ry cytokine transforming growth factor β1 (TGFβ1) may have a complex role in carcinogenesis.
TGFβ1 is a polypeptide that regulates cell growth and differentiation, immune modulation, wound healing, and embryogenesis [8]. Research-ers have proved that TGFβ1 plays a dual role in carcinogenesis, acting as a tumor suppressor in the early stages and as a tumor promoter in later stag-es, by enhancing tumor cell motility, immunosup-pression and invasiveness [9, 10].
Several genetic variants in the TGFβ1 gene have previously been identified. Some of these Lung cancer is the most common type of
can-cer and the main cause of cancan-cer-related mor-tality worldwide, leading to more than a million deaths annually [1]. Even though epidemiological research has revealed more than 80% of lung can-cers are attributed to tobacco, few smokers develop lung cancer [2]. Recent evidence suggests that ge-netic susceptibility may play a central role in carci-nogenesis [3–5]. Moreover, numerous reports have demonstrated that single nucleotide polymorphisms (SNPs) in cytokine genes are associated with suscep-tibility to cancer [6, 7]. Therefore,
anti-inflammato-*Zhaomin Deng
A–F, *Yuan Yang
A–F, Xiaojun Huang
A–F, Yu Kuang
A–F,
Zhen Qin
B–F, Baoning Wang
B–F, Hongren Wang
B–F, Mingyuan Li
A–FPolymorphisms of TGFβ1T+869C and C-509T
with Lung Cancer Risk: A Meta-analysis**
Department of Microbiology, West China School of Preclinical and Forensic Medicine, Sichuan University
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article
Abstract
Background. Lung cancer is the most common malignancy worldwide. A better understanding of the mechanisms may contribute to early diagnosis and establishment of new therapeutic targets.
Objectives. A meta-analysis was performed to investigate the association of transforming growth factor-beta 1 (TGFβ1) T+869C and C-509T polymorphisms with lung cancer susceptibility.
Material and Methods. Relevant studies were identified through PubMed, Medline, Embase and CNKI databases. The pooled odds ratios (ORs) with its 95% confidence intervals (CIs) were employed to assess these associations in a fixed- or random-effects model.
Results. For the TGFβ1 T+869C polymorphism, 5 published case-control studies with 1167 cases and 1365 con-trols were included. Overall, no significant association was found between the TGFβ1 T+869C polymorphism and lung cancer susceptibility under any genetic models in the total population (p > 0.05). A subgroup analysis by ethnicity showed no significant association among the Asian population as well, while a significant association was observed in Caucasian descendants. For the TGFβ1 C-509T polymorphism, 4 studies were considered, includ-ing 1029 cases and 1133 controls. However, this polymorphism also did not increase the risk of lung cancer in all genetic comparison models.
Conclusions. This meta-analysis suggests that TGFβ1 T+869C and C-509T polymorphisms may not contribute to lung cancer risk in the total population, while the T+869C polymorphism may increase the risk of lung cancer in the Caucasian population. However, many studies are still required to evaluate these associations in large popu-lations (Adv Clin Exp Med 2016, 25, 6, 1165–1172).
Key words: lung cancer, polymorphism, meta-analysis, transforming growth factor-beta 1.
ORIGINAL PAPERS
Adv Clin Exp Med 2016, 25, 6, 1165–1172
DOI: 10.17219/acem/36603 © Copyright by Wroclaw Medical University ISSN 1899–5276
* These authors contributed equally to this work.
Z. Deng et al.
1166
variants are associated with TGFβ1 produc-tion [11, 12]. A functional polymorphism in the TGFβ1 gene, a T-to-C substitution at nucleotide 29 of codon 10, leading to a replacement of leucine to proline (TGFβ1 T+869C, rs1982073), was locat-ed in the hydrophobic core of the signal peptide. This transition was shown to be related to higher circulating levels of TGFβ1 [13, 14]. Another poly-morphism, a C-to-T substitution at nucleotide 506 (TGFβ1 C-509T, rs1800469), is associated with in-creased susceptibility and severity of asthma, risk of developing breast cancer and Alzheimer’s dis-ease [15–17]. This variant is located in the nega-tive regulatory region, leading differential genetic regulation of TGFβ1 plasma levels [13].
Genetic variants which influence TGFβ1 ex-pression and protein serum levels may have an impact on lung cancer development and progno-sis. Furthermore, several articles have investigated the role of the TGFβ1 T+869C and C-509T poly-morphisms in the etiology of lung cancer. How-ever, the data from these studies was inconsistent. Hence, we conducted this meta-analysis to evalu-ate the associations of these polymorphisms with lung cancer risk.
Material and Methods
Selection of Studies
Relevant studies were identified by a com-puterized literature search of the Embase, Med-line, PubMed, Wanfang and CNKI (China Nation-al Knowledge Infrastructure) electronic data bases (prior to March 2014) using the following words and terms: lung cancer, lung carcinoma, transform-ing growth factor beta 1, TGFβ1, polymorphism, variant and mutation as well as their combinations. We also manually screened the references of the re-trieved articles to obtain more relevant articles.
Criteria for Inclusion
The inclusion criteria were as follows:
1. The paper should be a case-control study evaluating the association between lung cancer and TGFβ1 polymorphisms;
2. Each study involved T+869C and/or C-509T polymorphisms of the TGFβ1 gene;
3. The results were expressed as odds ratio (ORs) with its corresponding 95% confidence in-terval (CI);
4. Genotype distribution information of the control for each polymorphism must be in Hardy-Weinberg equilibrium (HWE).
Quality Assessment
and Data Extraction
Two investigators evaluated the quality of the screened studies independently. Any disagreement was discussed with a third expert to reach a con-sensus. The following information was collected from each study included: the first author’s name, published year, country where the study was con-ducted, ethnicity and sample size of the cases and controls, and genotype distribution of the TT, TC, and CC.
Statistical Analysis
OR with 95% CI was used to measure the strength of association of the T+869C and C-509T polymorphisms with lung cancer risk. The z-test was employed to determine the significance of the pooled OR (p < 0.05). For all the polymorphisms, the genetic models (allelic model, co-dominant ef-fects, dominant effect and recessive effect) were examined. The Cochran’s Q statistics test was used to assess the heterogeneity among the stud-ies (p ≤ 0.1 was considered significant) [18, 19]. The random-effect model (DerSimonian and Laird method) was used when the effects were hetero-geneous [20], whereas the fixed-effect model (the inverse variance-weighted method) was used in its absence [21]. To evaluate whether our results were affected by each individual study, a sensitivity analysis was conducted by systematically removing each study one time and recalculating the pooled ORs. Publication bias was investigated by using a funnel plot, in which the standard error of log (OR) of each study was plotted against its OR [22]. Hardy-Weinberg equilibrium was tested using the χ2-test for goodness of fit or Fisher’s exact
prob-ability test, where appropriate. P < 0.05 was con-sidered significant. All statistical tests for this me-ta-analysis were performed with Review Manager (v. 5.2; the Cochrane Collaboration, Oxford, UK). All p-values were two-sided.
Results
Study Characteristics
For the T+869C polymorphism, 5 relevant studies with a total number of 1167 cases and 1365 controls were included in the meta-analy-sis [23–27]. Of these studies, 3 were conducted on Asian populations, and 2 on Caucasian descen-dants. For the C-509T polymorphism, 4 case-control studies met our inclusion criteria, includ-ing 1029 cases and 1133 controls [23, 25, 26, 28]. All these studies were conducted on Asian popula-tions. The main study characteristics are summa-rized in Table 1.
Association Between TGFβ1
T+869C Polymorphism and
Lung Cancer Risk
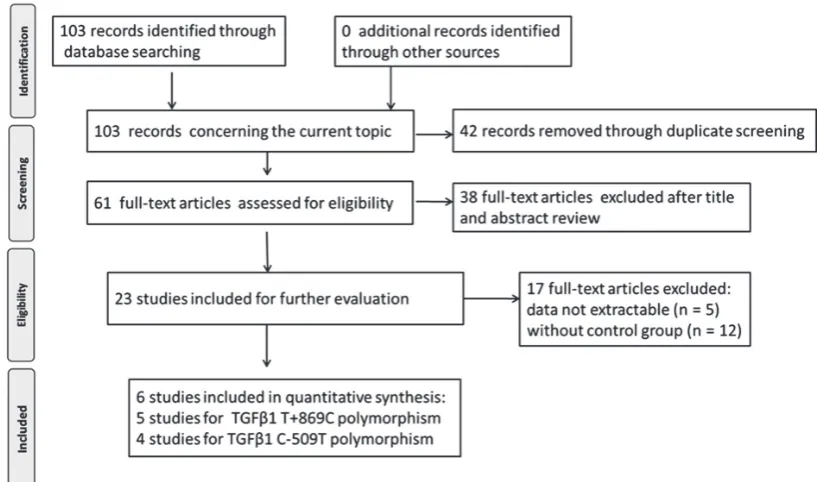
Table 2 lists the results of each comparison model in this meta-analysis. In the overall analy-sis, we found that the frequency of the C allele in the T+869C polymorphism is a little higher in lung cancer patients than in the healthy controls (48.4% vs. 44.4%). However, no significant association was found between the TGFβ1 T+869C polymor-Fig. 1. Literature search and study selection procedures
Table 1. Main characteristics of included studies in this meta-analysis
First author Year Country Ethnicity Total number Cases Controls cases controls CC CT TT CC CT TT
TGFβ1 T+869C
Kang HG 2006 Korea Asian 432 432 107 200 125 108 218 106
Park KH 2006 Korea Asian 194 283 43 97 53 58 133 87
Colakogullari M 2008 Turkey Caucasian 43 59 10 24 9 10 20 20 Teixeira AL 2011 Portugal Caucasian 305 380 53 165 87 44 166 170
Bai L 2013 China Asian 193 211 55 107 31 58 105 47
TGFβ1 C-509T
Kang HG 2006 Korea Asian 432 432 131 197 104 104 223 105
Park KH 2006 Korea Asian 194 283 53 100 41 84 137 62
Li T 2012 China Asian 210 208 18 87 105 36 92 80
Z. Deng et al.
1168
phism and lung cancer susceptibility under any ge-netic model (C vs. T: p = 0.12; CC vs. TT: p = 0.12; CT vs. TT: p = 0.13; CC + CT vs.TT: p = 0.12; CC vs. CT + TT: p = 0.22).
In the stratified analysis by ethnicity, we did not find a significantly association between the TGFβ1 T+869C polymorphism and cancer risk in the Asian descendants groups as well. Howev-er, significant association was observed in Cauca-sian descendants (C vs. T: p < 0.00001; CC vs. TT: p = 0.0002; CT vs. TT: p < 0.0001; CC + CT vs. TT: p < 0.00001; CC vs. CT + TT: p = 0.03), as shown in Fig. 2. No significant heterogeneity was found
between the included studies in Caucasian descen-dants (I2 = 0%).
Association Between TGFβ1
C-509T Polymorphism and Lung
Cancer Risk
Overall, there was no association between the TGFβ1 C-509T polymorphism and lung cancer risk in all genetic models (T vs. C: p = 0.39; TT vs. CC: p = 0.35; CT vs. CC: p = 0.49; CT + TT vs. CC: p = 0.40; TT vs. CT + CC: p = 0.26). Table 3
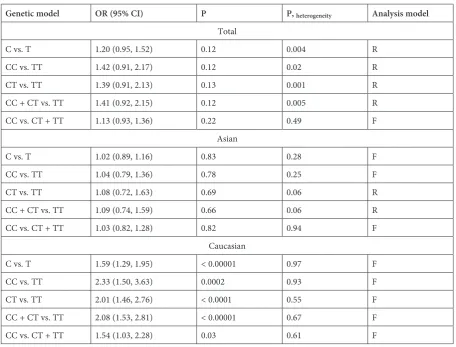
Table 2. Stratified analysis of TGFß1 T+869C polymorphism with lung cancer risk
Genetic model OR (95% CI) P P, heterogeneity Analysis model
Total
C vs. T 1.20 (0.95, 1.52) 0.12 0.004 R
CC vs. TT 1.42 (0.91, 2.17) 0.12 0.02 R
CT vs. TT 1.39 (0.91, 2.13) 0.13 0.001 R
CC + CT vs. TT 1.41 (0.92, 2.15) 0.12 0.005 R
CC vs. CT + TT 1.13 (0.93, 1.36) 0.22 0.49 F
Asian
C vs. T 1.02 (0.89, 1.16) 0.83 0.28 F
CC vs. TT 1.04 (0.79, 1.36) 0.78 0.25 F
CT vs. TT 1.08 (0.72, 1.63) 0.69 0.06 R
CC + CT vs. TT 1.09 (0.74, 1.59) 0.66 0.06 R
CC vs. CT + TT 1.03 (0.82, 1.28) 0.82 0.94 F
Caucasian
C vs. T 1.59 (1.29, 1.95) < 0.00001 0.97 F
CC vs. TT 2.33 (1.50, 3.63) 0.0002 0.93 F
CT vs. TT 2.01 (1.46, 2.76) < 0.0001 0.55 F CC + CT vs. TT 2.08 (1.53, 2.81) < 0.00001 0.67 F
CC vs. CT + TT 1.54 (1.03, 2.28) 0.03 0.61 F
F – fixed-effect model; R – random-effect model.
Table 3. Meta-analysis of the TGFβ1 C-509T polymorphism on lung cancer risk
Genetic model OR (95% CI) P P heterogeneity Analysis model
T vs. C 1.11 (0.87, 1.42) 0.39 0.01 R
TT vs. CC 1.27 (0.77, 2.08) 0.35 0.01 R
CT vs. CC 1.17 (0.75, 1.83) 0.49 0.01 R
CT+TT vs. CC 1.22 (0.77, 1.94) 0.40 0.04 R
TT vs. CT+CC 1.12 (0.92, 1.35) 0.26 0.22 F
shows the TGFβ1 C-509T polymorphism on lung cancer risk.
Sensitivity Analyses and
Publication Bias
The corresponding pooled ORs were not ma-terially changed when a single included study was deleted each time. This procedure confirms the stability of our overall result.
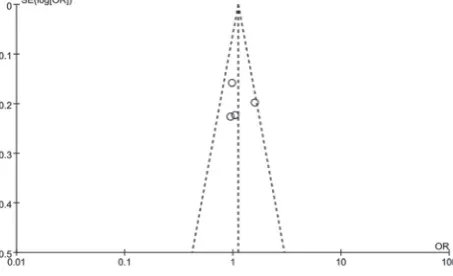
The shape of the funnel plots does not reveal any evidence of funnel plot asymmetry as shown in Fig. 3 and Fig. 4, indicating no publication bias was present.
Discussion
Genetic susceptibility to cancers has led to growing attention to the studies of the polymor-phism genes involved in carcinogenesis [29–31]. TGFβ1 is a multifunctional cytokine that is essen-tial for maintaining homeostasis involving bone and muscle differentiation, immune response, and tumor suppression [32, 33]. This cytokine, which induces cell proliferation and apoptosis, plays a key role in various types of cancers [34–36]. There is evidence that TGFβ1 functions as a tumor initia-tion suppressor, but as a tumor progression pro-moter when the proliferative inhibition effect of the TGFβ1 signaling pathway has been overridden by other oncogenic mutations [37, 38].
Z. Deng et al.
1170
A catalog of 106 single-nucleotide polymor-phisms (SNPs) and 11 other types of variations in the TGFβ1 gene and its signaling pathway have been identified, and a few of these have been as-sociated with human diseases [39]. Among the dif-ferent polymorphisms of TGFβ1, the polymor-phisms of C-509T and T+869C have been most intensively studied. Researchers have reported that C-509T and T+869C are significantly related to the disease-free survival of breast cancer patients in a large Chinese population [40]. Furthermore, the C-509T polymorphism of promoter region in the TGFβ1 has been shown to be associated with increased transcriptional activity with a gene dose effect [16]; the T+869C gives rise to a Leu to Pro substitution at amino acid residue 10 in the sig-nal peptide sequence and to increased formation of TGFβ1 [41]. Both of those SNPs have been shown to have a protective effect on hepatocellular carci-noma in Korean patients with chronic hepatitis B virus infection [42]. However, few reports have been conducted on the association between the SNPs of TGFβ1 and lung cancer risk.
To systematically explore the association be-tween TGFβ1 C-509T and T+869C polymorphisms and lung cancer risk, we conducted a meta-analysis of relevant studies. This meta-analysis, including 1166 cases and 1359 controls from 5 studies, ex-plored the association between the TGFβ1 T+869C polymorphism and cancer risk. We found that the TGFβ1 T+869C polymorphism was not signifi-cantly associated with cancer risk in overall com-parisons, compared to wild homozygotes. Using stratified analysis for ethnicity, the T+869C poly-morphism showed a significantly increased lung cancer risk in the Caucasian group. However, this association was not found among the Asian group.
For the TGFβ1 C-509T polymorphism, our meta-analysis analyzed 4 studies, including 1029 cases and 1133 controls. All of these 4 studies were conducted in the Asian population. We found that variant homozygotes or heterozygotes of the C-509T polymorphism were not associated with cancer risk in overall comparisons; the insignifi-cance of this relationship holds up under various genetic models. Our results are consistent with all the studies on lung cancer. While 1 study demon-strated that the TGFβ1 C-509T polymorphism was associated with higher lung cancer risk [25], this association is not significant according to our pres-ent meta-analysis.
TGFβ1 polymorphisms are associated with many human diseases. Wei et al. have suggested that TGFβ1 T+869C was a low-penetrant risk fac-tor for prostate cancer and cancer in Asians [43]. Liu et al. have proved that that the TGFβ1 C-509T polymorphism might contribute to a decreased risk of colorectal cancer susceptibility, especial-ly for Caucasians [44]. Hou et al. have demon-strated that serum TGFβ1 levels were significant-ly higher in patients with lung cancer compared to healthy volunteers [45]. Polymorphisms in TGFβ1 may influence its levels. A previous meta-analysis conducted by He et al. suggested that the T+869C polymorphism of TGFβ1 is associated with radi-ation pneumonia risk only in Caucasians, while there may be no association between the C509T polymorphism and radiation pneumonia risk [46].
Several limitations of this meta-analysis should be addressed. Firstly, the original information was insufficient and the assessment of potential inter-actions is limited. Secondly, the number of pub-lished studies was small and insufficient for com-prehensive analyses, particularly for lung cancer. Thirdly, a more precise analysis should be con-ducted if individual information, including other covariates such as age, sex and smoking condition, becomes available.
In conclusion, research on the relationship be-tween TGFβ1 polymorphisms and lung cancer is of Fig. 3. Funnel plot of T+869C polymorphism and cancer
risk for publication bias among Caucasian population
intense interest but is in conflict at present. Our me-ta-analysis suggests that the TGFβ1 T+869C allele is not significantly associated with lung cancer risk, especially in the Asian group, while a significant association was observed in the Caucasian group.
TGFβ1 C-509T polymorphism was also not asso-ciated with lung cancer risk. However, large trials, containing large numbers of cases and controls, and gene-environment interactions, should be consid-ered to evaluate the association in further analyses.
References
[1] The World Cancer Report: The major findings. Cent Eur J Public Health 2002, 11, 177–179.
[2] Wu X, Zhao H, Suk R, Christiani DC: Genetic susceptibility to tobacco-related cancer. Oncogene 2004, 23, 6500– –6523.
[3] Thorgeirsson TE, Geller F, Sulem P: A variant associated with nicotine dependence, lung cancer and peripheral arterial disease. Nature 2008, 452, 638–642.
[4] Hung RJ, McKay JD, Gaborieau V: A susceptibility locus for lung cancer maps to nicotinic acetylcholine receptor subunit genes on 15q25. Nature 2008, 452, 633–637.
[5] Wang Y, Broderick P, Webb E: Common 5p15.33 and 6p21.33 variants influence lung cancer risk. Nat Genet 2008, 40, 1407–1409.
[6] Shimura T, Hagihara M, Takebe K: The study of tumor necrosis factor beta gene polymorphism in lung cancer patients. Cancer 1994, 73, 1184–1188.
[7] Seifart C, Plagens A, Dempfle A: TNF-alpha, TNF-beta, IL-6, and IL-10 polymorphisms in patients with lung cancer. Dis Markers 2005, 21, 157–165.
[8] Huang XF, Chai Y: Molecular regulatory mechanism of tooth root development. Int J Oral Sci 2012, 4, 177–181.
[9] Siegel PM, Massague J: Cytostatic and apoptotic actions of TGF-beta in homeostasis and cancer. Nat Rev Cancer 2002, 3, 807–821.
[10] Gordon KJ, Blobe GC: Role of transforming growth factor-beta superfamily signaling pathways in human disease. Biochim Biophys Acta 2008, 1782, 197–228.
[11] Dunning AM, Ellis PD, McBride S: A transforming growth factorbeta1 signal peptide variant increases secretion
in vitro and is associated with increased incidence of invasive breast cancer. Cancer Res 2002, 63, 2610–2615.
[12] Suthanthiran M, Li B, Song JO: Transforming growth factor-beta 1 hyperexpression in African-American hyperten-sives: A novel mediator of hypertension and/or target organ damage. Proc Natl Acad Sci USA 2000, 97, 3479–3484.
[13] Grainger DJ, Heathcote K, Chiano M: Genetic control of the circulating concentration of transforming growth factor type beta1. Hum Mol Genet 1999, 8, 93–97.
[14] Yokota M, Ichihara S, Lin TL, Nakashima N, Yamada Y: Association of a T29-->C polymorphism of the trans-forming growth factor-beta1 gene with genetic susceptibility to myocardial infarction in Japanese. Circulation 2000, 101, 2783–2787.
[15] Luedecking EK, DeKosky ST, Mehdi H, Ganguli M and Kamboh MI: Analysis of genetic polymorphisms in the transforming growth factor-beta1 gene and the risk of Alzheimer’s disease. Hum Genet 2000, 106, 565–569.
[16] Silverman ES, Palmer LJ, Subramaniam V: Transforming growth factor-beta1 promoter polymorphism C-509T is associated with asthma. Am J Respir Crit Care Med 2004, 169, 214–219.
[17] Saha A, Gupta V, Bairwa NK, Malhotra D and Bamezai R: Transforming growth factor-beta1 genotype in spo-radic breast cancer patients from India: Status of enhancer, promoter, 5’-untranslated-region and exon-1 polymor-phisms. Eur J Immunogenet 2004, 31, 37–42.
[18] Lau J, Ioannidis JP, Schmid CH: Quantitative synthesis in systematic reviews. Ann Intern Med 1997, 127, 820–826.
[19] Berman NG, Parker RA: Meta-analysis: Neither quick nor easy. BMC Med Res Methodol 2002, 2, 10.
[20] Mantel N, Haenszel W: Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst 1959, 22, 719–748.
[21] DerSimonian R, Laird N: Meta-analysis in clinical trials. Control Clin Trials 1986, 7, 177–188.
[22] Egger M, Davey Smith G, Schneider M and Minder C: Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634.
[23] Bai L, Yu H, Wang H, Su H, Zhao J, Zhao Y: Genetic single-nucleotide polymorphisms of inflammation-related factors associated with risk of lung cancer. Med Oncol 2013, 30, 414.
[24] Teixeira AL, Araujo A, Coelho A: Influence of TGFB1+869T>C functional polymorphism in non-small cell lung cancer (NSCLC) risk. J Cancer Res Clin Oncol 2011, 137, 435–439.
[25] Park KH, Lo Han SG, Whang YM: Single nucleotide polymorphisms of the TGFB1 gene and lung cancer risk in a Korean population. Cancer Genet Cytogenet 2006, 169, 39–44.
[26] Kang HG, Chae MH, Park JM: Polymorphisms in TGF-beta1 gene and the risk of lung cancer. Lung Cancer 2006, 52, 1–7.
[27] Colakogullari M, Ulukaya E, Yilmaztepe Oral A: The involvement of IL-10, IL-6, IFN-gamma, TNF-alpha and TGF-beta gene polymorphisms among Turkish lung cancer patients. Cell Biochem Funct 2008, 26, 283–290.
[28] Li T, Ren J, Ma Y: Correlation of transforming growth factor-β 1 gene –509C/T polymorphism and genetic suscep-tibility to non-small cell lung cancer in Chinese population. Chinese Journal of Cancer Prevention and Treatment 2012, 19, 410–414.
Z. Deng et al.
1172
[30] Saltzman BS, Yamamoto JF, Decker R: Association of genetic variation in the transforming growth factor beta-1 gene with serum levels and risk of colorectal neoplasia. Cancer Res 2008, 68, 1236–1244.
[31] Garcia-Gonzalez MA, Strunk M, Piazuelo E: TGFB1 gene polymorphisms: their relevance in the susceptibility to
Helicobacter pylori-related diseases. Genes Immun 2006, 7, 640–646.
[32] Alliston T, Choy L, Ducy P, Karsenty G, Derynck R: TGF-beta-induced repression of CBFA1 by Smad3 decreases cbfa1 and osteocalcin expression and inhibits osteoblast differentiation. EMBO J 2001, 20, 2254–2272.
[33] Derynck R, Akhurst RJ, Balmain A: TGF-beta signaling in tumor suppression and cancer progression. Nat Genet 2001, 29, 117–129.
[34] Zhang L, Yang M, Bi N: Association of TGF-beta1 and XPD polymorphisms with severe acute radiation-induced esophageal toxicity in locally advanced lung cancer patients treated with radiotherapy. Radiother Oncol 2010, 97, 19–25.
[35] Cai Q, Tang Y, Zhang M: TGFbeta1 Leu10Pro polymorphism contributes to the development of prostate cancer: Evidence from a meta-analysis. Tumour Biol 2013, 35, 667–673.
[36] Huang Y, Li B, Qian J, Xie J, Yu L: TGF-beta1 29T/C polymorphism and breast cancer risk: A meta-analysis involving 25 996 subjects. Breast Cancer Res Treat 2010, 123, 863–868.
[37] Massague J: TGF beta in cancer. Cell 2008, 134, 215–230.
[38] Adorno M, Cordenonsi M, Montagner M: A mutant-p53/Smad complex opposes p63 to empower TGFbeta-induced metastasis. Cell 2009, 137, 87–98.
[39] Watanabe Y, Kinoshita A, Yamada T: A catalog of 106 single-nucleotide polymorphisms (SNPs) and 11 other types of variations in genes for transforming growth factor-beta1 (TGF-beta1) and its signaling pathway. J Hum Genet 2002, 47, 478–483.
[40] Shu XO, Gao YT, Cai Q: Genetic polymorphisms in the TGF-beta 1 gene and breast cancer survival: A report from the Shanghai Breast Cancer Study. Cancer Res 2004, 64, 836–839.
[41] Crilly A, Hamilton J, Clark CJ, Jardine A, Madhok R: Analysis of transforming growth factor beta1 gene poly-morphisms in patients with systemic sclerosis. Ann Rheum Dis 2002, 61, 678–681.
[42] Kim YJ, Lee HS, Im JP: Association of transforming growth factor-beta1 gene polymorphisms with a hepatocel-lular carcinoma risk in patients with chronic hepatitis B virus infection. Exp Mol Med 2003, 35, 196–202.
[43] Wei BB, Xi B, Wang R: TGFβ1 T29C polymorphism and cancer risk: A meta-analysis based on 40 case-control studies. Cancer Genet Cytogenet 2010, 196, 68–75.
[44] Liu Y, Lin XF, Lin CJ, Jin SS, Wu JM: Transforming growth factor beta-1 C-509T polymorphism and cancer risk: A meta-analysis of 55 case-control studies. Asian Pac J Cancer Prev 2012, 13, 4683–4688.
[45] Hou YL, Chen H, Dong ZH: Clinical significance of serum transforming growth factor-β1 in lung cancer. Cancer Epidemiol 2013, 37, 750–753.
[46] He J, Deng L, Na F, Xue J, Gao H, Lu Y: The association between TGF-β1 polymorphisms and radiation pneu-monia in lung cancer patients treated with definitive radiotherapy: A meta-analysis. PLoS One 2014, 9, e91100.
Address for correspondence:
Mingyuan Li
Department of Microbiology
West China School of Preclinical and Forensic Medicine Sichuan University
Chengdu Sichuan 610041 China
Tel.: +86 028 85 50 12 67 E-mail: [email protected]
Conflict of interest: None declared