Jacek Gajek
1, Dorota Zyśko
2, Anil K. Agrawal
3, Jerzy Rudnicki
4Patients with Atrioventricular Block
During Tilt Test-Induced Vasovagal Syncope
Pacjenci z blokiem przedsionkowo-komorowym
podczas testu pochyleniowego
1 Department of Cardiology, Wroclaw Medical University, Wrocław, Poland
2 Department of Emergency Medicine, Wroclaw Medical University, Wrocław, Poland
3 2nd Department and Clinic of General and Oncological Surgery, Wroclaw Medical University, Wrocław,
Poland
4 Department of Minimally Invasive Surgery and Proctology, Wroclaw Medical University, Wrocław, Poland
Abstract
Background. Sinus bradycardia or sinus arrest are the most prevalent rhythms during a cardioinhibitory type of neurocardiogenic reaction, while atrioventricular block (AVB) occurs rarely.
Objectives. The aim of the study was to compare the medical histories and tilt test (TT) findings among patients with and without AVB during a positive TT.
Material and Methods. The study group consisted of 578 vasovagal patients with positive TTs. Among them there were 34 patients with AVB, which constituted 5.9% of the total study group. The medical histories and TT data were analyzed. The TTs were performed according to the Italian protocol.
Results. The medical histories of patients with AVB showed a significantly higher incidence of syncope-related traumatic injuries requiring hospitalization. AVB occurrence was found to be independently related to a history of instrumentation-injection-blood (IIB) phobia and to the duration of the PR interval on a baseline electrocardio-gram. Receiver operating characteristic (ROC) analysis revealed that a PR interval ≤ 177 ms in duration differenti-ates patients without and with AVB during a neurocardiogenic reaction. It was also shown that other factors related to AVB occurrence include a shorter duration of the slowing of the heart rate and syncope as a TT outcome.
Conclusions. Patients with AVB during TT differ from those without AVB. Sudden onset of a syncopal event, particularly in women or in patients of either gender with instrumentation-injection-blood (IIB) phobia, can be an indicator for AVB during vasovagal syncope. The population of subjects with AVB during TT is not homogenous; it consists of a younger subgroup with IIB phobia, and an older subgroup with a concealed organic AV node dys-function (Adv Clin Exp Med 2011, 20, 3, 305–312).
Key words: vasovagal syncope, tilt test, atrioventricular block.
Streszczenie
Wprowadzenie. Bradykardia zatokowa i/lub zahamowanie zatokowe są najczęstszymi rytmami podczas reakcji neuro-kardiogennej typu kardiodepresyjnego. Bloki przedsionkowo-komorowe wyższych stopni są obserwowane rzadko.
Cel pracy. Porównanie danych z wywiadu oraz parametrów testu pochyleniowego u pacjentów, u których podczas reakcji neurokardiogennej wystąpił lub nie blok przedsionkowo-komorowy.
Materiał i metody. Badana grupa obejmowała 578 pacjentów z omdleniami wazowagalnymi, u których wykonano dodatni test pochyleniowy. Wśród badanych stwierdzono występowanie kardiodepresyjnego typu reakcji neuro-kardiogennej w mechanizmie bloku przedsionkowo-komorowego u 34 pacjentów, co stanowiło 5,9% wszystkich badanych. Analizie poddano dane z wywiadu od pacjentów oraz parametry testu pochyleniowego. Testy pochyle-niowe wykonywano zmodyfikowanym protokołem włoskim z prowokacją NTG w razie potrzeby.
Wyniki. Wywiad chorobowy u pacjentów z blokiem przedsionkowo-komorowym wskazywał na statystycznie istot-ną większą częstość występowania urazów związanych z omdleniami, które wymagały hospitalizacji. Wystąpienie bloku przedsionkowo-komorowego było niezależnie powiązane z wywiadem w kierunku omdleń na widok krwi i instrumentację wraz z czasem trwania odstępu PR w spoczynkowym elektrokardiogramie. Analiza krzywych ROC wykazała, że czas trwania odstępu PR ≤ 177 ms pozwalał na wyodrębnienie pacjentów z blokiem przedsionkowo- -komorowym podczas reakcji neurokardiogennej. Wykazano ponadto, że innymi czynnikami wystąpienia bloku
Adv Clin Exp Med 2011, 20, 3, 305–312 ISSN 1230-025X
ORIGINAl PAPERS
przedsionkowo-komorowego są krótszy czas trwania fazy zwalniania rytmu zatokowego oraz wystąpienie pełnego omdlenia jako wyniku testu pochyleniowego.
Wnioski. Pacjenci z blokiem przedsionkowo-komorowym podczas testu pochyleniowego różnią się od osób bez bloku. Nagły początek omdlenia, zwłaszcza u kobiet i pacjentów z omdleniami na widok krwi i instrumentację mogą wskazywać na blok przedsionkowo-komorowy podczas omdlenia wazowagalnego. Populacja pacjentów z blokiem przedsionkowo-komorowym podczas testu pochyleniowego nie jest jednorodna. Obejmuje osoby młod-sze z omdleniami na widok krwi i instrumentację oraz starmłod-sze, najprawdopodobniej z utajonym organicznym zabu-rzeniem funkcji węzła przedsionkowo-komorowego (Adv Clin Exp Med 2011, 20, 3, 305–312).
Słowa kluczowe: omdlenie wazowagalne, test pochyleniowy, blok przedsionkowo-komorowy.
Sinus bradycardia or sinus arrest are the most prevalent rhythms during a cardioinhibitory type of neurocardiogenic reaction, and atrioventricular block (AVB) occurs in 5% of tilt test-induced neu-rocardiogenic reactions [1]. Vasovagal reflexes vary from patient to patient, and may last from a few sec-onds to several minutes [2]. Progressive sinus bra-dycardia followed by AVB with a concomitant de-crease in the sinus rate is a feature of vagally induced AVB, in contrast to a sudden onset of AVB with a concomitant increase in the sinus rate, which is presumed to have an intrinsic origin [3]. The slow-ing of the heart rate durslow-ing a neurocardiogenic reac-tion is usually preceded by a decrease in blood pres-sure, but differences in the dynamics of the slowing of the heart rate may also reflect differences in the course of the neurocardiogenic reflex and lead to differences in its clinical consequences.
Prodromal signs and symptoms warn faint-ing subjects of impendfaint-ing syncope, which enables them to change their body position to prevent falls and injuries [4, 5].
Objectives
The aim of the study was to compare the medi-cal histories and tilt test (TT) findings among pa-tients with and without AVB during a positive TT, and to analyze whether patients with AVB during a neurocardiogenic reaction are a homogenous or heterogeneous population.
Material and Methods
The study group consisted of vasovagal pa-tients with positive TTs. Their medical histories were collected, focussing on the number of synco-pal episodes, traumatic injuries related to syncope, hospitalization due to such injuries, instrumenta-tion-injections-blood (IIB) phobia, autonomic fea-tures during events and jerking movements during spontaneous syncope.
The TT was performed according to the Italian protocol with a 20-minute passive phase (60
de-grees of tilt), nitroglycerine (NTG) provocation if necessary, and continuation of the test for a further 15 minutes. Throughout the entire procedure the subject’s ECG was recorded with the ECG Holter monitoring system.
The procedure was carried out on an electrical-ly controlled tilt table with a footboard for weight bearing. Blood pressure was measured automati-cally using an oscillometric method. Patients were asked to report any perception of sweating before and after TT termination. The following TT data were collected: the need for NTG provocation, the duration of the slowing of the heart rate during the neurocardiogenic reaction and the outcome of TT assessed as a total loss of consciousness (TlOC) or presyncope. The duration of TlOC was dichoto-mized and assessed as long when it lasted at least 32 seconds, or as short when it lasted no more than 31 seconds. The duration of the slowing of the heart rate was established by analyzing the heart rate trend line of the ECG recordings.
The patients were divided into four groups on the basis of their TT outcomes and the cardi-ac rhythm during the neurocardiogenic recardi-action: Group 1 had presyncope and no AVB, Group 2 had short syncope and no AVB, Group 3 had long syncope and no AVB and Group 4 had AVB dur-ing a TT-induced neurocardiogenic reaction.
Statistical Analysis
Continuous variables are presented as means ± SD, and categorical variables as percentages and counts. Continuous variables were compared using a one-way ANOVA with Tukey HSD post hoc test. Frequencies were compared with a χ2 test. A
CART is a non-parametric method of identifying predictor variables, described by Breiman et al. [6], using binary recursive partitioning: CART gener-ates a classification rule that can be visualized as a “classification tree”. A k-means cluster analysis assigned AVB patients to two subgroups of simi-lar age. The parameters studied were compared in these subgroups. All analyses were performed us-ing Statistica and MedCalc software; and p values < 0.05 were considered significant.
Results
A total of 578 patients were included in the study. There were 34 patients with AVB (Group 4), which constituted 5.9% of the total study popu-lation. The clinical characteristics of the patient population are shown in Table 1 and their TT data in Table 2.
Group 4 had a significantly higher incidence of syncope-related traumatic injuries requiring hospi-talization in their medical histories than Group 1.
Predicting AVB Using Data
From Medical Histories as
Independent Variables
The results of the univariate analysis indicat-ing predictors of AVB occurrence durindicat-ing TT are shown in Table 3.
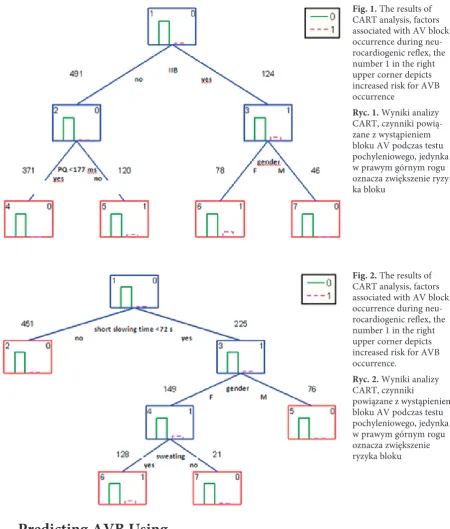
The multiple logistic regression analysis vealed that AVB occurrence was independently re-lated to a history of IIB phobia and to the duration of the PR interval on the baseline electrocardio-gram. ROC analysis revealed that patients without AVB during the neurocardiogenic reaction had PR intervals ≤ 177 ms in duration, while those with AVB had longer baseline PR intervals. CART anal-ysis revealed an increased risk of AVB occurrence among women with IIB phobia and among those without IIB phobia whose PR interval at baseline was longer than 177 ms. The sensitivity of this pa-rameter was 74% and the specificity was 70%. The results of this analysis are depicted in Fig. 1.
Table 1. Demographics, clinical and electrocardiographic data
Tabela 1. Charakterystyka demograficzna, kliniczna oraz wskaźniki elektrokardiograficzne badanych pacjentów Overall
without AVB n = 535 (Wszyscy pacjenci bez bloku)
Group 1
n = 146 Group 2n = 212 Group 3n = 177 Group 4n = 34 Control group n = 47 (Grupa kontrol-na)
Age – years ± SD
(Wiek – lata ± odchylenie standardowe) 42.3 ± 17.9 42.3 ± 22.3 37.1 ± 13.9 48.6 ± 17.4 40.7 ± 18.8 38.6 ± 13.9 Male gender – %
(Płeć męska) 36 38 34 38 24 45
Syncope number median – IQ
(liczba omdleń – mediana) 3 (1–6) 2 (0–5) 2 (1–5) 4 (2–10) 3 (1–7) 0
Traumatic injuries – % (Urazy) 30 25 26 40 32 0
Hospitalization due to trauma
(Hospitalizacja z powodu urazów) 6 3 7 8 12 0
IIB phobia – %
(Omdlewanie na widok krwi i instrumentację)
20 14 22 23 44 0
Jerks – % (Ruchy drgawkopodobne) 5 4 4 7 15 0
Sweating – % (Pocenie się) 29 27 33 27 24 0
PR interval at baseline – ms
(Odstęp PR w spoczynku) 159 ± 28 157 ± 29 155 ± 27 167 ± 29 179 ± 38 151 ± 25 RR interval at baseline – ms
(Odstęp RR w spoczynku) 952 ± 160 942 ± 154 934 ± 134 980 ± 158 922 ± 149 944 ± 153 # – p < 0.01 vs. control group.
Table 2. Tilt testing data Tabela 2. Test pochyleniowy
Overall without AVB n = 535
Group 1
n = 146 Group 2n = 212 Group 3n = 177 Group 4n = 34 Control group n = 47
NTG use – % (Prowokacja NTG) 77 66 80 82 88 100
Syncope – % (Omdlenie) 72 0 100 100 94 0
Sweating before TT termination (Pocenie się przed zakończeniem testu pochyleniowego)
18 26 18 11 3 0
Sweating after TT termination (Pocenie się po zakończeniu testu pochyleniowego)
23 13 21 33 32 0
Duration of heart rate slowing – s (Czas trwania spadku częstotliwości rytmu serca)
104 ± 60 128 ± 63 96 ± 54 81 ± 56 70 ± 34 100 ± 43
Table 3. Predictors of AVB occurrence during TT in univariate analysis
Tabela 3. Czynniki predykcyjne wystąpienia bloku AV podczas testu pochyleniowego w analizie jednoczynnikowej
Odds ratio
(Iloraz szans) 95% confidence interval(95% przedział ufności) P-value(Istotność staty-styczna) Age – years
(Wiek – lata) 0.69 0.17–2.79 ns.
Male gender (Płeć męska) 0.54 0.24–1.22 ns.
Syncope number (liczba omdleń) 0.11 0.00004–318 ns. Trauma related to syncope
(Uraz związany z omdleniem) 0.11 0.53–2.34 ns. Hospitalisation due to trauma
(Hospitalizacja z powodu urazów) 1.96 0.65–5.91 ns. IIB phobia (Omdlewanie na widok krwi
i instrumentację) 3.12 1.53–6.35 < 0.002
PR interval at baseline – ms
(Odstęp PR w spoczynku) 48.3 6.0–389 < 0.001
NTG use (Prowokacja NTG) 2.29 0.79–6.63 ns.
Jerks (Ruchy drgawkopodobne) 3.12 1.12–8.70 < 0.05 Syncope at TT (Omdlenie podczas testu
pochyleniowego) 6.18 1.46–26.18 < 0.02
Sweating before TT termination (Pocenie się przed zakończeniem testu pochyleniowego)
0.14 0.02–1.04 ns.
Sweating after TT termination (Pocenie się po zakończeniu testu pochyleniowego)
1.62 0.77–3.42 ns.
Duration of heart rate slowing – s
(Czas trwania spadku częstotliwości rytmu serca)
0.003 0.0001–0.11 < 0.002
Heart rate slowing less than 72 s
Predicting AVB Using
TT Data as Independent
Variables
The multiple logistic regression analysis revealed that a shorter duration of the slowing of the heart rate and syncope as a TT outcome are factors independently related to AVB occur-rence. ROC analysis revealed that in patients with AVB during the neurocardiogenic reaction the slowing of the heart rate lasted under 72 seconds, which distinguished them from those without AVB. CART analysis revealed that AVB in female subjects with a short duration of the slowing of the heart rate was related to a lack
of sweating before TT termination. The sensitiv-ity of this parameter was 50% and the specificsensitiv-ity was 94%. The results of this analysis are depicted in Fig. 2.
Patients with AVB
during TT
The k-means clustering analysis revealed that the subjects with AVB constituted a heterogene-ous population. Two clusters can be distinguished: The first cluster consisted of 20 subjects aged 27.4 ± 7.9 years and the second one consisted of 14 sub-jects aged 59.6 ± 12.0 years. A comparison of these groups is shown in Table 4.
Fig. 1. The results of CART analysis, factors associated with AV block occurrence during neu-rocardiogenic reflex, the number 1 in the right upper corner depicts increased risk for AVB occurrence
Ryc. 1. Wyniki analizy CART, czynniki powią-zane z wystąpieniem bloku AV podczas testu pochyleniowego, jedynka w prawym górnym rogu oznacza zwiększenie ryzy-ka bloku
Fig. 2. The results of CART analysis, factors associated with AV block occurrence during neu-rocardiogenic reflex, the number 1 in the right upper corner depicts increased risk for AVB occurrence.
Ryc. 2. Wyniki analizy CART, czynniki
Discussion
The main finding of our study is the fact that the clinical predictors for AVB during tilt test-in-duced neurocardiogenic reaction are IIB phobia in the medical history, a longer baseline PR duration and a shorter duration of the slowing of the heart rate. These predictors have a high sensitivity but a low specificity.
The shorter duration of the slowing of the heart rate during neurocardiogenic reaction in the AVB group, as in the group with a long syncope, may be associated with a significant decrease in the duration of prodromal symptoms, in comparison with the groups with presyncope and a short syn-cope. Assuming that this pattern during neurocar-diogenic reaction persists in spontaneous events, the clinical consequences of the shorter prodromal
phase could include an association between AVB occurrences during TT-induced neurocardiogenic reactions and a history of severe traumatic injuries during spontaneous syncopal spells. A longer pro-dromal phase allows the subject to find a safe place to lie down and facilitates the prevention of severe traumatic injuries.
Our study confirmed a disparityamong neu-rocardiogenic reactions in terms of the slowing of the heart rate and the correlation with the clinical courses of vasovagal reflexes assessed as presyncope, short syncope and long syncope. The frequency of sweating (an autonomic feature) also varied: sweating was more frequent among patients whose TT was terminated during pre-syncope. This finding indicates the importance of sympathetic activation in the initiation of the Table 4. Comparison of AVB patients subgroups
Tabela 4. Porównanie podgrup pacjentów z blokiem AV
Group 4 a Group 4 b P-value (Istotność statystyczna) Age – years ± SD
(Wiek – lata ± odchylenie standardowe) 27.4 ± 7.9 59.6 ± 12.0 < 0.001 Male sex – %
(Płeć męska) 10 43 < 0.001
Hypertension – % (Nadciśnienie) 0 57 < 0.001 Syncope number – median – IQ
(liczba omdleń – mediana) 5 (2–12) 2 (1–6) ns.
Traumatic injuries – % (Urazy) 25 42 ns.
Hospitalization due to trauma
(Hospitalizacja z powodu urazów) 5 21 ns.
IIB phobia – % (Omdlewanie na widok krwi
i instrumentację) 65 14 < 0.005
Jerking movements – % (Ruchy drgawkopodobne) 20 7 ns.
Sweating – % (Pocenie się) 20 29 ns.
PR interval at baseline ms (Odstęp PR w spoczynku) 164 ± 24 200 ± 45 < 0.01 RR interval at baseline ms (Odstęp RR w spoczynku) 897 ± 147 957 ± 149 ns. NTG provocation – % (Prowokacja NTG) 80 100 ns.
Syncope – % (Omdlenie) 100 86 ns.
Sweating before TT termination
(Pocenie się przed zakończeniem testu pochylenio-wego)
5 0 ns.
Sweating after TT termination (Pocenie się po zakończeniu testu pochyleniowego)
25 43 ns.
Duration of heart rate slowing – s
neurocardiogenic reaction as well as in the pro-longation of the slowing of the heart rate. The pathophysiological meaning of abrupt slowing of the heart rate is not fully understood, but its fundamental purpose in patients with IIB pho-bia can be speculated upon: Human beings have a natural fear of blood and injury. In the normal population exposure to blood or injury often re-sults in disgust, discomfort, light-headedness or even syncope. This kind of “emotional fainting” is a reflex which is thought to be an evolution-ary safety feature. According to Bracha et al., “the primary function of fear-induced faint ing may have been to non-verbally communicate to equally preverbal adversaries that one was not an immediate threat and could be safely ignored” [7]. According to that hypothesis, syncope relat-ed to IIB phobia should occur rapidly as a way to prevent injury.
The longer duration of the PR interval on the baseline electrocardiogram is related to AVB dur-ing the neurocardiogenic reaction. That observa-tion suggests that the vagal innervaobserva-tions of a cardiac conduction system may be enhanced in vasovagal patients with AVB during TT-induced syncope, or that there is a subclinical intrinsic abnormality of an atrioventricular node in these patients.
The significance of the type of neurocardio-genic reaction occurring during TT is usually overlooked because it is presumed to have low re-producibility during spontaneous syncope [8, 9]. However, neurocardiogenic reactions are deemed to have a stable electrocardiographic pattern dur-ing spontaneous syncope. It is puzzldur-ing that neu-rocardiogenic reactions of a given subject are simi-lar except when induced by TT. The reason may be a tendency to terminate TT at an earlier point than the subject breaks the reflex in environmental cir-cumstances by finding a suitable place to lie down.
In a previously published paper the authors of the current study reported that the cardiode-pressive type of neurocardiogenic reaction has the highest reproducibility [8, 9].This type of neuro-cardiogenic reaction is very common during ca-rotid sinus massage, and it has been reported that those patients had a similar type of the neurocar-diogenic reaction during spontaneous syncopal spells [10].
If the termination of TT occurs too early, the vasodepressive type of neurocardiogenic reaction predominates, similarly as in daily life circum-stances an immediate assumption of a supine po-sition, during the initial phase of vasovagal reflex can terminate the reaction. This can lead to pre-syncope with tachycardia and without the heart rate slowing and syncope [11, 12].
The differences observed between clinical and electrocardiographic parameters within the groups of patients presenting with and without AVB in-dicate the non-random nature of the groups’ dif-ferentiation. The presence of AVB during tilt test-induced neurocardiogenic reaction should alert the physician performing the test to the possibil-ity that the patient could experience such sudden reflex reactions in everyday life due to emotional factors.
The k-means cluster analysis that was per-formed to assess the homogeneity of the group of patients with AVB showed two populations of dif-ferent ages. In the younger subgroup there were more women, IIB phobia reactions were more fre-quent and the mean PR interval was much shorter. The duration of the slowing of the heart rate did not differ between the two subgroups.
CART analysis permits the identification of previously unrecognized patient subgroups and is a useful method for dissecting complex clinical situations and identifying heterogeneous patient populations.
In the current study, the CART analysis ba-sically separated the vasovagal patients into those who experienced neurocardiogenic reaction in re-sponse to the sight of blood, instrumentation or injection, and in those who did not do so. This finding is in line with the theory that AVB during neurocardiogenic reaction could be a mechanism for enabling a fast and total loss of consciousness. The presence of neurocardiogenic reactions in re-sponse to IIB in daily life circumstances predicts the increased probability of AVB occurrence dur-ing TT-induced vasovagal syncope. In the group with IIB phobia, female gender is the second fac-tor related to the AVB occurrence: women are more prone than men to have syncope in response to IIB [7]. In the group without IIB phobia, the branching of the CART analysis is caused by the duration of the PR interval, the duration of the slowing of the heart rate during the neurocardio-genic reaction and by gender.
References
[1] Kim PH, Ahn SJ, Kim JS: Frequency of arrhythmic events during head-up tilt testing in patients with suspected neurocardiogenic syncope or presyncope. Am J Cardiol 2004, 94, 1491–1495.
[2] Brignole M, Sutton R, Wieling W, Lu SN, Erickson MK, Markowitz T, Grovale N, Ammirati F, Benditt DG:
Analysis of rhythm variation during spontaneous cardioinhibitory neurally-mediated syncope. Implications for RDR pacing optimization: an ISSUE 2 substudy. Europace 2007, 9, 305–311.
[3] Moya A, Sutton R, Ammirati F, Blanc JJ, Brignole M, Dahm JB, Deharo JC, Gajek J, Gjesdal K, Krahn A, Massin M, Pepi M, Pezawas T, Granell RR, Sarasin F, Ungar A, van Dijk JG, Walma EP, Wieling W: Guidelines for the diagnosis and management of syncope (v. 2009): the Task Force for the Diagnosis and Management of Syncope of the European Society of Cardiology (ESC). Eur Heart J 2009, 30, 2631–2671.
[4] Guida P, Iacoviello M, Forleo C, Ferrara A, Sorrentino S, Balducci C, Sarlo M, Favale S: Prevalence, timing, and haemodynamic correlates of prodromes in patients with vasovagal syncope induced by head-up tilt test. Europace 2009, 11, 1221–1226.
[5] Linzer M, Yang EH, Estes NA 3rd, Wang P, Vorperian VR, Kapoor WN: Diagnosing syncope. Part 1: Value of history, physical examination, and electrocardiography. Clinical Efficacy Assessment Project of the American College of Physicians. Ann Intern Med 1997 126, 989–996.
[6] Breiman L, Friedman JH, Olshen A, Stone CJ: Classification and Regression Trees. Belmont, CA: Wadsworth; 1984.
[7] Bracha HS, Bracha AS, Williams AE, Ralston TC, Matsukawa JM: The human fear-circuitry and fear-induced fainting in healthy individuals – the paleolithic-threat hypothesis. Clin Auton Res 2005, 15, 238–241.
[8] Deharo JC, Jego C, Lanteaume A, Djiane P: An implantable loop recorder study of highly symptomatic vasovagal patients: the heart rhythm observed during a spontaneous syncope is identical to the recurrent syncope but not correlated with the head-up tilt test or adenosine triphosphate test. J Am Coll Cardiol 2006, 47, 587–593.
[9] Zyśko D, Gajek J, Szufladowicz E, Wilczyński J, Negrusz-Kawecka M, Mazurek W: Powtarzalność wyników testu pochyleniowego. Folia Cardiol 2005, 12, 458–464.
[10] Maggi R, Menozzi C, Brignole M, Podoleanu C, Iori M, Sutton R, Moya A, Giada F, Orazi S, Grovale N:
Cardioinhibitory carotid sinus hypersensitivity predicts an asystolic mechanism of spontaneous neurally mediated syncope. Europace 2007, 9, 563–567.
[11] Aerts AJ, Dendale P, Block P, Dassen WR: Reproducibility of nitrate-stimulated tilt testing in patients with sus-pected vasovagal syncope and a healthy control group. Am Heart J 2005, 150, 251–256.
[12] Foglia-Manzillo G, Romanò M, Corrado G, Tagliagambe LM, Tadeo G, Spata M, Spinelli A, Grieco A, Santarone M: Reproducibility of asystole during head-up tilt testing in patients with neurally mediated syncope. Europace 2002, 4, 365–367.
Address for correspondence:
Jacek Gajek
Department of Cardiology Wroclaw Medical University Borowska 213
50-556 Wrocław Poland
Tel.: 48 605 433 321
E-mail: [email protected]
Conflict of interest: None declared