A B S T R A C T
This study compared two groups of patients who were elderly and edentu-lous, one group included subjects who had mandibular overdentures supported by two implants (Group I); the other groups wore conventional complete dentures (Group II). This retrospective study included 100 edentulous patients (50 from each group) with an average age of 67.86 years, who had been followed for 4 years. The groups were compared in terms of patient satisfac-tion, quality of life (QOL), and bite force. The bite force and patient satisfaction scores of Group I were found to be statistically significantly higher than Group II (p ⬍.05). However, no statisti-cally significant difference was found between the two groups’ QOL scores (p ⬎.05) except on the physical pain subscale (p ⫽.013). Based on these results, it can be concluded that after 4 years of function, subjects wearing mandibular overdentures supported by two implants had higher values for bite force and patient satisfaction scores, but similar QOL scores when compared to conventional complete denture-wearers.
Comparison of patient satisfaction,
quality of life, and bite force between
elderly edentulous patients wearing
mandibular two implant-supported
overdentures and conventional complete
dentures after 4 years
Onur Geckili, PhD, DDS;1* Hakan Bilhan, PhD, DDS;2Emre Mumcu, PhD,
DDS;1Cagatay Dayan, DDS;3Ali Yabul, DDS;3Necat Tuncer, PhD, DDS4
1Research Assistant;2Associate Professor;3PhD Student; 4Professor—Department of Prosthodontics,
Faculty of Dentistry, Istanbul University, Istanbul, Turkey. *Corresponding author e-mail: [email protected]
Spec Care Dentist 32(4):136-141, 2012
With the introduction of dental implants that stabilize dentures, many conventional complete denture limita-tions are eliminated.4In both within-
and between-group comparisons,7-15
mandibular implant-supported overden-tures have been found to improve patient satisfaction, QOL, and masticatory func-tion. Moreover, a panel of experts in the field of dental implants has recom-mended a two implant retained
overdenture as the treatment of choice for the edentulous mandible (the McGill consensus statement).16The maximum
bite force (MBF) of subjects with a mandibular denture retained by implants was found to be up to twice as high when compared to subjects with a con-ventional complete denture.17,18After
implant treatment, subjects needed only about half the number of chewing cycles as before treatment to halve the initial
I n t r o d u c t i o n
Due to better oral health maintenance, the percentage of adults who are edentulous has decreased in industrialized nations in the past 20 years.1However, the growth of the
population 65 years of age or older has led to an absolute increase in the number of adults who are edentulous.1,2Epidemiological survey data indicate that the edentulous
adult population in the United States will increase from 35.4 million in 2000 to 37.9 million in 2020.2Similar assumptions can be made for other countries too.1,2As
eden-tulism can be regarded as a handicap3and is reported to affect oral and general health
as well as overall quality of life (QOL),4-6treatment of edentulism will continue to be a
challenge for clinicians. The success of the treatment of edentulism with conventional complete dentures is limited mainly because of the instability of mandibular den-tures,4,7impaired chewing ability,8,9and ongoing bone resorption, especially in the
mandible.4As a consequence, dissatisfaction with complete dentures has been a clinical
and social problem for many years.7,10,11
KEY WORDS:
denture, geriatricsize of a test food.19Moreover, it has
been shown that the treatment with two interforaminal implants provides evi-dence of neuromuscular adaptation toward values of healthy dentate patients.20However, it has been shown
that masticatory function is a patient factor rather than a parameter that pros-thetic treatment can qualify.21Therefore,
it can be assumed that patients with any denture type may have good chewing efficiency after an adequate adaptation time. To our knowledge, there is no published retrospective study comparing the satisfaction, QOL, and bite forces of people who have worn mandibular two implant-supported overdentures to those using conventional complete dentures after an extended period of time. The null hypothesis of this study was that two implant-retained mandibular over-dentures were superior to conventional complete dentures in terms of patient satisfaction, QOL, and bite force.
M a t e r i a l s a n d m e t h o d s
Patient selection
The study included 50 patients treated with two implant-retained mandibular overdentures (Group I) and maxillary complete dentures compared to
50 patients treated with conventional maxillary and mandibular complete dentures (Group II). All the patients were treated between 2006 and 2007 at Istanbul University Department of Prosthodontics. To be included in the study, subjects must have had treatment by qualified prosthodontists, no major denture problems, a panoramic radi-ograph showing a Type III or Type IV edentulous mandible according to the classification of the American College of Prosthodontics,22and the ability to give
informed consent. Subjects were selected randomly from a pool of 187 patients by a lottery method using Research Randomizer and were invited to be included in this retrospective trial in January 2009. The subjects’ appoint-ments were organized according to when their prosthesis was delivered; thus, all subjects were recalled after exactly 4 years of function. No subject refused to participate. All the implants were from the same manufacturer (Astra Tech, Mˆlndal, Sweden), and surgical instilla-tion was carried out as recommended by the manufacturer, by a qualified oral and maxillofacial surgeon using a one-stage surgical protocol. Locator abutments (Locator, Astra Tech; Astra Tech AB) were screwed to the implants and connected to the dentures by matching
attachments (Locator, Astra Tech) using a chair-side processing method.23All the
mandibular overdentures were delivered to the subjects 1.5 months after
installation of the implants (early loading protocol). Following the univer-sity clinic’s policy, the subjects’ recall appointments were scheduled on a monthly basis for 3 months after the insertion of their prosthesis, and they all were recalled annually thereafter.
The subjects provided informed writ-ten consent with regard to treatment and measurement procedures; approval from the university ethics commission was obtained.
Clinical examination
and MBF measurements
A clinical examination, including evaluation of prosthetic parameters such as occlusion, tissue adaptation, and con-dition of the retentive mechanism, was performed before measurements were made by two prosthodontists blinded to the study protocol. Before the study, the examiners were trained and calibrated in using the bite force device. If present, pressure spots were eliminated by grind-ing from inside the denture base. If the denture base adaptation was not accept-able, a relining was performed. The occlusion was checked for premature contacts due to wear and was eliminated. In case of loosening of an abutment or occlusal screws of the subjects in Group I, these were either changed or tightened. Loosened retentive mechanisms were either changed or tightened. Subjects receiving corrections (n ⫽12; nine subjects in Group I and three subjects in Group II) were allowed to use their adjusted dentures for an extra month before measurements were made.
The same prosthodontists measured MBF bilaterally in the first molar region, using a device with two strain gauges (Measurements Group Inc., Micro-Measurements Division, Type
the occlusal surfaces in the first molar region, as described previously,18and a
cubic silicone block of the same height as the bite fork was placed on the other side for occlusal stability. The measure-ments were repeated three times for each of the left and right sides, as suggested in a previous study.18The highest values
were recorded while patients were biting as hard as possible. The mean of the left-and right-side values was considered as one value. A 10-minute relaxation period after each bite was required, in order to obtain a reliable MBF value.
Patient satisfaction and QOL
measurements
All subjects were asked to complete a questionnaire recording six aspects of patient satisfaction using a 100 mm visual analog scale (VAS). The scales ranged from completely satisfied to com-pletely dissatisfied. The patients used the scales to record their personal opinions of six factors: general comfort, retention, chewing, speech, esthetics, and pain; these factors were based on previously published patient satisfaction studies.8,24
For the measurement of QOL, the oral health impact profile (OHIP) was used; OHIP is a disease-specific measure of an individual’s perception of the social impact of oral disorders on his or her well-being and the most commonly used measure to assess the impact of dental treatments on QOL.25,26The original
OHIP-49 consisted of 49 questions,26
whereas the shorter and more patient-friendly version consists of 14 questions and covers the same seven domains as OHIP-49 (functional limitation, physical
pain, psychological discomfort, physical disability, psychological disability, social disability, and handicap).27The five
responses for each item are: never, hardly ever, occasionally, fairly often, and very often. Items were scored on a five-point scale ranging from 0 (never) to 4 (very often). Achievable OHIP-14 scores range from 0 to 56. Lower scores represent a higher QOL. The Turkish version of OHIP-14 was used in this study.27,28
Statistical analyses
Statistical analysis was used to compare the two groups in terms of satisfaction, QOL, and bite force; results were analyzed using NCSS 2007 (Number Cruncher Statistical System) and PASS 2008 Statistical Software (UT, USA). The Kolmogorov–Smirnov test was used to test the normality of the distribution. In addition to descriptive statistics (mean and standard deviation), the evaluation of quantitative data was employed with the Student’s t-test for comparing two groups with parameters of normal distribution, whereas Mann–Whitney Utest was used when normal distribution was not achieved. The qualitative data were evaluated with the Chi-square test. The significance level was set at a p value of .05.
R e s u l t s
One hundred voluntary subjects with an average age of 67.86 years (range 65– 74 years) were included in the study (35 males and 65 females). In Group I, there were 16 males and 34 females; in Group II, there were 19 males and 31
females. No statistically significant differences were detected between the mean age and gender distribution in the two groups (p ⬎.05; Table 1).
There were no statistically significant associations between VAS and OHIP-14 scores and subjects’ gender (p ⬎.05).
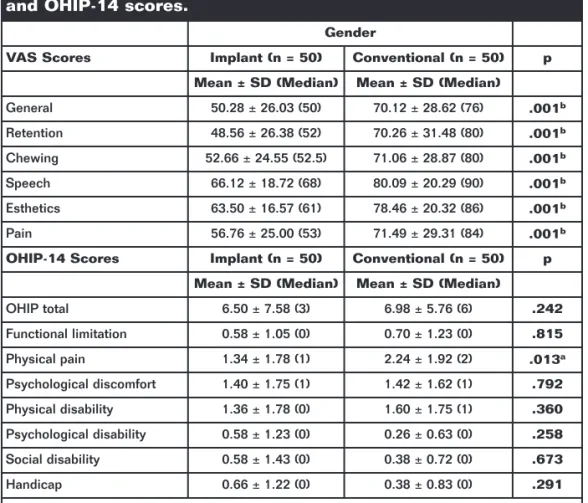
General comfort, retention, chewing, speech, esthetics, and pain scores in Group I were found to be statistically significantly higher than in Group II (p ⬍.05; Table 2). However, no statisti-cally significant differences were found between the two groups’ OHIP-14 scores (p ⬎.05) except on the physical pain subscale (p ⫽.013; Table 2).
For both groups, the MBF of the male subjects (mean 110.32 N) was found to be statistically significantly higher (p ⫽.021) than for the female subjects (mean 79.3 N). In Group I, the MBF of male subjects (mean 138.46 N) was found to be statistically significantly higher (p ⫽.027) than for the female subjects (mean 112.3 N); and in Group II, the MBF of males (mean 64.42 N) was also found to be statistically significantly higher (p ⫽.009) than for the females (mean 46.15 N).
The MBF of patients in Group I ranged from 60.5 to 305.5 N (mean 127.23 N), whereas Group II MBF values varied between 21 and 144 N (mean 53.09 N). The MBF of Group I was found to be statistically significantly higher than the MBF of Group II (p ⫽.001).
D i s c u s s i o n
Several studies9,10,24,28have reported that
patients who are treated with mandibular implant-supported overdentures are more satisfied than patients who receive a con-ventional denture. Also, the quality of their life improves with the stabilization of the mandibular complete denture.15,30-32
Additionally, implants have been found to enhance masticatory performance in various studies.8,33-35
All the reports mentioned above are subject comparisons or randomized clinical trials. In subject comparisons, subjects either compare their old and new dentures or use the new complete dentures for a period of time and, after
Table 1. The evaluation of mean age and gender distribution of the groups.
Protez Türü pa
Implant (n = 50) Conventional (n = 50)
Age (in years) 66.88 ± 6.93 68.84 ± 5.92 .302
Gender n (%) n (%) pb
Male 19 (38%) 16 (32%) .529
Female 31 (62%) 34 (68%)
they are stabilized, compare them to implants.32In randomized clinical trials,
subjects are randomly assigned into two groups receiving either new mandibular implant overdentures or new conven-tional complete dentures and the groups are compared.15,30,31
Our retrospective study is the only one to evaluate all subjects after they have been using their prosthesis for 4 years. Another important distinction was that subjects were selected from a group of patients who were functioning with their prosthesis and not seeking new dentures. MBF may vary even within the same day,35and it has been suggested that
meas-urements of participant performance often varied on different days,36but were far
more consistent when taken on the same day.36Therefore, all MBF measurements
were assessed three times in the same session for each patient and the highest value recorded was used in this study.
The null hypothesis of this study was confirmed, except for the QOL scores. In accordance with previous find-ings8,34,35at 4 years, subjects wearing
implant-supported overdentures had a greater bite force than conventional denture-wearers. Evaluation of the data from our study found that the mean bite force of subjects wearing implant-retained overdentures was more than twice as much as those wearing conven-tional dentures, which agrees with the findings of van Kampen et al.18and
Rismanchian et al.37The mean MBF
measurements found in both our study groups were lower than the findings reported by Fontijn-Tekamp et al.17and
van Kampen et al.18This difference may
be attributed to the difference in mean age and age range of the patients in these studies. The mean age of the subjects in the Fontijn-Tekamp et al.17study was
59.1 years, while the age range in the van
Kampen18study was 33–56 years. Our
patients’ age range was 65–74 years with a mean of 67.86 years, which was higher than in the previous studies.17,18The
MBF of males was found to be statisti-cally significantly higher than for females in both groups, and has also been previously reported in several other stud-ies.32,37,38Although not statistically
significant, the unbalanced proportion of male and female subjects in the two groups in our study may have influenced the results. However, it should be pointed out that there were more male subjects in the group with conventional dentures. Nonetheless, the mean bite force of subjects with implant-retained overdentures was more than double to the MBF of subjects wearing conven-tional dentures.
The satisfaction scores in subjects with mandibular two implant-supported overdentures (Group II) were found to be higher than subjects wearing conven-tional dentures, which is in agreement with the literature.9-11,24,29However, the
QOL scores of Group II in our study did not differ statistically significantly from Group I, except on the physical pain subscale, which may be associated with the lack of stability of conventional mandibular complete dentures. This finding is important because although the VAS scores indicated that complete dentures are functionally inferior, the patients wearing conventional complete dentures did not consider them to be a problem. The OHIP subscale scores in our study were not in agreement with previously published reports,15,30-32
where lower OHIP scores, indicating higher QOL, had been reported with mandibular implant-supported overden-tures. Allen and McMillan39found worse
QOL scores in subjects seeking implant-supported overdentures compared to subjects seeking conventional dentures. In our study, all the complete denture-wearers had been satisfactorily functioning with their prosthesis for 4 years and were not seeking implant-supported overdentures. This may be the reason why their QOL scores did not differ from subjects wearing mandibular two implant-supported overdentures.
Table 2. Comparison of the two study groups in terms of VAS and OHIP-14 scores.
Gender
VAS Scores Implant (n = 50) Conventional (n = 50) p
Mean ± SD (Median) Mean ± SD (Median)
General 50.28 ± 26.03 (50) 70.12 ± 28.62 (76) .001b
Retention 48.56 ± 26.38 (52) 70.26 ± 31.48 (80) .001b
Chewing 52.66 ± 24.55 (52.5) 71.06 ± 28.87 (80) .001b
Speech 66.12 ± 18.72 (68) 80.09 ± 20.29 (90) .001b
Esthetics 63.50 ± 16.57 (61) 78.46 ± 20.32 (86) .001b
Pain 56.76 ± 25.00 (53) 71.49 ± 29.31 (84) .001b OHIP-14 Scores Implant (n = 50) Conventional (n = 50) p
Mean ± SD (Median) Mean ± SD (Median)
OHIP total 6.50 ± 7.58 (3) 6.98 ± 5.76 (6) .242
Functional limitation 0.58 ± 1.05 (0) 0.70 ± 1.23 (0) .815
Physical pain 1.34 ± 1.78 (1) 2.24 ± 1.92 (2) .013a
Psychological discomfort 1.40 ± 1.75 (1) 1.42 ± 1.62 (1) .792
Physical disability 1.36 ± 1.78 (0) 1.60 ± 1.75 (1) .360
Psychological disability 0.58 ± 1.23 (0) 0.26 ± 0.63 (0) .258
Social disability 0.58 ± 1.43 (0) 0.38 ± 0.72 (0) .673
Handicap 0.66 ± 1.22 (0) 0.38 ± 0.83 (0) .291
Mann–Whitney U Test; n: number; SD: Standard deviation.
Additionally, in our opinion, the Turkish version of the OHIP-14 questionnaire is difficult to comprehend and could cause misleading results. Instead, this study should have used OHIP-EDENT, which is the modified shortened version of OHIP for edentulous patients and has proven to be more appropriate than OHIP-14 for use among edentulous sub-jects.40However, since the Turkish
version of the OHIP-EDENT has not been validated, it was not possible to use this measure in Turkey at the time we did the study. Another reason for similar OHIP scores for both denture types in our study could be the different method-ology and the absence of crossover and baseline data to adjust for the end-point outcomes. As stated previously, the sub-jects wearing complete dentures evaluated here were not able to compare their dentures with two implant-retained overdentures, thus may have expressed a higher expectation. As pointed out in a recent study,41participants in certain
ran-domized controlled trials do not pay the entire cost of their therapy, as it is the objective of the efficacy trial to test both interventions under balanced conditions. In a real-world setting, patients must bear the brunt of the cost of the therapy received. Because of the higher up-front cost of implant treatment, patients may be more critical of this therapy or may value it more highly. Either way, cost could influence the outcome of implant therapy.41
It has been established that denture wearing women present lower satisfac-tion scores than men.41-43Two studies
showed that women rated the esthetics of their dentures lower than men41,42and
the results of a randomized clinical trial showed both lower esthetic and chewing ability satisfaction scores among
women.43In our study, patient gender
did not influence patient satisfaction or QOL scores. This contradictory result may have been caused by the unequal distribution of male and female subjects (65 females and 35 males) or the socioeconomic status of the subjects evaluated here.
Our study had two limitations. One limitation was the absence of the
validated Turkish version of the OHIP-EDENT at the time of the study; therefore, the Turkish version of OHIP-14 had to be used for the assessment of the OHRQL. The other limitation was the absence of baseline data to adjust for the end-point outcomes.
C o n c l u s i o n
Within the limitations of this study, it can be concluded that after a 4-year adaptation time, the Turkish translated OHIP questionnaire failed to demon-strate any difference between subjects wearing mandibular two implant-retained overdentures and subjects wearing conventional complete dentures, except on the pain subscale. However, subjects wearing mandibular two implant-retained overdentures were found to have higher bite forces and greater patient satisfaction scores.
R e f e r e n c e s
1. Mojon P, Thomason JM, Walls AW. The impact of falling rates of edentulism. Int J Prosthodont2004;17:434-40.
2. Douglass CW, Shih A, Ostry L. Will there be a need for complete dentures in the United States in 2020? J Prosthet Dent2002;87: 5-8.
3. Locker D. Measuring oral health: a conceptual framework. Community Dent Health1988;5:3-18.
4. Mericske-Stern RD, Taylor TD, Belser U. Management of the edentulous patient.
Clin Oral Implants Res2000;1:108-25. 5. Gift HC, Redford M. Oral health and the
quality of life. Clin Geriatr Med1992;8: 673-83.
6. Marcus SE, Drury TF, Brown LJ, Zion GR. Tooth retention and tooth loss in the permanent dentition of adults: United States, 1988-1991. J Dent Res1996;75: 684-95.
7. de Grandmont P, Feine JS, Taché R, et al. Within-subject comparisons of implant-supported mandibular prostheses: psychometric evaluation. J Dent Res
1994;73:1096-104.
8. Feine JS, Maskawi K, de Grandmont P, Donohue WB, Tanguay R, Lund JP. Within-subject comparisons of implant-supported
mandibular prostheses: evaluation of masticatory function. J Dent Res1994;73: 1646-56.
9. Boerrigter EM, Stegenga B, Raghoebar GM, Boering G. Patient satisfaction and chewing ability with implant-retained mandibular overdentures: a comparison with new com-plete dentures with or without preprosthetic surgery. J Oral Maxillofac Surg
1995;53:1167-73.
10. Boerrigter EM, Geertman ME, Van Oort RP, et al. Patient satisfaction with implant-retained mandibular overdentures. A comparison with new complete dentures not retained by implants-a multicentre ran-domized clinical trial. Br J Oral Maxillofac Surg1995;33:282-8.
11. Geertman ME, Boerrigter EM, Van’t Hof MA, et al. Two-center clinical trial of implant-retained mandibular overdentures versus complete dentures-chewing ability.
Community Dent Oral Epidemiol1996;24: 79-84.
12. Geertman ME, van Waas MA, van’t Hof MA, Kalk W. Denture satisfaction in a compara-tive study of implant-retained mandibular overdentures: a randomized clinical trial. Int J Oral Maxillofac Implants1996;11:194-200. 13. Bouma J, Boerrigter LM, van Oort RP, van
Sonderen E, Boering G. Psychosocial effects of implant-retained overdentures. Int J Oral Maxillofac Implants1997;12:515-22. 14. Tang L, Lund JP, Taché R, Clokie CM, Feine
JS. A within-subject comparison of mandibular long-bar and hybrid implant-supported prostheses: evaluation of masticatory function. J Dent Res1999; 78:1544-53.
15. Awad MA, Lund JP, Dufresne E, Feine JS. Comparing the efficacy of mandibular implant-retained overdentures and conventional dentures among middle-aged edentulous patients: satisfaction and functional assessment. Int J Prosthodont
2003;16:117-22.
16. Feine JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Mandibular two-implant overdentures as first choice standard of care for edentulous patients. Int J Oral Maxillofac Implants2002;17:601-2.
17. Fontijn-Tekamp FA, Slagter AP, van’t Hof MA, Geertman ME, Kalk W. Bite forces with mandibular implant-retained overdentures.
18. van Kampen FM, van der Bilt A, Cune MS, Bosman F. The influence of various attach-ment types in mandibular implant-retained overdentures on maximum bite force and EMG. J Dent Res2002;81:170-3.
19. van Kampen FM, van der Bilt A, Cune MS, Fontijn-Tekamp FA, Bosman F. Masticatory function with implant-supported overden-tures. J Dent Res2004;83:708-11.
20. Heckmann SM, Heussinger S, Linke JJ, Graef F, Prˆschel P. Improvement and long-term stability of neuromuscular adaptation in implant-supported overdentures. Clin Oral Implants Res2009;20:1200-5.
21. Boretti G, Bickel M, Geering AH. A review of masticatory ability and efficiency.
J Prosthet Dent1995;74:400-3.
22. McGarry TJ, Nimmo A, Skiba JF, Ahlstrom RH, Smith CR, Koumjian JH. Classification system for complete edentulism. The American College of Prosthodontics.
J Prosthodont1999;8:27-39.
23. Geckili O, Bilhan H, Bilgin T. Locator attach-ments as an alternative to ball attachattach-ments in 2-implant retained mandibular overdentures.
J Can Dent Assoc2007;73:679-82. 24. Timmerman R, Stoker GT, Wismeijer D,
Oosterveld P, Vermeeren JI, van Waas MA. An eight-year follow-up to a randomized clinical trial of participant satisfaction with three types of mandibular implant-retained overdentures. J Dent Res2004;83:630-3. 25. Slade GD, Spencer AJ. Development and
evaluation of the oral health impact profile.
Community Dent Health1994;11:3-11. 26. Bilhan H, Geckili O, Sulun T, Bilgin T. A
quality-of-life comparison between self-aligning and ball attachment systems for
2-implant-retained mandibular overden-tures. J Oral Implantol2011;37:167-73. 27. Slade GD. Derivation and validation
of a short-form oral health impact profile.
Community Dent Oral Epidemiol1997;25: 284-90.
28. Mumcu G, Inanc N, Ergun T, et al. Oral health related quality of life is affected by disease activity in Behçet’s disease. Oral Dis
2006;12:145-51.
29. Cune MS, de Putter C, Hoogstraten J. Treatment outcome with implant-retained overdentures: part II—patient satisfaction and predictability of subjective treatment outcome. J Prosthet Dent1994;72:152-8. 30. Allen PF, McMillan AS, Walshaw D. A
patient-based assessment of implant-stabilized and conventional complete dentures. J Prosthet Dent2001;85:141-7. 31. Heydecke G, Locker D, Awad MA, Lund JP,
Feine JS. Oral and general health-related quality of life with conventional and implant dentures. Community Dent Oral Epidemiol
2003;31:161-8.
32. Geckili O, Bilhan H, Bilgin T. Impact of mandibular two-implant retained overden-tures on life quality in a group of elderly Turkish edentulous patients. Arch Gerontol Geriatr2011;53:233-6.
33. Fontijn-Tekamp FA, Slagter AP, Van Der Bilt A, et al. Biting and chewing in overdentures, full dentures, and natural dentitions. J Dent Res2000;79:1519-24.
34. Bakke M, Holm B, Gotfredsen K.
Masticatory function and patient satisfaction with implant-supported mandibular overdentures: a prospective 5-year study.
Int J Prosthodont2002;15:575-81.
35. van der Bilt A, van Kampen FM, Cune MS. Masticatory function with mandibular implant-supported overdentures fitted with different attachment types. Eur J Oral Sci2006;114:191-6.
36. Paphangkorakit J, Osborn JW. Effects on human maximum bite force of biting on a softer or harder object. Arch Oral Biol1998; 43:833-9.
37 Rismanchian M, Bajoghli F, Mostajeran Z, Fazel A, Eshkevari P. Effect of implants on maximum bite force in edentulous patients.
J Oral Implantol2009;35:196-200. 38. Lassila V, Holmlund I, Koivumaa KK. Bite
force and its correlations in different denture types. Acta Odontol Scand1985;43: 127-32.
39. Allen PF, McMillan AS. A longitudinal study of quality of life outcomes in older adults requesting implant prostheses and complete removable dentures. Clin Oral Implants Res
2003;14:173-9.
40. Allen F, Locker D. A modified short version of the oral health impact profile for assessing health-related quality of life in edentulous adults. Int J Prosthodont2002; 15:446-50.
41. Rashid F, Awad MA, Thomason JM, et al. The effectiveness of 2-implant overdentures— a pragmatic international multicentre study.
J Oral Rehabil2011;38:176-84. 42. Mersel A, Babayof I, Berkey D, Mann J.
Variables affecting denture satisfaction in Israeli elderly: a one year follow-up.
Gerodontology1995;12:89-94. 43. Pan S, Awad M, Thomason JM, et al.
Sex differences in denture satisfaction.