Alicja Kędzia
1, Michał Tkaczyszyn
1, Jowita Woźniak
1,
Arkadiusz Szkutnik
1, Krzysztof Dudek
2An Analysis of Pectoralis Major Muscle Morphology and
Topography During the Fetal Period – Clinical Aspects
Analiza morfologii i topografii mięśnia piersiowego większego
w okresie prenatalnym w aspekcie klinicznym
1 Department of Anatomy, Wrocław Medical University, Wrocław, Poland
2 Institute of Machine Design and Operation, Wrocław Technical University, Wrocław, Poland
Abstract
Background. Recognition of pectoralis major muscle morphology and variation is of major clinical importance both for mammography readings and for plastic surgery.
Objectives. The goal of the study was to describe pectoralis major muscle (PMM) morphology and topography in the fetal period.
Material and Methods. The observations were carried on 98 fetuses aged 16–26 weeks of fetal life, from the collection of Wroclaw Medical University’s Department of Anatomy. The study was based on anthropological methods, prepa-ration, computer image acquisition, computer image processing using the ImageJ measurement tool and statistical methods. Topographic parameters were designated and symmetry, sexual dimorphism and growth rates were noted. Results. No sexual dimorphism was found. Pectoral major muscle size symmetry was observed on the left and right sides. The muscle linear dimensions showed high interindividual variability.Two cases of sternal muscle presence were noted (Adv Clin Exp Med 2011, 20, 6, 699–709).
Key words: pectoralis major muscle, sternal muscle, fetal period, anatomy, morphometry.
Streszczenie
Wprowadzenie. Poznanie morfologii i odmian m. piersiowego większego ma duże znaczenie kliniczne w bada-niach mammograficznych i chirurgii plastycznej.
Cel pracy. Ocena morfologii i topografii m. piersiowego większego w okresie prenatalnym.
Materiał i metody. Zbadano 98 płodów, w tym 22 płci żeńskiej, w wieku 16–26 tygodni życia płodowego, w przed-ziale CRL: 104–215 mm. Materiał pochodził ze zbiorów Katedry i Zakładu Anatomii Prawidłowej Akademii Medycznej we Wrocławiu. W pracy posługiwano się metodami: antropologicznymi, preparacyjnymi, cyfrową akwizycją obrazu, komputerowym systemem przetwarzania obrazu z wykorzystaniem opcji pomiarowej Image J oraz metodami statystycznymi.
Wyniki. Dla każdego mięśnia piersiowego większego określono punkty pomiarowe: A – punkt przyczepu części obojczykowej PMM do bocznej części obojczyka, B – punkt przyczepu włókien części obojczykowej do przyśrodkowej części obojczyka, C – punkt przyczepu części mostkowo-obojczykowej do dolnej części mostka, E – punkt wyjścia wiązek mięśnia z przyczepu na kości ramiennej. Zmierzono odległości między nimi: AA, BB, CC, oraz długości poszczególnych odcinków: AE, AB, BC,AC oraz pole powierzchni mięśnia i wymiary kątowe: α – kąt między odcinkami AE i AB i kąt β – kąt między obojczykowym a mostkowym przyczepem mięśnia. Parametry topograficzne oznaczono w systemie „O/1”. Zbadano symetrię, dymorfizm płciowy i tempo wzrostu.
Wnioski. Stwierdzono brak dymorfizmu płciowego. Obserwowano symetrię po stronie prawej i lewej. Wymiary liniowe mięśnia cechowała duża zmienność międzyosobnicza, do opisu ich wzrastania użyto modeli regresyjnych liniowych. Wzrastanie pola powierzchni mięśnia opisano za pomocą modelu wielomianowego. Nie zaobserwow-ano różnic w częstości występowania analizowanych cech topograficznych u płodów żeńskich i męskich. Opiszaobserwow-ano dwa przypadki występowania mięśnia mostkowego (Adv Clin Exp Med 2011, 20, 6, 699–709).
Słowa kluczowe: mięsień piersiowy większy, mięsień mostkowy, okres prenatalny, anatomia, morfometria. Adv Clin Exp Med 2011, 20, 6, 699–709
ISSN 1230-025X
ORIgINAL PAPERS
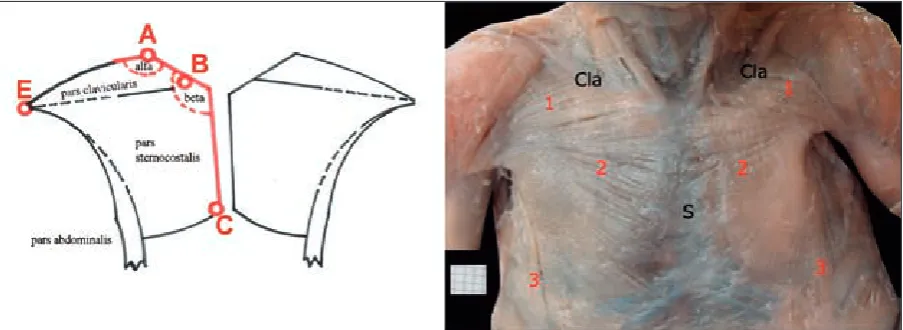
The pectoralis major muscle (PMM) consists of three parts: the clavicular part begins on the proxi-mal part of clavicle; the sternocostal part begins on the anterior surface of the sternum and the first six costal cartilages; the small ventral part originates from the tendinous sheath of rectus abdominis muscle. In the humerus attachment area there is a bistratal tendon [1]. Pectoral muscle variations are not rare. Numerous anomalies of the PMM have been described in the literature. During rou-tine post mortem dissections of two adult males, Yamasaki observed the absence of the clavicu-lar head and traces of a sternocostal head [2]. In 72 females, Mosconi and Kamath found nosternal part of the PMM sternocostal head and a total ab-sence of the muscle on the other side [3]. Cases of an extra muscle head also appear in the literature [4]. The PMM is not indispensable for the proper functioning of the shoulder girdle [5]. Lee et al. discussed the case of a 22-year-old male with con-genital unilateral absence of the PMM, which did not significantly influence his normal functioning [6]. Mysnyk and Johnson stated that congenital deficiency of the sternocostal head in major and minor pectoral muscles did not prevent two males from becoming college wrestling champions [7]. In accessory investigations carried out on these subjects, their muscle adductory force was found to be 20% to 30% less in the vertical plane than in normal subjects [7].
Recognizing muscle anomalies, variants and topography are especially useful in radiology (mammography) [8] and in plastic surgery, where this muscle flap is commonly used in head or neck reconstructions [9]. The goal of this study was to investigate PMM metrology and topography in the fetal period.
Material and Methods
The material consisted of pectoralis major muscles dissected from 98 fetuses (22 females) aged from 16 to 26 weeks of fetal life (crown to rump length [CRL] from 104 to 215 mm) from the collection of the Department of Anatomy at Wro-claw Medical University, Wrocław, Poland. The fetuses were preserved in formalin solution for similar time intervals.
The following methods were incorporated in the study: preparation with microsurgical instru-ments, anthropological methods, digital image acquisition, computer image processing using the ImageJ 1.41 measurement system and statistical methods (the Statistica software package). The anthropological methods involved determining the biological age of the fetuses using CRL in con-junction with the Scammon-Calkins formula [10]. Digital image acquisition enabled repeated and thorough measurements and prevented excessive damage of unique fetal material. The ImageJ pro-gram can convert pixels to millimeters and ensures measurement accuracy to within 0.01 mm.
For every PMM, the following measurement points were determined (Fig. 1): A – the attach-ment of the pars clavicularis of the pectoralis ma-jor muscle to the lateral part of the clavicle, B – the attachment of the pars clavicularis fibers to the median part of the clavicle, C – the attachment of the pars sternocostalis to the inferior part of the sternum, E – the divergence of the muscle bundles from the humerus attachment;angle α – the angle between sections AE and AB, and angle β – the angle between the muscle’s clavicular and sternal attachments.
For every fetus, the following measurements were taken: crown-to-rump length (CRL), vertex-to-plantare length (V-PL), the distance between points A on the left and right sides (AA distance), the distance between points B on the left and right sides (BB distance), the distance between points C on the left and right sides (CC distance), the dis-tance between points A and E (AE disdis-tance), the distance between points A and B (AB distance), the distance between points B and C (BC distance), the distance between points A and C (AC distance), the area of the PMM (Area), Angle α and Angle β. Figure 1 presents example preparation and mea-surement points.
Symmetry, sexual dimorphism and growth rate were examined. Topographic parameters were de-scribed using a “Yes/No” system for the following
features: Pars abdominalis – absent, Pars sternocos-talis – absent, connection with m. deltoideus – ab-sent, trigonum deltoidopectorale – clear and sulcus interpectoralis – clear. The pars clavicularis, pars sternocostalis and pars abdominalis were each de-scribed as symmetrical, larger on the left or larger on the right.
Results
The basic statistics describing the somatic features of the examined fetuses are presented in Table 1. The examined features were symmetrical in both genders with regard to pectoralis major shape; the only statistically significant difference was observed in BC length (Table 2). The
exam-Table 1. Characteristics of the examined fetuses (mean ± SD)
Tabela 1. Charakterystyka badanych płodów (mean ± SD) Week
(Tydzień) N (Liczba) CRL – mm (Długość CRL – mm) V-PL – mm (Długość v-pl – mm) Mass – g (Masa ciała – g)
F M female male female male female male
16 17 18 19 20 21 22 23 24 25 26 0 1 0 3 1 4 7 4 1 0 1 1 9 6 3 3 16 22 14 2 0 0 – 118 – 154 ± 21 155 159 ± 2 172 ± 4 184 ± 2 190 – 215
104 117 ± 4 130 ± 3 139 ± 3 153 ± 3 159 ± 7 173 ± 3 180 ± 15 194 ± 2 – –
– 169 – 261 ± 53 170 221 ± 5 255 ± 18 263 ± 11 276 – 310
144 161 ± 8 182 ± 3 200 ± 11 218 ± 8 222 ± 32 248 ± 16 258 ± 24 283 ± 16 – –
– 78 – 348 ± 150 350 246 ± 28 313 ± 72 374 64 415 – 590
63 100 ± 30 140 ± 12 194 ± 66 223 ± 45 269 ± 40 327 ± 74 358 ± 88 510 ± 0 – –
Table 2. Comparison of basic statistics (mean ± SD) of the muscle measurements on the right and left sides, with t-Student test results for related features
Tabela 2. Porównanie podstawowych statystyk (mean ± SD) badanych wymiarów mięśnia po stronie prawej i lewej oraz wyniki testów t-Studenta dla cech powiązanych
Dimensions
(Wymiary) Right (Prawa) n = 98
Left (Lewa) n = 98
t p
AE distance – mm (Odległość AE – mm) AB distance – mm (Odległość AB – mm) BC distance – mm (Odległość BC – mm) AC distance – mm (Odległość AC – mm) Area – mm2
(Pole powierzchni – mm2) Angle α – °
(Kąt α – °)
Angle β – °
(Kąt β – °)
14.0 ± 3.9
10.5 ± 4.0
18.9 ± 4.4
26.1 ± 6.3
437 ± 189
127 ± 21
119 ± 14
14.3 ± 4.3
10.5 ± 4.3
19.4 ± 4.9
26.1 ± 6.3
432 ± 182
128 ± 23
119 ± 12
ined fetuses were homogenous in terms of age, somatic features, pectoralis major muscle size, shape and location; the only statistically significant differences noted were in the V-PL and AA dis-tance (Table 3). In terms of qualitative features, no statistically significant differences were observed between male and female fetuses (Table 4). The statistical analysis revealed that the differences be-tween the topographic features of male and female fetuses were statistically insignificant (p < 0.05).
Due to the homogeneity of pectoral muscle size and the lack of sexual dimorphism, all mea-surements from all 98 fetuses were used in the further analysis. Table 5 presents the results of the different mathematical models for the parameters assessed and the relationship between PMM length and morphological age (in weeks).
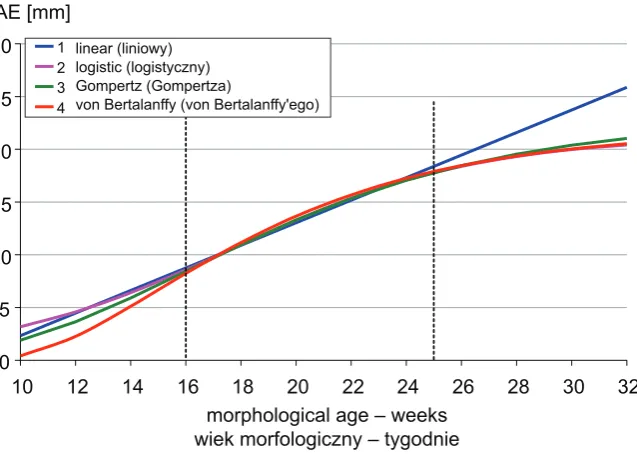
To describe the growth rate, four widely used formula types were applied (Table 5):
1. linear L(t) = a + b · c
2. logistic L(t) = A/(1 + c · exp(–K · t)) 3. gompertz’s (t) = A · exp(–c · exp(–K · t))
4. von Bertalanffy’s
L(t) = A · exp (1 – c · exp(–K · t))3
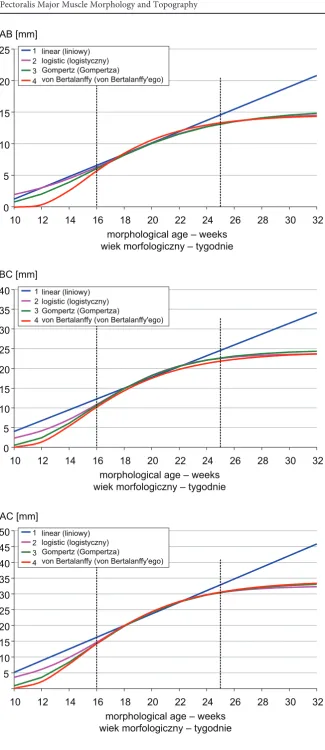
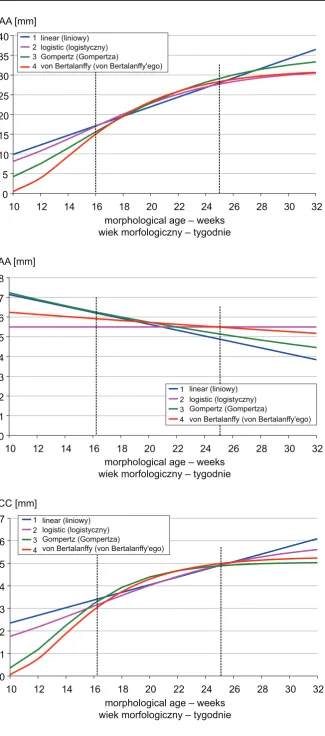
Mean absolute error was used as a measure of the degree to which the theoretical models matched the results obtained. A comparison of the modelsfor the dimensionsanalyzed is presented in Figs. 2–8. Due to the relatively high interindividual variability of pectoralis major muscle linear dimensions, lin-ear regression models seem suitable for describing their growth in weeks 16 to 26 of fetal life (Table 6). The highest growth rates were observed in AC distance (1.24 mm/week), AA distance (1.19 mm/ week) and BC distance (0.91 mm/week). In the ob-served period of fetal life, α and β angle values did not change significantly (p < 0.05). The polynomi-nal model: x = b0 + b1 * t + b2 * t2 provides a good approximation of the muscle area increase; with the parameters b0 = –2442 mm, b1 = 240 mm/week and b2 = –4.86 mm/week2, it explains almost 25% of the variations (Fig. 9). In the material examined, two cases of anomalies in the form of sternal mus-cles were observed (Fig. 10).
Table 3. Comparison of basic statistics (mean ± SD) of features of male and female fetuses, with t-Student test results
Tabela 3. Porównanie podstawowych statystyk (mean ± SD) badanych cech u płodów żeńskich i męskich oraz wyniki testów t-Studenta
Variables
(Zmienne) Female (Płeć żeńska) n = 22
Male (Płeć męska) n = 76
t p
Morphological age – week
(Wiek morfologiczny – tydzień) CRL – mm
(Długość ciała CRL – mm) V-PL – mm
(Długość ciała V-PL – mm) Mass – g
(Masa ciała – g)
21.5 ± 2.1
169 ± 20
247 ± 38
325 ± 113
20.8 ± 1.2
159 ± 24
225 ± 40
271 ± 114
1.403
1.858
2.253
1.949
0.164
0.066
0.027
0.054
AA distance – mm (Odległość AA – mm) BB distance – mm (Odległość BB – mm)
CC distance – mm
(Odległość CC – mm) AE distance – mm (Odległość AE – mm) AB distance – mm (Odległość AB – mm) BC distance – mm (Odległość BC – mm) AC distance – mm (Odległość AC – mm)
28.0 ± 9.0
4.6 ± 3.6
4.4 ± 2.0
14.1 ± 3.9
11.3 ± 4.1
19.6 ± 4.7
27.7 ± 6.4
24.2 ± 7.5
5.8 ± 3.2
4.5 ± 2.1
14.0 ± 3.9
10.2 ± 4.1
18.7 ± 4.3
25.6 ± 6.2
1.995
–1.470
–0.062
0.110
1.085
0.810
1.413
0.049
0.145
0.951
0.912
0.281
0.420
0.161
Area – mm2
(Pole powierzchni – mm2) Angle α – °
(Kąt α – °)
Angle β – °
(Kąt β – °)
476 ± 206
121 ± 24
121 ± 16
426 ± 183
129 ± 19
119 ± 13
1.089
–1.634
0.795
0.279
0.106
Table 4. Comparison of the numerousness (fraction) of pectoralis major muscles of male and female fetuses, divided into subgroups according to topography, with chi-square test results
Tabela 4. Porównanie liczności (frakcji) mięśni piersiowych większych płodów żeńskich i męskich w podgrupach różniących się topografią oraz wyniki testów chi-kwadrat
Topography
(Topografia) PMMs from females (Płeć żeńska) n = 44
PMMs from males (Płeć męska) n = 152
χ2 p
Pars clavicularis absent
(Część obojczykowa nieobecna) 0 (0.0%) 2 (1.3%) 0.008 0.931
Pars sternocostalis absent
(Część mostkowo-żebrowa nieobecna) 0 (0.0%) 0 (0.0%) – –
Pars abdominalis absent
(Część brzuszna nieobecna) 24 (54.5%) 88 (57.9%) 0.008 0.929
Connected with m. deltoideus
(Połączenie z mięśniem naramiennym) 3 (6.8%) 10 (6.6%) 0.083 0.774 Clear trigonum deltoideopectorale
(Czysty trójkąt naramienno-piersiowy) 33 (75.0%) 114 (75.0%) 0.004 0.949
Topography
(Topografia) Female (Płeć żeńska)
n = 22
Male (Płeć męska) n = 76
χ2 p
Clear sulcus interpectoralis
(Czysta bruzda między mięśniami piersiowymi większymi) 18 (81.8%) 62 (81.6%) 0.051 0.821 Superimpose of muscles
(Nakładanie się mięśni) 4 (18.2%) 14 (18.4%) 0.082 0.774
Pars clavicularis: (Część obojczykowa) symmetrical
larger on the left
larger on the right
17 (77.3%) 0 (0.0%) 5 (22.7%)
56 (73.7%) 11 (14.5%) 9 (11.8%)
4.629 0.099
Pars sternocostalis: (Część mostkowo-żebrowa) symmetrical
larger on the left
larger on the right
19 (86.4%) 1 (4.5%) 2 (9.1%)
69 (90.8%) 1 (1.3%) 6 (7.9%)
0.939 0.625
Pars abdominalis: (Część brzuszna) symmetrical
larger on the left
larger on the right
21 (95.5%) 1 (4.5%) 0 (0.0%)
73 (96.1%) 1 (1.3%) 2 (2.6%)
Table 5. PMM size increases over time (t) [weeks]
Tabela 5. Modele wzrastania wymiarów m. pectoralis maior z czasem t [tydzień] Distance L(t)
(Odległość L(t)) (Modele)Models
1. linear 2. logistic 3. gompertz 4. von Bertalanffy AE – mm a = –8.37
b = 1.07
R = 0.5927
A = 21.24
c = 54
K = 0.225
R = 0.5935
A = 22.97
c = 11.42
K = 0.152
R = 0.5941
A = 21.86
c = 3.71
K = 0.162
R = 0.5943
AB – mm a = –7.68
b = 0.89
R = 0.4980
A = 14.79
c = 93
K = 0.264
R = 0.4811
A = 15.45
c = 20.89
K = 0.194
R = 0.4823
A = 14.57
c = 13.38
K = 0.244
R = 0.5824
BC – mm a = –9.67
b = 1.37
R = 0.6776
A = 23.79
c = 279
K = 0.341
R = 0.6902
A = 24.71
c = 49.05
K = 0.254
R = 0.6898
A = 24.16
c = 9.17
K = 0.225
R = 0.6896 AC – mm a = –13.37
b = 1.85
R = 0.6620
A = 32.52
c = 197
K = 0.318
R = 0.6718
A = 33.66
c = 40.12
K = 0.240
R = 0.6720
A = 34.18
c = 7.91
K = 0.215
R = 0.6721
AA – mm a = –2.23
b = 1.21
R = 0.5216
A = 31.50
c = 22
K = 0.203
R = 0.5345
A = 35.61
c = 10.34
K = 0.158
R = 0.5359
A = 31.42
c = 6.00
K = 0.207
R = 0.5352 BB – mm a = 8.64
b = –0.15
R = –0.1923
A = 5.50
c = 0
K = –15
R = –0.1956
A = 0.36
c = –3.25
K = 0.008
R = –0.1962
A = 0.14
c = –2.65
K = 0.004
R = –0.1963 CC – mm a = 0.65
b = 0.17
R = 0.4216
A = 6.03
c = 11.8
K = 0.158
R = 0.4207
A = 5.05
c = 49.8
K = 0.294
R = 0.4228
A = 5.29
c = 9.01
K = 0.245
R = 0.4235
t: morphological age (in weeks), R: coefficient of determination
Fig. 2. Comparison ofmodels for AE distance
Ryc. 2. Porównanie modeli dla analizowanej odległości AE
0 5 10 15 20 25 30
10 12 14 16 18 20 22 24 26 28 30 32
morphological age – weeks wiek morfologiczny – tygodnie AE [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego) 1
Fig. 3. Comparison ofmodels for AB distance
Ryc. 3. Porównanie modeli dla analizowanej odległości AB
Fig. 4. Comparison ofmodels for BC distance
Ryc. 4. Porównanie modeli dla analizowanej odległości BC
Fig. 5. Comparison ofmodels for AC distance
Ryc. 5. Porównanie modeli dla analizowanej odległości AC
0 5 10 15 20 25 30 35 40
10 12 14 16 18 20 22 24 26 28 30 32
BC [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego)
morphological age – weeks wiek morfologiczny – tygodnie
1 2 3 4
0 5 10 15 20 25
10 12 14 16 18 20 22 24 26 28 30 32
morphological age – weeks wiek morfologiczny – tygodnie AB [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego) 4
1 2 3
5 10 15 20 25 30 35 40 45 50
10 12 14 16 18 20 22 24 26 28 30 32
AC [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego) 1
2 3 4
Fig. 6. Comparison ofmodels for AA distance
Ryc. 6. Porównanie modeli dla analizowanej odległości AA
Fig. 7. Comparison ofmodels for BB distance
Ryc. 7. Porównanie modeli dla analizowanej odległości BB
Fig. 8. Comparison ofmodels for CC distance
Ryc. 8. Porównanie modeli dla analizowanej odległości CC
0 1 2 3 4 5 6 7 8
10 12 14 16 18 20 22 24 26 28 30 32
AA [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego) 1
2 3 4
morphological age – weeks wiek morfologiczny – tygodnie 0
5 10 15 20 25 30 35 40
10 12 14 16 18 20 22 24 26 28 30 32
AA [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego)
morphological age – weeks wiek morfologiczny – tygodnie
1 2 3 4
0 1 2 3 4 5 6 7
10 12 14 16 18 20 22 24 26 28 30 32
CC [mm]
linear (liniowy) logistic (logistyczny) Gompertz (Gompertza)
von Bertalanffy (von Bertalanffy'ego) 1
2 3 4
Table 6. Regression models of PMM size increases over time t [weeks]: x = b0 + b1 ×t
Tabela 6. Modele regresyjne wzrastania wymiarów m. pectoralis maior z czasem t [tydzień]: x = b0 + b1 ×t Dimensions x
(Wymiary x) rx,t b0 b1
AE – mm
AB – mm
BC – mm
AC – mm Area F – mm2
(Pole powierzchni F – mm2) Angle α – °
(Kąt α – °)
Angle β – °
(Kąt β – °)
AA Distance
(Odległość między punktami A) BB Distance
(Odległość między punktami B) CC Distance
(Odległość między punktami C)
0.968 0.933 0.979 0.822 0.484
0.120
–0.005
0.958
0.850
0.909
– – – –
–468 (–701 ÷ –235)
127 (124 ÷ 130)
119 (117 ÷ 121)
–
–
–
0.68 (0.65 ÷ 0.70) 0.50 (0.47 ÷ 0.53) 0.91 (0.89 ÷ 0.94) 1.24 (1.20 ÷ 1.28) 43.0 (32.0 ÷ 54.0)
–
–
1.19 (1.12 ÷ 1.27)
0.26 (0.23 ÷ 0.29)
0.21 (0.19 ÷ 0.23)
Fig. 9. Model of increases in muscle area (F) with age (t), with the measurement results in the background
Ryc. 9. Model wzrastania powierzchni mięśnia (F) z wiekiem (t) na tle wyników pomiaru
0 100 200 300 400 500 600 700 800 900 1000
F [mm2]
15 16 17 18 19 20 21 22 23 24 25 26 27
t
Fig. 10. A case of sternal muscle (SM) in the prenatal period
Discussion
The available literature provides mainly de-scriptions of pectoralis major muscles of adult corpses. The paper by Pande and Singh is one of the few publications based on fetal material [11]. Those authors examined ten fetuses of CRL rang-ing from 195 to 290 mm. The prepared them, weighed them and measured the symmetry of the following muscles: the pectoralis major, deltoid, coracobiachialis, triceps, superficial flexors of the forearm and extensors of the forearm; they also ex-amined bones: the humerus, radius and ulna. The total mass of the dissected structures was bigger on the right (dominant) side in nine out of the ten examined fetuses (p < 0.001), but the average pec-toralis major muscle mass in was 137 mg larger on the left side. The authors were not able to explain why their results regarding the PMM differed from others. Chhibber and Singh, in turn, observed that the PMM increased in mass on the dominant side [12]. Other descriptions of PMM morphometry were not found.
The analysis of the material in the current study (two pectoral muscles per fetus) revealed the following features: In two cases (1.02%) there was no clavicular part of the pectoralis major muscle. The sternoclavicular part was found in all fetuses. In 112 cases (57.14%) the ventral part of the muscle was absent. In 13 cases (6.63%), the muscle fiber junction with the delta muscle was detected. Mus-cle absence within the trigonium deltoidepoctoralis was found in 147 cases (75%). In 28 cases (14.2%), muscle fibers overlapped on the sternum. No sig-nificant asymmetry was found in the dimensions of particular parts of the muscle. The influence of individual variations on PMM linear dimensions is so large that a simple linear model is sufficient to describe the size increases in the period from week 16 to week 26. For the same reason, a second degree polynomial can be adopted as a model of muscle area growth.
In two cases in the current study sternal mus-cles were observed on the left side with fibers
run-ning parallel to the sternum (Figure 10).The avail-able literature provides descriptions of numerous morphological variations of sternal muscles [13, 14]. Pojchamarnwiputh et al. observed that the frequency of rare anatomical variations can be estimated as about 8% in both sexes [15]. Harper dissected sternal muscles in three out of six fe-tuses with anencephaly, and in one fetus, sternal muscle was found bilaterally [16]. O’Neill et al. stated that sternal muscle presence in the anterior wall of the thoracic cavity can accompany PMM anomalies [17]. Kabay et al. examined the clinical significance of sternal muscles in mastectomies, and concluded that pre-operational identification of sternal muscles and a topographic description of them can help in making decisions about their potential resection during mastectomies [18]. Bra-dley et al. showed the presence of four sternal mus-cles in the mammographs of 32,000 women, and noted that the superficial location of the muscle favors sporadic mammogram visualization in the form of asymmetric condensation in the median part of the mammary gland [8]. Accessory muscles can be also a source of diagnostic mistakes. In such cases, Bradley et al. suggested CT or MR imaging in order to differentiate muscle from hyperplastic lesions of the mammary gland [8]. Sarıkçıoğlu et al. [19] described a case report of three sternal mus-cles co-existing in a 56-year-old male corpse, two on the left and one on the right side. The authors stated that PMM anomalies required diagnostic procedures so much indispensable in pectoral re-gion surgery.
The authors concluded that pectoralis major muscle size symmetry was observed on the left and right side. No sexual dimorphism was observed. The linear dimensions of the muscle in the exam-ined period (weeks 16 to 26 of fetal life) showed high interpersonal variability, so a linear regression model was used to describe their growth. The area increase was described using a binominal model. No differences were observed between male and female fetuses in terms of the topographic features analyzed.
References
[1] Connell DA, Potter HG, Sherman MF et al.: Injuries of the pectoralis major muscle: evaluation with MR imaging. Radiology 1999, 210, 785–791.
[2] Yamasaki M: Anatomical study on 2 cases of the congenital partial defect of pectoralis major and minor muscles. Anat Anz 1989, 168, 423–432.
[3] Mosconi T, Kamath S: Bilateral asymmetric deficiency of the pectoralis major muscle. Clin Anat 2003, 16, 346– 349.
[4] Marmor L, Bechtol CO, Hall CB: Pectoralis Major Muscle: Function of Sternal Portion and Mechanism of Rup-ture of Normal Muscle: Case Reports. J Bone Joint Surg Am 1961, 43, 81–87.
[5] Loukas M, South G, Louis RG et al.: A case of an anomalous pectoralis major muscle. Folia Morphol 2006, 65(1), 100–103.
[7] Mysnyk MC, Johnson DE: Congenital absence of the pectoralis muscles in two collegiate wrestling champions. Clin Orthop Relat Res 1991, 265, 183–186.
[8] Bradley FM, Hoover HC Jr, Hulka C et al.: The sternalis muscle: an unusual normal finding seen on mammog-raphy. Am J Roentgenol 1996, 166, 33–36.
[9] Kovacević P, Ugrenović S, Kovacević T: Vascularisation of pectoralis maior myocutaneous flap: anatomical study in human fetuses and cadavers. Bosn J Basic Med Sci 2008, 8, 183–187.
[10] Carlson BM: Human embryology and developmental biology. Mosby, St Louis 1999, 450.
[11] Pande BS, Singh I: One-sided dominance in the upper limbs of human fetuses as evidenced by asymmetry in muscle and bone weight. J Anat 1971, 109(3), 457–459.
[12] Chhibber SR, Singh I: Asymmetry in muscle weight in the human upper limbs. Acta Anat 1972, 81(3), 462–465. [13] Demirpolat G, Oktay A, Bilgen I et al.: Mammographic features of the sternalis muscle. Diagn Interv Radiol 2010,
16, 276–278.
[14] Loukas M, Bowers M, Hullett J: Sternalis muscle: a mystery still. Folia Morphol 2004, 63, 147–149.
[15] Pojchamarnwiputh S, Muttarak M, Na-Chiangmai W et al.: Benign breast lesions mimicking carcinoma at mam-mography. Singapore Med J 2007, 48, 958–968.
[16] Harper WF: The Sternalis Muscle in the Anencephalous Foetus. J Anat 1936, 70, 317–320.
[17] O’Neill MN, Folan-Curran J: Case report: bilateral sternalis muscles with a bilateral pectoralis major anomaly. J Anat 1998, 193, 289–292.
[18] Kabay B, Akdogan I, Ozdemir B et al.: The left sternalis muscle variation detected during mastectomy. Folia Morphol 2005, 64, 338–340.
[19] Sarıkçıoğlu L, Demirel DM, Oğuz N, Uçar Y: Three sternalis muscles associated with abnormal attachments of the pectoralis major muscle. Anatomy 2008, 2, 67–71.
Address for correspondence:
Alicja KędziaDepartment of Anatomy Wroclaw Medical University ul. Chałubińskiego 6a 50-368 Wrocław Poland
Tel.: +48 71 784 00 80
E-mail: [email protected]
Conflict of interest: None declared