THE TRAUMA PANDEMIC
A GLOBAL LENS FOR GLOBAL ACTION
K E L LY O ’ D O N N E L L , P S Y D A N D M I C H È L E L E W I S O ’ D O N N E L L , P S Y D M E M B E R C A R E A S S O C I AT E S , I N C .
International Trauma Collaborative—6 April 2019
Power point/slide notes and available on: membercareassociates.org
Image source: Cover detail from Global Member Care: Crossing Sectors for Serving
P U R P O S E
“ Y O U C A N ’ T J U S T P O N T I U S P I L A T E 8 0 0 , 0 0 0 P E O P L E . ”
R O M E O D A L L A I R E
• Overview the global burden of trauma
and relate it to major efforts for sustainable development and mental health
• Present core resources from the humanitarian sector and comment on them via the lens of trauma
PRESENTATION OVERVIEW
Part 1:
Global Burden of Trauma
•
Overviewing Trauma (Tt)
•
UN Sustainable Development Goals (SDGs)
•
Global Mental Health (GMH)
Part 2: Humanitarian Sector and
Trauma
•
UN Agenda for Humanity (A4H)
•
UN Global Compact for Migration (GCM)
.
Part One
Global Burden of Trauma
GLOBAL BURDEN OF TRAUMA
OVERVIEW—SOME STATISTICS
“
The importance of addressing the global problem
of psychological trauma can hardly be overestimated.
Big-picture ‘guesstimates’ of the current levels of
trauma
are staggering, running into the hundreds of millions
of [people]. Trauma adversely affects human
development,
socio-economic development, and even peace.
”
Global Initiative for Stress and Trauma Treatment (GIST-T)•
Four types of violence
Image courtesy
THE FOUR VIOLENCES QUANTIFIED
1.
Direct violence:
•
1.5 billion people live in countries afflicted by political or
criminal violence and war, 300 million people live amidst
violent insecurity. One-third of all women in the world
experience sexual, physical or other abuse in their lifetime
women are more than twice as likely as men to have PTSD.
•
Women are more than twice as likely as men to have PTSD.
•
“Silent emergencies” - stress at work, bullying, divorce,
abandonment, neglect, emotional abuse, etc.
2.
Natural violence:
•
268 million people are affected annually by natural
disasters
THE FOUR VIOLENCES QUANTIFIED
3.
Structural violence:
•
1.22 billion people lived in extreme poverty in
2010 (WB)
•
< US$1.50 a day; in all, 2.4 billion lived on <
US$2 a day that year
•
Hunger and malnutrition (925 million); 218
million are child laborers
4.
Cultural violence:
•
Discrimination, oppression, apartheid,
CONFRONTING THE TRAUMA PANDEMIC
(MEMBER CARE UPDATE, MARCH 2019)
Christian worldview and Christian hope:
Trauma reminds us that something is wrong—we are meant for a better
world.
Trauma is everywhere in creation--from the micro-atomic to the
macro-cosmic.
Trauma is another way to describe the maims and moans of fallen
creation. Wherever the Fall goes, trauma follows
.
TRANSFORMING OUR WORLD:
THE 2030 AGENDA FOR SUSTAINABLE DEVELOPM
ENT
UNITED NATIONS, 25 SEPTEMBER 2015,
PARAGRAPH 50
SDG 3.4
A MAIN SDG FOR CONNECTING
AND CONTRIBUTING TO TRAUMA
•
By 2030, reduce by one third premature
mortality from non-communicable diseases
through prevention and treatment and
promote mental health and wellbeing
•
Notes about the SDGs (Transforming our
World):
o
MH used two other times, Paragraphs 7,
26
o
Violence or violent is used 11 times
NON-COMMUNICABLE DISEASES (NCDS)
WHO 4 X 4
WHO 5 X 5
ADD AIR POLLUTION(RISK FACTORS)
AND MENTAL HEALTH (DISEASES)
G
yeongju Action Plan
“Education for Global Citizenship: Achieving the SDGs Together
”
“
In addition to literacy and numeracy, education must advance
G LO B A L M E N TA L H E A LT H
W E R E L AT E I T T O :
“ M E N TA L H E A LT H A S M I S S I O N ”
GMH is an emerging domain which promotes
mental health and wellbeing for all. GMH:
•
is international, interdisciplinary, culturally-relevant, multi-sectoral
•
emphasizes the right to health and equity in health;
•
encourages healthy behaviors and lifestyles;
•
is committed to preventing and treating mental, neurological, and
substance use conditions (MNS) especially for vulnerable
populations (e.g., settings of poverty, conflict, calamity, and
trauma) and in low- and middle-income countries;
•
seeks to improve policies and programs, professional practices
and research, advocacy and awareness, and social and
environmental factors that affect health and well being.
Updated March 2019; Based on the definition from:
•
“
Mental health conditions are responsible for much of the global
burden of disease. Mental health conditions cause more years
lived with disability (32.4%) than any other health condition and
nearly as many disability-adjusted life-years (13.0%) as
cardiovascular disease (13.5%). People living with mental health
conditions are also more likely to develop physical health
problems, less likely to receive quality healthcare and less likely
to adhere to treatment, resulting in poorer physical health
outcomes— including premature mortality.
•
But this is not just a health issue. People with mental health
conditions are often excluded from development interventions,
despite
strong evidence of the close links between mental
health and virtually every key issue in international
development;
for example, research has shown a cyclical
relationship between poor mental health and inequalities in
educational attainment, income, nutrition, housing and social
support.
•
The economic cost is overwhelming. Every year more than 12
billion working days are lost due to mental health conditions.
Between 2011-2030, this will cost the global economy $16 USD
trillion in lost economic output— more than cancer, diabetes, and
respiratory diseases combined.
”
Source:
MENTAL HEALTH ACTION PLAN 2013-20
20
WORLD HEALTH ORGANIZATION (2013)
Vision:
MH-AP 2013-2020/2030
The four major objectives of the action plan are to:
•
Strengthen effective leadership and governance for mental
health.
•
Provide comprehensive, integrated and responsive mental
health and social care services in community-based settings.
•
Implement strategies for promotion and prevention in
mental health.
•
Strengthen information systems, evidence and research for
mental health.
Note:
“Trauma”-related words used 7 times, 5 in context of
Overview: Mental Health Action Plan 2013-2020
Vision
A world in which mental health is valued, promoted, and protected, mental disorders are prevented and persons affected by these disorders are able to exercise the full range of human rights and to access high-quality, culturally appropriate health and social care in a timely way to promote recovery, all in order to attain the highest possible level of health and participate fully in
society and at work free from stigmatization and discrimination.
Cross-cutting Principles
Universal health coverage
Regardless of age, sex, socioeconomic status, race, ethnicity or sexual orientation,
and following the principle of equity, persons with mental
disorders should be able to access, without the risk of impoverishing themselves, essential health and social services that enable them to
achieve recovery and the highest attainable standard of
health.
Human rights
Mental health strategies, actions and interventions for treatment, prevention
and promotion must be compliant with the
Convention on the Rights of Persons with Disabilities and
other international and regional human
rights instruments.
Evidence-based practice
Mental health strategies and interventions for treatment, prevention and promotion need to
be based on scientific evidence and/or best practice, taking cultural
considerations into account.
Life course approach
Policies, plans, and services for mental health need to take account of health and social needs at all stages of the life course, including infancy, childhood,
adolescence, adulthood and older
age.
Multisectoral approach
A comprehensive and coordinated response for
mental health requires partnership with multiple
public sectors such as health, education, employment, judicial, housing, social and other relevant sectors as well as
the private sector, as appropriate to the country
situation. Empowerment of persons with mental disorders and psychosocial disabilities
Persons with mental disorders and psychosocial disabilities
should be empowered and involved in mental health advocacy, policy, planning, legislation, service provision,
monitoring, research and evaluation.
Goal
To promote mental well-being, prevent mental disorders, provide care, enhance recovery, promote human rights and reduce the mortality, morbidity and disability for persons with mental disorders
Objectives and Targets
1. To strengthen effective leadership and governance for mental health
Global target 1.1: 80% of countries will have developed or updated their policy/plan for mental health in line with international and regional human rights instruments (by the year 2020).
Global target 1.2: 50% of countries will have developed or updated their law for mental health in line with international and regional human rights instruments (by the year 2020).
2. To provide comprehensive, integrated and responsive mental health and social care services in community-based settings
Global target 2: Service coverage for severe mental disorders will have
increased by 20% (by the year 2020).
3. To implement strategies for promotion and prevention in mental health
Global target 3.1: 80% of countries will have at least two functioning national, multisectoral mental health promotion and prevention
programmes (by the year 2020).
Global target 3.2: The rate of suicide in countries will be reduced by 10% (by the year 2020).
4. To strengthen information systems, evidence and research for mental health
TRAUMA:
P R E V E N T I O N A N D T R E AT M E N T C AU S E S A N D C O N S E Q U E N C E S
<
CONFERENCES
TRAINING >
VIDEOS
V
Video:
Living Peace: The Story of Abby and Kyalu
FRAMEWORK FOUR
GLOBA L C OMPAC T FOR A S AFE, ORDERLY, AND REGU L AR MIGRATI ON
( G C M , 2 0 1 8 )
“The global compact comprises 23 objectives for better managing migration at local, national, regional and global levels. The compact:
• aims to mitigate the adverse drivers and structural factors that hinder people from building and maintaining sustainable livelihoods in their countries of origin;
• intends to reduce the risks and vulnerabilities migrants face at different stages of
migration by respecting, protecting and fulfilling their human rights and providing them with care and assistance;
• seeks to address the legitimate concerns of states and communities, while recognizing that societies are undergoing demographic, economic, social and environmental
changes at different scales that may have implications for and result from migration; • strives to create conducive conditions that enable all migrants to enrich our societies
through their human, economic and social capacities, and thus facilitate their
contributions to sustainable development at the local, national, regional and global levels.
• The list of the 23 objectives can be found in
paragraph 16 of the Global Compact for Migration.”
HUMANITARIAN INTERVENTION GUIDE
THE FRIENDSHIP BENCH
• “The Friendship Bench project is an evidence-based intervention
developed in Zimbabwe to bridge the mental health treatment gap. Their mission is to enhance mental
well-being and improve quality of life through the use of problem solving therapy delivered by trained lay health workers. The
Friendship Bench focuses on people who are
suffering from common mental disorders, such as anxiety and depression. Produced by: Nicky
Wimble, United For Global Mental Health”
• Video:
L ANCET COMMISSION ON GMH
A ND SUSTAINA BLE DEV ELOPME NT
( O CT O B E R 2 0 18 )
Summary of Key Recommendations
1.
Address mental health across all the Sustainable
Development Goals
2.
Include mental health in the essential package of services
for Universal Health Coverage
3.
Take a public health approach to prevention and
promotion
4.
Ensure inclusion of people with mental health conditions
5.
Increase investment in mental health
6.
Harness learning from research to help drive change
.
Part Two
Humanitarian Sector and Trauma
A4H, GCM, Examples
A G E N D A F O R H U M A N I T Y5 C O R E R E S P O N S I B I L I T I E S
1. Political leadership to prevent and end conflict. “Preventing conflicts and finding political solutions to resolve them is our first and foremost responsibility to humanity.”
2. Uphold the norms that safeguard humanity 3. Leave no one behind
4. Change people’s lives—from delivering aid to ending need 5. Invest in humanity
Notes:
• Trauma appears once and violence-related words 6 times (4 related to S/GBV), mental 0 times and psychosocial one in relation to S/GBV.
GLOBAL COMPACT FOR A SAFE, ORDERLY, AND REGULA
R MIGRATION
(GCM, 2018)
“The global compact comprises 23 objectives for better managing migration at local, national, regional and global levels. The compact:
• aims to mitigate the adverse drivers and structural factors that hinder people from building and maintaining sustainable livelihoods in their countries of origin;
• intends to reduce the risks and vulnerabilities migrants face at different stages of migration by respecting, protecting and fulfilling their human rights and
providing them with care and assistance;
• seeks to address the legitimate concerns of states and communities, while recognizing that societies are undergoing demographic, economic, social and environmental changes at different scales that may have implications for and result from migration;
• strives to create conducive conditions that enable all migrants to enrich our societies through their human, economic and social capacities, and thus
facilitate their contributions to sustainable development at the local, national, regional and global levels.
• The list of the 23 objectives can be found in
paragraph 16 of the Global Compact for Migration.”
TRAUMA AMONG REFUGEES
•
Rates of psychotic, mood and
substance use disorders similar to host
populations.
•
Rates of post-traumatic stress disorder
in refugees and asylum seekers are
higher.
Priebe S, Giacco D & El-Nagib R. (WHO, 2016)
Bogic M, Njoku A, Priebe S. Long-term mental health of war-refugees: a systematic literature review. BMC Int Health Hum Rights. 2015;15(1):29.
15% PTSD prevalence among
refugees
ALL REFUGEES HAVE
EXPERIENCED SOME
LEVEL OF TRAUMA:
•
Does this mean they are all
traumatized?
•
Do we pathologize their conditions
at the expense of overall mental
health & seeing strengths,
innovation, & resilience?
•
What are the risk and protective
MORE TRAUMA PERSPECTIVES
HUMANITARIAN SECTOR
• Psychological First Aid: Guide for Field Workers
(2011, WHO, War Trauma Foundation, World Vision)
• Core Humanitarian Standard on Quality and Accountability
(2014, CHS Alliance)
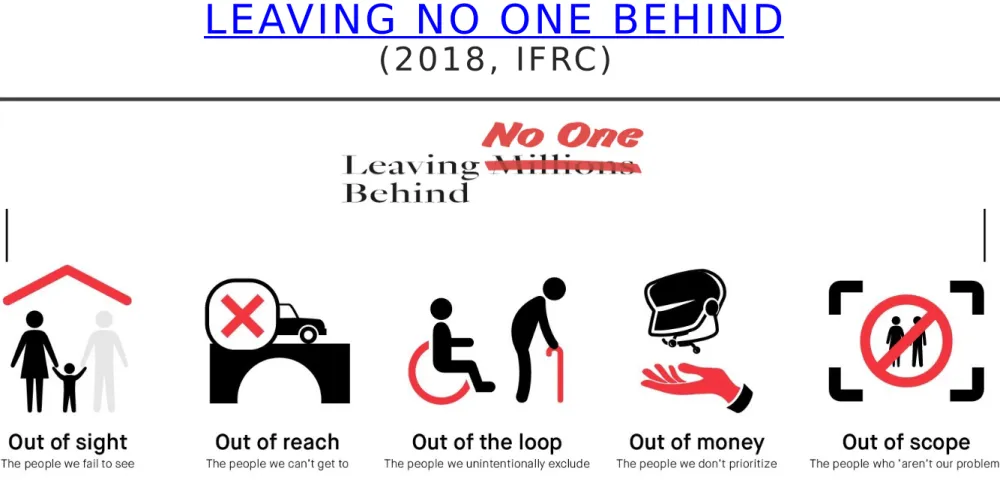
• World Disasters Report: Leaving No One Behind
(2018, IFRC)
• Guidelines on Mental Health and Psychosocial Support
“
Evidence-based psychological interventions commonly used
in high-resource settings can be effective in low-resource
contexts, including when they are delivered by trained and
supervised non-specialists. These interventions have proved
helpful in the treatment of common mental health problems,
such as depression, anxiety and traumatic and chronic stress,
as well as other difficulties, such as harmful alcohol use.
Cultural and contextual adaptations can increase the
effectiveness of psychological interventions, and make them
more accessible to people affected by crises. Treatments are
best delivered in local languages, using recognisable
terminology and case examples, and implemented in ways
that do not exacerbate stigma or exclusion. Humanitarian
settings demand psychological interventions that are as brief
and as low-cost as possible, and which optimise limited human
resources.
”
• Scalable psychological interventions for people affected by adversity, Schaefer et al (July 2018)
PSYCHOLOGICAL FIRST AID
What is it?
•
Early psychosocial support following
traumatic events/disasters
•
Brief evidence-informed intervention
•
Serves individuals, families & local
communities
Primary aim of PFA:
•
Reduce distress & promote basic needs
•
Deliver important information
•
Connect people with available support
networks
PSYCHOLOGICAL FIRST AID:
GUIDE FOR FIELD WORKERS
PFA RESEARCH
How has the WHO PFA 2011Guide been perceived
and used?
“
In conclusion, the PFA retrospective study allowed us
the chance to
Look
at the progression of the WHO PFA
guidance
, Listen
carefully to people’s experiences and
perceptions and hopefully now
Link
PFA within holistic,
comprehensive MHPSS responses in emergencies. Just as
medical first aid does not constitute a comprehensive
health response, so PFA is not a panacea for all the
mental health needs of people affected by crisis events –
it must be integrated as a component of wider MHPSS
frameworks and services to most effectively ‘reach out a
helping hand’.
”
[bold added for emphasis]
Psychological First Aid Around the World: Summary of a Five year Retrosp
ective
,
Snider, Schaefer, Winberg (July 2018).
CORE HUMANITARIAN STANDARD
ON QUALITY AND ACCOUNTABILITY
(2014, CHS ALLIANCE)
WORLD DISASTERS REPORT:
LEAVING NO ONE BEHIND
(2018, IFRC)
The report identifies five fatal flaws that are allowing so many people to fall through the cracks: too many affected people are 1) out of sight, 2) out of reach, 3) left out of the loop, or find themselves in crises that are 4) out of money, or deemed to be 5) out of scope because they are suffering in ways that are not seen as the responsibility of the humanitarian sector.
GUIDELINES ON MENTAL HEALTH
AND PSYCHOSOCIAL SUPPORT
(2017, ICRC)
SEE ALSO:
IASC MHPSS IN EMERGENCY SETTINGS
Example of one of the many approaches for MHPSS
group session for families of missing persons
,
CORE READINGS
•Transforming Our World: The 2030 Agenda for Sustainable Development)
United Nations (2015) UN Sustainable Development Knowledge Platform See:
Frequently Asked Questions
•One Humanity: Shared Responsibility. Report of the Secretary-General for the
World Humanitarian Summit. UN General Assembly, 70th Session. (2016).
•Mental Health Action Plan 2013-2020. World Health Organization. (2013).
•Global Compact for a Safe, Orderly, and Regular Migration , United Nations
(2018)
•World Disasters Report 2018: Leaving No One Behind International Federation
of the Red Cross and Red Crescent Societies (2018)
•Lancet Commission on Global Mental Health and the Sustainable Development
. (October 9, 2018). The Lancet, 392, 1553–1598.
•O’Donnell, K. & Eaton, J. (June 2017).
Global Mental Health: Collaborating Across Sectors for Sustainable Developme nt and Wellbeing
. Bulletin, Medicus Mundi Switzerland
•O’Donnell, K. & Lewis O’Donnell, M. (2016).
Multi-Sectoral Member Care: Engaging Our World as Global Integrators . Journal of Psychology and Theology, 44(4), 303-314
• O’Donnell, K. & Lewis O’Donnell, M. (2017).
Well-Being for All: Mental Health Professionals and the Sustainable Developme nt Goals
THE TRAUMA PANDEMIC
A GLOBAL LENS FOR GLOBAL
ACTION
“We can’t just Pontius Pilate 7.7 billion people!”
Thank you!
Michèle and Kelly O’Donnell
Member Care Associates, Inc.
A framework for actively and responsibly engaging in
our world—locally through globally—for God’s glory:
•
By connecting relationally and contributing relevantly
on behalf of human wellbeing and the issues facing humanity
•
In light of our integrity, commitments, and core values
(e.g., ethical, humanitarian, human rights, faith-based).
See Global Integration: Staying Current and Relevant (March 2019 update)
PA RT N E R I N G - - FA I T H - B A S E D I N I T I AT I V E S
M AT E R I A L S - M I L E S T O N E S
• Building from Common Foundations:The
World Health Organization and Faith-Based Organizations in Primary Care
(2008), Geneva Global, World Health Organization (overview and guidelines)
• Ending Extreme Poverty: A Moral and Religious Imperative (2015), World Bank
(joint inter-religious statement)
• Laudato Si: Caring for Our Common Home (2015), Pope Francis (encyclical on creation care)
• Faith-Based Health Care (7 July 2015), The Lancet (special issue) • International Partnership on Religion and Sustainable Development
(organization/website)
• A Faith-Sensitive Approach to Humanitarian Response: Guidance on Ment al Health and Psychosocial Programming
(2018) The Lutheran World Federation and Islamic Relief Worldwide
• Source for the first five items:
Multi-Sectoral Member Care: Engaging Our World as Global Integrators
S E V E N D I R E C T I O N A L C O M M I T M E N T S E N G A G I N G O U R W O R L D A S G LO B A L I N T E G R AT O R S
W E L L - B E I N G F O R A L L : M H P S A N D T H E S D G S
(J O U R N A L O F P S Y C H O L O G Y A N D C H R I S T I A N I T Y, S P R I N G 2 0 1 7 )
Commitment 1. We commit to diligently pursue our own journeys of personal
and professional growth—to grow deeply as we go broadly.
Commitment 2. We commit to integrate the inseparable areas of our
character (resilient virtue) and competency (relevant skills) with compassion (resonant love).
Commitment 3. We commit to go into new areas of learning and work:
crossing sectors, cultures, disciplines, and comfort zones.
Commitment 4. We commit to embrace our duty to work in difficult settings,
including those permeated by conflict, calamity, corruption, and poverty as those in great need are often in places of great risk.
Commitment 5. We commit to have clear ethical commitments and
standards that guide our work, respecting the dignity and worth of all people.
Commitment 6. We commit to working with others to promote wellbeing and
sustainable development, building the future we want--being the people we need.
Commitment 7. We commit to base our work on the practice of fervently