (2.4) 287 (3.9) 17 (2.3)
2b 50 (1.1) 0 (0.0) 52 (1.9) 5 (0.7) 102 (1.4) 5 (0.7)
2c 59 (1.3) 0 (0.0) 190 (6.9) 4 (0.6) 249 (3.4) 4 (0.5)
2d 23 (0.5) 0 (0.0) 51 (1.8) 10 (1.4) 74 (1.0) 10 (1.3)
3 21 (0.5) 0 (0.0) 27 (1.0) 3 (0.4) 48 (0.6) 3 (0.4)
4 5 (0.1) 0 (0.0) 2 (0.1) 2 (0.3) 7 (0.1) 2 (0.3)
Distance Visual Acuity
Normal 1723 (37.2) 711 (42.2) 1021 (36.9) 354 (48.5) 2744 (37.1) 1065 (44.1) Impaired 1826 (39.5) 612 (36.3) 1119 (40.5) 267 (36.6) 2945 (39.8) 879 (36.4)
Blind 1078 (23.3) 361 (21.4) 626 (22.6) 109 (14.9) 1704 (23.0) 470 (19.5) Lower Eyelid TT
no 4588 (98.0) 1691 (98.9) 2687 (97.0) 713 (97.1) 7275 (97.6) 2404 (98.4) yes 93 (2.0) 18 (1.1) 83 (3.0) 21 (2.9) 176 (2.4) 39 (1.6) Herbert’s pits
None -- -- 1414 (51.2) 555 (76.4) 1414 (51.2) 555 (76.4)
1-3 typical -- -- 947 (34.3) 153 (21.1) 947 (34.3) 153 (21.1)
>3, upper lunular
not involved -- -- 373 (13.5) 17 (2.3) 373 (13.5) 17 (2.3)
Entire upper
lunular involved -- -- 18 (0.7) 0 (0.0) 18 (0.7) 0 (0.0)
Cornea encircled -- -- 9 (0.3) 1 (0.1) 9 (0.3) 1 (0.1)
Pannus
extension 2.0- <4.0 mm extension
-- -- 185 (6.7) 7 (1.0) 185 (6.7) 7 (1.0)
4.0 - <6.0 mm extension
-- -- 81 (2.9) 5 (0.7) 81 (2.9) 5 (0.7)
6.0 mm or more extension
--
--56 (2.0) 1 (0.1) 56 (2.0) 1 (0.1)
*All eyes from the cohort are included and are divided in eyes that had TT and eyes that did not have TT across the early and late phase of the study.
Table 3 - Trachomatous Scarring and Graded Severity of Five Other Signs of Trachoma*
No Conjunctival Scarring Yes Conjunctival Scarring
Number 51 2393
Total Number of Other Signs n (%) n (%)
0 21 (41) 226 (9)
1 19 (37) 1045 (44)
2 8 (16) 734 (31)
3 3 (6) 369 (15)
4 0 (0) 19 (1)
5 0 (0) 0 (0)
Trichiasis Severity
None 0 (0) 0 (0)
Mild 35 (69) 916 (38)
Moderate 5 (10) 478 (20)
Severe 11 (22) 999 (42)
Herbert’s pits
None 29 (57) 1305 (55)
1-3 typical 22 (43) 789 (33)
>3, upper lunular not involved 0 (0) 279 (12)
Entire upper lunular involved 0 (0) 12 (1)
Cornea encircled 0 (0) 0 (0)
Pannus
0 mm extension 44 (86) 1719 (72)
>0 - <2.0 mm extension 6 (12) 458 (19)
2.0- <4.0 mm extension 0 (0) 130 (5)
4.0 - <6.0 mm extension 1 (2) 59 (2)
6.0 mm or more extension 0 (0) 27 (1)
Corneal Scar (CO) Grade
0 38 (75) 553 (23)
1 11 (22) 1434 (60)
2c 1 (2) 153 (6)
2d 1 (2) 37 (2)
3 0 (0) 18 (1)
4 0 (0) 1 (0)
Lower Lid Trachomatous Trichiasis
no 49 (96) 2317 (97)
yes 2 (4) 72 (3)
Prior TT Surgery
no 51 (100) 2363 (99)
yes 0 (0) 27 (1)