Maciej Dzierżanowski
1, a, c, D, f, Marcin Dzierżanowski
1, b, c, Paweł Maćkowiak
1, a–c,
Witold Słomko
1, b, c, agnieszka Radzimińska
2, b, c, Urszula Kaźmierczak
2, b, c,
Katarzyna Strojek
2, b, c, Grzegorz Srokowski
2, b, c, Walery Żukow
3, e, fThe Influence of Active Exercise in Low Positions
on the Functional Condition of the Lumbar-Sacral
Segment in Patients with Discopathy
Wpływ ćwiczeń czynnych w pozycjach niskich na stan funkcjonalny
lędźwiowego odcinka kręgosłupa u pacjentów z dyskopatią
1 Department and Institute of Manual Therapy of collegium Medicum at the Nicolaus copernicus University,
bydgoszcz, Toruń, Poland
2 Department and Institute of Kinesiotherapy and Therapeutic Massage of collegium Medicum at the Nicolaus
copernicus University, bydgoszcz, Toruń, Poland
3 Department of Health University of economy, bydgoszcz, Poland
A – research concept and design; B – collection and/or assembly of data; C – data analysis and interpretation;
D – writing the article; E – critical revision of the article; F – final approval of article; G – other
Abstract
Background. Pain in the lower segments of the spine is among the most frequent symptoms in industrialized coun-tries. Injuries to intervertebral discs are the cause of this kind of discomfort in 90% of cases. The factors promoting the disease are: physical activity limitation, prolonged sitting position, overweight and bad movement stereotypes. New methods of treating sacral pain ignore the aspect of weakening the muscle force and do not introduce active exercise to the program of rehabilitation.
Objectives. The aim of the work was to describe the influence of active exercise in low positions on the functional condition of patients with L-S segment discopathy.
Material and Methods. The examination group consisted of 20 patients, including 17 women and 3 men. The examination was conducted twice, before and after a two-week long series of rehabilitation. The examined patients practiced a 20-minute exercise program for 10 days. The subjective part of the examination referred to pain dis-comfort felt by the patients and existing difficulties in performing everyday activities. The objective part included the measurement of movement range of the lumbar segment with the use of Schober’s test, finger-to-floor test and spine rotation in the sitting position.
Results. It was shown that intervertebral disc disease may lead to spine flexibility limitation and to pain occur-rence.
Conclusions. Practicing active exercise in low positions significantly improves the movement range and body pos-ture and it reduces pain in the lower segments of the spine. Moreover, the patient’s functional abilities are improved while performing everyday activities (Adv Clin Exp Med 2013, 22, 3, 421–430).
Key words: discopathy, active exercise, kinesiotherapy, rehabilitation, intervertebral disc.
Streszczenie
Wprowadzenie. bóle dolnego odcinka kręgosłupa są jednymi z najczęstszych schorzeń występujących w pań-stwach uprzemysłowionych. Ponad 90% dolegliwości jest spowodowanych uszkodzeniem krążka międzykręgowe-go. czynnikami sprzyjającymi rozwojowi choroby jest ograniczenie aktywności fizycznej, długotrwałe siedzenie, podwyższona ponad normę masa ciała i złe stereotypy ruchowe. Nowe metody leczenia bólu krzyża często pomijają aspekt osłabienia siły mięśniowej, nie wprowadzając ćwiczeń czynnych do programu rehabilitacji.
Cel pracy. Określenie wpływu ćwiczeń czynnych w pozycjach niskich na stan funkcjonalny osób z dyskopatią lędźwiowego odcinka kręgosłupa.
adv clin exp Med 2013, 22, 3, 421–430 ISSN 1899–5276
ORIGINaL PaPeRS
Material i metody. Zbadano łącznie 20 pacjentów, w tym 17 kobiet i 3 mężczyzn. badania przeprowadzono dwu-krotnie, przed i po dwutygodniowej serii zabiegów. Przez 10 dni badane osoby wykonywały 20-minutowy program ćwiczeń. część podmiotowa dotyczyła odczuwanych dolegliwości bólowych oraz istniejących utrudnień w wyko-nywaniu czynności dnia codziennego. W części przedmiotowej dokonano pomiaru zakresu ruchomości odcinka lędźwiowego za pomocą objawu Schobera, testu palce-podłoga oraz rotacji kręgosłupa w pozycji siedzącej.
Wyniki. choroba krążka międzykręgowego może doprowadzić do ograniczenia ruchomości kręgosłupa i wystą-pienia dolegliwości bólowych.
Wnioski. Zastosowane leczenie w postaci ćwiczeń czynnych w pozycjach niskich wpływa znacząco na zwiększenie zakresu ruchu, poprawę postawy ciała oraz zmniejszenie bólu dolnego odcinka kręgosłupa. Poprawiają się również możliwości funkcjonalne pacjenta podczas wykonywania czynności dnia codziennego (Adv Clin Exp Med 2013, 22, 3, 421–430).
Słowa kluczowe: krążek międzykręgowy, dyskopatia, kinezyterapia, ćwiczenia czynne, rehabilitacja, odcinek lędź-wiowy.
Pain in the lower segment of the spine fre-quently occurs in the population of industrialized countries. 60–90% of adults suffer from pain in the sacral part and the number of people with discom-fort is constantly rising [1, 2]. The source of pain in most cases (over 90%) is an injury to the inter-vertebral disc in the lumbar segment [1].
Spine overload nowadays is becoming very com-mon and it is an important etiological factor in the start of pain in the sacrum. Spine overload occurs when people do not obey ergonomic rules during their work and they lead an improper lifestyle [2].
Nowadays, people spend most of the time in a sitting position which is unfavorable in biome-chanical terms. It leads to lower spine overload and, as a consequence, intervertebral discs wear out faster [3, 4].
first, children are forced to sit at the school desk; at home they do their homework and play computer games or watch TV in a sitting position. Then, adults work, travel and rest in the sitting po-sition. It does influence body posture shaping and increases the risk of degeneration changes in the whole spine. Using a car or other means of trans-port, our spine is additionally exposed to shocks and vibrations leading to micro injuries [4, 5].
a sitting lifestyle leads to weakening of the muscular force, particularly of the muscles respon-sible for the proper posture and spine stabilization. as a result, passive elements of the motoric system take over the supporting function [3, 5].
Lack of physical activity and bad eating hab-its are the main sources of obesity. enlarged body weight overloads the motoric system and speeds up the process of degeneration [4, 5].
another factor influencing the risk of lumbar discopathy is prolonged work requiring bending and heavy lifting [6].
Degenerative changes of the intervertebral disc lead to pain and limitation of spine movement range. The patient’s physical activity and function-al abilities are seriously limited [3].
Discopathy in most cases is treated
conserva-tively. The few patients who undergo surgery do so because of ineffective conservatory treatment or the appearance of serious neurological injuries such as paresis, lack of reflex, or sphincter function disorders [1, 5].
The main part of the conservative treatment is rehabilitation. The aim of the treatment is the re-duction of pain and improvement of the patient’s everyday functioning. Improvement is gained through reduction of the load on pressed tissues, increasing the force of trunk muscles and stabiliza-tion of the spine and finally shaping up the prop-er posture. Kinesiothprop-erapy is the main means of achieving the aims mentioned above [3, 7].
The goal of the work was to assess the influence of kinesiotherapy (in the form of active exercise in the low positions) on the functional condition of the lumbar segment in patients with discopathy. The assessment concerns:
– feeling pain or discomfort during the day and night,
– the amount and type of medicines taken by the patients,
– patients’ functional condition reflected in difficulties in performing everyday activities,
– spine movement range in sagittal, transverse and coronal planes.
In this work, the authors examined the relation-ship between the unilateral symptoms of nerve root irritation and the side of appearing lateral trunk compensation and the lateral flexion range and trunk rotation. Moreover, the aim of the work was also the examination of the relationship between:
– the patients’ age and pain or discomfort, – the patients’ age and the movement range in the lumbar segment,
– the patients’ age and the improvement ob-tained during the rehabilitation,
Material and Methods
a group of 20 patients with diagnosed lum-bar discopathy took part in the examination. all patients were treated conservatively and they were directed to undergo treatment in the “ReH-MeD” Rheumatological-Rehabilitation clinic in bydgoszcz. The process of rehabilitation covered a 2-week long rehabilitation period with a series of 10 kinesiotherapy sessions.
The group consisted of 85% women and 15% men.
The patients were from 24 to 73 years old. Most patients were aged from 51 to 65 and the smallest group consisted of patients aged from 36 to 50 years.
Most patients, 11 people, suffered from an inju-ry to the L4/L5 disc, 8 people to the L5/S1 disc, and only 1 patient with an injury to the Th12/L1 disc.
examination took place twice, during the first and the last day of the rehabilitation period. The ex-amination consisted of a subjective interview with the patient and objective tests for spine functioning.
The interview referred to the patient’s condi-tion on the day of the examinacondi-tion. The informa-tion obtained included:
– type and doses of medicines taken,
– assessment of pain intensity according to the 10-point NRS scale,
– paresthesia location, pain radiation within back and lower limbs,
– limitation of everyday activity performance and its reflection on the 10-point scale, with 0 meaning no limitation and 10 as total incapacity to perform the activity.
Objective examination consisted of a measure-ment of symptoms according to Schober’s test, the distance between the fingers and the floor while bending forward, lateral flexion to the left and right and spine rotation in the sitting position.
Exercise Program
During the 2-week period of rehabilitation, patients performed a 20-minute exercise pro-gram. The exercises aimed at stabilizing muscles
reinforcement and controlling the spine and also shaping up a proper posture. all exercises were performed on a mattress in the low position: lying on the abdomen, lying on the back and support-ed kneeling. after assuming the initial position, the patient went to an active position requiring isometric muscle contraction. The patient spent 5 seconds in the active position and then went back to the initial position and rested. each exercise was repeated 12 times.
Results
examination results are presented in the form of tables and figures with the data obtained dur-ing the first and the last day of the rehabilitation period.
Medicines Taken by the Patients
On the first day of the rehabilitation period, 35% of patients did not take any medicines and 65% of respondents took medicines for sacral pain reduction. after the period of rehabilitation, the number of patients who did not need to take medicines increased to 60%. 40% of respondents decreased doses of the medicines taken and 10% did not change the dose of the medicines. None of the respondents increased the dose of the medi-cines taken.
21–35 years 20%
36–50 years 15%
51–65 years 40%
66–80 years 25%
disk L5/S1 40%
disk L4/L5 55%
another disks 5%
Fig. 2. Division according to age of patients
Ryc. 2. Podział pacjentów w zależności od wieku
Fig. 3. Division according to segment of patients’ dis-copathy
Ryc. 3. Podział pacjentów w zależności od odcinka kręgosłupa, gdzie wystąpiła dyskopatia
women 85% men
15%
Fig. 1. Patients’ division according to sex
Test of Subjective Assessment of Pain
Felt During the Day According to NRS
Scale
all examined patients felt pain in the lower segment of the spine. The average intensity of pain was described at the level of 5.9 (σ = 2.04) on a 0–10 scale. The assessment reflected numbers from 1 to 10. The modal result and median was 6. after rehabilitation, the patients assessed their pain at an average level of 3.85 (σ = 2.08). Im-provement appeared in 75% of examined patients, 10% of patients did not feel pain at all, 25% felt the same intensity of pain as before the rehabilitation and no one felt more intense pain. The assessment reflected numbers from 0 to 8. The modal result was 5 and median was 4.5. The average value of improvement was 2.05 (σ = 1.98). The modal value was an improvement by 1 grade, median – an im-provement by 1.5 grades. The correlation factor between the age and the intensification of percep-tible pain before the rehabilitation was –0.22. The correlation factor between perceptible pain before and after the rehabilitation was 0.46, and between the age and improvement, –0.13.
Test of Subjective Assessment of Pain
Felt During the Night According to
NRS Scale
60% of examined patients felt pain in the lower segments of the spine during the day. The average assessment level after the first examination was 5. The assessment reflected numbers from 1 to 10, me-dian was 4. after 10 treatments, the patients assessed their pain at an average level of 2.33 (σ = 2.66). Im-provement was observed by 83% of patients, 42% of patients noticed no pain at all, no change was no-ticed by 17%, none of the patients reported intensi-fication of the pain. The assessment reflected num-bers from 0 to 9. The modal result was 0, median – 0.5. The arithmetic average of the second exami-nation was 2.33 (σ = 3.28). The average value of im-provement was 2.67 (σ = 1.87). The differences were
reflected in the range from 0 to 6. The modal result was by 2 grades, median – by 2.5 grades. The cor-relation factor between the age and the intensifica-tion of perceptible pain before the rehabilitaintensifica-tion was 0.11. The correlation factor between the perceptible pain during the first examination and improvement after the rehabilitation was –0.01, and between the age and improvement, 0.22.
Location of Perceptible Pain
in the Back
Pain in the lumbar segment of the spine ini-tially appeared in all patients. after the rehabilita-tion, 15% of patients stopped reporting any pain of the lower back.
Pain Radiation to Lower Limbs
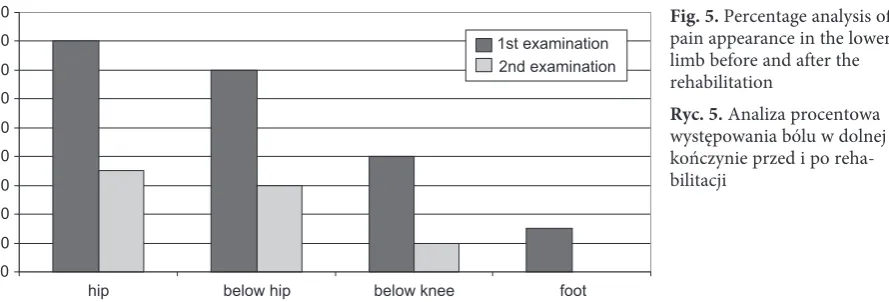
The pain radiated to lower limbs in 80% of pa-tients. 20% of patients reported pain coming from the central back part. The radiation went on der-matomes L4, L5 or S1, always from the hip to the lower limb in the distal direction. During the first examination, 15% of patients reported radiation to the foot, in 25% the pain went below the knee, in 30% it went below the hip and in 10% it stopped at the hip. During the second examination, in 50% of examined patients the pain was less severe, because it was centralized and did not reach distal parts of lower limbs. It was noticed that pain did not radi-ate to the foot, in 10% of the patients it went be-low the knee, in 20% – bebe-low the hip and in 5% it stopped at the hip.
Everyday Activity Performance
Most patients pointed to the movement of bending as the activity most limited by the inter-vertebral disc disease (65%). The second difficult activity was prolonged standing (50%) and the third activity limited by the disease was prolonged sitting (45%). Other problems concerned walking – 25%, carrying and standing up – 20% each, and getting dressing – 5%.
0 2 4 6 8 10 12
NLPZ gals miorelaxants
the number of people
before the period no medicines dose reduction no change
Fig. 4. Quantitative analysis of differences in medicine taking after rehabilitation
Bending
bending was problematic for 65% of the exam-ined patients. They assessed the difficulty in per-forming this type of movement on a scale from 0 to 10. During the examination before the rehabilita-tion, the average assessment was from 5 to 8. The modal value was 5, median 6 and arithmetic aver-age was 6.23 (σ = 1.3). after the rehabilitation, the assessments were from 2 to 7. The most frequent numbers describing the intensification of diffi-culty in bending were 3 and 4, the middle value was 4 and arithmetic average was 4.23 (σ = 1.69). Improvement was noticed by 69% of patients, in 31% the problems with bending did not change. None of the patients noticed worse problems with bending. The average value of improvement was by 2 grades (σ = 1.68). The most frequent value describing the grade of improvement was 3. The correlation factor between the age and intensifica-tion of problems before the rehabilitaintensifica-tion was 0.05. The correlation factor between the intensification of difficulties stated in the first examination and improvement after the rehabilitation was 0.38 and between the age and improvement – 0.08.
Prolonged Standing Position
Prolonged standing was problematic for 50% of examined patients. During the examination be-fore the rehabilitation, the assessments were from 4 to 8. The modal value was 5, median – 5.5 and arithmetic average was 6 (σ = 1.41). after the re-habilitation, the assessments were from 2 to 8. The most frequent number describing the intensifica-tion of pain during prolonged standing was 4, me-dian value was also 4 and arithmetic average was 4.5 (σ = 1.64). Improvement was noticed in half of the group of patients. The other half noticed no change in the pain during prolonged standing. None of the patients noticed worsening. The average value of improvement was 1.5 grades (σ = 2.12). The cor-relation factor between the age and intensification of the difficulty before the rehabilitation was 0.15. The correlation factor between the intensification
of difficulties stated in the first examination and improvement after the rehabilitation was 0.63 and between the age and improvement 0.28.
Prolonged Sitting Position
Prolonged sitting was reported as problematic by 45% of examined patients. before the rehabilita-tion the assessments were from 5 to 8. The modal value and median was 5 and arithmetic average was 5.56 (σ = 1.33). after the rehabilitation, the assess-ments were from 3 to 8. The modal value and me-dian did not change and the arithmetic average was 4.89 (σ = 1.69). Improvement was noticed by 56% of examined patients. In 44% of patients, the problem occurring before the rehabilitation remained the same after the rehabilitation. None of the patients reported worsening. The average value of improve-ment was 0.67 grade (σ = 0.7). The most frequent value of improvement in prolonged sitting was 1. The correlation factor between the intensification of difficulties stated in the first examination and improvement after the rehabilitation was –0.31 and between the age and improvement, 0.11. The cor-relation between the age and intensification of dif-ficulties before the rehabilitation was –0.02.
Analysis of Changes in the
Assessments of Everyday Activity
Disorders
after the period of rehabilitation, the biggest change of the average assessment of disordered ac-tivities concerned bending. The improvement that occurred was noticed by 2 grades. Other activities were: standing up – improvement by 1.75 grades, prolonged standing – improvement by 1.5 grades, walking – improvement by 1.2 grades, prolonged sitting – improvement by 0.67 grades and carrying things by 0.25 grades. During the first examina-tion, the average assessment value for all activities was 5.96, whereas during the second examination it was 4.74, which indicates an improvement by 1.23 grades.
0 10 20 30 40 50 60 70 80 90
foot below knee
below hip hip
1st examination 2nd examination
Fig. 5. Percentage analysis of pain appearance in the lower limb before and after the rehabilitation
The increase in the distance between the S1 disc styloid process and the point located 10 cm below appears physiologically while bending forward and it equals app. 5 cm. In the examined patients, the increase was from 0.3 cm (that is 6% of the norm) to 4.5 cm (90% of the norm). The arithmetic aver-age, mode and median of all obtained results were the same, that is 2.5 cm (σ = 1.07) which was 50% of the physical norm. During the second exami-nation, the increase was from 0.5 (that is, 10% of the norm) to 4.8 – 96% of the norm. The arith-metic average was 3.4 cm (σ = 1.07), that is 68% of the physiological movement range. Thus it changed by 0.9 cm (σ = 0.57), which is 18% of the norm. The mode result was 3.9 cm and me-dian – 3.75 cm. The meme-dian of distance increase was 0.75 cm. all patients reported the increase. The correlation factor between the age and result obtained before the rehabilitation was –0.36. The correlation factor between the result stated in the first examination and improvement after the re-habilitation was –0.23 and between the age and improvement, 0.05.
Schober’s Test for Straightening
The decrease of the distance between the S1 disc styloid process and the point located 10 cm above in straightening backwards physiologically equals 2 cm. In the examined patients, the distance decrease was from 0.1 cm, which was 5% of the norm, to 2 cm (100% of the norm). The arithme-tic average was 1 cm (σ = 0.52) and the mode and median of the obtained results was 0.9 cm, which equals 45% of the physiological range. During the second examination, the distance decrease was from 0.4 cm (10% of the norm) to 2.5 cm (125% of the norm). The arithmetic average was 1.43 cm (σ = 0.50), which equaled 71.5% of the physiological movement range. Thus it was changed by 0.42 cm (σ = 0.41), which equaled 26.5% of the norm. The mode and the median were 1.3 cm, which indicates their increase by 0.4 cm. Improvement was noticed by 85% of patients. The rest of the patients did not state a difference between the results of the first and second examination. The correlation factor between the age and result obtained before the re-habilitation was –0.24. The correlation factor be-tween the result stated in the first examination and
Table 1. average grading of activity disorders and their changes after 2-week rehabilitation period
Tabela 1. Średnia klasyfikacja zaburzeń czynności i ich zmian po 2-tygodniowym okresie rehabilitacji No.
(Lp.) Disordered activites (Zaburzone czynności) 1st exam. (1. badanie) 2nd exam. (2. badanie) Difference (Różnica)
1 bending 6.23 4.23 2.00
2 prolonged standing 6.00 4.50 1.5 3 prolonged sitting 5.56 4.89 0.67
4 walking 6.00 4.80 1.2
5 carrying 5.00 4.75 0.25 6 standing up 7.00 5.25 1.75 average (Średnio) 5.96 4.74 1.23
0 10 20 30 40 50 60 70 80
bending prolonged
standing prolongedsitting walking carrying standing up
Improvement No change
Fig. 6. Percentage analysis of the number of patients who noticed a change in difficult activities assessment because of intervertebral disc disease after 2-week rehabilitation Schober’s test for bending
improvement after the rehabilitation was –0.35 and between the age and improvement, 0.33.
Fingers-to-Floor Test – Bending
Forward
The test measured the distance between the longest finger and the floor while being bent for-ward without feeling pain. The first examination showed that the distance was from 0.2 cm below the level of the feet to 67.1 cm. The average was 28.97 cm (σ = 20.62), median – 27.15. after the rehabilitation period, 95% of the patients noticed improvement, 5% of the patients stated the same distance before and after the rehabilitation. The average distance from the fingers to the floor while bending forward was 22.55 cm (σ = 19.87), median – 17.65 cm. Shortening of the distance measured in the fingers-to-floor test was noticed in a wide range, from 0.2 cm to 22.9 cm. The average dis-tance difference between the results before and after the rehabilitation reached the value 6.43 cm (σ = 7.08). The improvement median was 3.9 cm. The correlation factor between the age and result obtained before the rehabilitation was 0.04. The correlation factor between the result stated in the first examination and improvement after the reha-bilitation was 0.28 and between the age and im-provement, 0.02.
Fingers-to-Floor Test for the
Lateral Flexion to the Right
The next test measured the distance between the longest finger of the hand placed along the low-er limb and the floor in the position of maximum flexion to the right side. The obtained results de-pended not only on spine mobility but on the pa-tients’ height and the length of their limbs as well. both the height and the limb length did not change
within the period of rehabilitation thus the differ-ence obtained from the comparison of the distance before and after the rehabilitation gives the infor-mation about the improvement or deterioration in spine mobility. The average distance between the longest finger and the floor in the maximum lat-eral flexion to the right was 52.56 cm (σ = 5.14). The distance shortened after the rehabilitation to an average value of 50.56 cm (σ = 4.54). The range improved in 90% of patients, 5% of the patients noticed limitation of the range and for 5% the value did not change. The differences be-tween the first and the second examination were from –7.7 cm to +1 cm. The median was –1 cm. The correlation factor between the age and result obtained before the rehabilitation was –0.02. The correlation factor between the result stated in the first examination and improvement after the re-habilitation was –0.47 and between the age and improvement, 0.48.
Fingers-to-Floor Test for the
Lateral Flexion to the Left
a similar measurement was conducted for the flexion to the left side. The average distance be-tween the longest finger of the left hand and the floor in the position of maximum flexion to the left side was 52.19 cm (σ = 5.96) during the first examination. The second examination showed a shortening of the average distance by 2.03 cm (σ = 2.19), and it was 50.16 cm (σ = 5.11). The mo-bility range was improved in 95% of the patients and did not change in 5% of the patients. The dif-ferences between the first and second examination were from –6.9 cm to 0 cm. Median was 1.1 cm. The correlation factor between the age and result obtained before the rehabilitation was –0.15. The correlation factor between the results stated in the first examination and improvement after the
reha--10 0 10 20 30 40 50 60 70 80
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 1st examination
2nd examinatoin
Fig. 7. The results of the fingers-to-floor test for the movement of bending forward
bilitation was –0.54 and between the age and im-provement, 0.13.
after two weeks of rehabilitation, 90% of the patients noticed improvement of the spine lateral flexion. flexion to the right and left side became deeper in both cases by approx. 2 cm in the fin-gers-to-floor test. also, a smaller range of mobil-ity to the right was observed in comparison to the movement to the left. The average difference was 0.36 cm during the first examination and 0.39 cm during the second.
Spine Rotation Test
in the Sitting Position
a test of spine rotation to the right in the sit-ting position before the rehabilitation showed av-erage results of 6 up to 46 degrees. after the reha-bilitation, the results changed to 12 and up to 59 degrees. The arithmetic average and the median of spine rotation to the right during the first examina-tion were 25 degrees (σ = 9.6). The second exami-nation showed 34 degrees (σ = 9.9). Improvement was noticed by 95% of the patients, the rest did not notice any change. The increase of spine rotation range to the right was from 0 to 23 degrees. The median was 8 degrees and the arithmetic average showed an improvement by 9 degrees (σ = 5.4). The correlation factor between the age and the re-sult obtained before the rehabilitation was –0.32. The correlation factor between the results stated in the first examination and improvement after the rehabilitation was –0.22 and between the age and improvement, 0.05. In spine rotation to the left, the results from the first examination were from 4 to 52 degrees. The second examination showed values from 13 to 64 degrees. The arithmetic aver-age and median before the rehabilitation were 28 degrees (σ = 13). after rehabilitation, the average went up to 39 degrees (σ = 11.8) and the median up to 40 degrees. Improvement was noticed by 95% of patients, 5% of patients did not notice any change in rotation range to the left. The improvement obtained by the patients was between 0 to 25 de-grees. The median was improvement of the range by 10.5 degrees and the arithmetic average was 11 degrees (σ = 6.3). The correlation factor between the age and the result obtained before the rehabili-tation was –0.20. The correlation factor between the results stated in the first examination and im-provement after the rehabilitation was –0.22 and between the age and improvement, 0.11.
after two weeks of rehabilitation, 95% of pa-tients noticed an improvement in spine rotation and 5% of patients did not notice any change. Dur-ing the first examination, the arithmetic average of results of the rotation to the left was greater by
3 degrees in comparison to the rotation to the right. The second examination showed that rotation to the left was greater by 5 degrees in comparison to the rotation to the right.
Discussion
Incidents of pain are being observed more and more nowadays. They are often connected with injuries of the intervertebral disc. This situation is a real challenge for contemporary physiotherapy. The basic aims of the conservatory treatment in-clude pain reduction and improvement of the pa-tient’s functional condition [8, 9].
The rising number of patients suffering from this type of disease and the need for fast recovery have led to several new methods of conservatory treatment of sacral pain. Prophylactic elements reducing the overload of the spine have also been introduced. They mainly relate to the elimination of harmful environmental factors and acquiring the proper models of movement while performing everyday activities. Special new sets of exercises are emerging. They are supported by theory and assume the rank of a method. They often include a non-stereotypical attitude towards spine degen-eration caused by overload [1, 8].
It is difficult to compare the efficiency of the applied therapies in the conservatory treatment of sacral pain. according to Dziak, the cause is de-fined by irregular periods of remission and exac-erbation and also different levels of disability of patients with lumbar discopathy. The results of examinations are frequently contradictory. Some researchers point to the efficiency of a particular method and others deny it. Physical exercise is a therapy that evokes the least doubts. There has been research conducted on a variety of programs including isometric exercises, isokinetic exercises and active exercises in reduced load. Many authors have examined the subjective judgment of the pa-tient and spine mobility in the sagittal plane with the use of Schober’s test and also the fingers-to-floor test. Some of them have measured trunk ro-tation and flexion range in the coronal plane. The influence of active exercise in low positions on everyday activities has not been described in the literature [8–11].
Hakkinen underlines that an exercise program directed to improving the patient’s muscular force, if well planned and individualized, plays a prophy-lactic and therapeutic role for the proper function-ing of the neuromuscular system [12].
patients with lumbar discopathy. However, if the exercises are meant to lead to muscle hypertrophy, which means its overgrowth in terms of force and volume, the number of repetitions should not ex-ceed 12 and the load should cause the feeling of fa-tigue. Thus exercises based on multiple repetitions (for ex. 25 times) and with a small load (for ex. 20% of maximum ability) or practicing isometric exer-cises will not lead to a significant improvement of muscular force. However, improvement in mus-cular endurance will appear, which brings positive results observed by researchers [13].
Strojnik and Vengust, after a period of 8 weeks of training directed to improvement in the muscular force of patients with chronic sacral pain, did not notice improvement in the force of the muscles straightening the back. However, they stated a decrease in pain discomfort from an aver-age value of 4.4 to 2.4 points according to the NRS scale [14].
The aim of several examinations was to de-scribe the influence of the exercises and their type on the changes in the mobility range. Sous and Stryła conducted an examination on a group of pa-tients with herniated discs in the lumbar segment. They measured the distances in the Schober’s test for bending forward before and after a series of rehabilitation exercises. before the rehabilitation, they obtained the result of 4.6 cm and after the re-habilitation, 43.6% of patients noticed an average improvement by 1.3 cm [15].
Trzaskoma and Drapała, after a period of 3-months’ rehabilitation obtained using the same test, obtained the results of improvement by an average value of 1.7 cm. The initial range was also the value of 4.6 cm [13]. In this research, improve-ment was observed in all patients by an average value of 0.9 cm, starting from 2.5 cm measured before the rehabilitation and finishing at a value of 3.4 cm after the rehabilitation. The lower value of improvement may result from the shorter pe-riod of rehabilitation (6 times shorter) and from the differences in the group concerning the phase of the disease. There were patients with chronic discomfort and patients in the subacute phase of intervertebral disc disease.
Not all publications confirm an improvement in mobility range after systematic exercise.
Trzaskoma and Drapała state that exercises improving the trunk straightening range also re-duce the pain discomfort. They showed that their patients improved the mobility ranges and their pain discomfort was reduced. This is consistent with the conclusions presented in this work [13].
complex rehabilitation together with studying everyday exercises to avoid pain has been applied to patients of the experimental group. Pain
reduc-tion has been shown among 59% of the patients. agility at the cervical spine has improved among 49% of the patients, at the lumbar part of the spine of the patients. Rehabilitation during prophylaxis treatment has a beneficial effect on pain reduc-tion as well as agility improvement at the cervi-cal spine among the majority of the experimental group [17]. In present research, the Schober’s test showed an improvement of the straightening range in 85% of patients.
Mach-Ossowska, in a group of 55 patients with lower back pain, obtained a higher average im-provement in trunk rotation to the left than to the right after the rehabilitation [18]. Present research also showed a greater improvement in the trunk rotation to the left in comparison to the right, by an average value of 2 degrees.
bentsen et al., in a group of 74 women with chronic lumbar pain, did not notice any significant changes in the range of flexion, straightening, trunk lateral flexion and in symptoms of the Schober’s test after 12 months of dynamic exercises of the back and abdominal muscles. However, he stated a pain discomfort decrease [19].
Present research in addition to that quoted above shows that practicing active exercise in low positions results in a pain discomfort decrease, im-provement in spine movement range and general improvement of the functioning condition of the patient.
The efficiency of performing active exercise in low positions by patients with lumbar discopathy may be confirmed by:
– a reduction of day and night pain discomfort after the kinesiotherapy,
– a reduction of the amount of medicines tak-en by patitak-ents or evtak-en discontinuance of medicine taking,
– improvement of the functional condition of the patient, reflected by the decrease of disorders in everyday activity performance,
– improvement in painless spine movement ranges in all three planes.
The pain accompanying lumbar discopathy activates impulsive muscle contraction, which may be the cause of spine movement range limitation in three planes.
The research conducted and the analyzed doc-umentation show that:
– elderly patients notice less pain discomfort dur-ing the day in comparison to younger ones. at night, the elderly patients feel worse than the young,
– spine movement range depends on the age and is more limited in the case of elderly patients,
range and the decrease of pain perceived during the rehabilitation,
– patients with greater initial limitations in spine movement range and more intense pain discomfort obtain more improvement in these aspects.
The research conducted points to the need for the continuation of applied rehabilitation.
an assessment of the long-term results of the therapy, referring to the prophylactics against repeated periods of exacerbation, requires longer observations.
References
[1] Dziak A: bóle krzyża. Med Sport, Kraków 2003.
[2] Dziak A: Postępowanie diagnostyczne w bólach krzyża. Rehab Med 2001, 5, 4, 9–23.
[3] Dziak A: Leczenie bólów krzyża. Rehab Med 2002, 6, 4, 26–43.
[4] Rakowski A: Kręgosłup w stresie. Gdańskie Wydawnictwo Psychologiczne, Gdańsk 2003.
[5] Kiwerski J: Przyczyny zespołów bólowych kręgosłupa. Post Rehab 2000, 14, 2, 41–44.
[6] Stodolny J: choroba przeciążeniowa kręgosłupa. ZL Natura, Kielce 2000.
[7] Dega W, Milanowska K: Rehabilitacja medyczna. PZWL, Warszawa 1983.
[8] Kokosz M, Saulicz E: Porównanie skuteczności leczenia szpitalnego i ambulatoryjnego u chorych z dolegliwościa-mi bólowydolegliwościa-mi dolnego odcinka kręgosłupa. fizjoterapia 1996, 4 (1–2), 71–75.
[9] McGrill, Stuart M: Poprawienie skuteczności ćwiczeń fizycznych stosowanych w bólach krzyża. Rehab Med 1999. 3 (4), 44–64.
[10] Huijbregts P: Możliwości odprowadzenia przepukliny krążka międzykręgowego – fakty i fikcje. Rehab Med 2000, 4 (2), 60–72.
[11] Roczniak W, Oświęcimska J: Podstawowe zalecenia rehabilitacyjne dla pacjentów z bólami krzyża. Lekarz 2007, 7–8, 19–25.
[12] Häkkinen A, Ylinen J, Kautiainen H, Tarvainen U, Kiviranta I: effects of home strength training and stretching versus stretching alone after lumbar disk surgery: a randomized study with a 1-year follow-up. arch Phys Med Rehabil 2005, 86, 865–870.
[13] Trzaskoma Z, Drapała G: Zmiany siły maksymalnej mięśni zginających i prostujących tułów i zakresów ruchów kręgosłupa w procesie usprawniania kobiet i mężczyzn z bólem lędźwiowego odcinka kręgosłupa. Post Rehab 2006, 20 (4), 23–32.
[14] Strojnik V, Vengust R: effect of strength training on chronic low back pain. Serres. Greece. ed. Kellis e, amiridis IG, Vrabas IS, book of abstracts of Intern. conf. on Strength Training 2004, 11, 3–7.
[15] Sous M, Stryła W: Ocena gibkości kręgosłupa chorych z zespołami bólów części lęźwiowej kręgosłupa na tle prze-pukliny jądra miażdżystego. Post Rehab 1999, 13(3), 45–55.
[16] Tłustochowicz M, Zakrzewska A, Śliwińska J: bóle dolnego odcinka kręgosłupa u kobiet po 55. roku życia – ana-liza patogenetyczna. Reumatologia 2006, 1, 41–44.
[17] Wolan-Nieroda A, Depa A, Przysada G, Pop T: Ocena efektów rehabilitacji pacjentow z zespołem bólowym krę-gosłupa w odcinku szyjnym. Young Sport Sci Ukraine 2011, 3, 75–81.
[18] Mach-Ossowska U: Ocena efektów rehabilitacji chorych ze zmianami zwyrodnieniowymi odcinka lędźwiowego kręgosłupa. Post Rehab 2000, 1, 29–30.
[19] Bentsen H, Lindgarde F, Manthorpe R: The effect of dynamic strength back exercise and/or a home training pro-gram in 57-year-old women with chronic low back pain. Results of a prospective randomized study with a 3-year follow-up period. Spine 1997, 22, 1494–1500.
Address for correspondence:
Walery Żukow
Institute of Health and Physical culture and Sport University of economy in bydgoszcz
Garbary 2 85-229 bydgoszcz Poland
e-mail: [email protected]
conflict of interest: None declared