BIOEQUIVALENCE OF MICRONUTRIENT POWDERS TO CONVENTIONAL FORTIFICATION ON ZINC STATUS OF CHILDREN AGED 6-36 MONTHS IN
THIKA INFORMAL SETTLEMENTS, KENYA
JULIANA N. KIIO
(BSC. FOOD SC., MSC. FOOD TECH, PGD. FOOD SC. & NUTRITION) (H87/10719/08)
DEPARTMENT OF FOOD, NUTRITION AND DIETETICS
A RESEARCH THESIS SUBMITTED IN PARTIAL FULFILLMENT FOR THE
DEGREE OF DOCTOR OF PHILOSOPHY IN THE SCHOOL OF APPLIED HUMAN SCIENCES OF KENYATTA UNIVERSITY
Declaration
This is my original work and has not been presented for a degree in any University for any award
Signature _____________________________ Date _________________________ Juliana N. Kiio (Bsc. Food Science & Technology, MSc. Food Technology, PgD. Food Science and Nutrition) Reg. No. (H87/10719/08) Department of Food, Nutrition and Dietetics
Kenyatta University
Supervisors:
This thesis has been submitted for review with our approval as University Supervisors: Signature _____________________________ Date _________________________
Sophie Ochola (B.Ed Home Economics; MSc. Applied Human Nutrition; PhD, Nutritional Sciences)
Department of Food, Nutrition and Dietetics Kenyatta University
Signature _____________________________ Date _________________________ Prof. Ruth Nduati (MBChB; MMed; MPH)
Department of Paediatrics and Child Health University of Nairobi
Signature _____________________________ Date __________________________ Prof. Elizabeth Kuria (B.Ed Home Economics; PgD. Food Science and Nutrition; MSc.Education, Home Economics; PhD, Education)
TABLE OF CONTENT
Declaration ... ii
TABLE OF CONTENT ... iii
LIST OF APPENDICES ... viii
LIST OF TABLES ... x
LIST OF FIGURES ... xii
DEDICATION ... xiii
ACKNOWLEDGEMENT ... xiv
LIST OF ABBREVIATIONS AND ACRONYMS ... xv
1.10 Definitions of terms ... xix
1.11 Operational definitions of terms ... xx
ABSTRACT ... xxiii
CHAPTER ONE: INTRODUCTION ... 1
1.0 Background to the study ... 1
1.1 Problem statement and justification of the study ... 5
1.2 Purpose of the study ... 8
1.3 Study objectives ... 8
1.4 Hypotheses ... 9
1.5 Significance of the study ... 10
1.6 Assumptions ... 10
1.7 Conceptual framework ... 10
CHAPTER TWO: LITERATURE REVIEW ... 13
2.0 Role of Zn in human health ... 13
2.1 Biological functions of Zn ... 13
2.1.1. Effect of Zn deficiency on linear Growth ... 13
2.1.2 Effect of Zn deficiency on immunity ... 14
2.1.3 Effect of Zn deficiency on appetite ... 17
2.2 Manifestation of Zn deficiency ... 17
2.2.1 Manifestation of Zn deficiency among young children ... 17
2.3 Global estimates and trends of malnutrition, Zn deficiency and mortality among
children underfive years of age in Kenya ... 19
2.4 Factors associated with Zn status among children aged 6-36 months ... 23
2.4.1 Dietary intake and poor feeding practices ... 23
2.4.2 Infections, diarrhoea and other disease states ... 25
2.4.3 Age and increased growth requirements ... 26
2.4.4 Socio-emographic and socio-economic status factors ... 26
2.5 Urban slum population and malnutrition levels ... 28
2.6 Recommended strategies to alleviate Zn deficiency ... 30
2.7. Effect of Zn fortification on serum levels, growth velocity, morbidity and appetite outcomes among moderately malnourished children ... 32
2.8 Multiple micronutrient interventions ... 34
2.9 CSB and MNPs for the management of moderately malnourished children ... 35
2.10 Safety of micronutrient powders ... 37
2.11 Methods of assessing Zn status ... 38
2.12 Bioequivalence studies... 39
2.13 Occurrence, sources and bioavailability of Zn in foods ... 40
2.13.1. Inhibitors of Zn absorption ... 41
2.13.2 Zn absorption enhancers ... 43
2.13.3 Physiological status and total intakes affect bioavailability of Zn ... 44
2.13.4 Micronutrient interactions and bioavailability of Zn ... 44
2.14 Zn absorption, transport and homeostasis ... 45
2.15 Zn requirements in normal and malnourished children ... 46
2.16 The Recommended Daily Intake, Tolerable Upper Intake Levels and adverse effects of Zn intake ... 46
2.17 Summary of literature review ... 47
CHAPTER THREE: METHODOLOGY ... 49
3.0 Overview ... 49
Phase I: In vitro bioaccessibility of zinc and iron ... 49
3.1. Food samples and sample preparation ... 50
3.3 Determination of the tannin content by colorimetric analysis ... 51
3.4 Determination of phytate content in the selected cereal, legume and tuber flours by HPLC method ... 53
3.5 Determination of the total Zn and iron concentration of fortified porridges ... 54
3.6 Determination of the in vitro bio-accessibility of Zn and iron in porridge preparations ... 55
3.7 Determination of phytic acid/Zn and phytic acid/iron molar ratios ... 56
3.8 Quality control and validity ... 57
3.9 Pilot study ... 58
3.9.1 Findings of the pilot study ... 58
3.10 Phase II: Intervention study ... 59
3.10.1 Study design ... 60
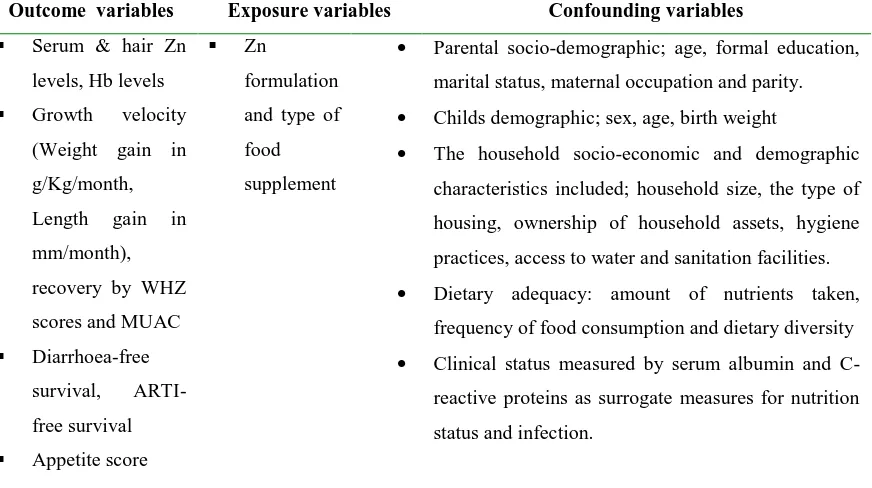
3.10.2 Study variables ... 60
3.10.3 Study area... 61
3.10.4 Target population ... 62
3.10.5 Sample size determination ... 64
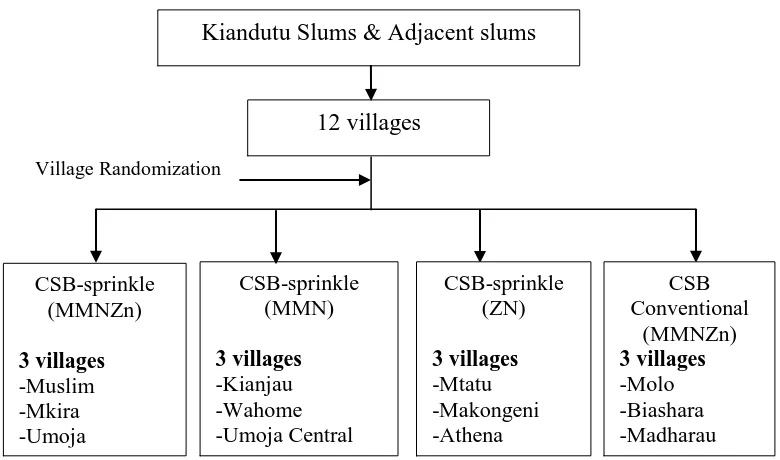
3.10.6 Sampling frame and randomization ... 65
3.10.7 Blinding... 66
3.10.8 Community mobilization ... 67
3.10.9 Recruitment of study participants ... 68
3.10.10 Household survey and baseline data collection ... 71
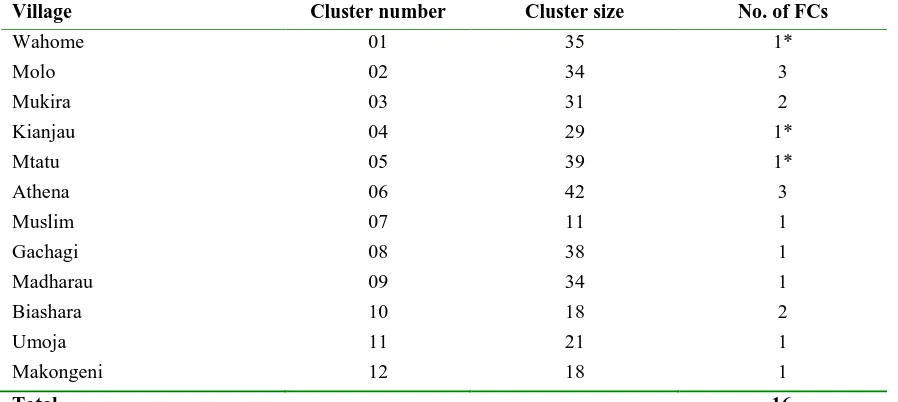
3.10.11 Establishment of feeding centres ... 71
3.10.12 Description of the intervention ... 72
3.10.13 Study groups ... 73
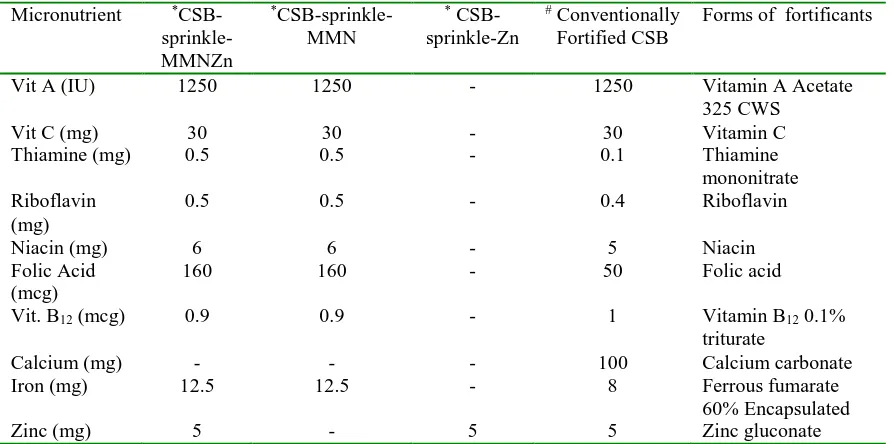
3.10.14 Porridge preparation in the feeding centres, standardization of preparation procedures and feeding of the study children ... 75
3.10.15 Follow-up procedures ... 77
3.10.16 Data collection tools and procedures ... 80
3.10.17 Validity and reliability of the tools ... 83
3.10.18 Clinical procedures ... 84
3.10.20 Sample collection ... 87
3.10.21 Laboratory methods ... 88
3.10.22 Data management and data analyses... 91
3.10.23 Ethical considerations ... 98
CHAPTER FOUR: RESULTS ... 100
I. FINDINGS OF THE IN VITRO BIOAVAILABILITY STUDY ... 100
4.1 Moisture content ... 100
4.2 Tannin content ... 100
4.3 Phytate (PA) content ... 100
4.4 Total and in vitro bio-accessible Zn and iron in CSB and other staples ... 102
4.4.1 Total Zn and iron content ... 102
4.4.2 In vitro soluble Zn and iron fractions ... 103
4.4.3 Phytate: mineral molar ratios and iron:Zn molar ratios ... 104
4.4.4 Association between anti-nutrient content and mineral bio-accessibility ... 104
II. FINDINGS OF THE RANDOMIZED TRIAL ... 107
4.5 Enrolment of study subjects ... 107
FINDINGS AT BASELINE ... 109
4.6 Study population ... 109
4.6.1 Socio-demographic characteristics and socio-economic status ... 109
4.6.2 Zn status and nutrition status of the study population ... 111
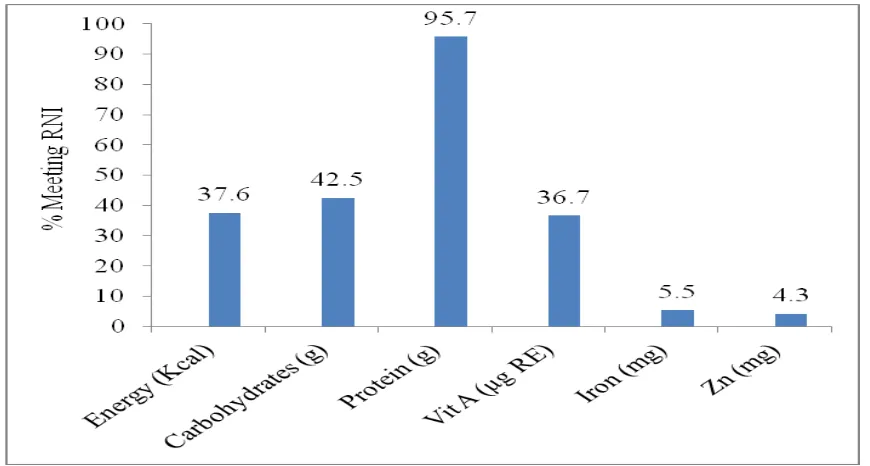
4.6.3 Dietary intake of energy, protein, Zn, iron and vitamin A ... 114
4.6.4 Meal frequency and dietary diversity of the children ... 115
4.6.5 Appetite, morbidity, Vitamin A supplementation and health seeking behaviour .. 116
4.6.6 Access to water and sanitation facilities and hygiene practices ... 118
4.7 Comparison of the study groups at baseline ... 120
4.8 Baseline comparison of children who completed the study and those lost to follow-up ... 124
4.9 Completeness of data collection ... 126
4.10 Compliance of the study groups to the intervention ... 126
4.11 Trends in dietary intake of selected nutrients during the intervention period ... 127
4.12 Adverse effects... 131
EFFECTS OF THE MNP AND CONVENTIONAL FORTIFICATION ON ZN STATUS, MORBIDITY, GROWTH VELOCITY AND APPETITE ... 131
4.13 The effect of MNP and conventional Zn-fortification of CSB on serum Zn levels 131 4.14 Bioequivalence of micronutrient sprinklestm to CSB on the serum Zn levels ... 134
4.15 The effect of MNP and conventional Zn-fortification on hair Zn levels ... 136
4.16 The effect of MNP and conventional Zn-fortification on growth velocity ... 137
4.16.1 The effect of MNP and conventional Zn-fortification on weight gain ... 137
4.16.2 The effect of MNP and conventional Zn-fortification on height gain ... 138
4.16.3 The effect of MNP and conventional Zn-fortification on nutritional recovery ... 138
4.17 The effect of MNP and conventional Zn-fortification on morbidity ... 141
4.18 The effect of MNP and conventional Zn-fortification on appetite ... 143
III.FACTORS ASSOCIATED WITH ZN STATUS ... 145
4.19 Socio-demographic, morbidity, dietary and biochemical factors ... 145
CHAPTER FIVE: DISCUSSION ... 149
5.1 Anti-nutrients and bio-accessibility of Zn and Fe in CSB and other selected foods 149 5.2 Zn status of moderately malnourished children aged 6-36 months in Thika informal settlements... 152
5.3 The effect of the intervention on serum Zn status of moderately malnourished children ... 154
5.4 Bioequivalence of MNPs to conventional fortification on serum Zn levels of moderately malnourished children ... 155
5.5 The effect of the intervention on morbidity patterns of the children ... 156
5.6 The effect of the intervention on appetite of the children ... 157
5.7 The effect of the intervention on growth velocity of the children ... 157
5.8 Factors associated with Zn status among malnourished children aged 6-36 months in Thika informal settlements ... 159
5.8.1 Socio-demographic and socio-economic characteristics associated with Zn status ... 159
5.8.2 Association between nutrition status and Zn status ... 161
5.8.4 Association between appetite and Zn status ... 162
5.8.5 Association between morbidity and Zn status ... 162
5.8.6 Biochemical parameters associated with plasma Zn concentration ... 163
5.9 Predictors of Zn status ... 164
5.10 The strengths and limitations of the study ... 165
CHAPTER 6: SUMMARY, CONCLUSIONS AND RECOMMENDATIONS ... 167
6.0 Overview ... 167
6.1 Summary ... 167
6.2 Conclusions ... 169
6.3 Recommendations ... 172
6.3.1 Recommendations for policy ... 172
6.3.2 Recommendations for practice ... 173
6.3.3 Recommendations for further research ... 173
References ... 174
LIST OF APPENDICES Appendix A: Enrolment Informed Consent ... 206
Appendix B: Baseline questionnaires ... 209
Appendix C: Interviews at six months to assess the acceptability of micronutrient sprinklestm/CSB by the mothers ... 228
Appendix D: FGDs at six months to assess the caregivers’ knowledge on food fortification and the acceptability of micronutrient sprinklestm/CSB ... 231
Appendix E: Kiswahili translation of the study instruments ... 232
Appendix F: Research authorization from the National Commission for Science, Technology and Innovation (NACOSTI) ... 253
Appendix G-1: Ethical clearance ... 254
Appendix G-2: Ethical clearance (Renewal) ...………...256
Appendix H: Research authorization from Kenyatta University Graduate School ... .257
Appendix I: Research authorization from MoPHS ... 258
Appendix K: Research authorization from Ministry of State in the of Office of the
President ... 260
Appendix L: Course schedule for training research assistants in Kiandutu, Thika ... 261
Appendix M: Local calendar of events ... 263
Appendix N: Demonstration tool for micronutrient sprinkletm use ... 266
Appendix O: Baseline characteristics of study population (pilot study) ... 266
Appendix P: Baseline characteristics of study population (pilot study) ... 267
Appendix Q: Serum zinc levels and nutrition status after intervention by study group (pilot study) ... 267
LIST OF TABLES
Table 2.1 The odds ratio of mortality from diarrhoea or pneumonia in malnourished
children* (Source: Liu et al., 2012; Adapted from Black et al, 2008, pp 243–260) ... 22
Table 2.2 Global trends in deaths attributable to selected micronutrient deficiencies (Source: Lim et al., 2012) ... 23
Table 2.3 Content and bioavailability of Zn in selected foods (Source: IZiNCG, 2004) . 41 Table 2.4 Zn bioavailability in diets of varying anti-nutrient content (Source: Roohani et al., 2013) ... 42
Table 2.5 RDAand tolerable upper intake levels for Zn in children (Source: IOM, 2001) ... 47
Table 3.1 Outcome and exposure variables of the study ... 61
Table 3.2 Feeding centres by study groups ... 72
Table 3.3 Composition of micronutrient sprinklestm and conventionally fortified CSB by study groups ... 75
Table 3.4 Follow-up procedures and frequency of data collection ... 79
Table 3.5 Data analysis methods ... 98
Table 4.1 Anti-nutrient content and bio-accessibility of Zn and iron fortified (conventional or MNP) and unfortified other selected staplesdw ... 101
Table 4.2 The association between Zn and Fe bio-accessibility and the anti-nutrient content ... 105
Table 4.3 Socio-demographic and socio-economic status of study population ... 110
Table 4.4 Zn status and nutrition status of the study population ... 111
Table 4.5 Dietary intake of Zn and other selected nutrients ... 114
Table 4.6 Dietary diversity and meal frequency of study children ... 116
Table 4.7 Morbidity, health-seeking behaviour and access to water and sanitation facilities and hygiene practices (self reported behaviour) ... 119
Table 4.8 Socio-demographic and socio-economic characteristics by study groups... 121
Table 4.9 Nutrition status and Zn status by study groups ... 122
Table 4.10 Dietary practices by study groups ... 123
LIST OF FIGURES
Figure 1.1 Dietary and physiological factors affecting Zn status and functional outcomes
of malnourished children (Source: Author) ... 11
Figure 2.1 Trends in stunting, underweight and wasting among Kenyan children aged below 5 years (Source: Adapted from KDHS, 2014; UNICEF, 2011) ... 19
Figure 2.2 The estimated national risk of Zn deficiency (Source: Wessells & Brown, 2012) ... 21
Figure 2.3 Direct and indirect causes of malnutrition and micronutrient deficiencies (Adopted from Müller & Krawinkel, 2005) ... 27
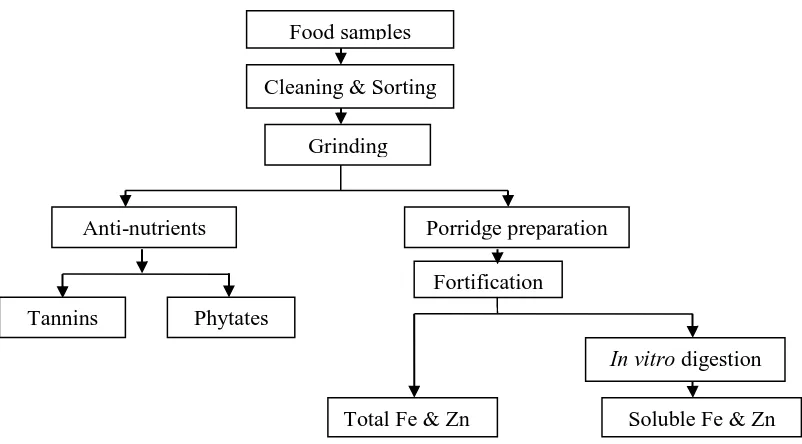
Figure 3.1 Flow chart on determination of anti-nutrient content and bio-accessibility of FE & Zn ... 49
Figure 3.2 Sampling frame and randomization of villages into study groups; MMNZn (Multiple micronutrients containing Zn), MMN (Multiple micronutrients without Zn), Zn (Zn only) ... 66
Figure 3.3 Flow chart describing the study protocols and intervention ... 76
Figure 3.4 Schematic diagram of the study design, intervention groups and follow-up .. 78
Figure 4.1 Trial profile on recruitment, treatment groups and completion rates ... 108
Figure 4.2 Dietary and other selected nutrients adequacy for Zn ... 115
Figure 4.3 Food Approach Scores (FAPP) ... 117
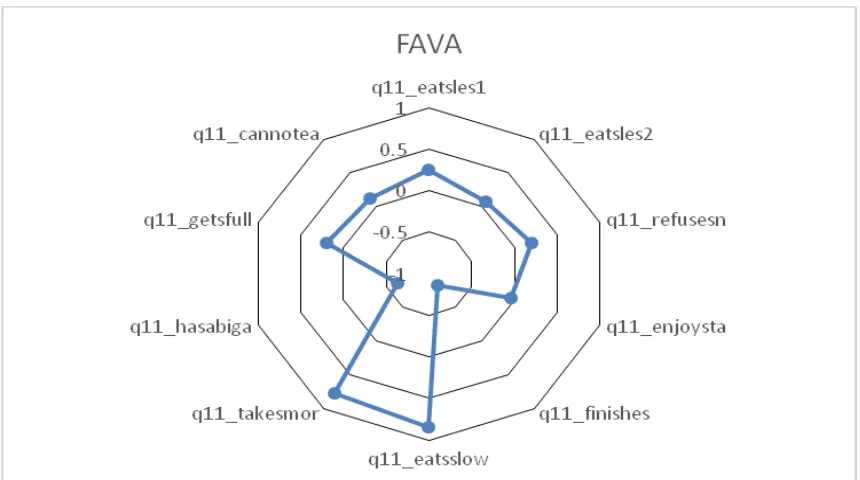
Figure 4.4 Food Avoidance Scores (FAVA) ... 117
Figure 4.5 Zn deficiency levels at baseline and end-of-intervention by study group ... 134
Figure 4.6 The bioequivalence margin of the micronutrient formulations ... 135
Figure 4.7 Kaplan Meier survival curve on recovery from wasting by WHZ scores ... 139
Figure 4.8 Kaplan Meier survival curve on recovery by MUAC ... 140
Figure 4.9 Kaplan Meier survival analysis on diarrhoea-free survival ... 141
DEDICATION
ACKNOWLEDGEMENT
LIST OF ABBREVIATIONS AND ACRONYMS
AAS Atomic Absorption Spectrophotometer
ACF Action Contre la Faim Action (Action Against Hunger)
ANOVA Analysis of Variance
AOAC Association of Official Analytical Chemists
AOR Adjusted Odds Ratio
APHRC African Population and Health Research Center ARTI Acute Respiratory Tract Infections
BMS Between Cluster Mean Square (ANOVA)
CAS Combined Appetite Score
CDC Centers for Disease Control and Prevention CEBQ Children's Eating Behaviour Questionnaire
CF Complementary Foods
CHEW Community Health Extension Worker
CHW Community Health Worker
CI Confidence Intervals
CO Clinical Officer
CRP C-Reactive Proteins
CSB Corn-Soy Blend
CV Coefficient of Variation
DD Desire to Drink
DDS Dietary Diversity Score
DEFF Design Effect
DNA Deoxyribonucleic Acid
DPHK Development Partners in Health Kenya DPHO District Public Health Officer
DW Dry Weight
EF Enjoyment of Food
EMEA European Medicines Agency
EOE Emotional Over-eating
FAO Food and Agricultural Organization
FC Feeding Centre
FDA Food and Drug Administration
Fe Iron
FF Food Fussiness
FFQ Food Frequency Questionnaire
FGD Focus Group Discussion
FNB Food and Nutrition Board (US)
FR Food Responsiveness
GAIN Global Alliance for Improved Nutrition
GAM Global Acute Malnutrition
GH Growth Hormone
GOK Government of Kenya
GP Group
HAZ Height-for-Age Z-scores
Hb Haemoglobin
HC Health Centre
HDL High Density Lipoproteins
HF-TAG Home Fortification Technical Advisory Group HINIs High Impact Nutrition Interventions
HPLC High Performance liquid Chromatography
HR Hazard Ratios
ICC Intra-cluster Correlation Coefficient IGF-1 Insulin-like Growth Factor
ITT Intention To Treat
IOM Institute of Medicine (United States of America) IYCF Infant and Young Child Feeding
KNBS Kenya National Bureau of Statistics
LBW Low Birth Weight
MC Moisture Content
MDG Millennium Development Goals
MM Moderately Malnourished
MMF Minimum Food Frequency
MMN Multiple Micronutrients
MMNZn Multiple Micronutrients containing Zinc
MN Micronutrients
MNP Micronutrient Powder
MoE Ministry of Education
MoH Ministry of Health
MoPHS Ministry of Public Health and Sanitation
MUAC Mid-Upper Arm Circumference
NACOSTI National Commission for Science, Technology and Innovation NCHS National Centre for Health Statistics
NGO Non-Governmental Organizations
OECD Organization for Economic Co-operation and Development
OR Odds Ratio
PA Phytic Acid
PCA Principal Component Analysis
PCGs Primary Care Givers
RA Research Assistant
RCT Randomize Controlled Trials
RDA Recommended Daily Allowance
RID Refractive Index Detector
RNI Recommended Nutrient Intake
SCUK Save the Children UK
SDG Sustainable Development Goals
SE Slowness in Eating
SFP Supplementary Feeding Programmes SPSS Statistical Package for Social Science
SR Satiety Responsiveness
SUN Scaling Up Nutrition
UK United Kingdom
ULs Tolerable Upper Intake Levels
UN-DESA United Nations Department of Economic and Social Affairs UNICEF United Nations Children Education Fund
USA United States of America
WASH Water, Hygiene and Sanitation
WAZ Weight-for-Age Z-scores
WFP World Food Programme
WHO World Health Organization
WHZ Weight-for-Height Z-scores
WMS Within Cluster Mean Square (ANOVA)
ZIP Zrt-, Irt-like Proteins
Zn Zinc
Definitions of terms
Bioaccessibility is defined as the quantity or fraction of a nutrient which is released from the food matrix in the gastro-intestinal tract and becomes available for absorption (Heaney, 2001).
Bioavailability refers to the fraction of nutrient intake that can be absorbed into the blood system and used for physiologic functions of the body (Krebs, 2001).
Bioequivalence is the absence of a greater-than-allowable difference between systemic bioavailability of a test product and that of a reference product (WHO & FAO, 2006).
Diarrhoea is defined as three or more loose or watery stools that would take the shape of the container in a 24-hour period as reported in a two-week recall (WHO, 2013).
Efficacy is defined as the performance of an intervention under ideal and controlled circumstances (Revicki & Frank, 1999).
Home fortification refers to addition of micronutrients (dry powder) to cooked food just before eating, usually administered once each day (Zlotkin et al., 2005).
Reference product: A product used as a comparator in a clinical trial (WHO & FAO, 2006).
Sprinklestm are microencapsulated, tasteless, colourless, multiple-micronutrient fortificant, provided in single-dose sachets, for use at home on a daily basis to improve the nutritional value of young children’s foods (Zlotkin et al., 2005).
Zinc deficiency: Serum zinc levels <65 µg/dL for non-fasting blood samples (IZiNCG et al., 2004).
Operational definitions of terms
Acceptability in this study referred to the overall liking of the intervention product by the children as reported by the mother on assessing the response of the child in consuming the intervention product. Acceptability by mothers was defined as continued consumption of the product during the intervention and intention to use after the intervention completion, even when micronutrient sprinklestm were added to other foods.
Acute respiratory tract infections (ARTIs) in this study referred to any respiratory illness that incorporated at least one of the upper or lower respiratory tract symptom as reported by a caregiver and/or observed by study personnel in the two weeks preceding the day of data collection. The symptoms included cough, cough with fast or difficulty breathing, cold or running nose, sore throat or otitis media.
Adherence or Compliance referred to the proportion of days fortified product was consumed by the children to the total recommended number of intervention days as assessed using daily attendance and consumption registers. An adherence level of 80% of the intervention days was considered adequate.
Control group in this study referred to the study group which was randomized to the standard protocol of managing moderately malnourished group using conventionally fortified Corn-Soy-Blend.
Bioequivalence in this study was used to refer to the effect of the MNPs on improving serum zinc status within the ±20% range compared to the comparator product (conventionally fortified CSB).
Efficacy referred to impact assessment within a trial in a controlled study set-up to ensure that the outcomes are attributable to the intervention; controlled treatments such as standardized treatments, blinding, adherence monitoring and homogenous study population achieved through randomized design (RCT).
Episode of ARTI and fever a new episode was defined as the presence of symptoms separated by seven or more days.
Episode of diarrhoea a new episode was defined as a period of diarrhoea separated by two or more diarrhoea-free days.
In vitro bio-accessibility in this study referred to the proportion of nutrient solubilized
from a food product after subjecting it to in vitro enzyme digestion mimicking the human gastro-intestinal tract which is the first basic step before assimilation.
Micronutrient Powders (MNPs) was defined as any form of micronutrients pre-packaged in a sachet to be sprinkled in to food products at the time and point-of-consumption.
Minimum dietary diversity referred to the minimum number of four or more food groups consumed by the child both at home and out of the home in the 24-hr period.
Minimum meal frequency referred to the minimum number of meals including meals and snacks consumed in a 24-hr period .
Moderately malnourished children in this study refers to a children with a Mid-Upper Arm Circumference (MUAC) within the range of ≥115-<125 mm without bilateral oedema.
Multiple micronutrients (MMN) in this study refer to a mixture containing three or more micronutrients.
Sampling cluster in this study refers to pre-existing villages in the study area whose boundaries were identified using the local village elders.
ABSTRACT
CHAPTER ONE: INTRODUCTION
1.0 Background to the study
The global mortality of children aged below five years has been on a declining trend. Sub-Saharan Africa however, remains as the region with the highest child mortality rates in the world with one in every twelve children dying before their fifth birthday (UNICEF, 2015). Kenya has made slow progress in reducing childhood deaths (UNICEF, 2015) but has not achieved the Millennium Development Goal (MDG) four of reducing the rate of under-five mortality by two-thirds by the year 2015 (UNICEF, 2015). Undernutrition accounts for nearly half of deaths among children, either directly or indirectly (Black et al., 2013). In developing countries, malnutrition underlies 53% of the deaths associated with infectious disease among children aged below five years (Benguigui & Stein, 2006; Rodriguez, Cervantes, & Ortiz, 2011). Many studies have demonstrated increasing case-fatality rate with worsening nutritional status. This association of malnutrition with increased incidence of illness and death is often referred to as the vicious cycle of malnutrition and disease (Jones, Thitiri, Ngari, & Berkley, 2014).
intake, further exacerbating the vicious cycle (Sunguya, 2006). Growth faltering in children therefore is mainly due to sub-optimal dietary intake of nutrients, mal-absorption and/or gastro-intestinal losses due to infections (Rodriguez et al., 2011). The alarming observation is that, three quarters of the children who die from causes related to malnutrition are only mildly or moderately undernourished (UNICEF, 2007).
Zn is an essential micronutrient for growth and development, appetite, immunity, anti-oxidative protection and reproduction (Katona & Katona-Apte, 2008; McCall, Huang, & Fierke, 2000). The physiological outcomes may be compromised in depleted individuals. Sub-optimal dietary intake is the main cause of Zn deficiency with an estimated 17% of the world’s population consuming diets with inadequate amounts of bio-available Zn (Wessells & Brown, 2012). Typical diets in developing countries mainly consist of starchy staples; cereals, tubers and legumes which have low levels of bio-available Zn. The foods richest in Zn are from animal sources, but these are not often included in children diets because of limited availability, unaffordability, entrenched custom, religion or cost. Plant sources of Zn contain high levels of phytic acid, a potent inhibitor of Zn absorption (Davidsson, Ziegler, Kastenmayer, van Dael, & Barclay, 2004; Wessells & Brown, 2012). As a result, the content and the amount of Zn available for absorption from such diets are low, and probably the primary cause of Zn deficiency.
growth may extend beyond 23 months (Lundeen et al., 2014; Prentice et al., 2013). The current study therefore targeted moderately malnourished children aged 6-36 months.
The key strategies to prevent Zn deficiency are micronutrient supplementation, bio-fortification or bio-fortification of local foods and dietary diversification (IZiNCG, 2009). Food fortification has been a top development agenda to curb “hidden hunger” which continues to prevail in many developing countries. Current science suggests that, combining strategies provides the most efficacious method of preventing micronutrient deficiency (Bhutta, Salam, & Das, 2013). Fortification is a cost effective food-based approach when targeting large populations. Food fortification at the household level is a preferred approach where large segments of the populations at risk lack ready access to centrally processed foods (HF-TAG, 2013). Target groups with a high nutrient requirement may fail to meet their needs from a centrally fortified food.
the impact of other micronutrients included in the multiple micronutrient mixes particularly Zn. A study carried out in Western Kenya demonstrated that home fortification is acceptable to mothers and effective in reducing Iron Deficiency Anaemia (IDA) among children aged below five years (Suchdev et al., 2012). MNPs have been recommended as one of the High Impact Nutrition Interventions (HINIs) and the WHO (2011b) guidelines recommend the use of MNPs as a public health intervention. In 2010, the Kenyan Government adopted distribution and use of MNPs and subsequently, the Scaling-Up Nutrition (SUN) movement of the Ministry of Health (MoH) has also adopted the MNPs to ensure country wide coverage (MoPHS, 2012b).
1.1 Problem statement and justification of the study
children affected in urban slum populations therefore warrants the management of moderate malnutrition to be made a public health priority.
The current study was carried out in Kiandutu slums in Thika Town and other neighbouring slum areas of Makongeni, Umoja, Madharau and Gachagi. According to the Centre for Urban Research and Innovations (CURI) report, Kiandutu is one of the largest slums in Kiambu County (CURI, 2012). The slum is characterized by poor infrastructure, poor sanitation, overcrowding, unemployment and food insecurity (Njoroge & Kibunga, 2007). There was no previous documented evidence on the prevalence of malnutrition in this slum, but all the factors known to aggravate vulnerability of the children were present, making this an ideal setting for testing the efficacy of community level fortification of Zn among young children.
The management of moderately malnourished children is based on improving the existing diets or by the provision of supplementary food products such as fortified blended foods. Diets of children from resource poor setting lack diversification and are mainly derived from cereal-based complementary foods with poor Zn bioavailability (Samuel, Egal, Oldewage-Theron, Napier, & Venter, 2010) and hence the dietary approach of management may not be effective. Corn-Soya-Blend (CSB) is the standard food for rehabilitation of moderately malnourished children (De Pee & Bloem, 2009). A major limitation of CSB however, is the poor bioavailability of micronutrients due to its high level of anti-nutrient content (Wood & Sibanda-Mulder, 2011). The anti-nutrients form complexes with Zn, iron and other minerals resulting to poor bioavailability (Hurrell & Egli, 2010; Hurrell, 2004). Iron interacts with Zn and may affect the bioavailability in fortified foods (Hurrell & Egli, 2010). The poor bioavailability has driven researchers into finding alternative supplementary products for managing moderate acute malnutrition. Home fortification of supplementary food products may be a better approach of improving the micronutrient bioavailability in the supplementary foods. The anti-nutrient content and the in vitro bioavailability of Zn and iron in selected foods fortified using either micronutrient sprinklestm or conventional fortification were investigated.
lacking. An information gap also exists on the effect of Zn fortification of supplementary food products on the appetite and morbidity outcomes of malnourished children. The current study was therefore designed to investigate the relative efficacy of micronutrient sprinklestm compared to the conventionally fortified CSB in improving the serum Zn levels among moderately malnourished children aged 6-36 months. Appetite, growth velocity and morbidity patterns of the children were also assessed.
1.2 Purpose of the study
This study investigated the bioequivalence of micronutrient sprinklestm compared to conventionally fortified CSB on the serum Zn status among moderately malnourished children aged 6-36 months.
1.3 Study objectives
The study objectives were to:
1. Compare the anti-nutrient content of CSB and other selected local complementary feeding flours.
2. Establish the in vitro bio-accessibility of Zn and iron in micronutrient sprinkled CSB and the local porridges as compared to the conventionally fortified CSB. 3. Assess the socio-demographic characteristics, dietary practices, nutritional status,
appetite and morbidity patterns of moderately malnourished children aged 6-36 months in Thika informal settlements.
4. Assess the serum and hair Zn status of moderately malnourished children aged 6-36 months in Thika informal settlements pre- and post-intervention.
fortified CSB on serum Zn levels, growth velocity, appetite and morbidity patterns of moderately malnourished children aged 6-36 months.
6. Establish the bioequivalence of MNPs to conventionally fortified CSB on the serum Zn levels of moderately malnourished children aged 6-36 months in Thika informal settlements within ±20% limit.
7. Establish the predictors of Zn status among malnourished children aged 6-36 months in Thika informal settlements.
1.4 Hypotheses
Ho1: No significant difference between MNPs and conventionally fortified CSB on the in vitro bio-accessibility of Zn.
Ho2: No significant difference between MNPs and conventionally fortified CSB in improving serum Zn levels of moderately malnourished children within the ± 20% bioequivalence limit.
Ho3: Serum Zn levels of moderately malnourished children do not respond significantly different to Zn fortification of CSB using either MNPor conventional fortification.
Ho4: Growth velocity in moderately malnourished children does not respond significantly different to Zn fortification of CSB using either MNPor conventional fortification.
Ho5: The appetite of moderately malnourished children does not respond significantly different to Zn fortification of CSB using either MNPor conventional fortification.
1.5 Significance of the study
Home fortification strategies to prevent micronutrient deficiencies have been newly adopted in Kenya. The findings of the current study demonstrate the potential for home fortification in improving the Zn status of moderately malnourished children. This information may be useful to governments, MoH and health sector partners to formulate policy dealing with fortified blended foods in the management of moderately malnourished children. The findings will also provide information on Zn status and nutritional recovery of the malnourished which may be useful in designing and implementation of programmes. It may also be useful to industries and regulatory bodies dealing with food fortification in considering the food processing technologies in favor of improved micronutrient bioavailability considering the recommended safe levels of fortification.
1.6 Assumptions
The current study assumed that Zn intake of the study population was mainly derived from diet with a limited contribution from breastfeeding.
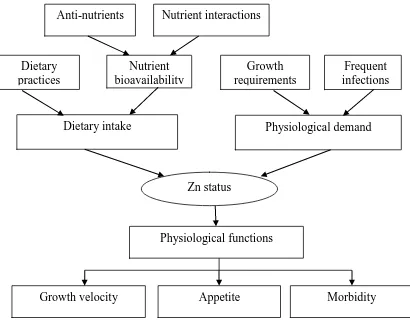
1.7 Conceptual framework
and limited bioavailability of Zn in plant foods because of presence of anti-nutrients mainly phytates and polyphenolic compounds such as tannins.
The interaction of Zn with other nutrients contained in multiple micronutrient formulations such as iron also affects the bioavailability. Utilization of Zn is impaired in the presence of infection as decreased circulation of Zn reduces the availability of Zn to the tissues. Disease states such as persistent diarrhoea and worm infestation have been implicated in causing Zn loss through the gastro-intestinal tract.
Figure 0.1 Dietary and physiological factors affecting Zn status and functional outcomes of malnourished children (Source: Author)
Morbidity Dietary intake
Frequent infections
Physiological demand
Physiological functions Growth requirements Dietary
practices
Appetite Growth velocity
Nutrient bioavailability
CHAPTER TWO: LITERATURE REVIEW
2.0 Role of Zn in human health
2.1 Biological functions of Zn
Zn is an essential micronutrient playing a key role in human health. The biological role of Zn is categorized into three general functional classes; catalytic, structural and regulatory. The structural role of Zn is stabilization of the tertiary and quaternary structure of proteins (Andreini, Bertini, & Cavallaro, 2011). Zn is found in all biologic systems and its biological functions associated with proteins with more than 300 enzymes requiring Zn for catalytic functions (IOM, 2001; McCall et al., 2000). Zn-mediated signaling in some proteins plays a regulatory function. Zn affects a multiple physiologic and metabolic functions, such as physical growth (Brown, Peerson, Rivera, & Allen, 2002; Maret & Sandstead, 2006), immuno-competence (Fraker & King, 2004; Rink & Gabriel, 2000), reproductive, neuro-behavioral (Gibson et al., 2006), anti-oxidative (Powell, 2000) and sensory development (Heyneman, 1996; Shay & Mangian, 2000). There is a renewed interest in the contribution of Zn to human health with a focus on growth, appetite.and immune-protection among young children.
2.1.1. Effect of Zn deficiency on linear Growth
supplementation enhances growth among growth-restricted (stunted or underweight) children. More recent publications are less emphatic about this relationship and state that Zn supplementation may help to improve linear growth of children below five years of age (Imdad & Bhutta, 2011). Therefore, research is needed to demonstrate the effect of Zn fortification among malnourished children.
The mechanism of Zn in promoting linear growth has not been clearly understood. However, this may be explained by the essential role played by Zn in bone metabolism and DNA synthesis. Linear growth is controlled by growth hormone (GH) and insulin-like growth factor I (IGF-I) (Ahmed & Farquharson, 2010). Zn deficiency has been associated with decreased levels of both IGF-I plasma concentration and GH receptors, consequently impairing linear growth (Porto et al., 2011). Despite there being several studies on Zn supplementation, there is conflicting information on the response of Zn fortification either alone or in MMN on growth outcomes of malnourished children.
2.1.2 Effect of Zn deficiency on immunity
deficiency are therefore associated with increased morbidity. The mechanism for immune-protection is not fully elucidated leading to different hypotheses.
Zn deficiency reduces the number of B and T lymphocytes through increased cell death and also reduces their functionality (King, Osati-Ashtiani, & Fraker, 2002; Prasad, 2007). This would then have an effect on both the humoral and cell mediated immunity, the two key arms of the immune system. During growth and development, Zn plays a role in thymic development further affecting the production and maturation of B and T lymphocytes. Malnutrition results into permanent reductions in thymus size which can persist till the child is one year of age (McCall et al., 2000; Palmer, 2011). Maternal Zn deficiency is also contributory and is linked to intra-uterine growth retardation leading to decreased cellular immunity lasting several years (Uriu-Adams & Keen, 2010).
Positive response to Zn supplementation on infectious diseases has been demonstrated. Daily Zn supplementation reduced the hazard rate of diarrhoea by 24% diarrhoea among rural Tanzanian children aged 6–60 months with height-for-age z-score below –1.5 SD (Veenemans et al., 2012). A systematic review and meta-analysis on the effectiveness of Zn supplementation for treating diarrhoea among malnourished children showed a reduction in diarrhoea duration by 33.17 hours (95% CI = –38.55 to –27.79) (Galvao, Thees, Pontes, Silva, & Pereira, 2013). Zn supplementation is also effective in the treatment of respiratory tract infections. A 2-month Zn supplementation of young children resulted to a significant reduction in the episodes of acute lower respiratory infections reported over a 6-month period (Shah et al., 2013b). Among malnourished Ecuadorian children, the incidence of cough (RR: 0.52, 95% CI 0.32-0.84, p = 0.004) and upper respiratory tract secretions (RR: 0.72, 95% CI. = 0.59-0.88, p = 0.001) was significantly lower in the Zn supplemented group compared to the non-supplemented group following a 60-day Zn supplementation (Sempertegui et al., 1996).
2.1.3 Effect of Zn deficiency on appetite
Several researchers have demonstrated that Zn deficiency is characterized by loss of taste (ageusia), decrease taste acuity (hypogeusia) and decreased olfactory sensitivity (hyposmia) which is associated with abnormal taste (dysgeusia) (Atkin-Thor, Goddard, O’Nion, Stephen, & Kolff, 1978; Khademian et al., 2014; Umeta, West, Haidar, Deurenberg, & Hautvast, 2000). The production of gustin which is a Zn-containing protein of the parotid salivary gland and functions in the growth and nutrition of taste buds, is depressed in times of Zn deficiency (Henkin, Martin, & Agarwal, 1999; Padiglia et al., 2010; Wharton, 2000). There is limited scientific evidence on the effect of Zn fortification on the appetite of malnourished children. A Zn supplementation study among malnourished Ethiopian children resulted in reduced anorexia (Umeta et al., 2000) and improved taste acuity (Campos et al., 2004; Shakur, Bano, Malek, Kundu, & Ahmed, 2009). The current study sought to establish the appetite of malnourished children and the responsiveness of appetite to Zn fortification.
2.2 Manifestation of Zn deficiency
2.2.1 Manifestation of Zn deficiency in young children
nutrient deficiencies and childhood illnesses, making it challenging to diagnose mild to moderate forms of Zn deficiency (Brown, Peerson, Baker, & Hess, 2009; de Benoist et al., 2007).
2.2.2. Zn deficiency and manifestation among malnourished children
Malnourished children are usually Zn deficient and further Zn depletion occurs due to feacal losses as a result of frequent diarrhoea (Guerrant, DeBoer, Moore, Scharf & Lima, 2012). Zn is a limiting micronutrient in children recovering from malnutrition (Imdad & Bhutta, 2011; Umeta et al., 2000) and Zn deficiency among malnourished children contributes to growth failure and susceptibility to infections (Katona & Katona-Apte, 2008). Several researchers demonstrated that impaired immunity, skin lesions and poor wound healing, diarrhoea, anorexia are among the clinical features of Zn deficiency in children with severe malnutrition (Qasemzadeh et al., 2014; Shakur, Malek, Bano, Rahman, & Ahmed, 2009; Singla, Chand, Kumar, & Kachhawaha, 1996). A clear relationship between the presence of clinical signs and low plasma Zn concentration has been demonstrated (Wessells, King, & Brown, 2014).
of morbidity and mortality (Malina, Bouchard, & Bar-Or, 2004). There is limited information on Zn status of malnourished children and its relationship with the morbidity, nutrition status and appetite.
2.3 Global estimates and trends of malnutrition, Zn deficiency and mortality among children underfive years of age in Kenya
Global estimates indicate that 165 million children underfive years of age are stunted and 52 million are wasted (Black et al., 2013). According to Black and others, undernutrition plays a major role in mortality levels and has been blamed for 45% of all deaths among the children. Figure 2.1 show the malnutrition trends in Kenya. The findings of the latest Kenyan Demographic Health Survey (KDHS) shows that the malnutrition levels are still high; wasting (4%), stunting (26%) and underweight (11%) (KDHS, 2014).
Despite the reduction in wasting and stunting, Kenya has not achieved the MDG targets. With the reduction in the prevalence of underweight however, one of the indicators for MDG 1 was achieved. Other associated factors are; food insecurity, poor infant and young child feeding practices, poor access to water and sanitation services and poor hygiene practices and high morbidity as well (Shrimpton & Saldanha, 2011).
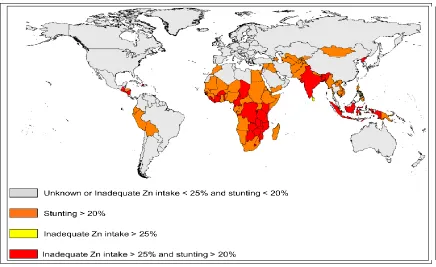
Figure 0.2 The estimated national risk of Zn deficiency (Source: Wessells & Brown, 2012)
and diarrhoea (Black, 2014), which significantly increases their risk of mortality (MoPHS & SCUK, 2011).
Table 0.1 The odds ratio of mortality from diarrhoea or pneumonia in malnourished children* (Source: Liu et al., 2012; Adapted from Black et al, 2008, pp 243–260)
Odds ratio (95% CI) Severe
undernutrition
Moderate Undernutrition
Mild
undernutrition
No
undernutrition
Underweight
Diarrhoea 9.5 (5.5-16.5) 3.4 (2.7-4.4) 2.1 (1.6-2.7) 1.0
Pneumonia 6.4 (3.9-10.4) 1.3 (0.9-2.0) 1.2 (0.7-1.9) 1.0
Stunting
Diarrhoea 4.6 (2.7-8.1) 1.6 (1.1-2.5) 1.2 (0.9-1.7) 1.0
Pneumonia 3.2 (1.5-6.7) 1.3 (0.8-2.1) 1.0 (0.6-1.6) 1.0
Wasting
Diarrhoea 6.3 (2.7-14.7) 2.9 (1.8-4.5) 1.2 (0.7-1.9) 1.0
Pneumonia 8.7 (4.8-15.6) 4.2 (3.2-5.5) 1.6 (1.1-2.4) 1.0
*Bangladesh, Ghana, Guinea-Bissau, India, Nepal, Pakistan, the Philippines and Senegal
Table 0.2 Global trends in deaths attributable to selected micronutrient deficiencies (Source: Lim et al., 2012)
Micronutrie nt status
Deaths Disease burden (1000 DALYs)
1990 2010 1990 2010
Iron deficiency
168 084
(130 444-197 085)
119 608
(93 261-139 985)
51 841
(37 477 -71 202)
48 225
(33 769-67 592)
Vitamin A deficiency
349 354
(170 504-632149)
119 762
(61 723-191 846)
30 288
(14 884-54 488)
10 770 (5 625-17 149)
Zn deficiency
275 590
(51 274-529 451)
97 330
(17 575-190 527)
24 375 (5 385-45 685)
9 136
(2 458-16 903)
2.4 Factors associated with Zn status among children aged 6-36 months
2.4.1 Dietary intake and poor feeding practices
Orun, Yalcin, Aykut, Orhan and Morgil (2012) who reported low levels of Zn in breast milk at the second month of lactation. A recent isotopic study also revealed that, less than 25% of the total absorbed Zn comes from breast milk in 9-month old breastfed infants (Krebs et al., 2012).
Sub-optimal complementary feeding practices have been observed to be the main cause of Zn deficiency in young children. A review by Dewey (2013) demonstrated that it remains a big challenge to meet the nutrient needs of young children during the complementary feeding period due to the sub-optimal feeding practices. According to Umeta et al. (2000), poor infant and young feeding practices such as earlier or delayed initiation of complementary foods before and after six months of age respectively and diets of poor bioavailability exposes the children at an increased risk of Zn deficiency. Animal products are rarely fed to young children due to availability, poor access, high costs, taboos and customs (Krebs et al., 2006; Krebs, et al., 2012; Krebs, et al., 2012).
complementary foods of low Zn bioavailability raises concerns about the Zn status of children aged 6-36 months in developing countries. The current study therefore, established the phytate and tannin levels (being the main anti-nutrients in plant foods) in CSB and other local foods. The in vitro bioavailability of Zn in the fortified porridges prepared from conventionally fortified CSB or CSB fortified at the point of consumption using MNPs was also determined.
A report by Golden (2009) demonstrated that inadequate Zn intake by malnourished children may be a limiting factor for growth. There is scarcity of information on Zn intake and the bioavailability of Zn in the locally consumed complementary foods and supplementary food products. Information on the Zn bioavailability and efficacy of fortified blended foods recommended for malnourished children on improving the Zn status is also lacking. Studies on bioavailability of Zn in complementary foods fortified with MNPs are biased for iron but few studies have evaluated the bioavalability of Zn. Information is also lacking on whether the recommended fortification levels are effective enough especially in fortified blended foods with high anti-nutrients levels targeted for supplementation of malnourished children. The dietary intake of Zn among moderately malnourished children aged 6-36 months in Thika informal settlements was assessed in the current study.
2.4.2 Infections, diarrhoea and other disease states
reported that diarrhoea and other conditions that alter the gastro-intestinal absorption promote Zn losses (Manary et al., 2010). Zinc deficiency is also associated with other chronic conditions such as liver and renal diseases, sickle cell disease, diabetes and cancer (Prasad, 1993; Zemel, Kawchak, Fung, Ohene-Frempong, & Stallings, 2002), digestive disorders and acrodermatitis enteropathica (Dufner-Beattie et al., 2007). The current study investigated the association between Zn deficiency and morbidity.
2.4.3 Age and increased growth requirements
Zn is essential for growth and development. Children are vulnerable to Zn deficiency during periods of rapid growth and development. The vulnerability is higher among premature and low-birth-weight babies, and pre-schoolers and more specifically those aged 6-23 months. Substantial evidence shows that, failure to address malnutrition among children below two years of age, the consequences on growth and development may be irreversible and hence the so called “window of opportunity” (Levinson & Bassett, 2007; Victora et al., 2010; World Bank, 2010). Therefore, it is critical that suitable interventions implemented at the critical age in programme targeting.
2.4.4 Socio-emographic and socio-economic status factors
Kimiywe, Chianu, Mbithe, & Sanginga, 2007; Sachs & McArthur, 2005; Thomas & Frankenberg, 2002).
Figure 0.3 Direct and indirect causes of malnutrition and micronutrient deficiencies (Adopted from Müller & Krawinkel, 2005)
The WHO estimated that 85% of the two billion people suffering from micronutrient deficiencies live in resource poor settings (WHO, 2000) and that multiple micronutrient deficiencies are usually reported in these populations (Abu-Saad & Fraser, 2010). Poor households are at a risk of undernutrition because of food and nutritional insecurity (Peña & Bacallao, 2002; World Bank, 2010). According to the reports, lack of resources for food purchase or production, low levels of education and nutritional health information and poor access and utilization of healthcare are some of the underlying causes of malnutrition and micronutrient deficiencies. The food security situation has been
Malnutrition Marasmus, Kwashiorkor, micronutrient deficiencies
Insufficient supply of protein,
energy or micronutrients Severe or frequent
infection; diarrhoea
Ill health, unhealthy environment Insufficient child and
maternal care Insufficient household food
security
War, natural disasters, civil disorder Low socio-economic status
and low education of women
worsening due to unfavourable trends of soaring food prices, economic depression and climate change, thus increasing the vulnerability of urban poor. Insufficient caregiving behaviour is also contributory to poor the nutrition status of children (Wachs, 2008). Zn deficiency is prevalent among children from resource poor settings (Cole et al., 2010). A report by UNICEF and Development Partners in Health Kenya (DPHK) has emphasized the need to address the underlying causes of child undernutrition (UNICEF & DPHK, 2009). Due to the complexity of the underlying factors and the absence of single and simple solutions however, governments and partners in developing countries tend to focus on the effects of malnutrition and even more on those already malnourished rather than on the causes of malnutrition. Population specific information on the determinants of malnutrition and micronutrient deficiencies among vulnerable groups in Kenya is lacking. Identifying factors associated with Zn deficiency among malnourished populations can be useful in selecting priority areas for targeting and designing Zn intervention programmes. The current study therefore, sought to assess the dietary, morbidity, biochemical and socio-economic and demographic factors associated with Zn status among moderately malnourished children in Thika informal settlements.
2.5 Urban slum population and malnutrition levels
Kenya has gradually increased to 7% with an expected increase in slum population (UN HABITAT, 2010). The ever increasing population, coupled with rural-urban migration has contributed to growing urban slums amidst the limited resources, unemployment, poor infrastructure and insufficient affordable housing (Cohen, 2004). Urban slums are usually insecure, densely populated and characterized by poor hygiene, poor access to water and sanitation facilities, overcrowding, poor housing with inadequate ventilation resulting to rampant disease outbreaks. Children living in slum environments are therefore at an increased risk of malnutrition, morbidity and mortality. A report by the APHRC (2002) further showed that, the nutrition and health outcomes of children to the urban poor are poorer compared their rural counterparts. Other researchers have reported similar findings (Fotso et al., 2012; Olack et al., 2014; UNICEF, 2012).
in urban slum settings, the design of effective programs and interventions may be quite different from rural areas and emergency settings.
Undernutrition has a role to play in a country’s socio-economic development and the potential to reduce poverty. Undernutrition also increases mortality from diarrhoea, pneumonia, malaria and other infections affecting the achievement of MDG 4 of reducing child mortality. Undernutrition affects cognitive development in children, school enrolment, school drop-out rates and educational attainments (ACC/SCN, 2004; Amuyunzu-Nyamongo & Taffa, 2004; FAO, 2005). This study therefore, designed a food supplementation programme targeting malnourished children in an urban slum setting.
2.6 Recommended strategies to alleviate Zn deficiency
Food-based approaches provide a long-term strategy for improving nutrition (Allen, 2008) and hence should be embraced. Dietary diversification or modification is usually a sustainable long-term strategy for improving the intake of bioavailable Zn and other micronutrients. Dietary modification of diets however, involves changing the dietary habits which is difficult to achieve hence rendering it ineffective. Poverty and food insecurity further renders foods with high levels of Zn bioavailability inaccessible as these foods are usually expensive and unaffordable to households in resource-poor settings (Macharia-Mutie et al., 2010; Roohani, Hurrell, Kelishadi, & Schulin, 2013). Due to the limitations of dietary modification and supplementation approaches, fortification of foods is a top agenda to ensure adequate intake of micronutrients (WHO/UNICEF, 2008).
Fortification is a food based approach which is cost-effective when targeting large populations. Food fortification increases the levels of the total absorbable Zn (López de Romaña et al., 2005). Households from resource-poor settings however, may not afford the centrally fortified foods. On the other hand, the quantity of the fortified food consumed by young children may not cater for their recommended daily intakes (WHO & FAO, 2006). Targeted food fortification programmes for young children are therefore recommended (de Benoist et al., 2007).
underfive years of age using home fortification is supported by substantial evidence there is information gap on the effect of MNPs on Zn status. According to Zlotkin et al. (2006), MNPs provide a low bioavailability form of Zn, yet providing adequate amounts of absorbable Zn in young children. There is conflicting information however, on the effectiveness of MNPs on improving serum Zn levels and other Zn-related functional outcomes (Adu-Afarwuah et al., 2008; IZiNCG, 2009; Zlotkin et al., 2003). The conflicting results may be partly due to the choice of food fortification channels, the age and Zn status of study populations (IZiNCG, 2009). The efficacy of MNPs in improving the micronutrient status of malnourished children has not been demonstrated.
2.7. Effect of Zn fortification on serum levels, growth velocity, morbidity and
appetite outcomes among moderately malnourished children
growth when Zn is supplemented alone than when in multiple micronutrient formulations.
In a systematic review, Ramakrishnan et al. (2009) reported that, several supplementation studies administering iron-Zn combinations found no improvements in child growth but resulted in improved iron and Zn status. The review also highlighted that, although there was no positive response in growth, other benefits such as reduced morbidity and mortality may be realized. Therapeutic Zn supplementation has shown to be effective in reducing the severity and duration of diarrhoea (Mayo-Wilson, Imdad, Junior, Dean, & Bhutta, 2014). Despite the recognized role of Zn in immune-protection, Brown, Romaña, Arsenault, Peerson and Penny (2007) did not find evidence for Zn fortification in improving the morbidity outcomes of diarrhoea and respiratory tract infections. Evidence of Zn fortification on reducing diarrhoeal morbidity among malnourished children is however scarce. Zn supplementation studies conducted by Umeta et al. (2000) and Khademian et al. (2014) reported improved appetite among children. Evidence of Zn fortification on appetite among malnourished children who are likely to be anorexic is lacking.
improving the Zn status of children and the associated functional outcomes of growth, appetite and morbidity. Additionally, the MNPs are designed for individuals who obtain adequate amounts of the macronutrients of energy, protein and fat in the diet. Information lacks on the potential benefits in undernourished and micronutrient-deficient populations. There is need to establish the efficacy of MNPs on the management of micronutrient deficiencies among malnourished children.
The interaction of the micronutrients in the MNP formulation however, has not been fully understood given that the micronutrients are added at the point of consumption in comparison to the conventionally fortified food. The research findings of Choudhury, Aimone, Hyder and Zlotkin (2012) indicate possible effects of micro-encapsulation, micronutrient interactions and food matrix on iron bioavailability. The evidence for the efficacy of Zn fortification in the multiple micronutrient formulations warrants further investigation because of the potential negative interaction among multiple micronutrients which possibly limits their absorption and utilization and hence the associated outcomes.
2.8 Multiple micronutrient interventions
Scientific evidence shows that multiple micronutrient interventions have a proven efficacy on biological outcomes (Allen, Peerson, & Olney, 2009; Habicht & Pelto, 2012).
Providing multiple micronutrient formulations are more beneficial and cost effective than single nutrient interventions (Ramakrishnan & Huffman, 2001; Semba, 2012). The prevention of multiple micronutrient malnutrition is a key factor in the realization of SDGs, given the important effects of micronutrients on child health and survival. Currently, there is a growing interest of including Zn into other micronutrient formulations containing iron, vitamin A, folic acid and iodine in fortification intervention programs due to its recognized importance in health (Brown, Hambidge, & Ranum, 2010). There is conflicting information on the effect of fortification of Zn alone or in MMN formation on growth, appetite and morbidity outcomes (IZiNCG, 2009). The current study investigated the efficacy of fortifying food with Zn alone or when included in a multi-micronutrient mix containing iron, vitamin A and other micronutrients on the serum Zn levels.
2.9 CSB and MNPs for the management of moderately malnourished children
research efforts are therefore geared towards improving CSB composition or developing substitutes for supplementary feeding programmes.
Micronutrient powders (MNPs) are single-dose packets of dry powder containing lipid-encapsulated iron among other micronutrients. MNPs were first developed in the last decade at the Hospital for Sick Children in Toronto, Canada. MNPs are sprinkled into any semi-solid food immediately before consumption to enhance the micronutrient level (Zlotkin et al., 2005). The lipid-encapsulation protects the iron from dissolving into the food hence preventing undesirable change in colour, flavour or taste usually associated with other forms of conventional iron fortification or supplementation. Home fortification refers to the strategy where micronutrients are added to the commonly eaten, prepared food just before consumption. The WHO (2011a) guidelines have recommended the use of MNPs as one of the High Impact Nutrition Interventions (HINIs).
Community based studies conducted in Bangladesh, Ghana and Kenya demonstrated acceptability of MNPs by mothers (Dewey, Yang, & Boy, 2009; Jefferds et al., 2010; Rah et al., 2011). The addition of MNP at the point of consumption may favour micronutrient bioavailability compared to the conventional fortification as the food matrix effects may be minimized. To the knowledge of the researcher however, no studies have demonstrated the effect of Zn fortification using MNPs on the Zn status and the functional outcomes of growth, appetite and morbidity among moderately malnourished children. This study assessed the bioequivalence of micronutrient sprinklestm to conventionally fortified CSB in improving the Zn status of moderately malnourished children.
2.10 Safety of micronutrient powders
2.11 Methods of assessing Zn status
Simple, quantitative biomarkers that can be used to identify Zn deficiency at the individual level are lacking. The IZiNCG however recommends serum or plasma Zn as the biomarker of the Zn status in populations (IZiNCG et al., 2004). This is because serum Zn levels have been shown to correlate with dietary Zn intake and respond to Zn supplementation interventions (de Benoist et al., 2007; Hess, Lönnerdal, Hotz, Rivera, & Brown, 2009). Serum Zn concentration is however affected by factors such as age, sex, stress, infection and fasting status (Shah, Sachdev, Gera, De-Regil, & Pena-Rosas, 2013). Biomarkers of the acute phase response should be assessed and consequently considered in the interpretation of results (IZiNCG et al., 2004). Zn is mainly transported in plasma bound to albumin. As a result, protein-energy malnutrition and liver conditions that lead to hypoalbuminaemia (Chowdhury, Akhter, Haque, Aziz, & Nahar, 2008) result in lower serum Zn concentrations (Shakur et al., 2009; Wessells & Brown, 2012). Hair Zn, alkaline phosphatase and erythrocyte Zn have also been proposed as possible biomarkers. However, their reliability has not been proven to date. Hair Zn not affected by inflammation, stress, fasting status and is an indicator of chronic Zn deficiency and may be a preferred indicator. Based on the poor reliability of serum Zn as a biomarker of Zn deficiency, hair Zn was used to validate the observed serum Zn levels in the current study.
Zn and is widely used in most health and nutrition monitoring activities due to which it has been recommended as a functional marker of Zn status (de Benoist et al., 2007; Imdad & Bhutta, 2011). Assessing the Zn status of undernourished populations is critical in designing intervention programmes. The current study assessed the serum and hair Zn levels and the functional outcomes of growth velocity, appetite and frequency of infections in response to Zn fortification.
2.12 Bioequivalence studies
substance. The test conditions should be standardised in order to minimise the variability of all factors involved except that of the products being tested (EMEA, 2010). Parallel design was adopted for the current study to investigate the Zn status during the nutrition recovery of the children over a period of six months.
2.13 Occurrence, sources and bioavailability of Zn in foods
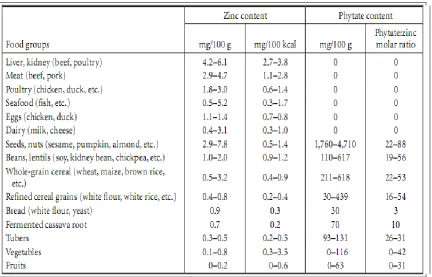
The content and bioavailability of Zn in foods is widely varied. Zn content is higher in foods of animal origin compared to plant-based foods. Foods such as organ meat, beef, pork, poultry, fish and shellfish are among the rich sources of Zn (Krebs et al., 2006; Krebs, Westcott, et al., 2012). Among the plant-based foods, Zn content is relatively higher in nuts, seeds, legumes and whole-grain cereals and lower in tubers, fruits and vegetables (Mann & Truswell, 2012). Bioavailability is defined as the fraction of nutrient taken which is absorbable into the human body and is further utilized for physiologic functions. Bio-accessibility refers to the solubilization of nutrients under enteric conditions before absorption and is an important step determining bioavailability. Bioavailability of Zn is high in animal based diets and limited in diets rich in plant sources.
2.13.1. Inhibitors of Zn absorption
Phytic acid and tannins are the main inhibitors of Zn absorption. Phytic acid (myo-inositol-6-phosphate) is an anti-nutrient abundant in unrefined cereals, legumes, tubers and oil seeds. Among the anti-nutrients, phytic acid is the most important inhibitor of Zn absorption (Hemalatha, Platel, & Srinivasan, 2006; Ramírez-Cárdenas, Leonel, Costa, & Reis, 2010). It forms complexes with Zn, calcium and iron and causes the formation of insoluble salts of the minerals resulting in poor bioavailability (Abebe et al., 2007; Baye, Mouquet-Rivier, Icard-Vernière, Rochette, & Guyot, 2013; Lönnerdal, 2000).
Table 0.3 Content and bioavailability of Zn in selected foods (Source: IZiNCG, 2004)