Original Article
Serum miR-125a-5p, miR-145 and miR-146a as
diagnostic biomarkers in non-small cell lung cancer
Rui-Juan Wang1,3*, Yan-Hua Zheng2*, Ping Wang3, Jian-Zhong Zhang1,4
1Chinese PLA General Hospital/Chinese PLA Medical School, Beijing 100853, China; 2Department of Special
Medical Center, 306 Hospital of PLA, Beijing 100101, China; 3Department of Respiratory Medicine, 306 Hospital
of PLA, Beijing 100101, China; 4Department of Pathology, 306 Hospital of PLA, Beijing 100101, China. *Equal
contributors.
Received November 5, 2014; Accepted December 23, 2014; Epub January 1, 2015; Published January 15, 2015
Abstract: Background: Lung cancer is becoming the leading cause of cancer-related deaths with high mortality worldwide and in China as well. Non-small-cell lung cancer (NSCLC) is the most common type of lung cancer ac-counting for approximately 85% of all cases. Over 70% of cases are at loco-regionally advanced stages or have distant metastasis at the time of presentation with subsequently poor prognosis. MiRNAs are stable molecules in blood and used as biomarkers for the early diagnosis of various malignancy. The purpose of this study was to evalu-ate whether circulating miR-125a-5p, miR-145 and miR-146a could be used as biomarkers for the diagnosis of NSCLC through measuring their expression and assess their relationship with clinical pathological factors. Methods: Expression levels of serum miR-125a-5p, miR-145 and miR-146a were detected in 70 pairs of NSCLC patients and healthy controls using quantitative real-time PCR analysis. Results: Serum miR-125a-5p, miR-145 and miR-146a were overexpressed in NSCLC patients compared with healthy controls. Their values of the area under the receiver –
operating characteristic curve (AUC-ROC) were 0.71, 0.84 and 0.78. Optimal sensitivity and specificity were 73.53%
and 55.71%, 92.75% and 61.43%, 84.06% and 58.57%, respectively in differentiating NSCLC patients from healthy controls. Conclusions: These preliminary data suggest that serum miR-125a-5p, miR-145 and miR-146a may be useful noninvasive biomarkers for the clinical diagnosis of NSCLC.
Keywords: MicroRNAs, non-small cell lung cancer, serum, diagnosis
Introduction
Lung cancer is becoming the leading cause of cancer-related deaths with high mortality worldwide [1] and in China [2] as well. Non-small-cell lung cancer (NSCLC) is the most com-mon type of lung cancer accounting for approxi-mately 85% of all cases, which is subdivided into three major types: adenocarcinoma (ADC), squamous-cell carcinoma (SCC) and large-cell carcinoma (LCC) [3, 4]. Over 70% of cases are at loco-regionally advanced stages or have distant metastasis at the time of presenta- tion with subsequently poor prognosis [5]. Additionally for the intrinsic resistance and recurrence, the survival rate for NSCLC still remains at low level, including early-stage group. The overall 5-year survival rate is only 17.1% in the United States [6]. It is urgent to explore the pathogenesis and identify more effective biomarkers, especially using
noninva-NSCLC as early as possible and develop effec-tive individualized treatment programs to improve the quality of life and survival.
patients and control subjects are summarized in Table 1.
Total RNA extraction
Total RNA was isolated from 300 μl serum specimens of patients and controls by using miRNA isolation Kit (Applied Biosystems, Foster City, CA, USA) according to the manufacturer’s protocol. RNA concentration was measured using Nanodrop 2100. Then the RNA samples were preserved at -80°C for use. Repeated freeze-thawing was avoided to ensure the qual-ity of the samples during storage,
Quantitative reverse transcription-PCR (qRT-PCR)
TaqMan MicroRNA Kit (Applied Biosystems)
was used to perform the expression profiling of
serum miRNA of all patients and controls. All reagents, primers and probes were also bought from Applied Biosystems. The cDNA reverse
transcription was first carried out according
to the manufacture’s instruction. The 15 μl reverse transcription reaction system
consist-ed of 0.15 μl of dNTPs mix (100 mM total), 1.0 μl of reverse transcriptase (50 U/μl), 1.5 μl of RT Buffer (10×), 0.19 μl of RNase inhibitor (20
U/μl), 4.16 μl of nuclease free water, 3.0 μl of
gene-specific miRNA primer and 5 μl of RNA extract sample. For synthesis of cDNA, reaction conditions of upper mixtures were: incubated at 16°C for 30 min, at 42°C for 30 min, at 85°C for 5 min, and at 4°C for any length of time. Then cDNA was amplified. The 20 μl qRT-PCR system contained: 1.0 μl of TaqMan Small RNA
Assay (20×), 1.33 μl of cDNA solution, 10 μl of TaqMan Universal PCR Master Mix (2×) and 7.67 μl of nuclease free water. Quantitative PCR were performed on Applied Biosystems lung cancer cells by regulating several
down-stream genes involved in EGFR signaling path-way [11], restoration of miR-145 can inhibit cancer cell growth in EGFR mutant lung adeno-carcinoma [12] and miR-146a can target EGFR and its downstream gene with potential
func-tional significance in lung cancer [13]. These
conclusions from above-mentioned studies were drawn in vitro or detecting tissue samples aiming at one single miRNA. Recently circulat-ing miR-145 and miR-146a were found to be overexpressed in breast cancer and might be used for detection of breast cancer [14, 15]. In the present study we performed the miRNAs
expression profiling in NSCLC serum compared
with healthy controls using quantitative RT-PCR and constructed the receiver operating charac-teristic (ROC) curves in order to identify
wheth-er specific miRNAs could discriminate between
NSCLC patients and healthy controls. Material and methods
Patients and samples
Seventy cases were collected from primary NSCLC patients who were diagnosed by histol-ogy or cytolhistol-ogy from March 2013 to May 2014 in our hospital. Histological diagnoses were independently formulated by two pathologists.
Disease stage classifications were determined
according to the world health organization
(WHO) classification and the international asso -ciation for the study of lung cancer staging sys-tem [3, 4]. Clinic pathological characteristics were collected whenever available for all the patients. Peripheral blood samples were col-lected before they received any anticancer treatment, including surgery, chemotherapy, radiotherapy and hormonal treatment, etc. 70
samples from healthy individuals with same age and gender were also collected. Blood samples (3.5 ml) were drawn from subjects using tubes without anticoagu-lant. These samples were processed by centrifugation at 3500 g for 5 minutes at room temperature. Serum was
trans-ferred into RNA-free EP tube every 500 μl
[image:2.612.91.329.96.230.2]aliquot and stored at -80°C before RNA extraction. This study was approved by the Ethics Committee of 306 Hospital of PLA. All specimens were collected after obtaining the patients’ informed con-sents. The characteristics with respect to age, gender and smoking status of NSCLC Table 1. Clinical characteristics of 70 NSCLC patients
and 70 healthy individuals
Patients Individuals P-value Age (years), median 64.41 ± 10.77 63.74 ± 10.32 0.7189
≥ 60 48 46
< 60 22 24
Gender 1.0000
Male 43 43
Female 27 27
Smoking status 0.1756
Yes 37 29
serum miRNAs and clinic pathological factors of NSCLC patients. P-value < 0.05 was defined as statistical significance.
Results
Patient characteristics
There were 43 males and 27 females among the 70 NSCLC patients, including 48 ADCs, 20 SCCs and 2 LCCs. The mean age and gender distribution were similar between the NSCLC patients and the healthy controls. Smoking rate was higher in NSCLC patients than that in con-trols but without statistical difference (P = 0.1756).
Serum miRNAs expression in NSCLC patients and healthy controls
The serum level of miR-125a-5p, miR-145 and miR-146a were compared between the two 7500 Real Time PCR system (Applied
Biosystems) and the reaction conditions were: 10 min at 95°C, and 40 cycles of 95°C for 15 sec and 60°C for 60 sec. All qRT-PCR assays were undertaken in duplicate, using miR-39 as the internal reference gene to normalize the sample-to-sample variation during the RNA iso-lation procedure. The fold change of gene rela-tive expression was calculated by using the equation of comparative cycle threshold (2-ΔΔCt) method.
Statistical analysis
Statistical analysis was performed with SPSS 17.0 statistical software (SPSS, Inc., Chicago, IL, USA) and graphs were generated using Graphpad Prism 6.0. Two-tailed unpaired t-test was used to evaluate the differential expres-sion of serum miRNA level between NSCLC patients and normal controls. Receiver
operat-ing characteristic (ROC) curves were generated to assess the diagnostic accuracy of each serum miRNA, and the area under the ROC curve (AUC) were used to assess the
sensi-tivity and specificity. Chi-squared
[image:3.612.92.525.69.378.2]test was used to assess the correla-tion between the expression level of Figure 1. Serum expression levels of miR-125a-5p, miR-145 and miR-146a in healthy controls and NSCLCs.
Table 2. AUC ROC values of different miRNAs in NSCLC patients
miRNA AUC ROC 95% CI Cut-off Sensitivity Specificity
[image:3.612.91.351.411.466.2]groups. As shown in Figure 1, the expression of
all three miRNAs was significantly higher in
NSCLC patients than that in healthy controls (P
< 0.0001).
Serum miRNAs as diagnosis signatures for NSCLCs
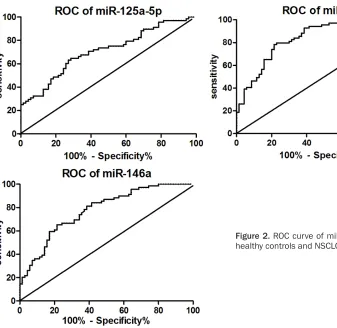
The ROC curve was plotted to identify a cut-off value that could distinguish NSCLCs from healthy controls. Analysis revealed that the area under the ROC curves (AUC) for serum
miR-125a-5p was 0.71 (95% confidence inter -val 0.62-0.79). At an optimal cut-off -value of
1.41, the sensitivity and specificity was 73.53%
and 55.71%, respectively. Similarly, for miR-145 and miR-146a, results were shown in Table 2 and Figure 2.
Correlation between miRNAs expression levels and clinic pathological factors
The correlation between these three miRNAs expression levels and various clinic pathologi-cal factors was examined. These factors includ-ed gender, age, smoking status, lymph node
metastasis and TNM stage. NSCLC patients were divided into miRNA high and low groups according to the median fold-change values.
There were no significant associations between
the analyzed miRNAs and the main clinic patho-logical characteristics of the NSCLC patients. Nevertheless, we found that expression of miR-145 in serum was higher in patients in stage IV than that in other stages, even though without
statistical significance.
Discussion
MiRNAs are involved in the whole biological and physiological processed by regulating target mRNA. Severe dysfunctions and aberrant expressions are present by acting in certain cases as oncogenes while in others as tumor suppressor genes through different targets in human malignancy [16]. MiRNAs are released from primary tumor into peripheral circulation, which are stable molecules and resistant to RNase digestion and other harsh conditions in
serum. Since circulating miRNAs were first
[image:4.612.100.437.70.398.2]for several human cancers, including NSCLC [14, 17-21]. However the technique of detecting miRNAs from tissue is limited owing to its com-plication and need of invasive method to obtain.
In the current study we compared the profile of
three miRNAs in serum from 70 healthy con-trols with 70 NSCLCs and demonstrated that serum expression of miR-125a-5p, miR-145 and miR-146a strongly differentiated the NSCLC patients from healthy controls. A highly
significant increase was found in these three
miRNAs in serum of NSCLC compared with that of healthy individuals. Moreover, receiver oper-ating curve analysis indicated that the AUC of these three miRNAs were all greater than 0.7, indicating that they might be potential biomark-ers in the diagnosis of NSCLC. Especially miR-145 was proved to be the most accurate tumor marker in distinguishing NSCLC patients from healthy controls with AUC ROC reaching 0.84
and the sensitivity and specificity at optimal
cutoff being 92.75% and 61.43%.
We also analyzed the serum expression levels of these miRNAs in relation to the different clin-ical pathologic characteristics in NSCLC
patients. Unfortunately, no significant relation -ships were found between them.
MiR-125a-5p, miR-145 and miR-146a were known as tumor suppressors and down-regu-lated in a variety of malignant tumor tissues. But in some malignant tumors they might be up-regulated and the serum expressions of these miRNAs were not identical, even in the same tumor. For instance, miR125a-5p was down-regulated in gastric cancer and sup-pressed cell proliferation by targeting ERBB2 [22]. In our study we found miR-125a-5p was overexpressed in serum of NSCLC, unlike a prior report which found no difference between NSCLCs and healthy controls [23]. MiR-145 inhibits proliferation of NSCLC cells by targeting c-Myc [24] and plays an inhibitory role in tumor angiogenesis, cell growth and invasion and tumor growth through the post-transcriptional regulation through N-RAS and VEGF-A in breast cancer [25]. Nevertheless conclusions from several studies which focused on the serum expression of miR-145 were not consistent, such as in breast cancer [14, 26, 27]. For miR-146a, its role can also vary in different types of cancer. It worked as tumor suppressor in
pros-tate cancer [28] and gastric cancer [29] expressing lower regulation whereas in ana-plastic thyroid cancer [30] and cervical cancer [31] it was up-regulated as an oncogene. Even converse expression levels of miR-146a in tis-sue were tested in some malignancy like gas-tric cancer [29, 32]. All of these studies indi-cate that the targets and expressions are varied in different tumors, especially the
expression profiling in peripheral blood.
Meanwhile, few literatures were related to their serum expression in NSCLC to date.
In view of these three miRNAs targeting EGFR and its downstream gene to play their roles, we may be able to investigate the relationship between the EGFR mutation status and serum expression level in future studies.
In conclusion, the high stability of serum miR-NAs makes them become noninvasive biomark-ers for NSCLC detection. However, the
sensitiv-ity and specificsensitiv-ity are not satisfied in
distinguishing NSCLCs from healthy controls and their expression is different in various tumors, and therefore their roles and possible targets in NSCLC require further investigation. Acknowledgements
This work was supported by the Capital Medical Development Funds for Special Research Project (SF2011-5005-01) and the Medical Research Funds of 306 Hospital (2013ZD06). Disclosure of conflict of interest
None.
Address correspondence to: Dr. Jian-Zhong Zhang, Department of Pathology, 306 Hospital of PLA, 9 North Anxiang Road, Chaoyang District, Beijing 100101, China. Tel: 10-66356237; Fax: +86-10-64871261; E-mail: zhangjz55@sina.com
References
[1] Siegel R, Naishadham D, Jemal A. Cancer sta-tistics, 2012. CA Cancer J Clin 2012; 62: 10-29.
[2] Guo P, Huang ZL, Yu P, Li K. Trends in cancer mortality in China: an update. Ann Oncol 2012; 23: 2755-62.
classi-fication of lung adenocarcinoma. J Thorac On -col 2011; 6: 244-85.
[4] Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger K, Yatabe Y, Ishikawa Y, Wistuba I, Flieder DB, Franklin W, Gazdar A, Hasleton PS, Henderson DW, Kerr KM, Petersen I, Roggli V, Thunnissen E, Tsao M. Diagnosis of lung cancer in small biopsies and cytology: implica-tions of the 2011 International Association for the Study of Lung Cancer/American Thoracic
Society/European Respiratory Society classifi -cation. Arch Pathol Lab Med 2013; 137: 668-84.
[5] Reungwetwattana T, Weroha SJ, Molina JR. On-cogenic pathways, molecularly targeted thera-pies, and highlighted clinical trials in non-small-cell lung cancer (NSCLC). Clin Lung Cancer 2012; 13: 252-66.
[6] Siegel R, DeSantis C, Virgo K, Mariotto A, Smith T, Cooper D, Gansler T, Lerro C, Fedewa S, Lin C, Leach C, Cannady RS, Cho H, Scoppa S, Hachey M, Kirch R, Jemal A, Ward E. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin 2012; 62: 220-41.
[7] Friedman RC, Farh KK, Burge CB, Bartel DP. Most mammalian mRNAs are conserved tar-gets of microRNAs. Genome Res 2009; 19: 92-105.
[8] Mitchell PS, Parkin RK, Kroh EM. Circulating microRNAs as stable blood-based markers for cancer detection. Proc Natl Acad Sci U S A 2008; 105: 10513-8.
[9] Chen X, Ba Y, Ma L. Characterization of microR-NAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res 2008; 18: 997-1006.
[10] Prenzel N, Fischer OM, Streit S, Hart S, Ullrich A. The epidermal growth factor receptor family as a central element for cellular signal
trans-duction and diversification. Endocr Relat Can -cer 2001; 8: 11-31.
[11] Wang G, Mao W, Zheng S, Ye J. Epidermal growth factor receptor-regulated miR-125a-5p--a metastatic inhibitor of lung cancer. FEBS J 2009; 276: 5571-8.
[12] Cho WC, Chow AS, Au JS. Restoration of tu-mour suppressor hsa-miR-145 inhibits cancer cell growth in lung adenocarcinoma patients with epidermal growth factor receptor muta-tion. Eur J Cancer 2009; 45: 2197-206. [13] Chen G, Umelo IA, Lv S, Teugels E, Fostier K,
Kronenberger P, Dewaele A, Sadones J, Geers C, De Grève J. miR-146a inhibits cell growth, cell migration and induces apoptosis in non-small cell lung cancer cells. PLoS One 2013; 8: e60317.
[14] Mar-Aguilar F, Mendoza-Ramirez JA,
Malagon-Santiago I. Serum circulating microRNA profil
-ing for identification of potential breast cancer
biomarkers. Dis Markers 2013; 34: 163-9.
[15] Kumar S, Keerthana R, Pazhanimuthu A, Pe-rumal P. Overexpression of circulating miR-NA-21 and miRNA-146a in plasma samples of breast cancer patients. Indian J Biochem Bio-phys 2013; 50: 210-4.
[16] Croce CM. Causes and consequences of mi-croRNA dysregulation in cancer. Nat Rev Genet 2009; 10: 704-14.
[17] Zhang C, Wang C, Chen X, Yang C, Li K, Wang J, Dai J, Hu Z, Zhou X, Chen L, Zhang Y, Li Y, Qiu H, Xing J, Liang Z, Ren B, Yang C, Zen K, Zhang
CY. Expression profile of microRNAs in serum: a fingerprint for esophageal squamous cell car -cinoma. Clin Chem 2010; 56: 1871-9.
[18] Shen J, Todd NW, Zhang Hl. Plasma microRNAs as potential biomarkers for non-small-cell lung cancer. Lab Invest 2011; 91: 579-87.
[19] Shen J, Hruby GW, McKiernan JM. Dysregula-tion of circulating microRNAs and predicDysregula-tion of aggressive prostate cancer. Prostate 2012; 72: 1469-77.
[20] Giraldez MD, Lozano JJ, Ramirez G, Hijona E, Bujanda L, Castells A, Gironella M. Circulating microRNAs as biomarkers of colorectal cancer:
results from a genome-wide profiling and vali -dation study. Clin Gastroenterol Hepatol 2013; 11: 681-8.e3.
[21] Zhu C, Ren C, Han J, Ding Y, Du J, Dai N, Dai J,
Ma H, Hu Z, Shen H, Xu Y, Jin G. A five-microR
-NA panel in plasma was identified as potential
biomarker for early detection of gastric cancer. Br J Cancer 2014; 110: 2291-9.
[22] Nishida N, Mimori K, Fabbri M, Yokobori T, Sudo T, Tanaka F, Shibata K, Ishii H, Doki Y, Mori M. MicroRNA-125a-5p is an independent prognostic factor in gastric cancer and inhibits the proliferation of human gastric cancer cells in combination with trastuzumab. Clin Cancer Res 2011; 17: 2725-33.
[23] Lin Q, Mao W, Shu Y, Lin F, Liu S, Shen H, Gao
W, Li S, Shen D. A cluster of specified microR -NAs in peripheral blood as biomarkers for met-astatic non-small-cell lung cancer by stem-loop RT-PCR. J Cancer Res Clin Oncol 2012; 138: 85-93.
[24] Chen Z, Zeng H, Guo Y. miRNA-145 inhibits non-small cell lung cancer cell proliferation by targeting c-Myc. J Exp Clin Cancer Res 2010; 29: 151.
[25] Zou C, Xu Q, Mao F. MiR-145 inhibits tumor an-giogenesis and growth by N-RAS and VEGF. Cell Cycle 2012; 11: 2137-45.
[26] Zhu W, Qin W, Atasoy U, Sauter ER. Circulating microRNAs in breast cancer and healthy sub-jects. BMC Res Notes 2009; 2: 89.
[27] Ng EK, Li R, Shin VY. Circulating microRNAs as
specific biomarkers for breast cancer detec -tion. PLoS One 2013; 8: e53141.
suppressor in prostate cancer by targeting Rac1. Prosta te 2014; 74: 1613-21.
[29] Kogo R, Mimori K, Tanaka F, Komune S, Mori
M. Clinical significance of miR-146a in gastric
cancer cases. Clin Cancer Res 2011; 17: 4277-84.
[30] Pacifico F, Crescenzi E, Mellone S, lannetti A,
Porrino N, Liguoro D, Moscato F, Grieco M, For-misano S, Leonardi A. Nuclear factor-{kappa} B contributes to anaplastic thyroid carcinomas through up-regulation of miR-146a. J Clin En-docrinol Metab 2010; 95: 1421-30.
[31] Wang X, Tang S, Le SY, Lu R, Rader JS, Meyers C, Zheng ZM. Aberrant expression of oncoge-nic and tumor-suppressive microRNAs in cervi-cal cancer is required for cancer cell growth. PLoS One 2008; 3: e2557.


![(3aS,8aS,9R,9aS) 9 Hydroxy 2,3,3a,7,8,8a,9,9a octahydrofuro[3,2 f]indolizin 6(4H) one](data:image/gif;base64,R0lGODlhAQABAIAAAP///wAAACH5BAEAAAAALAAAAAABAAEAAAICRAEAOw==)