Effects of Individualized Developmental Care in a
Randomized Trial of Preterm Infants
⬍
32 Weeks
WHAT’S KNOWN ON THIS SUBJECT: Follow-up studies of the
effectiveness of NIDCAP showed conflicting results and were based on trials with small sample sizes. A Cochrane meta-analysis recommended conducting larger trials with more follow-up monitoring.
WHAT THIS STUDY ADDS: This large RCT comparing NIDCAP with
basic developmental care showed no significant improvement in respiratory support, days of intensive care, or growth or neuromotor development at term age.
abstract
OBJECTIVE:The goal was to investigate the effects of the Newborn
Individualized Developmental Care and Assessment Program (NIDCAP) on days of respiratory support and intensive care, growth, and neuro-motor development at term age for infants born at⬍32 weeks.
METHODS:Infants were assigned randomly, within 48 hours after
birth, to a NIDCAP group or basic developmental care (control) group. The NIDCAP intervention consisted of weekly formal behavioral obser-vations of the infants and caregiving recommendations and support for staff members and parents, as well as incubator covers and posi-tioning aids. The control group infants were given basic developmental care, which consisted of only incubator covers and positioning aids. Out-come measures were respiratory support, intensive care, and weight of ⬍1000 g. Growth parameters were measured weekly or biweekly and at term age. Neuromotor development was assessed at term age.
RESULTS:A total of 164 infants met the inclusion criteria (NIDCAP:N⫽ 81; control: N⫽83). In-hospital mortality rates were 8 (9.9%) of 81 infants in the NIDCAP group and 3 (3.6%) of 83 infants in the control group. No differences in mean days of respiratory support (NIDCAP: 13.9 days; control: 16.3 days) or mean days of intensive care (NIDCAP: 15.2 days; control: 17.0 days) were found. Short-term growth and neu-romotor development at term age showed no differences, even with correction for the duration of the intervention.
CONCLUSIONS:NIDCAP developmental care had no effect on
respira-tory support, days of intensive care, growth, or neuromotor development at term age.Pediatrics2009;124:1021–1030
AUTHORS:Celeste M. Maguire, PhD,aFrans J. Walther,
MD, PhD,aArwen J. Sprij, MD,bSaskia Le Cessie, PhD,c
Jan M. Wit, MD, PhD,aand Sylvia Veen, MD, PhD,afor the
Leiden Developmental Care Project
aDepartment of Pediatrics, Division of Neonatology, and cDepartment of Medical Statistics, Leiden University Medical
Center, Leiden, Netherlands; andbDepartment of Pediatrics,
Division of Neonatology, Juliana Children’s Hospital, The Hague, Netherlands
KEY WORDS
preterm infants, developmental care, Newborn Individualized Developmental Care and Assessment Program, growth, respiratory support, intensive care, neurodevelopment
ABBREVIATIONS
NIDCAP—Newborn Individualized Developmental Care and Assessment Program
RCT—randomized, controlled trial PDA—patent ductus arteriosus
CPAP— continuous positive airway pressure GA— gestational age
This trial has been registered at www.trialregister.nl (identifier ISRCTN84995192).
www.pediatrics.org/cgi/doi/10.1542/peds.2008-1881
doi:10.1542/peds.2008-1881
Accepted for publication Apr 9, 2009
Address correspondence to Sylvia Veen, MD, PhD, Department of Pediatrics, J-6-S, Leiden University Medical Center, PO Box 9600, 2300 RC Leiden, Netherlands. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
Advanced technology in neonatal care has resulted in increased survival rates for preterm infants1–3but not in
major improvements in morbidity rates or decreased risks of develop-mental delays, physical disabilities, and behavioral disorders.1,4,5
Develop-mental care programs have been used to support infants and families in the NICU. Most research has been based on the Newborn Individualized Devel-opmental Care and Assessment Pro-gram (NIDCAP), in which caregiving is based on the individual behavior of the infant.6 Evidence showing positive
ef-fects of NIDCAP is inconclusive, and ad-ditional randomized, controlled trials (RCTs) with larger sample sizes and long-term follow-up monitoring have been recommended.7
Between April 2000 and May 2002, our first RCT comparing basic develop-mental care (incubator covers, nests, and positioning aids) with standard care showed no short-term effects.8The
aim of this RCT was to explore the effec-tiveness of the more-comprehensive NIDCAP, compared with basic develop-mental care, with respect to neonatal morbidity, neuromotor development, and growth at term age of preterm in-fants of gestational age (GA) of⬍32 weeks.
METHODS
Study Design and Intervention
The study was carried out by using a standard protocol, at two locations of a tertiary NICU in the Netherlands: den University Medical Center in Lei-den and Juliana Children’s Hospital in the Hague. The inclusion criterion was GA of ⬍32 weeks; exclusion criteria were major congenital anomalies, a need for major surgery, and having a drug-addicted mother. After parental informed consent was obtained, in-fants were assigned randomly to the NIDCAP or control group within 48 hours after birth, by using sealed
en-velopes prepared in groups of 6 through computer-generated random-ization. Power analysis performed be-fore the study showed that a sample size of 140 infants was needed to show a significant difference (P⬍.05) with a power of 80%, on the basis of a differ-ence of 0.5 SD in the Bayley II scores at 1 and 2 years of age, which was deemed sufficient power for the short-term primary neonatal outcomes.
The NIDCAP intervention consisted of weekly behavioral observations of the infants by trained, certified, NIDCAP de-velopmental specialists, with the first observation occurring within 48 hours after birth. Individual care plans that were based on these observations, with caregiving recommendations, were formulated with parents’ and caregivers’ input and were available at the infant’s bedside. Parents were sup-ported in understanding their infant’s behavior and how to approach and to support their infant during caregiving interactions and were provided with photographic booklets explaining
pre-term infant behavior. Infants in the NIDCAP group were cared for primarily by nurses who had received extra training and support in behavior-based, individualized, developmental care and were familiar with perform-ing individualized care on the basis of the infant’s behavior and recommen-dations. Incubator covers, nests, and positioning aids to encourage flexion and containment were used. Reflection periods for discussion and support were provided for the NIDCAP care team, as was daily support for the par-ents. If an infant was transferred to a regional hospital, then a report with recommendations for caregiving was prepared for the parents. A NIDCAP-certified developmental psychologist supervised the intervention, con-ducted observations, and supported the parents and staff members. In-fants in the control group received only basic developmental care (incu-bator covers, nests, and positioning aids). Control group nurses performed basic developmental care. No formal
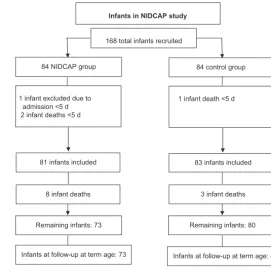
168 total infants recruited
84 NIDCAP group
1 infant excluded due to admission <5 d 2 infant deaths <5 d
1 infant death <5 d
81 infants included 83 infants included
8 infant deaths 3 infant deaths
Remaining infants: 73 Remaining infants: 80 84 control group
Infants at follow-up at term age: 73 Infants at follow-up at term age: 80 Infants in NIDCAP study
FIGURE 1
observations in which the control in-fants’ behavior was described were made. The ethics committees of both locations approved the study.
Neonatal Outcomes and Follow-up Evaluations
Primary medical outcomes were days of respiratory support, days of inten-sive care, and short-term growth. Mechanical ventilation (synchronized intermittent mandatory ventilation and/or high-frequency oscillation) and continuous positive airway pressure (CPAP) therapy were measured in days. If an infant received both me-chanical ventilation and CPAP therapy in the same day, then the method of respiratory support used for more hours was chosen. Days of respiratory support were defined as total com-bined days of mechanical ventilation and CPAP therapy. Short-term growth (weight, head circumference, and length) was measured at term age; mean daily weight gain (in grams) and mean weekly length and head circum-ference growth (in centimeters) also were recorded.
Discharge from intensive care was based on the infant requiring no me-chanical ventilation and/or CPAP ther-apy for 24 hours and weighingⱖ1000 g. Infants were seen at term age by neonatologists who were experienced in developmental assessments and were blinded to the group assignment of the infants. A standardized neuro-logic examination, as described by Pre-chtl,9was performed, and results were
defined as definitely abnormal (pres-ence of a full neonatal neurologic syn-drome, such as apathy, hyperexcitability, hypotonia, hypertonia, hyporeflexia, hy-perreflexia, hypokinesia, or hyperkine-sia, or a hemisyndrome), mildly abnor-mal (presence of only part of such a syndrome), or normal. Examples of mi-nor neurologic signs are abmi-normal posture, abnormal head control, and
absent or abnormal responses or re-flexes. Secondary outcomes are de-fined in the tables and were described in a previous article.8
Statistical Analyses
Data were analyzed by using SPSS 14.0 for Windows (SPSS Inc, Chicago, IL). In-fant and parent characteristics and outcome parameters were compared with the 2 test (for trend) or the
2-sample ttest or Mann-Whitney test where appropriate.P values of⬍.05 were considered significant. Linear re-gression was used to evaluate the in-fluence of the duration of the interven-tion on term age outcomes, by testing whether there was an interaction ef-fect between the intervention dura-tion and the 2 treatment groups.
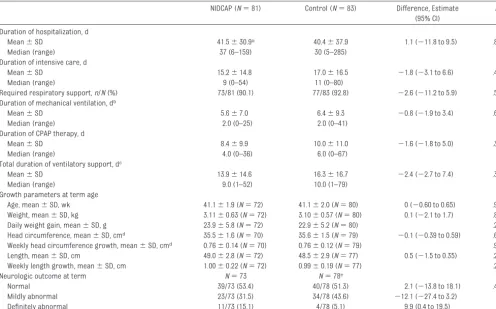
Me-dian days of CPAP therapy, days of respiratory support, and days of in-tensive care were obtained from Kaplan-Meier curves and were com-pared by using the log-rank test, with measurements for infants who died being censored.
RESULTS
Study Groups
A total of 168 infants (NIDCAP:N⫽84; control:N⫽ 84) were recruited be-tween July 2002 and August 2004. Four infants (NIDCAP:n⫽3; control: n ⫽ 1) were excluded according to protocol because they were trans-ferred to another hospital or died within the first 5 days of admission, leaving a total of 164 infants who met TABLE 1 Maternal Medical and Parental Demographic Background Variables
NIDCAP (N⫽81) Control (N⫽83) Obstetric history,n/N(%)
Preexisting disease (diabetes mellitus, hypertension, or other)
9/81 (11.1) 14/83 (16.9)
Pregnancy induction 13/81 (16.0) 14/83 (16.9)
Disease during pregnancy,n/N(%)
Diabetes mellitus gravidarum 2/81 (2.5) 3/83 (3.6)
Preeclampsia, eclampsia, or HELLP syndrome 13/81 (16.0) 16/83 (19.3) Medication use during pregnancy,n/N(%)
Antihypertensive agents 14/81 (17.3) 19/83 (22.9)
Antibiotics 32/81 (39.5) 25/83 (30.1)
Tocolytic agents 45/81 (55.6) 43/83 (51.8)
Other 7/81 (8.6) 14/83 (16.9)
Prenatal glucocorticoid treatment,n/N(%)
1 dose 29/80 (36.3) 35/83 (42.2)
1 course (2 doses) 33/80 (41.3) 29/83 (34.9)
Mode of delivery,n/N(%)
Vaginal 41/81 (50.6) 45/83 (54.2)
Cesarean section 40/81 (49.4) 38/83 (45.8)
PROM for⬎24 h,n/N(%) 25/81 (30.9) 19/83 (22.9)
Primipara,n/N(%) 54/81 (66.7) 42/83 (50.6)
Parental demographic background
Maternal age, mean⫾SD, y 30.0⫾5.2 (N⫽74) 31.9⫾5.0 (N⫽78) Paternal age, mean⫾SD, y 32.3⫾5.6 (N⫽72) 34.1⫾5.5 (N⫽77)
Mother white,n/N(%) 66/80 (82.5) 70/80 (87.5)
Father white,n/N(%) 63/79 (79.7) 64/80 (80.0)
Education level of mother,n/N(%)a
Low 26/72 (36.1) 19/77 (24.7)
Intermediate 25/72 (34.7) 26/77 (33.8)
High 21/72 (29.2) 32/77 (41.6)
Education level of father,n/N(%)a
Low 19/69 (27.5) 15/76 (19.7)
Intermediate 22/69 (31.9) 32/76 (42.1)
High 28/69 (40.6) 29/76 (38.2)
HELPP, hemolysis, elevated liver enzyme levels, and low platelet count; PROM indicates premature rupture of membranes.
the inclusion criteria. Of these in-fants, 8 (9.9%) of 81 in the NIDCAP group and 3 (3.6%) of 83 in the con-trol group died during hospitaliza-tion, with the main cause of death being cerebral or pulmonary compli-cations. The mortality rate and loss to follow-up monitoring are shown in Fig 1. Parent and infant characteris-tics were similar, with no significant differences being found (Tables 1 and 2).
Primary Outcomes
No significant differences in the days of intensive care, days of respiratory support, or growth were found be-tween the NIDCAP and control groups. There were no significant differences between the NIDCAP and control groups in the neurologic outcomes or
growth parameters at term age, in daily weight gain, or in weekly length and head circumference growth (Ta-ble 3). Linear regression analysis showed no interaction effect between the intervention duration and the 2 treatment groups with respect to neu-rologic outcome (P⫽.72) or term age growth, including head circumference (P⫽.94), weight (P⫽.28), and length (P ⫽ .54). No interaction effect was found between the 2 sites in total days of ventilatory support (P⫽.7), weight at term age (P⫽.07), or head circum-ference at term age (P⫽.07). Differ-ences were not significant except for term length in the Leiden Hospital site (mean⫾SD: control: 48.4⫾2.9 cm; in-tervention: 49.9⫾2.1 cm;P⫽.006); the intervention group performed slightly
better in the Leiden hospital site and slightly worse in the Juliana Children’s Hospital site.
Secondary Outcomes
No differences were found between groups in the total length of stay from birth to discharge from the hospital or the GA of infants at discharge from the hospital. There was no difference be-tween the 2 groups in the days of oxy-gen therapy, numbers of infants who required oxygen after 28 days, or inci-dence of bronchopulmonary dysplasia. A total of 7 (8.6%) of 81 infants in the NIDCAP group required postnatal cor-ticosteroid treatment, compared with 11 (13.3%) of 83 infants in the control group (P⫽ .35), with twice as many infants in the control group requir-ing corticosteroid treatment for ⬎2 weeks. There were significantly more infants in the NIDCAP group (25 [30.9%] of 81 infants) than in the control group (11 [13.3%] of 83 infants) with patent ductus arteriosus (PDA) requiring medication and/or surgical ligation. Of the 25 infants with PDA in the NIDCAP group, 6 (24%) of 25 died in the hospi-tal; 1 (9%) of 11 infants with PDA in the control group died. Among the surviv-ing infants, the NIDCAP group still had twice as many infants with PDA (19 [26%] of 73 infants), compared with the control group (10 [12.5%] of 80 in-fants;P ⫽ .03). No significant differ-ences in the remaining secondary out-comes were found (Table 4).
Survivor Analyses
A Kaplan-Meier analysis that included respiratory data for infants who died in the hospital was performed, with no differences found in the total popula-tion (Fig 2). Because of the significant difference in the incidence of PDA be-tween the groups (Table 4), a posthoc analysis was performed and stratified with respect to infants with PDA re-quiring medication/surgery versus in-fants without significant PDA. In the TABLE 2 Infant Medical Background Variables for All Participating Infants
NIDCAP Control
GA, wk N⫽81 N⫽83
Mean⫾SD 29.3⫾1.8 29.2⫾1.6
Range 24.7–31.9 25.6–31.6
Birth weight, g N⫽81 N⫽83
Mean⫾SD 1215⫾328 1226⫾343
Range 577–1939 625–2060
Length, cm N⫽81 N⫽83
Mean⫾SD 37.1⫾3.1 36.8⫾3.3
Range 29.0–43.0 29.0–44.0
Head circumference, cm N⫽81 N⫽83
Mean⫾SD 26.8⫾2.2 26.6⫾2.3
Range 22.4–32.0 21.5–30.5
Male,n/N(%) 46/81 (56.8) 43/83 (51.8)
SGA,⬍10th andⱖ3rd percentile,n/N(%) 15/81 (18.5) 10/83 (12.0) SGA,⬍3rd percentile,n/N(%) 3/81 (3.7) 5/83 (6.0)
Twin,n/N(%) 27/81 (33.3) 34/83 (41.0)
Inborn,n/N(%) 51/81 (63.0) 49/83 (59.0)
Apgar score at 5 min N⫽80 N⫽80
Mean⫾SD 8.1⫾2.2 8.3⫾1.4
Median 8 8
Range 3–10 4–10
CRIB score N⫽81 N⫽83
Median 2 3
Range 0–14 0–13
RDS,n/N(%)
Grade 1 20/81 (24.7) 23/82 (28.0)
Grade 2 11/81 (13.6) 13/82 (15.9)
Grade 3 17/81 (21.0) 17/82 (20.7)
Grade 4 6/81 (7.4) 8/82 (9.8)
Surfactant treatment,n/N(%) 41/81 (50.6) 39/83 (47.0) Hyperbilirubinemia,n/N(%) 73/81 (90.1) 76/83 (91.6) Duration of phototherapy, mean⫾SD, d 4.4⫾2.9 4.8⫾3.4
Comparisons were performed by using2tests (for linear trend) orttests where appropriate. SGA indicates small for GA;
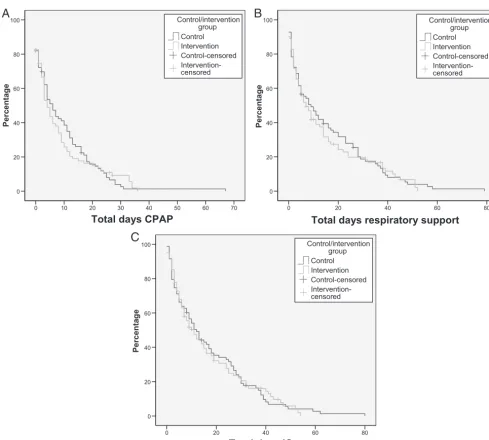
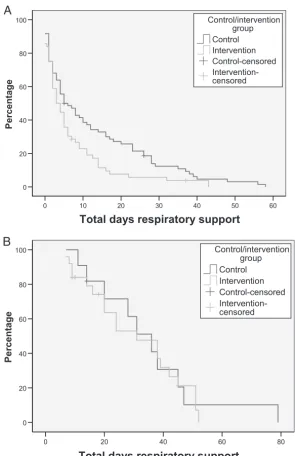
subgroup of infants with no PDA, the NIDCAP group required fewer days of CPAP therapy (P⫽.02), total respira-tory support (P⫽.02), and intensive care (P⫽.06), compared with the con-trol group (Fig 3). Because photother-apy may influence the closure and/or reopening of a PDA,10 days of
photo-therapy were compared, but no differ-ence between the groups was found (mean: NIDCAP: 4.4 days; control: 4.8 days).
DISCUSSION
Overall Findings
In this RCT examining short-term ef-fects of the comprehensive NIDCAP, compared with basic developmental care, on neonatal morbidity, neuro-logic outcomes, and growth at term
age of infants born at⬍32 weeks, no significant positive effects of the inter-vention on the need for respiratory support or days of intensive care were found. No differences between the NIDCAP and control groups with re-spect to growth and neurologic out-comes at term age were found with correction for days of intervention.
Respiratory Support
A Cochrane meta-analysis found that infants who received NIDCAP care showed significantly fewer days of ven-tilation and no differences in days of oxygen therapy; the authors stated that the results were conflicting and, be-cause the studies showed much hetero-geneity, the results should be viewed with caution.11A RCT of 25 infants who
were born at GA of⬍32 weeks and re-quired ventilatory support at 24 hours showed no significant difference in days of mechanical ventilation, a trend in days of CPAP therapy in favor of the NIDCAP group (NIDCAP: 43.9 days; control: 26.1 days;P⫽.045), and a younger postcon-ceptual age of oxygen withdrawal.12The
number of patients included in that study was small (NIDCAP:N⫽12; con-trol:N⫽13), because the trial needed to be terminated earlier than expected.12
Earlier NIDCAP studies by Als et al13and
Fleischer et al14also showed positive
re-sults concerning the need for ventilatory support; however, only infants born at GA of ⬍30 weeks and birth weight of ⬍1250 g were included, and specific ventilation inclusion criteria were used. A 3-center trial showed significant differ-TABLE 3 Comparison of Data on Primary Outcome Measures
NIDCAP (N⫽81) Control (N⫽83) Difference, Estimate (95% CI)
P
Duration of hospitalization, d
Mean⫾SD 41.5⫾30.9a 40.4⫾37.9 1.1 (⫺11.8 to 9.5) .83
Median (range) 37 (6–159) 30 (5–285)
Duration of intensive care, d
Mean⫾SD 15.2⫾14.8 17.0⫾16.5 ⫺1.8 (⫺3.1 to 6.6) .46
Median (range) 9 (0–54) 11 (0–80)
Required respiratory support,n/N(%) 73/81 (90.1) 77/83 (92.8) ⫺2.6 (⫺11.2 to 5.9) .54 Duration of mechanical ventilation, db
Mean⫾SD 5.6⫾7.0 6.4⫾9.3 ⫺0.8 (⫺1.9 to 3.4) .60
Median (range) 2.0 (0–25) 2.0 (0–41)
Duration of CPAP therapy, d
Mean⫾SD 8.4⫾9.9 10.0⫾11.0 ⫺1.6 (⫺1.8 to 5.0) .35
Median (range) 4.0 (0–36) 6.0 (0–67)
Total duration of ventilatory support, dc
Mean⫾SD 13.9⫾14.6 16.3⫾16.7 ⫺2.4 (⫺2.7 to 7.4) .35
Median (range) 9.0 (1–52) 10.0 (1–79)
Growth parameters at term age
Age, mean⫾SD, wk 41.1⫾1.9 (N⫽72) 41.1⫾2.0 (N⫽80) 0 (⫺0.60 to 0.65) .94 Weight, mean⫾SD, kg 3.11⫾0.63 (N⫽72) 3.10⫾0.57 (N⫽80) 0.1 (⫺2.1 to 1.7) .86
Daily weight gain, mean⫾SD, g 23.9⫾5.8 (N⫽72) 22.9⫾5.2 (N⫽80) .25
Head circumference, mean⫾SD, cmd 35.5⫾1.6 (N⫽70) 35.6⫾1.5 (N⫽79) ⫺0.1 (⫺0.39 to 0.59) .62
Weekly head circumference growth, mean⫾SD, cmd 0.76⫾0.14 (N⫽70) 0.76⫾0.12 (N⫽79) .90
Length, mean⫾SD, cm 49.0⫾2.8 (N⫽72) 48.5⫾2.9 (N⫽77) 0.5 (⫺1.5 to 0.35) .23 Weekly length growth, mean⫾SD, cm 1.00⫾0.22 (N⫽72) 0.99⫾0.19 (N⫽77) .29
Neurologic outcome at term N⫽73 N⫽78e
Normal 39/73 (53.4) 40/78 (51.3) 2.1 (⫺13.8 to 18.1) .47
Mildly abnormal 23/73 (31.5) 34/78 (43.6) ⫺12.1 (⫺27.4 to 3.2)
Definitely abnormal 11/73 (15.1) 4/78 (5.1) 9.9 (0.4 to 19.5)
Comparisons were performed by using2tests (for linear trend),ttests, or Mann-Whitney tests where appropriate. CI indicates confidence interval. aAlso indicates number of days intervention was given.
bSynchronized intermittent mandatory ventilation and/or high-frequency oscillation.
cTotal days of synchronized intermittent mandatory ventilation, high-frequency oscillation, and CPAP therapy combined.
ences in respiratory support between the NIDCAP group and the control group, but there were differences between sites (parental demographic and infant medical background variables).11,15Our
study included infants who were born at⬍32 weeks, regardless of their need for ventilatory support, and had lower Clinical Risk Index for Babies scores,16
which indicated that they were in more-stable condition in the first 12 hours of life.
Days of Intensive Care
A 3-center RCT of 92 preterm infants with birth weights of⬍1250 g and GAs
of ⬍28 weeks showed significantly fewer days of intensive care for the NIDCAP group.15 We were not able to
duplicate those findings in our study; however, our population was different, in that we included older infants with GAs of⬍32 weeks, with no restriction on birth weight. The total number of days of intensive care in our study was considerably less than that in the aforementioned study, which perhaps reflects the different populations or different definitions of days of inten-sive care, because the criteria for days of intensive care were not defined in the multicenter trial. Another Dutch
study found no significant difference in days of intensive care between NIDCAP and conventional care but also did not define the criteria for days of intensive care and included only infants with GAs of ⬍30 weeks.17 Other NIDCAP
studies reported total days of hospital-ization but not days of intensive care.
Growth
One study by Als et al15showed
signifi-cantly better average daily weight gain and better growth (weight, head cir-cumference, and height) to term age for the infants receiving NIDCAP, whereas the study by Westrup et al12
showed no significant effect on growth (weight gain and head growth) up to postconceptual age of 35 weeks. The Cochrane meta-analysis,11 which
ex-cluded the multicenter trial by Als et al15because of site differences,
con-cluded that NIDCAP did not affect growth for infants surviving to cor-rected age of 9 months. Our short-term growth results are comparable to those findings.
Neurobehavioral Outcomes
Two previous NIDCAP studies showed significant improvements in neurobe-havioral outcomes, according to the method described by Prechtl,9 which
they defined with 12 summary vari-ables and a total score showing the proportion of abnormal scores in each group.18,19We found no significant
dif-ference in our study, in which neurobe-havioral outcomes, according to the method described by Prechtl,9 were
defined as definitely abnormal, mildly abnormal, or normal.
Incidence of PDA
After random assignment, our study showed significantly more infants in the NIDCAP group with PDA requiring medication or surgery (Table 4). The mean days of phototherapy, which can influence ductal reopening, were simi-lar for the 2 groups; therefore, there is TABLE 4 Comparison of Data on Secondary Outcome Measures
NIDCAP (N⫽81) Control (N⫽83) P
In-hospital death,n/N(%) 8/81 (9.9) 3/83 (3.6) .14
Early neonatal deatha 1/81 (1.2) 0/83 (0)
Late neonatal deatha 7/81 (8.6) 3/83 (3.6)
LOS, d N⫽70 N⫽74 .24
Mean⫾SD 61.9⫾24.5 67.6⫾34.2
Median (range) 57.5 (32–159) 58.5 (30–285)
GA at discharge to home, mean⫾SD, wk 38.5⫾2.7 (N⫽70) 38.9⫾4.4 (N⫽74) .50 Total time of supplemental oxygen treatment, d
Mean⫾SD 17.2⫾22.6 16.4⫾25.4 .84
Median (range) 6 (0–100) 3 (0–121)
Oxygen requirement at⬎28 d of life,n/N(%) 25/81 (30.9) 24/82 (29.3) .82 BPD (oxygen dependence after 36 wk of
postconceptual age),n/N(%)
12/80 (15.0) 16/81 (19.8) .43
Postnatal corticosteroid treatment,n/N(%)b
⬍7 d 1/81 (1.2) 1/83 (1.2) .35
7–14 d 2/81 (2.5) 2/83 (2.4)
15–20 d 2/81 (2.5) 7/83 (8.4)
⬎20 d 2/81 (2.5) 1/83 (1.2)
IVH,n/N(%)
Grade I–II 17/81 (21.0) 19/83 (22.9) .72
Grade III (and periventricular echodensity) 6/81 (7.4) 4/83 (4.8)
Posthemorrhagic ventricular dilation,n/N(%) 2/81 (2.5) 6/83 (7.2) .16
NEC,n/N(%) 3/81 (3.7) 3/83 (3.6) .86
Sepsis,n/N(%) 38/81 (46.9) 45/83 (54.2) .35
Meningitis,n/N(%) 1/81 (1.2) 1/83 (1.2) .99
PDA (indomethacin and/or surgery),n/N(%) 25/81 (30.9) 11/83 (13.3) .01c
Dopamine/dobutamine treatment,n/N(%) 22/81 (27.2) 23/83 (27.7) .94
ROP,n/N(%) 8/70 (11.4) 10/73 (13.7) .82
PVL at follow-up evaluation at term age,n/N(%)
Grade 1 5/72 (6.9) 10/80 (12.5) .76
Grade 2 1/72 (1.4) 0 (0)
Grade 3 1/72 (1.4) 1/80 (1.3)
Grade 4 0 (0) 0 (0)
Physical therapy required at term age,n/N(%) 16/73 (21.9) 11/80 (13.8) .32
Comparisons were performed by using2tests (for linear trend) orttests where appropriate. LOS indicates length of stay
until discharge to home; BPD, bronchopulmonary dysplasia22; IVH, intraventricular hemorrhage23; NEC, necrotizing
entero-colitis; PDA, patent ductus arteriosus; ROP, retinopathy of prematurity; PVL, periventricular leukomalacia.24
aEarly neonatal death denotes death within the first 7 days of life; late neonatal death denotes death after 7 days but before
28 days of life.
no plausible reason why infants in the NIDCAP group had significantly more cases of PDA that needed treatment.10
Most of the infants (NIDCAP: 17 of 19 infants; control: 9 of 10 infants) were given a 3-dose course of indomethacin, which successfully closed the PDA. Two infants in the NIDCAP group and 2 in the control group were given a course of indomethacin and then treated with surgical ligation. These findings differ from the outcomes in the Cochrane
meta-analysis,11in which no influence
of the NIDCAP intervention on the inci-dence of PDA was found.
Because PDA may influence days of ventilation and days of intensive care, we performed further analysis (Kaplan-Meier analysis). In the subgroup of in-fants with no PDA (NIDCAP:n⫽56; con-trol: n ⫽ 72), we found significant differences in days of CPAP therapy and total respiratory support in favor of the NIDCAP group. We assume, on
clinical grounds, that most of the PDA cases were diagnosed after inclusion (within 48 hours after birth) in the study. Although there may be a possi-ble benefit from NIDCAP in days of re-spiratory support for a subgroup of in-fants without PDA, these findings should be interpreted with caution. The presence of PDA did seem to influ-ence neurodevelopmental outcomes, because 7 (64%) of 11 infants in the NIDCAP group with definitely abnormal
70 60 50 40 30 20 10 0 100
80
60
40
20
0
Percentage
Total days CPAP
80 60
40 20
0 100
80
60
40
20
0
Percent
a
ge
Total days respiratory support
80 60
40 20
0 100
80
60
40
20
0
P
e
rcenta
g
e
Total days IC
Intervention-censored Control-censored Intervention Control
Control/intervention group
Intervention-censored Control-censored Intervention Control
Control/intervention group
Intervention-censored Control-censored Intervention Control
Control/intervention group
A
B
C
FIGURE 2
scores on the Prechtl examination at term age had PDA and only 1 (25%) of 4 control infants with definitely abnormal scores had PDA, which reflects the higher incidence of PDA in the NIDCAP group. There also were more boys (57.9% vs 30%) and small-for-GA in-fants (31.6% vs 20%) with PDA in the NIDCAP group than in the control group.
Secondary Outcomes
Wielenga et al17showed that
NIDCAP-treated infants had a lower incidence of severe cerebral damage in a phase-lag study of infants born at⬍30 weeks of gestation, in which 26 infants re-ceived conventional treatment, fol-lowed by 25 infants who received NIDCAP developmental care. There were significant differences in the neonatal
background characteristics of the 2 groups (NIDCAP-treated infants were smaller and included fewer multiple births, compared with the conven-tional care group, and the NIDCAP-treated infants developed significantly more pneumonia, possibly because of an outbreak of a nosocomial infection in the NICU during the NIDCAP imple-mentation). One advantage of a phase-lag study is the ability to implement a program such as NIDCAP throughout the entire department; however, the disadvantage of having different peri-ods of research, in which there may be changes in the department, may affect results. Therefore, the authors stated that their results should be inter-preted with caution.17
A meta-analysis of 3 studies13,18,20
showed no evidence that NIDCAP af-fected the incidence of grade 3 or 4 intraventricular hemorrhage,11 and
there was not a significant difference in either the Swedish trial12 or the
3-center trial.15Our study was
compa-rable, in that no differences in the out-comes of intraventricular hemorrhage and/or periventricular leukomalacia were found.
A significant effect of NIDCAP on mod-erate/severe chronic lung disease was found in the Cochrane review.11In our
study, although the control group re-quired more postnatal corticosteroid treatment than did the NIDCAP group, there was no difference in the inci-dence of bronchopulmonary dysplasia.
Total days of intervention were less than in previous NIDCAP trials, which is a limitation of our study, because this would affect the number of days on which NIDCAP developmental care would be given. When we compared the number of days of intensive care and the total days of hospitalization, the infants in our study required fewer days of intensive care and were trans-ferred to regional hospitals earlier; therefore, the number of days of inter-60
50 40
30 20
10 0
100
80
60
40
20
0
Percentage
Total days respiratory support
80 60
40 20
0 100
80
60
40
20
0
Percent
a
ge
Total days respiratory support
Intervention-censored Control-censored Intervention Control
Control/intervention group
Intervention-censored Control-censored Intervention Control
Control/intervention group
A
B
FIGURE 3
vention was, for a proportion of our participating infants, smaller than in previously reported studies. Because of the regionalization of neonatal in-tensive care in the Dutch neonatal health care system, infants often are transferred to regional hospitals that can provide postintensive care and in-termediate care. Thirty-three (41%) of 80 surviving infants in the control group and 37 (51%) of 73 surviving in-fants in the NIDCAP group remained in the participating hospitals for ⱖ6 weeks. Because of this variation, we did correct for the number of days of intervention, but this did not change the term age outcomes.
This study is, to our knowledge, the largest RCT examining the effects of NIDCAP developmental care on pre-term infants. All except 2 of the surviv-ing 153 infants were seen at follow-up evaluations at term age. The infants were assigned randomly in an appro-priate manner; however, there could
be no blinding of the intervention, be-cause all infants were cared for in the same unit and the NIDCAP-treated in-fants had recommendations for care-giving at their bedside. The amount of respiratory support given to an infant was decided on by several neonatolo-gists and was not influenced by the study group in which the infant partic-ipated. Discharge from the NICU was based on 2 criteria, that is, the infant required no mechanical ventilation and/or CPAP therapy for 24 hours and weighed ⱖ1000 g; therefore, days of intensive care also could not be influenced by group participa-tion. Follow-up evaluations at term age were conducted by neonatolo-gists blinded to the participation group.
Despite the large sample size, com-pared with previous NIDCAP studies, and well-defined outcome measure-ments, as well as the addressing of methodologic concerns identified in
ⱖ1 trial,21 we were not able to find
any significant differences in our pri-mary outcomes. Future research on NIDCAP should include not only neo-natal intensive care centers but also the regional hospitals to which in-fants are transferred.
ACKNOWLEDGMENTS
This study was funded by the Nether-lands Organisation for Health
Re-search and Development (grant
2100.0072) and the Health Care Effi-ciency Research Fund of the Leiden University Medical Center.
We thank Sylvia M. van der Pal, PhD, Monique Rijken, MD, PhD, Shirley Mar-tens, MD, and Monique de Haan, MD, and the NIDCAP nurses (Annemieke de Waal, Thayla Halfwerk, Thea van Enge-lenberg, Karima Balarbi, Els van Veldhuijzen, and Hanneke Entrop) for their contribution to this research project.
REFERENCES
1. Hack M, Fanaroff AA. Outcomes of children of extremely low birthweight and gestational age in the 1990s.Semin Neonatol.2000;5(2):89 –106
2. Stoelhorst GM, Rijken M, Martens SE, et al. Changes in neonatology: comparison of two cohorts of very preterm infants (gestational age⬍32 weeks): the Project on Preterm and Small for Gesta-tional Age Infants 1983 and the Leiden Follow-Up Project on Prematurity 1996 –1997.Pediatrics.
2005;115(2):396 – 405
3. Horbar JD, Badger GJ, Carpenter JH, et al. Trends in mortality and morbidity for very low birth weight infants, 1991–1999.Pediatrics.2002;110(1):143–151
4. Blanco F, Suresh G, Howard D, Soll RF. Ensuring accurate knowledge of prematurity outcomes for prenatal counseling.Pediatrics.2005;115(4). Available at: www.pediatrics.org/cgi/content/full/ 115/4/e478
5. Botting N, Powls A, Cooke RW, Marlow N. Attention deficit hyperactivity disorders and other psychiatric outcomes in very low birthweight children at 12 years.J Child Psychol Psychiatry.
1997;38(8):931–941
6. Als H.Manual for the Naturalistic Observation of the Newborn (Preterm and Full term). 3rd rev. Boston, MA: Children’s Hospital, 1995
7. Jacobs SE, Sokol J, Ohlsson A. The Newborn Individualized Developmental Care and Assessment Program is not supported by meta-analyses of the data.J Pediatr.2002;140(6):699 –706 8. Maguire CM, Veen S, Sprij AJ, et al. Effects of basic developmental care on neonatal morbidity,
neuromotor development, and growth at term age of infants who were born at⬍32 weeks.
Pediatrics.2008;121(2). Available at: www.pediatrics.org/cgi/content/full/121/2/e239
9. Prechtl HFR.The Neurological Examination of the Full-Term Newborn Infant. Philadelphia, PA: Lippincott; 1977
10. Benders MJNL, Van Bel F, Van de Bor M. Cardiac output and ductal reopening during phototherapy in preterm infants.Acta Paediatr.1999;88(9):1014 –1019
12. Westrup B, Kleberg A, von Eichwald K, Stjernqvist K, Lagercrantz H. A randomized, controlled trial to evaluate the effects of the Newborn Individualized Developmental Care and Assessment Pro-gram in a Swedish setting.Pediatrics.2000;105(1):66 –72
13. Als H, Lawhon G, Duffy FH, McAnulty GB, Gibes-Grossman R, Blickman JG. Individualized develop-mental care for the very low-birth-weight preterm infant: medical and neurofunctional effects.
JAMA.1994;272(11):853– 858
14. Fleisher BE, VandenBerg K, Constantinou J, et al. Individualized developmental care for very-low-birth-weight premature infants.Clin Pediatr (Phila).1995;34(10):523–529
15. Als H, Gilkerson L, Duffy FH, et al. A three-center, randomized, controlled trial of individualized developmental care for very low birth weight preterm infants: medical, neurodevelopmental, parenting, and caregiving effects.J Dev Behav Pediatr.2003;24(6):399 – 408
16. International Neonatal Network. The CRIB (Clinical Risk Index for Babies) score: a tool for assess-ing initial neonatal risk and comparassess-ing performance of neonatal intensive care units.Lancet.
1993;342(8865):193–198
17. Wielenga J, Smit B, Merkus M, Kok J. Individualized developmental care in a Dutch NICU: short-term clinical outcome.Acta Paediatr.2007;96(10):1409 –1415
18. Als H, Duffy FH, McAnulty GB, et al. Early experience alters brain function and structure.Pediatrics.
2004;113(4):846 – 857
19. Buehler DM, Als H, Duffy FH, McAnulty GB, Liederman J. Effectiveness of individualized develop-mental care for low-risk preterm infants: behavioral and electrophysiologic evidence.Pediatrics.
1995;96(5):923–932
20. Als H, Lawhon G, Brown E, et al. Individualized behavioral and environmental care for the very low birth weight preterm infant at high risk for bronchopulmonary dysplasia: neonatal intensive care unit and developmental outcome.Pediatrics.1986;78(6):1123–1132
21. Ohlsson A, Jacobs SE. Meta-regression can indicate if further NIDCAP studies are justified [in Swedish].Lakartidningen.2007;104(3):134 –137
22. Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in pre-mature infants: prediction from oxygen requirement in the neonatal period.Pediatrics.1988; 82(4):527–532
23. Volpe JJ.Neurology of the Newborn. 4th ed. Philadelphia, PA: Saunders; 2001
DOI: 10.1542/peds.2008-1881 originally published online September 28, 2009;
2009;124;1021
Pediatrics
and Sylvia Veen
Celeste M. Maguire, Frans J. Walther, Arwen J. Sprij, Saskia Le Cessie, Jan M. Wit
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/4/1021
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/4/1021#BIBL
This article cites 17 articles, 7 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2008-1881 originally published online September 28, 2009;
2009;124;1021
Pediatrics
and Sylvia Veen
Celeste M. Maguire, Frans J. Walther, Arwen J. Sprij, Saskia Le Cessie, Jan M. Wit
Infants <32 Weeks
Effects of Individualized Developmental Care in a Randomized Trial of Preterm
http://pediatrics.aappublications.org/content/124/4/1021
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.