APPLICATIONS OF MCGILL PAIN QUESTIONNAIRE AS AN ASSESSMENT TOOL FOR PATIENTS
WITH PAIN: LITERATURE REVIEW
1,*
Edirisinghe, N.P.,
2Goonewardena, C.S.E.,
1
Faculty of Graduates Studies, University of Sri Jayewardenepura, Sri Lanka
2Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
3Faculty of Medicine, General Sir John Kotelawala Defense University, Sri Lanka
4
Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
ARTICLE INFO ABSTRACT
Pain is the most
Pain assessment is vital in supporting the diagnosis of the source of pain and for effective treatment. McGill Pain Questionnaire (MPQ)
significant qualities of pain. It can be used to assess the pain over time and to determine the usefulness of any intervention. It was developed by Dr. Melzack at McGill University in Montreal Canada and updated for another two ve
neuropathic and non
objective of this paper was to review the published literature to describe the applications of MPQ in pain assessment.
versions were identified.
validated in different patient populations such as those with operative pain.
for statistical analysis among cross cultures and languages were shown
Copyright © 2018, Edirisinghe et al. This is an open access distribution, and reproduction in any medium, provided
INTRODUCTION
Pain is the most common and distressing symptom ever experienced by the patients with terminal illnesses like cancers. As defined by the International Association for the Study of Pain (IASP) (International_ Association_ the_Study_of_Pain., 2017) pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is a
subjective, multidimensional experience th
significantly between individuals. Pain assessment is therefore a fundamental part of the appropriate treatment and control of pain. Pain should be regarded as an important vital sign and therefore should regularly assess using validated scales improving outcomes in pain management. Among the variety of methods available for pain assessment however no single perfect system exists and there is no simple device that can objectively record how much pain an individual experience. Pain experience is influenced by age, character, gender, past experience, individual coping strategies, culture and
circumstances. Therefore, what one patient may describe as severe may be only mild to another patient as pain is a highly subjective experience.
ISSN: 0975-833X
Article History:
Received 20th March, 2018 Received in revised form 19th April, 2018 Accepted 15th May, 2018 Published online 28th June, 2018
Citation: Edirisinghe, N.P., Goonewardena, C.S.E., Makuloluwa, P.T.R. and as an assessment tool for patients with pain: Literature Review
Key words:
McGill Pain Questionnaire, Reliability, Validity, Cross cultural adaptation.
Key words:
McGill Pain Questionnaire, Reliability, Validity, Cross cultural adaptation.
*Corresponding author
REVIEW ARTICLE
APPLICATIONS OF MCGILL PAIN QUESTIONNAIRE AS AN ASSESSMENT TOOL FOR PATIENTS
WITH PAIN: LITERATURE REVIEW
Goonewardena, C.S.E.,
3Makuloluwa, P.T.R. and
4Amarasekara, A.A.T.D.
Faculty of Graduates Studies, University of Sri Jayewardenepura, Sri Lanka
Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
Faculty of Medicine, General Sir John Kotelawala Defense University, Sri Lanka
aculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
ABSTRACT
Pain is the most distressing consequence ever experienced by the patients during their life journey. Pain assessment is vital in supporting the diagnosis of the source of pain and for effective treatment. McGill Pain Questionnaire (MPQ) is a multidimensional tool widely
significant qualities of pain. It can be used to assess the pain over time and to determine the usefulness of any intervention. It was developed by Dr. Melzack at McGill University in Montreal Canada and updated for another two versions; the latest version being enabled to assess both neuropathic and non-neuropathic pain. It demonstrated good construct and concurrent validity. The objective of this paper was to review the published literature to describe the applications of MPQ in pain assessment. From the eligible studies, 23 different MPQ language versions
versions were identified. The MPQ has been adopted as a pain assessment tool in many countries and validated in different patient populations such as those with cancer pain, low back pain and post operative pain. Validity and reliability of the MPQ as a qualitative and quantitative measure of pain for statistical analysis among cross cultures and languages were shown
access article distributed under the Creative Commons Attribution the original work is properly cited.
Pain is the most common and distressing symptom ever experienced by the patients with terminal illnesses like cancers. As defined by the International Association for the Association_ for_ the_Study_of_Pain., 2017) pain is an unpleasant sensory and emotional experience associated with actual or potential tissue or described in terms of such damage. Pain is a
subjective, multidimensional experience that diverges
significantly between individuals. Pain assessment is therefore a fundamental part of the appropriate treatment and control of pain. Pain should be regarded as an important vital sign and therefore should regularly assess using validated scales in improving outcomes in pain management. Among the variety of methods available for pain assessment however no single perfect system exists and there is no simple device that can objectively record how much pain an individual experience. is influenced by age, character, gender, past experience, individual coping strategies, culture and current Therefore, what one patient may describe as severe may be only mild to another patient as pain is a highly
Similarly, the quality of pain, such as
may interpret differently making the assessment and measurement of pain even more complex. Therefore, it is important to utilize an appropriate pain assessment tool in order to assess the pain adequately and accurately. An Expert Working Group was convened under the auspices of the Steering Committee of the Research Network of the European Association of Palliative Care to review the status of the use of pain measurement tools (PMTs) in palliati
conducted in a multilingual multicenter setting (Caraceni, 2002). Based on a literature review and on the experts’ opinion, the authors recommend that standardized methods should be applied for the use of PMTs in research and in patient care. Visual analogue scales, numerical rating scales, and verbal rating scales are considered valid to assess pain intensity in clinical trials and in other types of studies. Among the multidimensional questionnaires designed to assess pain, the McGill Pain Questionnaire and Brief Pain Inventory are valid in many multilingual versions (Caraceni, 2002). objective of this review of the published literature was to provide an update of prevailing evidence on applications of MPQ in assessment of patients wit
importance.
International Journal of Current Research
Vol. 10, Issue, 06, pp.70116-70121, June, 2018
, C.S.E., Makuloluwa, P.T.R. and Amarasekara, A.A.T.D. 2018. “Applications of mcgill pain questionnaire
as an assessment tool for patients with pain: Literature Review”, International Journal of Current Research, 10, (06), 70116 Available online at http://www.journalcra.com
z
APPLICATIONS OF MCGILL PAIN QUESTIONNAIRE AS AN ASSESSMENT TOOL FOR PATIENTS
Amarasekara, A.A.T.D.
Faculty of Graduates Studies, University of Sri Jayewardenepura, Sri Lanka
Faculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
Faculty of Medicine, General Sir John Kotelawala Defense University, Sri Lanka
aculty of Medical Sciences, University of Sri Jayewardenepura, Sri Lanka
distressing consequence ever experienced by the patients during their life journey. Pain assessment is vital in supporting the diagnosis of the source of pain and for effective treatment. is a multidimensional tool widely used clinically to evaluate significant qualities of pain. It can be used to assess the pain over time and to determine the usefulness of any intervention. It was developed by Dr. Melzack at McGill University in Montreal rsions; the latest version being enabled to assess both neuropathic pain. It demonstrated good construct and concurrent validity. The objective of this paper was to review the published literature to describe the applications of MPQ in From the eligible studies, 23 different MPQ language versions and 5 adapted pain assessment tool in many countries and cancer pain, low back pain and post-Validity and reliability of the MPQ as a qualitative and quantitative measure of pain for statistical analysis among cross cultures and languages were shown.
License, which permits unrestricted use,
Similarly, the quality of pain, such as gnawing or stabbing, may interpret differently making the assessment and measurement of pain even more complex. Therefore, it is important to utilize an appropriate pain assessment tool in adequately and accurately. An Expert Working Group was convened under the auspices of the Steering Committee of the Research Network of the European Association of Palliative Care to review the status of the use of pain measurement tools (PMTs) in palliative care research conducted in a multilingual multicenter setting (Caraceni, 2002). Based on a literature review and on the experts’ opinion, the authors recommend that standardized methods should be applied for the use of PMTs in research and in re. Visual analogue scales, numerical rating scales, and verbal rating scales are considered valid to assess pain intensity in clinical trials and in other types of studies. Among the multidimensional questionnaires designed to assess pain, Questionnaire and Brief Pain Inventory are valid in many multilingual versions (Caraceni, 2002). The objective of this review of the published literature was to provide an update of prevailing evidence on applications of MPQ in assessment of patients with pain which is of timely INTERNATIONAL JOURNAL OF CURRENT RESEARCH
McGill Pain Questionnaire: The visual analogue scale (VAS) and the MPQ appear to be the most frequently used instruments for the measurement of pain in clinical and research settings. Melzack and Torgerson in 1975 first developed the long version of MPQ and found to be valid, reliable, and consistent and provides a relatively rapid way of measuring subjective pain experience. Since its introduction in 1975, the MPQ has been used in more than 500 studies of acute, chronic, and laboratory-produced pains. It has been translated into several languages and has also adapted to development of similar pain questionnaires in other languages
(Katz, 1999). Thereafter, Short Form McGill Pain
Questionnaire (SF-MPQ) was developed in 1984 with 15 descriptors consisting of 11 sensory and 4 affective which are rated from 0= none to 3= severe. Dworkin and colleagues (Dworkin, 2009), developed the SF-MPQ-2, an expanded and revised version of the SF-MPQ, designed to measure qualities of both neuropathic and non-neuropathic pain in research and clinical settings. This includes seven new descriptors relevant to neuropathic pain and 11-point Numerical Rating Scale (NRS) for each descriptor (Dworkin, 2009). This latest version was tested on patients with chronic pain syndromes and painful diabetic neuropathy. Excellent validity and reliability was found for this new version, namely SF-MPQ-2 (Dworkin, 2009). SF-MPQ-2 has been translated and validated in several countries such as Greece, Sweden, Thailand, Japan and Korea (Georgoudis, 2001 and Burckhardt, 2001). The MPQ can be used to evaluate the efficacy and effectiveness of pain interventions and to identify qualities of pain associated with distinct nociceptive disorders and neuropathic pain disorders, including arthritis (Hawker, 2011).
Applicability of a measurement tool: The applicability of a
measurement tool depends on the properties of the tool as an outcome measure. They are known as psychometric properties or clinometric properties of the tool. Psychometric properties
involve construction and validation of measurement
instruments, whereas clinometric properties involve the clinical application into screening, diagnosis and prognosis (Kumar, 2011). The applicability is determined by two factors: (1) Validity: how accurately it measures what it was supposed to measure and (2) Reliability: how accurately the measure reflects differences due to time, repeated testing, situation, condition, intervention and testers. The measurement property of validity is the construct validity which is further subcategorized into translation validity (face validity or content validity) and criterion-related validity (four subtypes: predictive validity, concurrent validity, convergent validity, and discriminant validity) (Kumar, 2011). Reliability is referred to as the extent to which results are consistent over time and an accurate representation of the total population under study, and if the results of a study can be reproduced under a similar methodology (Golafshani, 2003). The subtypes of reliability include inter-rater reliability, test–retest reliability, parallel-forms reliability and internal consistency (Moss, 1994). Inter-rater or inter-observer reliability is used to assess the degree to which different raters/ observers give consistent estimates of the same phenomenon. Test–retest reliability is used to assess the consistency of a measure from one time to another. Parallel-forms reliability is used to assess the consistency of the results of two tests constructed in the same way from the same content domain. Internal consistency reliability is used to assess the consistency of results across items within a test consistency (Kumar, 2011). Often, a measurement tool which has a good validity need not be
reliable; and a reliable tool need not necessarily be valid (Moss, 1994).
MATERIALS AND METHODS
A review of the published literature on ‘application of MPQ as an assessment tool for pain’ was performed using online databases such as MEDLINE, PUBMED, PsycInfo and Google Scholar during the period November 2017 to March 2018. The articles were selected based on titles and abstracts published between 1981 to 2017. The search terms used MPQ, McGill pain questionnaire cross cultural adaptations, validity and reliability. The results of the search were completed by tracing references from studies already published. The search was limited to original articles published in English and review research manuscripts.
RESULTS AND DISCUSSION
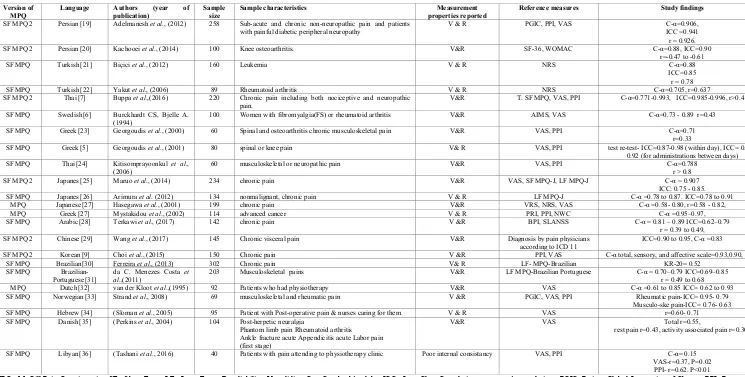
From the eligible studies, 23 different MPQ language versions, 5 adapted versions and different applications of MPQ versions were identified (Table 1). The 23 language versions represent 16 different languages/ cultures as there were multiple versions for the same language (2 Turkish, 2 Persian, 3 Japanese, 2 Thai, 3 Greek). The Spanish version was tested in 5 Spanish speaking countries Argentina, Costa Rica, Mexico, Panama, and Spain (Lázaro, 2001). Among the MPQ versions, 3 were long form MPQ, 14 were SF-MPQ and 6 were SF-MPQ-2 latest version. The different applications of MPQ included cancer pain, acute low back pain, chronic pain diagnoses, surgery related pain, orthodontic pain and pain due to burns and irritable bowel syndrome. Construct validity of MPQ: Factors are subcategories, or dimensions, of a more general topic (e.g., sensory pain is a dimension of total pain phenomena) (Mason, 2008). Melzack, proposed that the SF-MPQ consists of 2 independent factors. One was referred to as sensory, which described the nociceptive pain experience of the individual, and the other was referred to as affective, which described the emotional impact of the nociceptive pain experience. Confirmatory factor analysis is a structural equation modeling method used to test the viability of hypothesized models (Mason, 2008). A 2-factor solution was
reported by Beattie et al (Beattie, 2004), from a sample of 187
patients undergoing lumbar magnetic resonance imaging (MRI) to diagnose chronic lower back pain. Confirmatory
Factor Analysis of SF MPQ: Mason et al (Mason, 2008),
conducted a study among 338 burn injury patients with a 14% mean total body surface area burnt who met the criteria for American Burn Association’s for major burn injury. Confirmatory factor analysis produced fit index values representing viability of a 2-factor, oblique, solution composed of sensory and affective latent constructs. Those findings were consistent with previous work and the theoretic constructs (Mason, 2008). Cross cultural adaptation: With the increase in the number of multinational and multicultural research projects, the need to adapt health status measures for use in other than the source language has also grown rapidly. The cross-cultural adaptation of a health status self-administered questionnaire for use in a new country, culture, and/or language necessitates use of a unique method, to reach equivalence between the original source and target versions of the questionnaire. It is now recognized that if measures are to
beusedacrosscultures,theitemsmustnotonlybetranslated well
linguistically, but also must be adapted culturally to maintain
the content validity of the instrument at a conceptual level across different cultures (Beaton,
2000). A study done by Lazaro et al (Lázaro, 2001), investigates the psychometric
properties of a Spanish version of the MPQ in five Spanish-speaking countries. Study was performed in pain clinics and acute pain units of four Latin American countries (Argentina, Costa Rica, Mexico, and Panama) and Spain. This study included 205 patients (84 with acute pain, 121 with chronic pain) from Latin America.
[image:3.842.42.787.68.445.2]Their data were compared with those of 282 Spanish patients. Patients were evaluated once with a Spanish version of the MPQ, a visual analog scale, and a verbal rating scale. It was found that the Spanish version of the MPQ maintained a high internal validity when tested in different countries. Ordinal consistency, inter category, inter parameter, and qualitative-to-quantitative parameter correlations were similar in all countries. However, a few descriptors were considered as inappropriate or difficult to understand (Lázaro, 2001).
Table 1. Comparison of MPQ translation versions
Version of MPQ
Language Authors (year of
publication)
Sample size
Sample characteristics Measurement
properties reported
Reference measures Study findings
SF MPQ 2 Persian [19] Adelmanesh et al., (2012) 258 Sub-acute and chronic non-neuropathic pain and patients
with painful diabetic peripheral neuropathy
V & R PGIC, PPI, VAS C-α=0.906,
ICC =0.941 r = 0.926.
SF MPQ 2 Persian [20] Kachooei et al., (2014) 100 Knee osteoarthritis. V&R SF-36, WOMAC C-α=0.88, ICC=0.90
r=-0.47 to -0.61
SF MPQ Turkish[21] Biçici et al., (2012) 160 Leukemia V & R NRS C-α=0.88
ICC=0.85 r = 0.78
SF MPQ Turkish[22] Yakut et al., (2006) 89 Rheumatoid arthritis V & R NRS C-α=0.705, r=0.637
SF MPQ 2 Thai[7] Buppa et al.,(2016) 220 Chronic pain including both nociceptive and neuropathic
pain.
V&R T. SF MPQ, VAS, PPI C-α=0.771-0.993, ICC=0.985-0.996, r>0.4
SF MPQ Swedish[6] Burckhardt CS, Bjelle A.
(1994)
100 Women with fibromyalgia(FS) or rheumatoid arthritis V&R AIMS, VAS C-α=0.73 - 0.89 r=0.43
SF MPQ Greek[23] Georgoudis et al., (2000) 60 Spinal and osteoarthritis chronic musculoskeletal pain V&R VAS, PPI C-α=0.71
r=0.33
SF MPQ Greek[5] Georgoudis et al., (2001) 80 spinal or knee pain V& R VAS, PPI test re-test- ICC=0.87-0.98 (within day), ICC= 0.70–
0.92 (for administrations between days)
SF MPQ Thai[24] Kitisomprayoonkul et al.,
(2006)
60 musculoskeletal or neuropathic pain V&R VAS, PPI C-α=0.788
r > 0.8
SF MPQ 2 Japanes[25] Maruo et al., (2014) 234 chronic pain V&R VAS, SF MPQ-J, LF MPQ-J C-α = 0.907
ICC: 0.75 - 0.85.
SF MPQ Japanes[26] Arimura et al. (2012) 134 nonmalignant, chronic pain V & R LF MPQ-J C-α =0.78 to 0.87. ICC=0.78 to 0.91
MPQ Japanese[27] Hasegawa et al., (2001) 199 chronic pain V&R VRS, NRS, VAS C-α =0.58- 0.80, r=0.58 - 0.82,
MPQ Greek[27] Mystakidou et al., (2002) 114 advanced cancer V & R PRI, PPI, NWC C-α =0.95–0.97,
SF MPQ Arabic[28] Terkawi et al., (2017) 142 chronic pain V &R BPI, SLANSS C-α = 0.81 – 0.89 ICC=0.62–0.79
r = 0.39 to 0.49,
SF MPQ 2 Chinese[29] Wang et al., (2017) 145 Chronic visceral pain V&R Diagnosis by pain physicians
according to ICD 11
ICC=0.90 to 0.95, C-α =0.83
SF MPQ 2 Korean[9] Choi et al., (2015) 150 Chronic pain V &R PPI, VAS C-α total, sensory, and affective scale=0.93,0.90, 0.91,
SF MPQ Brazilian[30] Ferreira et al., (2013) 302 Chronic pain V& R LF- MPQ-Brazilian KR-20= 0.52
SF MPQ
Brazilian-Portuguese[31]
da C. Menezes Costa et al.,(2011)
203 Musculoskeletal pains V&R LF MPQ-Brazilian Portuguese C-α = 0.70–0.79 ICC=0.69–0.85
r = 0.49 to 0.68
MPQ Dutch[32] van der Kloot et al.,(1995) 92 Patients who had physiotherapy V&R VAS C-α =0.61 to 0.85 ICC= 0.62 to 0.93
SF MPQ Norwegian[33] Strand et al., 2008) 69 musculoskeletal and rheumatic pain V &R PGIC, VAS, PPI Rheumatic pain-ICC= 0.95- 0.79
Musculo-ske pain-ICC= 0.76- 0.63
SF MPQ Hebrew[34] (Sloman et al., 2005) 95 Patient with Post-operative pain & nurses caring for them V & R VAS r=0.60- 0.71
SF MPQ Danish[35] (Perkins et al., 2004) 104 Post-herpetic neuralgia
Phantom limb pain Rheumatoid arthritis Ankle fracture acute Appendicitis acute Labor pain (first stage)
V&R VAS Total r=0.55,
rest pain r=0.43, activity associated pain r=0.30)
SF MPQ Libyan[36] (Tashani et al., 2016) 40 Patients with pain attending to physiotherapy clinic Poor internal consistancy VAS, PPI C-α= 0.15
VAS-r=0.37, P=0.02 PPI- r=0.62. P<0.01
MPQ= McGill Pain Questionnaire, SF= Short Form, LF= Long Form, R: reliability; V: validity; C-α: Cronbach’s alpha, ICC= Intra Class Correlation, r= person’s correlation , PGIC=Patient Global Impression of Change, PPI=Present Pain Intensity, VAS=Visual Analogue Scale, NRS: Numerical Rating Scale, AIMS: Arthritis Impact Measurement Scales , WOMAC: Western Ontario and McMaster Universities Arthritis Index , MPI=Multidimensional Pain Inventory, PDI=Pain Disability Index , VRS= Visual Rating Scale, MHAQ= Modified Health Assessment Questionnaire, PRI=Present Rating Index ,SF 36=36-Item Short Form Survey, NWC= Number of Words Chosen, S-LANSS= Self-Completed Leeds Assessment of Neuropathic Symptoms and Signs, ICD 11= International Classification of Disease Eleventh version, KR-20=Kuder-Richardson 20 coefficient
MPQ versions have been translated in to several languages, comparison is shown in the Table 1.
Use of MPQ in different patient populations: Patients with
cancer: A systematic search of research was conducted by
Ngamkham et al (2012) to evaluate the MPQ as a
multidimensional measure of pain in adults with cancer and published in English from1975 to 2009. 30 studies have met their inclusion criteria and among them four groups of investigators reported the construct validity, five studies supported the strength of the content validity while five investigative groups reported criterion validity. The reliability of the MPQ was reported as a test-retest reliability of 0.70 (Lázaro, 1975). Findings were supportive of MPQ as an effective multidimensional measure with good stability, content, construct, and criterion validity and showed sensitivity to treatment or known-group effects. The MPQ is a valid, reliable, and sensitive multidimensional measure of cancer
pain. Another study was done by Mystakidou et al (Perkins,
2004), to assess the applicability, reliability, and validity of the MPQ on a sample of Greek patients with cancer receiving palliative treatment. MPQ was administered to 114 cancer patients before the initiation of palliative treatment, and then to 80 cancer patients during the treatment and 7 days later. The study reported a very favorable scale reliability (0.95–0.97). During the pretreatment period, correlations between Present Rating Index (PRI), Present Pain Intensity (PPI), and Number of Words Chosen (NWC) ranged between 0.42 and 0.92. During the post-treatment time, the correlations ranged between 0.28 and 0.91. Patients presented a desirable level of convergent construct validity (P<0.05) concerning their performance status. Results revealed Greek-MPQ as a reliable and valid measure for evaluating the qualities of cancer pain. Another study evaluated age differences in the validity, reliability and use of the SF-MPQ-2 in 244 people with advanced cancer pain in home palliative care in Toronto, Canada (Gauthier, 2014). It was confirmed the previously
reported four-factor solution (Affective, Continuous,
Intermittent and Neuropathic pain) in older (≥60 years) and younger (<60 years) patients. Convergent validity for total and subscales of the SF-MPQ-2 were correlated with BPI (Brief Pain Inventory) with average pain (total younger 0.67, older 0. 55). Cronbach’s alpha for younger and older patients ranged (0.89-0.93) from acceptable to excellent in each age group. Internal consistency reliability and convergent validity were similar across age groups. Therefore, this study demonstrated SF MPQ-2 as a valid tool in older and younger people with
advanced cancer pain. Chronic pain diagnoses: Lovejoy et al
(Lovejoy, 2012), evaluated the psychometric properties of SF-MPQ-2 in a sample of 186 U.S. veteran patients with a range of chronic pain diagnoses. Internal consistency reliability was in the excellent range for total pain score (Cronbach’s alpha = 0.96) and in the good to excellent range for each of the pain scale scores (Cronbach’s alpha between 0.84 and 0.92). Convergent validity was tested with Multidimensional Pain Inventory (MPI) Severity and Interference scales, The Pain Disability Index (PDI), Beck Depression Inventory, second edition (BDI-II) and the Generalized Anxiety Disorder 7-Item (GAD-7) scale. Moderate to high correlations were found between SF-MPQ-2 pain scale scores and other pain measures, ranging from 0.50 to 0.74. Four factor model confirmed and coefficients for continuous pain = 0.98, intermittent pain = 0.88, neuropathic pain = 0.94, and affective descriptors = 0.86.
Acute Low Back Pain: A study done by Dworkin et al
(2015), among 666 patients with acute low back and associated radicular leg pain assessed the psychometric properties of SF-MPQ-2. It was shown that Cronbach‘s alpha coefficients for the total score and each subscale ranged from 0.77 to 0.93, suggestive of excellent internal consistency reliability. The SF-MPQ-2 total and subscale scores were also significantly correlated with BPI-SF pain interference scale, the BPI-SF sleep interference item, the Roland and Morris Disability Questionnaire (RMDQ), and the (Hospital Anxiety and Depression Scale) HADS total score and anxiety and depression subscales. These correlations were all moderate in magnitude, ranging from .21 to .52 (all p < .001). High responsiveness was shown when baseline and endpoint data were analyzed. The results suggested that the SF-MPQ-2 has generally excellent reliability, validity, and responsiveness in a large sample of patients with acute low back and associated radicular leg pain. Surgery related pain and symptoms: The
study done by Ortner et al (2014) used SF-MPQ- 2 to evaluate
persistent pain in a healthy obstetric population undergoing planned Cesarean Delivery (CD) and to provide a comprehensive description of pain quality. Three hundred eighty-one women with no pain history, undergoing CD were included in this prospective, observational cohort study. Spinal anesthesia was standardized, and postoperative pain was recorded at 24 hours. In each woman, pain was assessed at 8 weeks, and 6 and 12 months using questionnaires of pain intensity and interference. Pain quality was assessed using the SF-MPQ-2. Post-caesarean pain has been shown to be predominantly of neuropathic nature; therefore, the SF-MPQ-2, which particularly evaluates symptoms relevant to neuropathic and musculoskeletal pain, was well suited. The most frequently reported descriptors 12 months after delivery were peri-incisional “numbness,” followed by “itching” and “tenderness.” Patients with irritable bowel syndrome (IBS):
Tanhaee et al. (2012), have done a study with a total of 107
(40 males, 67 females) IBS patients diagnosed according to Rome III criteria who referred to the Gastroenterology Clinic at Baqiyatallah Hospital, Iran. Patients completed the short-form SF-MPQ-2 which had been translated into Farsi. The findings showed acceptable reliability and validity for the short-form SF-MPQ-2 in confirming the presence of IBS.
Modified MPQ for orthodontic patients: University of
Missouri at Kansas City conducted a study aiming to modify and validate the SF-MPQ among 61 orthodontic patients (2013). Internal and external expert panels developed a Modified MPQ-SF with 15 descriptors and 4-point Likert severity scales (MMPQ-SF15). Sixty-one subjects completed the MMPQ-SF15, a visual analogue scale (VAS), and the present pain index (PPI) 24 hours after an orthodontic visit. According to the preliminary findings, MMPQ-SF15 and VAS (r = 0.78, r2s = 0.61, P, .0001), MMPQ-SF15 and PPI (r = 0.84, r2s =0.71, P, .0001), and VAS and PPI (r = 0.70, r2s = 0.48, P, .0001) were correlated positively and significantly. Internal consistency estimates of reliability (Cronbach’s alpha) for the general/emotional and localized pain subscales were 0.883 and 0.857, respectively. It was found that out of 15 descriptors 11 were discriminating pain, other 4 did not contribute meaningfully to the total score (P > 0.05) were eliminated from the MMPQ-SF15, and MMPQ-SF11 scores were computed. The investigated MMPQ-SF, particularly MMPQ-SF11, demonstrated efficiency and utility in the assessment of pain in adolescent orthodontic patients and correlated well with VAS and PPI ratings.
Adapted versions of the MPQ: In view of differences in pain reports between languages and cultures made researchers start the elaborate work of developing adapted versions of the MPQ (Strand, 1997). Adapted versions of MPQ found in the literature include Finnish pain questionnaire (Ketovuori, 1981), Italian pain (De Benedittis, 1988), Arabic pain questionnaire (Harrison, 1988) Norwegian Pain Questionnaire (Strand, 1997) and French (Boureau, 1992).
Conclusion
This review of the literature describes the development of the MPQ and its different uses in pain assessment to which the MPQ is well-matched. The MPQ can be used as both a quantitative and a qualitative measure of pain for statistical analysis in research. The MPQ is a powerful tool and, having demonstrated both reliability and validity across cultures and languages, is being adopted in many countries for clinical pain assessment, epidemiological studies, and in studies of the effectiveness of pain treatment in patients with many diagnoses. It is proposed to develop more language versions of validated MPQs enabling their application across the world for better outcomes in health care.
REFERENCES
Adelmanesh, F., Jalali, A., Attarian, H., Farahani, B., Ketabchi, S. M., Arvantaj, A. and Raissi, G. R. 2012. Reliability, Validity, and Sensitivity Measures of Expanded and Revised Version of the Short-Form McGill Pain Questionnaire (SF-MPQ-2) in Iranian Patients with
Neuropathic and Non-Neuropathic Pain. Pain Medicine,
13(12), 1631–1636.
Arimura, T., Hosoi, M., Tsukiyama, Y., Yoshida, T., Fujiwara,
D., et al. 2012. Pain questionnaire development focusing
on cross-cultural equivalence to the original questionnaire: The Japanese version of the Short-Form McGill Pain
Questionnaire. Pain Medicine, 13(4), 541–551.
Beaton, D. E., Bombardier, C., Guillemin, F. and Ferraz, M. B. 2000. Guidelines for the process of cross-cultural
adaptation of self-report measures. Spine, 25(24), 3186–
3191.
Beattie, P. F., Dowda, M. and Feuerstein, M. 2004.
Differentiating sensory and affective-sensory pain
descriptions in patients undergoing magnetic resonance
imaging for persistent low back pain: Pain, 110(1), 189–
196. https://doi.org/10.1016/j.pain.2004.03.026
Biçici, B. and Yapucu Güneş, Ü. 2012. The validity and reliability of the Turkish version of short-form McGill Pain
Questionnaire in patients with leukemia: Turkish version of
short-form MPQ. Journal of Clinical Nursing, 21(23–24),
3328–3334.
https://doi.org/10.1111/j.1365-2702.2012.04107.x
Boureau, F., Luu, M. and Doubrère, J. F. 1992. Comparative study of the validity of four French McGill Pain
Questionnaire (MPQ) versions. Pain, 50(1), 59–65.
Buppha, P. and Tontisirin, N. 2016. Reliability and Validity of the Thai Short-Form McGill Pain Questionnaire-2
(SF-MPQ-2). Journal of Anesthesia and Clinical Research,
7(8). https://doi.org/10.4172/2155-6148.1000650
Burckhardt, C. S. and Bjelle, A. 1994. A Swedish version of
the short-form McGill Pain Questionnaire. Scandinavian
Journal of Rheumatology, 23(2), 77–81.
Caraceni, A., Cherny, N., Fainsinger, R., Kaasa, S., Poulain, P., Radbruch, L. and De Conno, F. 2002. Pain
measurement tools and methods in clinical research in palliative care: recommendations of an Expert Working Group of the European Association of Palliative Care.
Journal of Pain and Symptom Management, 23(3), 239–
255.
Choi, S., Son, C., Lee, J.H. and Cho, S. 2015. Confirmatory factor analysis of the Korean version of the short-form McGill pain questionnaire with chronic pain patients: a
comparison of alternative models. Health and Quality of
Life Outcomes, 13(1), 15.
https://doi.org/10.1186/s12955-014-0195-z
da C. Menezes Costa, L., Maher, C. G., McAuley, J. H., Hancock, M. J., Oliveira, W. de M., Azevedo, D. C., … Costa, L. O. P. 2011. The Brazilian-Portuguese versions of the McGill Pain Questionnaire were reproducible, valid, and responsive in patients with musculoskeletal pain.
Journal of Clinical Epidemiology, 64(8), 903–912.
https://doi.org/10.1016/j.jclinepi.2010.12.009
De Benedittis, G., Massel, R., Nobili, R. and Pieri, A. 1988.
The Italian pain questionnaire. Pain, 33(1), 53–62.
Dworkin, R. H., Turk, D. C., Revicki, D. A., Harding, G.,
Coyne, K. S., Melzack, R. et al 2009. Development and
initial validation of an expanded and revised version of the
Short-form McGill Pain Questionnaire (SF-MPQ-2): Pain,
144(1), 35–42. https://doi.org/10.1016/j.pain.2009.02.007
Dworkin, R. H., Turk, D. C., Trudeau, J. J., Benson, C., Biondi, D. M., Katz, N. P. and Kim, M. 2015. Validation of the Short-Form McGill Pain Questionnaire-2 (SF-MPQ-2)
in Acute Low Back Pain. The Journal of Pain, 16(4), 357–
366. https://doi.org/10.1016/j.jpain.2015.01.012
Ferreira., K.A.S.L, Andrad, D.C, Teixeira, M.J, 2013 Development and Validation of a Brazilian Version of the
Short-Form McGill Pain Questionnaire (SF-MPQ), Pain
Management Nursing, 14(4) , 210 – 219
Gauthier, L. R., Young, A., Dworkin, R. H., Rodin, G., Zimmermann, C., Warr, Gagliese, L. 2014. Validation of the Short-Form McGill Pain Questionnaire-2 in Younger
and Older People With Cancer Pain. The Journal of Pain,
15(7), 756–770. https://doi.org/10.1016/j.jpain.2014.04.004
Georgoudis, G., Oldham, J. A. and Watson, P. J. 2001. Reliability and sensitivity measures of the Greek version of
the short form of the McGill Pain Questionnaire. European
Journal of Pain, 5(2), 109–118.
Georgoudis, G., Watson, P. J. and Oldham, J. A. 2000. The development and validation of a Greek version of the
short-form McGill Pain Questionnaire. European Journal of
Pain, 4(3), 275–281.
https://doi.org/10.1053/eujp.2000.0186
Golafshani, N. 2003. Understanding reliability and validity in
qualitative research. The Qualitative Report, 8(4), 597–606.
Harrison, A. 1988. Arabic pain words. Pain, 32(2), 239–250.
Hasegawa, M., Hattori, S., Mishima, M., Matsumoto, I., Kimura, T., Baba, Y., Senami, K. 2001. The McGill Pain Questionnaire, Japanese version, reconsidered: confirming
the theoretical structure. Pain Research and Management,
6(4), 173–180.
Hawker, G. A., Mian, S., Kendzerska, T. and French, M. 2011. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale
(CPGS), Short Form-36 Bodily Pain Scale (SF. Arthritis
Care and Research, 63(S11), S240–S252.
https://doi.org/10.1002/acr.20543
International Association for the Study of Pain (IASP),1979 by IASP in PAIN, number 6, page 250, Available from: https://en.wikipedia.org/wiki/International_Association_for _the_Study_of_Pain
Iwasaki, L. R., Freytag, L. E., Schumacher, C. A., Walker, M. P. and Williams, K. B. 2013. Validation of a modified
McGill Pain Questionnaire for orthodontic patients. The
Angle Orthodontist, 83(5), 906–912.
https://doi.org/10.2319/110812-859.1
Kachooei, A. R., Ebrahimzadeh, M. H., Erfani-Sayyar, R., Salehi, M., Salimi, E. and Razi, S. 2015. Short Form-McGill Pain Questionnaire-2 (SF-MPQ-2): a cross-cultural adaptation and validation study of the persian version in
patients with knee osteoarthritis. Archives of Bone and
Joint Surgery, 3(1), 45.
Katz, J. and Melzack, R. 1999. Measurement of pain. Surgical
Clinics of North America, 79(2), 231–252.
Ketovuori, H. and Pöntinen, P. J. 1981. A pain vocabulary in
Finnish—the Finnish Pain Questionnaire. Pain, 11(2), 247–
253.
Kitisomprayoonkul, W., Klaphajone, J. and Kovindha, A. 2006. Thai short-form McGill pain questionnaire.
JOURNAL-MEDICAL ASSOCIATION OF THAILAND,
89(6), 846.
Kumar, S. 2011. Utilization of brief pain inventory as an assessment tool for pain in patients with cancer: A focused
review. Indian Journal of Palliative Care, 17(2), 108.
https://doi.org/10.4103/0973-1075.84531
Lázaro, C., Caseras, X., Whizar-Lugo, V. M., Wenk, R., Baldioceda, F., Bernal, R. Baños, J. E. 2001. Psychometric properties of a Spanish version of the McGill Pain
Questionnaire in several Spanish-speaking countries. The
Clinical Journal of Pain, 17(4), 365–374.
Lovejoy, T. I., Turk, D. C. and Morasco, B. J. 2012. Evaluation of the Psychometric Properties of the Revised
Short-Form McGill Pain Questionnaire. The Journal of
Pain, 13(12), 1250–1257. https://doi.org/ 10.1016/ j.jpain
.2012.09.011
Maruo, T., Nakae, A., Maeda, L., Kenrin, S., Takahashi, K., et
al. 2014. Validity, reliability, and assessment sensitivity of
the Japanese version of the short-form McGill pain questionnaire 2 in Japanese patients with neuropathic and
non-neuropathic pain. Pain Medicine, 15(11), 1930–1937.
Mason, S. T., Arceneaux, L. L., Abouhassan, W., Lauterbach, D., Seebach, C. and Fauerbach, J. A. 2008. Confirmatory factor analysis of the Short Form McGill Pain
Questionnaire with burn patients. Eplasty, 8.
Melzack, R. 1975. The McGill Pain Questionnaire: major
properties and scoring methods. Pain, 1(3), 277–299.
Melzack, R. 1987. The short-form McGill pain questionnaire.
Pain, 30(2), 191–197.
Melzack, R. 1987. The short-form McGill pain questionnaire.
Pain, 30(2), 191–197.
Moss, P. A. 1994. Can there be validity without reliability?
Educational Researcher, 23(2), 5–12.
Mystakidou, K., Parpa, E., Tsilika, E., Kalaidopoulou, O., Georgaki, S., Galanos, A. and Vlahos, L. 2002. Greek McGill Pain Questionnaire: validation and utility in cancer
patients. Journal of Pain and Symptom Management, 24(4),
379–387.
Ngamkham, S., Vincent, C., Finnegan, L., Holden, J. E., Wang, Z. J. and Wilkie, D. J. 2012. The McGill Pain Questionnaire as a Multidimensional Measure in People
with Cancer: An Integrative Review. Pain Management
Nursing, 13(1), 27–51. https://doi.org/10.1016/j.pmn.
2010.12.003
Ortner, C. M., Turk, D. C., Theodore, B. R., Siaulys, M. M., Bollag, L. A. and Landau, R. 2014. The Short-FormMcGill Pain Questionnaire-Revised to Evaluate Persistent Pain and
Surgery-Related Symptoms in Healthy Women
Undergoing a Planned Cesarean Delivery: Regional
Anesthesia and Pain Medicine, 39(6), 478–486.
https://doi.org/10.1097/AAP.0000000000000158
Perkins, F. M., Werner, M. U., Persson, F., Holte, K., Jensen, T. S. and Kehlet, H. 2004. Development and validation of a brief, descriptive Danish pain questionnaire (BDDPQ).
Acta Anaesthesiologica Scandinavica, 48(4), 486–490.
Sloman, R., Rosen, G., Rom, M. and Shir, Y. 2005. Nurses’
assessment of pain in surgical patients. Journal of
Advanced Nursing, 52(2), 125–132.
Strand, L. I. and Ljunggren, A. E. 1997. Different approximations of the McGill Pain Questionnaire in the Norwegian language: a discussion of content validity.
Journal of Advanced Nursing, 26(4), 772–779.
Strand, L. I. and Ljunggren, A. E. 1997. Different approximations of the McGill Pain Questionnaire in the Norwegian language: a discussion of content validity.
Journal of Advanced Nursing, 26(4), 772–779.
Tanhaee Z, Fathi-Ashtiani A , Amini M, Vahedi H, Shaghaghi F. 2012. Validation of a Revised Version of the Short-form Mc-Gill Pain Questionnaire (SF-MPQ-2) for IBS Patients. Govaresh.,17:91-7.
Tashani, O. A., Alabas, O. A. and Johnson, M. I. 2016. Development of a Short-Form McGill Pain Questionnaire
for use in Libyan Populations. Pain and Rehabilitation-the
Journal of Physiotherapy Pain Association, 2016(41), 25–
30.
Terkawi, A., Tsang, S., Abolkhair, A., Alsharif, M., Alswiti,
M., Altirkawi, K. et al 2017. Development and validation
of Arabic version of the Short-Form Mcgill Pain
Questionnaire. Saudi Journal of Anaesthesia, 11(5), 2.
https://doi.org/10.4103/sja.SJA_42_17
Van der Kloot, W.A., Oostendorp, R.A., van der Meij, J., van den Heuvel J.1995. The Dutch version of the McGill pain
questionnaire: a reliable pain questionnaire, Ned Tijdschr
Geneeskd. 1995 Apr 1;139(13):669-73
Wang, J.-L., Zhang, W.-J., Gao, M., Zhang, S., Tian, D.-H. and Chen, J. 2017. A cross-cultural adaptation and validation of the short-form McGill Pain Questionnaire-2: Chinese version in patients with chronic visceral pain.
Journal of Pain Research, Volume 10, 121–128.
https://doi.org/10.2147/JPR.S116997
Yakut, Y., Yakut, E., Bayar, K. and Uygur, F. 2007. Reliability and validity of the Turkish version short-form McGill pain
questionnaire in patients with rheumatoid arthritis. Clinical
Rheumatology, 26(7), 1083–1087. https://doi.org/ 10.1007/
s10067-006-0452-6