A Randomized, Controlled Trial of Prophylactic Granulocyte-Macrophage
Colony-Stimulating Factor in Human Newborns Less Than
32 Weeks Gestation
Robert Carr, MBChB*; Neena Modi, MBChB§; Caroline J. Dore´, BSc\; Rim El-Rifai, MBBS‡; and Dwight Lindo, MBBS§
ABSTRACT. Objective. Preterm neonates undergoing intensive care have high morbidity from sepsis. These infants also frequently develop neutropenia, and when this is associated with sepsis, mortality is high. This study investigates the potential for granulocyte-macro-phage colony-stimulating factor (GM-CSF) to effect a clinically relevant increase in neutrophil number when used prophylactically in high-risk preterm neonates, and assesses its safety in this population.
Design. In an open, randomized, controlled study, 75 neonates (25 small for gestational age)<32 weeks gesta-tion were randomized to receive GM-CSF (10mg/kg/d) by subcutaneous injection for 5 days from<72 hours after birth, or to a control group. The primary outcome mea-sure was the neutrophil count during 14 days from study entry. The infants were monitored for potential toxicity. Clinical outcomes, sepsis, and mortality, were recorded, but this initial study was not designed to address clinical benefit.
Results. Prophylactic GM-CSF therapy completely abolished neutropenia in treated infants, when both well and septic, throughout the period of study. Neutropenia (<1.73109/L) developed in 16 of 39 control infants. Five
control infants experienced an acute decrease in neutro-phil count coincident with the onset of sepsis. There was no evidence of hematologic, respiratory, or gastrointesti-nal toxicity in treated infants. Treated infants had a trend to fewer symptomatic, blood culture positive septic epi-sodes than controls during 2 weeks from study entry (11/36 vs 18/39).
Conclusion. Five-day prophylactic GM-CSF com-pletely abolishes postnatal neutropenia and sepsis-in-duced neutropenia in preterm neonates at high risk of sepsis, and so removes an important risk factor for sepsis and sepsis-related mortality.Pediatrics1999;103:796 – 802; GM-CSF, preterm neonates, neutropenia, sepsis.
ABBREVIATIONS. G-CSF, granulocyte colony-stimulating factor; GM-CSF, granulocyte-macrophage colony-stimulating factor; CSF, colony-stimulating factor; AGA, appropriately grown for gestational age; SGA, small for gestational age; FG, French gauge; REML, restricted maximum likelihood; CI, confidence interval.
B
acterial sepsis is an important cause of morbid-ity and mortalmorbid-ity in preterm neonates, partic-ularly in those of very low birth weight.1 At-tempts to prevent sepsis or reduce sepsis-related mortality using intravenous immunoglobulin have failed to make a major impact2 and attention has recently turned to the potential enhancement of phagocyte immunity using the hemopoietic colony-stimulating factors.3Neutrophil leukocytes are central to the defenses against bacterial infection and in neonates both neu-trophil production4 and function5– 8 are immature. Bactericidal activity of circulating, morphologically mature neutrophils is impaired at birth. Reduced numbers of neutrophil precursors are exacerbated by a reduced capacity to increase neutrophil production rapidly in response to sepsis.9 As a consequence, neutropenia occurs commonly in preterm neo-nates10,11 and when sepsis is associated with severe neutropenia and marrow neutrophil storage pool de-pletion mortality exceeds 50%.11–13
The hemopoietic colony-stimulating factors, gran-ulocyte colony stimulating factor (G-CSF) and granulocyte-macrophage colony stimulating factor (GM-CSF), have become standard treatment for pre-venting chemotherapy-induced neutropenia and ac-celerating neutrophil recovery after marrow trans-plantation. However, because of anxiety about potential acute and long-term toxicity of hemopoietic colony-stimulating factor (CSF) therapy in the new-born period,3 clinical trials in neonates have been preceded by extensive in vitro and animal studies. These trials have demonstrated that cord blood mononuclear cells produce less G-CSF and GM-CSF than adults14,15 but that neonate granulocyte-mac-rophage committed progenitors respond well to the proliferative stimulus of both cytokines16,17; cord blood neutrophils have normally functioning G-CSF and GM-CSF receptors15,18and, in vitro, GM-CSF can prime term and preterm neutrophils for enhanced chemotaxis and respiratory burst responses.19 –21 In addition, studies in newborn rats have demonstrated that both G-CSF22 and GM-CSF23 can increase sur-vival after experimental sepsis, provided they are given before bacterial inoculation.24These preclinical studies were followed by two phase I/II studies of CSF treatment in a small number of newborn infants with suspected sepsis,25,26which showed that short-term treatment with either G-CSF or GM-CSF in
From the *Departments of Haematology and ‡Paediatrics, King’s College, St Thomas’ Hospital; the §Department of Paediatrics and Neonatal Medicine; and the\Department of Medical Statistics and Evaluation, Imperial College School of Medicine, Hammersmith Hospital, London, United Kingdom. Received for publication Sep 14, 1998; accepted Jan 4, 1999.
Reprint requests to (R.C.) Department of Haematology, St Thomas’ Hospi-tal, Lambeth Palace Rd, London, SE1 7EH, United Kingdom.
varying doses by intravenous infusion could increase the neutrophil count. However, blood counts were not reported beyond the end of treatment and proven sepsis was too infrequent to draw clinical conclusions.
G-CSF has begun to enter clinical neonatal practice as salvage therapy for infants who develop neutro-penia in the presence of severe sepsis27–29or to treat persistent preeclampsia-associated neutropenia.30 –32 However, GM-CSF might be the more appropriate CSF for prospectively enhancing the immature im-mune system of preterm neonates. It has more wide ranging activities, stimulating the proliferation of both monocyte and neutrophil precursors33together with a greater effect on the bactericidal function of mature neutrophils than G-CSF,34as well as function-ally enhancing monocytes.35,36
In the randomized, controlled trial described here we studied the prophylactic role of GM-CSF in non-infected, preterm neonates at high risk of both neu-tropenia and sepsis. We report the effect of early postnatal treatment with GM-CSF on blood counts and on clinical outcome, including toxicity, in both appropriately grown for gestation (AGA) and small for gestation infants (SGA).
METHODS Study Design
The study was a randomized, controlled trial designed to test the hypothesis that the prophylactic administration of GM-CSF to extremely preterm newborns leads to a clinically relevant increase in neutrophil number. The primary outcome measure was the neutrophil count during 14 days from study entry. Secondary outcomes were: neutrophil numbers in the 3rd and 4th week from study entry, monocyte, eosinophil, and platelet numbers during the same periods, and clinical evidence of toxicity until discharge from hospital. Clinical outcomes, sepsis and mortality, were re-corded but this initial study was not designed to have sufficient power to address clinical benefit.
Study infants were recruited from the neonatal intensive care units of the Hammersmith Hospitals Trust, and Guy’s and St Thomas’ Hospital Trust, London. The study was approved by the research ethics committees of both institutions and informed writ-ten parental consent was obtained before randomization.
Infants were eligible for entry if born ,32 weeks gestation. Recruitment was within 72 hours of birth. Subjects were excluded if there was life-threatening congenital abnormality or clinical evidence of sepsis at recruitment. Infants were randomized (com-puter-generated, block randomization), stratified by growth status (AGA or SGA), either to receive GM-CSF for 5 consecutive days (study days 1–5), or to a control group. A dose of 10mg/kg/d was chosen for its proliferative effect, while remaining within accepted safety margins. SGA infants were defined as being below the 10th centile birth weight for gestational age. GM-CSF (Leucomax, No-vartis, UK) was supplied as lyophilized powder and reconstituted at a concentration of 10 mg in 0.1 mL. Administration was by subcutaneous injection into the thigh, using a 27 French gauge (FG) needle.
Data Collection Full Blood Counts
Blood counts (arterial or venous samples) were monitored daily during study days 1 to 14. During days 15 to 28 blood counts were measured only as clinically indicated. GM-CSF was discontinued before 5 days if the total white cell count exceeded 503109/L.
Individual white cell counts were derived from 100 cell manual differentials by laboratory staff blinded to treatment allocation. Neutrophil counts included bands and metamyelocytes. Neutro-penia was defined according to the reference range for healthy neonates beyond 60 hours after birth established by Manroe et al37
(lower limit of normal51.753109/L). The data are also analyzed
in relation to the revised neutrophil reference range for very low birth weight neonates (#1500 g) established by Mouzinho et al38
(lower limit of normal51.13109/L).
Toxicity
In view of concerns regarding potential toxicity, control infants did not receive placebo, as clinical staff wished to be aware of whether an infant was assigned to treatment or control group. A record was made of the following: oxygen requirements; daily weight; incidence of chronic lung disease (continuing oxygen re-quirement at 36 weeks postmenstrual age, with characteristic chest radiograph); necrotizing enterocolitis (abdominal distention, blood-stained stools, and intestinal pneumatosis); pyrexia.37.5°; and irritability, as assessed by unit nursing and medical staff.
Sepsis
Episodes of sepsis were monitored for 4 weeks from study entry. An episode of sepsis was strictly defined as a positive blood culture associated with the acute onset of at least three of the following clinical signs: 1) increase in apneic/bradycardic attacks, 2) sudden increase in the fraction of inspired oxygen requirement, 3) temperature instability, 4) lethargy, 5) capillary refill time.3 seconds/core peripheral temperature gap exceeding 2°C.
Data Analysis
White cell and platelet counts were analyzed based on sum-mary data for each individual.39For each treated subject the
pre-treatment value was represented by the day 1 count and the during treatment value as the mean of counts obtained on study days 2 to 6 (ie, the count obtained 18 –24 hours after each GM-CSF dose). A 1-week posttreatment value was represented by the mean of counts obtained on study days 11 to 14. Control infants’ blood counts were analyzed at equivalent times, similarly defining day 1 as the day of study entry. Thirteen infants (5 treated; 8 control) were commenced on dexamethasone because of their respiratory condition, between days 9 and 14. Blood counts during dexameth-asone treatment were not included in the analysis, because of its known effect of causing a neutrophil leukocytosis.
Statistical Methods
Study groups were compared using Fisher’s exact test. Periph-eral blood count data were analyzed using the restricted maxi-mum likelihood (REML) procedure in Genstat 5 (Release 3.2, second edition, Lawes Agricultural Trust, [Harpenden, United Kingdom]) to perform an unbalanced analysis of variance, after logarithmic transformation of the data to improve variance equal-ity. As the logarithm of 0 is undefined, 0.1 was added to each eosinophil or monocyte count before performing the transforma-tion. Variables were tested for the influence of treatment and time (pretreatment, during, posttreatment) taking into account the vari-ation between and within subjects, and for the influence of growth status group (SGA or AGA). Interactions between these three fixed effects were also assessed. The REML procedure was used to calculate predicted means and standard errors for each variable, on the logarithmic scale. Descriptive data were transformed back to give geometric means and 95% confidence intervals (CIs) on the original scale. Clinical outcomes (ie, toxicity, sepsis, mortality) were analyzed by logistic regression analysis in STATA (Stata Statistical Software, Release 5.0,College Station, TX, Stata Corpora-tion) for the effect of treatment and for interaction between treat-ment and growth status group. Weight changes were analyzed by 2-way analysis of variance.
RESULTS
GM-CSF was started in all treated infants within 72 hours of birth, (median day 2).
Peripheral Blood Counts
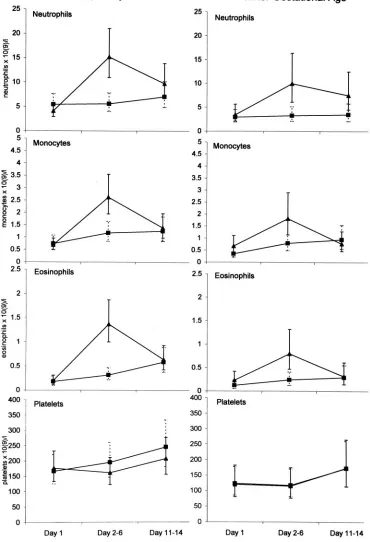
In infants receiving GM-CSF peripheral blood neu-trophils increased progressively during treatment to a geometric mean peak value in AGA infants of 22.0 3 109/L, 95% CI 17.1, 28.4; mean peak in SGA infants of 14.5 3 109/L, 95% CI 9.4, 22.6. In most infants the highest neutrophil count was recorded on the day after the final dose (median study day 6, range 4 – 8) and thereafter decreased toward pretreat-ment values. In only 1 infant, an SGA twin, was there no neutrophil increase with GM-CSF. In 5 AGA in-fants GM-CSF was discontinued after 2 to 4 doses because the total white blood cell count exceeded 503 109/L.
The monocyte count showed a similar pattern of increase in response to GM-CSF therapy to a mean peak in AGA infants of 3.83109/L, 95% CI 3.0, 4.8; mean peak in SGA infants of 2.83109/L, 95% CI 1.6, 5.0. The monocyte count returned to control levels by 1 week after GM-CSF ceased. Eosinophils also in-creased transiently to a mean peak in AGA infants of 2.5 3 109/L, 95% CI 1.9, 3.8; mean peak in SGA infants of 1.3 3109/L, 95% CI 0.8, 2.1.
Individual blood cell summary data before, dur-ing, and 1 week after treatment, and at equivalent times in controls, is shown in Fig 1. The increase in neutrophil, monocyte, and eosinophil counts during
treatment (days 2– 6) were highly significant, as dem-onstrated by an interaction between treatment and time in the REML analysis (P , .001 for all 3 cell types; Table 2). The platelet count was not signifi-cantly affected by GM-CSF treatment at any time point (P 5 .4). SGA infants had significantly lower white blood cell values than AGA infants overall
(P , .01, Fig 1, Table 2). However GM-CSF was
equally effective at increasing granulocyte and monocyte counts in SGA and AGA infants as dem-onstrated by lack of interaction between treatment and growth status, or treatment, growth status, and time (Table 2).
Blood counts between days 15 to 28 from trial entry were taken only as clinically indicated, conse-quently the majority of counts beyond day 15 were from infants who were clinically unstable or in whom sepsis was suspected. The counts were there-fore too few and not representative enough of steady state hematopoiesis for valid comparative analysis between groups.
Incidence of Neutropenia
Neutropenia was completely prevented by GM-CSF treatment in both SGA and AGA infants throughout the 2-week period of observation from study entry. In the 39 untreated control infants dur-ing the same period, a neutrophil count#1.73109/L occurred in 16 (P , .001) and #1.0 3 109/L in 7 subjects (P5.01). Of the 14 control infants who were small for gestation, 10 developed neutropenia to
#1.73109/L and 5 to#1.03109/L. There were no episodes of neutropenia identified in either control or treated infants during the 3rd or 4th week.
During the 14-day study period 5 control infants (3 SGA, 2 AGA) experienced an acute decrease in pe-ripheral blood neutrophils in response to 6 episodes of blood culture positive sepsis. Four episodes oc-curred between days 2 to 7 and two between days 8 to 14. The mean neutrophil nadir during these epi-sodes was 0.93109/L (range 0.3–1.9). No GM-CSF-treated infant experienced a decrease in neutrophils in response to sepsis at any time (P 5 .055). The lowest neutrophil count recorded during a septic episode in treated infants was 5.63 109/L.
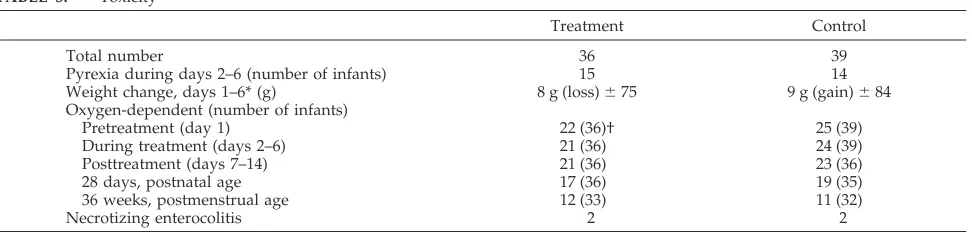
Toxicity
Infants were closely monitored for evidence of adverse effect from GM-CSF until discharge from hospital. During GM-CSF administration there was no local toxicity at injection sites, no evidence of increased irritability, which might suggest bone pain, and no difference from controls in terms of pyrexia or weight change. There was no significant differ-ence between the groups in oxygen requirement dur-ing treatment or durdur-ing the subsequent week. Simi-lar numbers of treated and control infants were oxygen-dependent at 28 days postnatal age and 36 weeks postmenstrual age. No gastrointestinal toxic-ity was observed, in particular necrotizing enteroco-litis was suspected or confirmed in 2 infants in each treatment group (Table 3). There was no evidence to suggest from the logistic regression analysis that there was an effect of treatment on any of these
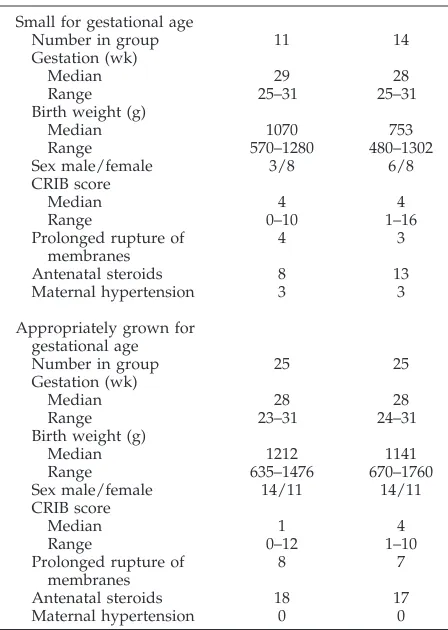
TABLE 1. Population Characteristics
Treatment Control Small for gestational age
Number in group 11 14
Gestation (wk)
Median 29 28
Range 25–31 25–31
Birth weight (g)
Median 1070 753
Range 570–1280 480–1302 Sex male/female 3/8 6/8 CRIB score
Median 4 4
Range 0–10 1–16
Prolonged rupture of membranes
4 3
Antenatal steroids 8 13 Maternal hypertension 3 3
Appropriately grown for gestational age
Number in group 25 25
Gestation (wk)
Median 28 28
Range 23–31 24–31
Birth weight (g)
Median 1212 1141
Range 635–1476 670–1760 Sex male/female 14/11 14/11 CRIB score
Median 1 4
Range 0–12 1–10
Prolonged rupture of membranes
8 7
variables, or that the effect of treatment differed be-tween AGA and SGA infants.
Sepsis and Mortality
During the period of GM-CSF treatment and the subsequent week (ie, days 2–14), 7/14 control SGA infants and 11/25 control AGA infants developed
one or more episode(s) of symptomatic, blood cul-ture-positive sepsis, whereas 2/11 treated SGA in-fants and 9/25 treated AGA inin-fants did so. The odds ratio for overall treatment effect for the combined SGA and AGA groups was 0.51, 95% CI 0.20, 1.31; ie, treated infants were about half as likely to have an episode of systemic infection as control infants,
al-Fig 1. A, Neutrophil; B, monocyte; C, eosinophil; and D, platelet count summary data, by growth status and treatment group. For each
though this did not reach significance. There was no significant effect of growth status (P 5 .68) and no
significant interaction between treatment and
growth status (P 5 .29). Most isolates were coagu-lase-negative staphylococci. Other organisms iso-lated from treated infants were enterococcus (1); and from controls: enterobacter sp (2), citrobacter (1), corynebacterium (1), Gram-negative bacillus (1). Be-tween days 15 to 28, 8 treated and 6 control infants developed sepsis.
During 4 weeks from study entry there were no deaths in the treatment group, but 5 control infants died: 3 of these deaths were sepsis-related (on days 5, 7, 28 from study entry). During subsequent fol-low-up between 1 and 6 months postnatal age there were 4 deaths in each study group.
DISCUSSION
GM-CSF administered prophylactically for 5 days, commencing within 72 hours of birth, is effective in elevating neutrophil counts in newborn infants born ,32 weeks gestation. This regimen also completely abolished the subsequent development of neutrope-nia, including sepsis-related neutropeneutrope-nia, in both ap-propriately grown as well as small for gestation in-fants. In untreated control infants, 41% (16/39) developed neutropenia with an absolute neutrophil count of #1.73 109/L, and 18% (7/39) severe neu-tropenia (#1.03 109/L).
Treated infants showed a more mature hemopoi-etic response to acute infection by mounting an ap-propriate neutrophil leukocytosis. In contrast, 29% (6/21) of episodes of sepsis that occurred during the first 14 days from study entry in control infants were accompanied by an acute decrease in neutrophil count.
The mechanism underlying postnatal neutropenia during the neonatal period appears to be a combina-tion of a reduced whole body neutrophil cell mass, together with reduced numbers of committed neu-trophil progenitors in the bone marrow at birth and
an inability to increase granulopoiesis in response to sepsis.4,9Sequential measurements of neutrophil cell mass in neonatal rats suggests that it takes 4 weeks for adult levels of neutrophil reserves to be achieved.41 In infants born to hypertensive mothers, in whom neutropenia is particularly common, there appears in addition to be a CSF inhibitor interfering with normal granulopoiesis.42 In the present study, the 3 treated SGA infants from hypertensive preg-nancies had a neutrophil response to GM-CSF simi-lar to other treated SGA infants, suggesting that any inhibitor can be overcome by pharmacological CSF doses. The observation that just 5 days prophylactic GM-CSF prevented the occurrence of neutropenia not only during treatment, but also during the sub-sequent 3 weeks of observation, tempts speculation that early stimulation by GM-CSF accelerates matu-ration of neonatal granulopoiesis by early expansion of the progenitor and neutrophil storage pool.
A major concern over the use of the CSFs in the newborn has justifiably been that of toxicity. In adults and children the most common side effects are bone pain and low-grade fever during administra-tion, and at high doses a capillary leak syndrome with fluid retention has been observed. None of these effects were identified in treated infants. With rapid intravenous infusion a first dose effect of pul-monary leukocyte sequestration and hypoxia may occur.43An additional concern in this population was that inappropriate activation of monocytes and neu-trophils in the pulmonary and mesenteric circulation might lead to an increased incidence of chronic lung disease or necrotizing enterocolitis. The majority of very immature infants already have respiratory problems and it was reassuring to find no difference in oxygen requirements between treatment and con-trol group subjects either during GM-CSF treatment or during follow-up. Neither was there increased evidence of necrotizing enterocolitis in treated in-fants. An important additional point is that subcuta-neous administration proved possible in all infants,
TABLE 2. PValues From the Analysis of Peripheral Blood Count Data
Effect or Interaction Neutrophils Monocytes Eosinophils Platelets
Treatment1time ,.001 ,.001 ,.001 .4
Growth .004 .002 .003 .02
Treatment1growth .4 .7 1.0 .8
Treatment1growth1time .7 .2 .4 .5
Treatment: GM-CSF treatment versus control group; time: pretreatment versus posttreatment; growth: SGA versus AGA infants.
TABLE 3. Toxicity
Treatment Control
Total number 36 39
Pyrexia during days 2–6 (number of infants) 15 14 Weight change, days 1–6* (g) 8 g (loss)675 9 g (gain)684 Oxygen-dependent (number of infants)
Pretreatment (day 1) 22 (36)† 25 (39)
During treatment (days 2–6) 21 (36) 24 (39)
Posttreatment (days 7–14) 21 (36) 23 (36)
28 days, postnatal age 17 (36) 19 (35)
36 weeks, postmenstrual age 12 (33) 11 (32)
Necrotizing enterocolitis 2 2
despite the extremely low birth weight of many of them. Other groups have appeared reluctant to use the subcutaneous route in neonates, although this route has advantages over intravenous administra-tion in terms of both increased therapeutic efficacy as well as safety, by avoiding the high peak blood levels that are associated with greater toxicity.44
There are anxieties about the long-term conse-quences of exposing the immature immune system to pharmacological doses of CSFs. Long-term G-CSF therapy of Kostmann’s syndrome (congenital neutro-penia) has been associated with an increased inci-dence of leukemia, although this is most likely a consequence of longer survival in a premalignant condition.45,46It has also been suggested that stimu-lation of granulopoiesis could result in a lineage steal effect with a reduction in erythropoiesis and throm-bopoiesis. Recent data from cell line and animal studies that growth factors play a permissive rather than instructive role in hematopoiesis suggest that neonatal exposure to CSFs is unlikely to fundamen-tally change the future balance of blood cell produc-tion.47,48 In the present study the platelet count ap-peared to be unaffected by GM-CSF either during treatment or subsequently. This contrasts with other reports that have suggested that GM-CSF might in-crease platelet numbers26 and G-CSF might exacer-bate thrombocytopenia,27 but in each report only small numbers of infants were studied. Any effect on erythropoiesis could not be assessed in the short-term because of variable iatrogenic blood loss. Two-year follow-up of infants in an early phase I/II study of G-CSF49 found no evidence of long-term alter-ations in hematopoiesis. However, it is clearly im-portant that all CSF-treated infants are monitored during their future development.
There is a relationship between a low neutrophil count and the risk of subsequent sepsis in preterm neonates. It has been reported that neutropenia at 12 hours after birth in infants born to mothers with pregnancy-induced hypertension was associated with increased risk of nosocomial infection in the first 18 days of postnatal life.50Further evidence sug-gests that persistence of neutropenia beyond 60 hours of age is a more important predisposing fac-tor.50,51 It is beyond dispute that when sepsis and neutropenia occur together, mortality is high.11Thus, prevention of sepsis-induced neutropenia is likely to reduce mortality and the prevention of neutropenia, however defined,37,38 during early postnatal life is likely to reduce the risk of acquiring a life-threaten-ing infection.
In the present study there were fewer episodes of symptomatic, blood culture-positive sepsis in treated infants while receiving GM-CSF and during the sub-sequent week. However, the study was not designed to address this issue and had insufficient power to do so. This observation needs to be tested in a larger study, which we are currently planning.
Many questions remain over the most effective use of CSFs in neonates. Studies of therapeutic G-CSF are focused on whether mortality can be reduced when given to neonates with established sepsis and neu-tropenia. Current multicenter studies addressing this
issue have yet to report. In one single center study, 14 neutropenic neonates with systemic signs of infec-tion who received G-CSF for 3 days had a reduced mortality compared with similar, retrospectively se-lected controls.28 In another randomized placebo-controlled study involving a total of 20 infants with clinical signs of early onset sepsis, G-CSF adminis-tered for 3 days did not alter disease severity, mor-tality, or increase the neutrophil count in treated compared with control subjects.29 A recently pub-lished unrandomized study using G-CSF as prophy-laxis against infection in neutropenic newborns showed a reduction in sepsis rate [treated 13% (2/ 15); case-matched controls 54% (7/13)], very similar to that observed in our GM-CSF treated SGA sub-jects.52
The data reported here, which show that 5-day prophylactic GM-CSF completely abolishes postnatal neutropenia, including sepsis-related neutropenia, is apparently free from adverse effects and is perhaps able to reduce sepsis in high-risk neonates, indicates that this prophylactic approach warrants further in-vestigation.
ACKNOWLEDGMENTS
GM-CSF (Leucomax) was supplied by Novartis UK and Scher-ing-Plough UK.
Robert Carr had the original idea for this study. This study was designed and the clinical protocol written jointly by Robert Carr and Neena Modi. Rim El-Rifai and Dwight Lindo recruited the subjects and gathered data, with help from Anne Opute (Ham-mersmith Hospital) and Judy Rissik (Guy’s Hospital). The data were analyzed by Caroline Dore´. The paper was written by Robert Carr, Neena Modi and Caroline Dore´. Additional thanks go to Professor Anthony Milner and Anthony Kaiser (Department of Paediatrics, St Thomas’ Hospital) and Irene Roberts (Department of Haematology, Hammersmith Hospital) for their support.
REFERENCES
1. Baley JE, Fanaroff AA. Neonatal infections. In: Sinclair J, Bracken MB, eds.Effective Care of the Newborn Infant.Oxford, England: University Press; 1992:454 –506
2. Lacy JB, Ohlsson A. Administration of intravenous immunoglobulins for prophylaxis or treatment of infection in preterm infants: meta-analyses.Arch Dis Child.1995;72:F151–F155
3. Carr R, Modi N. Haemopoietic colony stimulating factors for preterm neonates.Arch Dis Child.1997;76:F128 –F133
4. Christensen RD. Neutrophil kinetics in the fetus and neonate.Am J Pediatr Hematol Oncol.1989;11:215–223
5. Hill HR. Biochemical, structural, and functional abnormalities of poly-morphonuclear leukocytes in the neonate.Pediatr Res.1987;22:375–382 6. Carr R, Pumford D, Davies JM. Neutrophil chemotaxis and adhesion in
preterm babies.Arch Dis Child.1992;67:813– 817
7. Falconer AE, Carr R, Edwards SW. Impaired neutrophil phagocytosis in preterm neonates: lack of correlation with expression of immunoglob-ulin or complement receptors.Biol Neonate.1995;68:264 –269
8. Ka¨llman J, Schollin J, Schale`n C, Erlandsson A, Kihlstro¨m E. Impaired phagocytosis and opsonisation toward group B streptococci in preterm neonates.Arch Dis Child.1998;78:F46 –F50
9. Christensen RD, Harper TE, Rothstein G. Granulocyte-macrophage pro-genitor cells in term and preterm neonates.J Pediatr.1986;109:1047–1051 10. Baley JE, Stork EK, Warkentin PI, Shurin SB. Neonatal neutropenia. Clinical manifestations, cause and outcome.Am J Dis Child.1988;142: 1161–1166
11. Rodwell RL, Taylor KMCD, Tudehope DI, Gray PH. Hematologic scor-ing system in early diagnosis of sepsis in neutropenic newborns.Pediatr Infect Dis J.1993;12:372–376
12. Christensen RD, Rothstein G. Exhaustion of mature marrow neutrophils in neonates with sepsis.J Pediatr.1980;96:316 –318
14. Schibler KR, Liechty KW, White WL, Christensen RD. Production of granulocyte colony-stimulating factor in vitro by monocytes from pre-term and pre-term neonates.Blood.1993;82:2478 –2484
15. Cairo MS, Yu Suen, Knoppel E, van de Ven C, Nguyen A, Sender L. Decreased stimulated GM-CSF production and GM-CSF gene expres-sion but normal numbers of GM-CSF receptors in human term new-borns compared with adults.Pediatr Res.1991;30:362–367
16. Bedford Russell AR, Davies EG, Gibson FM, Gordon-Smith EC. The in vitro effects of granulocyte and granulocyte-macrophage colony-stimulating factor on interleukin-3-dependent proliferation of human neonatal circulating progenitor cells.Pediatr Res.1995;37:630 – 633 17. Westwood NB, Chung R, Emmerson AJB, Pearson TC. The in vitro
effects of stem cell factor, interleukin 3 and granulocyte-macrophage colony stimulating factor on haemopoietic progenitor cells from prema-ture infants.Br J Haematol.1994;86:468 – 474
18. Cairo MS, Yu Suen, Knoppel E, Dana R, Park L, Clark S, van de Ven C, Sender L. Decreased G-CSF and IL-3 production and gene expression from mononuclear cells of newborn infants.Pediatr Res.1992;31:574 –578 19. Jaswon MS, Jones MH, Linch DC. The effects of recombinant human granulocyte-macrophage colony stimulating factor on the neutrophil respiratory burst in the term and preterm infant when studied in whole blood.Pediatr Res.1994;36:623– 627
20. Cairo MS, van de Ven C, Toy C, Mauss D, Sender L. Recombinant human granulocyte-macrophage colony-stimulating factor primes neo-natal granulocytes for enhanced oxidative metabolism and chemotaxis. Pediatr Res.1989;26:395–399
21. Frenck RW Jr, Buescher ES, Vadhan-Raj S. The effects of recombinant human granulocyte-macrophage colony stimulating factor on in vitro cord blood granulocyte function.Pediatr Res.1989;26:43– 48
22. Cairo MS, Plunkett JM, Mauss D, van de Ven C. Seven-day adminis-tration of recombinant human granulocyte colony-stimulating factor to newborn rats: modulation of neonatal neutrophilia, myelopoiesis, and group B Streptococcus sepsis.Blood.1990;76:1788 –1794
23. Frenck RW, Sarman G, Harper TE, Buescher ES. The ability of recom-binant murine granulocyte-macrophage colony-stimulating factor to protect neonatal rats from septic death due toStaphylococcus aureus. J Infect Dis.1990;162:109 –114
24. Cairo MS, Mauss D, Kommareddy S, Norris K, van de Ven C, Modanlou H. Prophylactic or simultaneous administration of recombinant human granulocyte colony stimulating factor in the treatment of group B streptococcal sepsis in neonatal rats.Pediatr Res.1990;27:612– 616 25. Gillan ER, Christensen RD, Yu Suen, Ellis R, van de Ven C, Cairo MS.
A randomized, placebo-controlled trial of recombinant human granu-locyte colony-stimulating factor administration in newborn infants with presumed sepsis: significant induction of peripheral and bone marrow neutrophilia.Blood.1994;84:1427–1433
26. Cairo MS, Christensen RD, Sender LS, Ellis R, Rosenthal J, van de Ven C, Worcester C, Agosti JM. Results of a phase I/II trial of recombinant human granulocyte-macrophage colony-stimulating factor in very low birthweight neonates: significant induction of circulatory neutrophils, monocytes, platelets, and bone marrow neutrophils.Blood. 1995;86: 2509 –2515
27. Bedford Russell AR, Davies EG, Ball SE, Gordon-Smith E. Granulocyte colony-stimulating factor treatment for neonatal neutropenia.Arch Dis Child.1995;72:F53–F54
28. Kocherlakota P, La Gamma EF. Human granulocyte colony-stimulating factor may improve outcome attributable to neonatal sepsis compli-cated by neutropenia. Pediatrics. 1997;100(1). URL: http:// www.pediatrics.org/cgi/content/full/100/1/e6
29. Schibler KR, Osborne KA, Leung LY, et al. A randomized placebo-controlled trial of granulocyte colony-stimulating factor administration to newborn infants with neutropenia and clinical signs of early-onset sepsis.Pediatrics.1998;102:6 –13
30. Roberts RL, Szelc CM, Scates SM, et al. Neutropenia in an extremely premature infant treated with recombinant human granulocyte colony-stimulating factor.Am J Dis Child.1991;145:808 – 812
31. La Gamma EF, Alpan O, Kocherlakota P. Effect of granulocyte colony-stimulating factor on preeclampsia-associated neonatal neutropenia. J Pediatr.1995;126:457– 459
32. Makhlouf RA, Doron MW, Bose CL, Price WA, Stiles AD. Administra-tion of granulocyte colony-stimulating factor to neutropenic low birth
weight infants of mothers with preeclampsia. J Pediatr. 1995;126: 454 – 459
33. Rapoport AP, Abboud CN, DiPersio JF. Granulocyte-macrophage col-ony-stimulating factor (GM-CSF) and granulocyte colcol-ony-stimulating factor (G-CSF): receptor biology, signal transduction, and neutrophil activation.Blood Rev.1992;6:43–57
34. Sullivan GW, Carper HT, Mandell GL. The effect of three human recombinant hematopoietic growth factors (granulocyte-macrophage colony-stimulating factor, granulocyte colony-stimulating factor, and interleukin-3) on phagocyte oxidative activity.Blood.1993;81:1863–1870 35. Nemunaitis J, Cox J, Meyer W. Comparison of neutrophil and monocyte function by microbial cell-kill assay in patients with cancer receiving granulocyte colony-stimulating factor, granulocyte-macrophage colony-stimulating factor, or no cytokine after cytotoxic chemotherapy. A phase II trial.Am J Clin Oncol.1998;21:308 –312
36. Williams MA, Kelsey SM, Collins PW, Gutteridge CN, Newland AC. Administration of rHuGM-CSF activates monocyte reactive oxygen species secretion and adhesion molecule expression in vivo in patients following high-dose chemotherapy.Br J Haematol.1995;90:31– 40 37. Manroe BL, Weinberg AG, Rosenfeld CR, Browne R. The neonatal blood
count in health and disease. I. Reference values for neutrophilic cells. J Pediatr.1979;95:89 –98
38. Mouzinho A, Rosenfeld CR, Sa´nchez PJ, Risser R. Revised reference ranges for circulating neutrophils in very-low-birth-weight neonates. Pediatrics.1994;94:76 – 82
39. Matthews JNS, Altman DG, Campbell MJ, Royston P. Analysis of serial measurements in medical research.Br Med J.1990;300:230 –235 40. CRIB Investigators’ Group and writing committee. The CRIB (clinical
risk index for babies) score: a tool for assessing initial neonatal risk and comparing performance of neonatal intensive care units.Lancet.1993; 342:193–198
41. Erdman SH, Christensen RD, Bradley PP, Rothstein G. Supply and release of storage neutrophils. A developmental study.Biol Neonate. 1982;41:132–137
42. Koenig JM, Christensen RD. The mechanism responsible for diminished neutrophil production in neonates delivered of women with pregnancy-induced hypertension.Am J Obstet Gynaecol.1991;165:467– 473 43. Lieschke GJ, Cebon J, Morstyn G. Characterization of the clinical effects
after the first dose of bacterially synthesized recombinant human gran-ulocyte-macrophage colony-stimulating factor. Blood. 1989;74: 2634 –2643
44. Lieschke GJ, Maher D, O’Connor M, Green M, Sheridan W, Rawlings M. Phase I study of intravenously administered bacterially synthesized granulocyte-macrophage colony-stimulating factor and comparison with subcutaneous administration.Cancer Res.1990;50:606 – 614 45. Naparstek E. Granulocyte colony-stimulating factor, congenital
neutro-penia, and acute myeloid leukemia.N Engl J Med.1995;333:516 –518 46. Fan Dong, Brynes RK, Tidow N, Welte K, Lo¨wenberg B, Touw IP.
Mutations in the gene for the granulocyte colony-stimulating-factor receptor in patients with acute myeloid leukemia preceded by severe congenital neutropenia.N Engl J Med.1995;333:487– 493
47. Fairbairn LJ, Cowling GJ, Reipert BM, Dexter TM. Suppression of apo-ptosis allows differentiation and development of a multipotent hemo-poietic cell line in the absence of added growth factors.Cell.1993;74: 823– 832
48. Stoffel R, Ledermann B, de Sauvage FJ, Skoda RC. Evidence for a selective-permissive role of cytokine receptors in hematopoietic cell fate decisions.Blood.1997;90(suppl 1):123. Abstract
49. Rosenthal J, Healey T, Ellis R, Gillan E, Cairo MS. A two-year follow-up of neonates with presumed sepsis treated with recombinant human granulocyte colony-stimulating factor during the first week of life. J Pediatr.1996;128:135–137
50. Koenig JM, Christensen RD. Incidence, neutrophil kinetics, and natural history of neonatal neutropenia associated with maternal hypertension. N Engl J Med.1989;321:557–562
51. Cadnapaphornchai M, Faix RG. Increased noscomial infection in neu-tropenic low birth weight (2000 grams or less) infants of hypertensive mothers.J Pediatr.1992;121:956 –961
DOI: 10.1542/peds.103.4.796
1999;103;796
Pediatrics
Robert Carr, Neena Modi, Caroline J. Doré, Rim El-Rifai and Dwight Lindo
Colony-Stimulating Factor in Human Newborns Less Than 32 Weeks Gestation
A Randomized, Controlled Trial of Prophylactic Granulocyte-Macrophage
Services
Updated Information &
http://pediatrics.aappublications.org/content/103/4/796
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/103/4/796#BIBL
This article cites 50 articles, 12 of which you can access for free at:
Subspecialty Collections
b
http://www.aappublications.org/cgi/collection/infectious_diseases_su
Infectious Disease
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
http://www.aappublications.org/cgi/collection/agency_abcs
Agency ABC's
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.103.4.796
1999;103;796
Pediatrics
Robert Carr, Neena Modi, Caroline J. Doré, Rim El-Rifai and Dwight Lindo
Colony-Stimulating Factor in Human Newborns Less Than 32 Weeks Gestation
A Randomized, Controlled Trial of Prophylactic Granulocyte-Macrophage
http://pediatrics.aappublications.org/content/103/4/796
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.