Monika Bronkowska, Marcin Gołecki
2, Justyna Słomian
1, Anna Markiewicz
1,
Jolanta Mikołajczak
1, Monika Kosacka
2, Irena Porębska
2, Renata Jankowska
2,
Jadwiga Biernat
1Dietary Patterns in Overweight and Obese Subjects
with Obstructive Sleep Apnea
Ocena podaży podstawowych składników odżywczych
oraz grup produktów w całodziennych racjach pokarmowych
otyłych osób z rozpoznanym obturacyjnym bezdechem sennym
1 Division of Human Nutrition, Department of Food Storage and Technology, Wrocław Universityof Environmental and Life Sciences, Poland
2 Lower Silesian Pulmonary Center, Department and Clinic of Pulmonology and Lung Cancers, Wrocław Medical University, Poland
Abstract
Objectives. The aim of the study was to evaluate selected nutrients and food product groups in the daily food intake of obese patients diagnosed with obstructive sleep apnea (OSA).
Material and Methods. The eating habits of 93 patients, including 22 women and 71 men, were evaluated from 2006 to 2008. The 72-hour dietary recall method and diet history were used to evaluate dietary intake.
Results. The study showed that the food intake of women and men differ greatly with regard to the individual supply of energy and major nutrients. Analyses demonstrated an incorrect diet structure in patients with OSA in terms of the percentages of energy derived from fats, protein and carbohydrates. In the average food ration of the men and women surveyed the percentages of energy derived from fat, protein and carbohydrates reached 37%, 17.5% and 46.8–50.2% respectively. The analyzed diets were found to include a high percentage of meat and meat products, as well as of eggs. The diets were also characterized by a low content of cereal products, vegetables, fruits, milk and dairy products. The study also involved determining BMI values for all the patients under scrutiny. The entire surveyed group of patients diagnosed with OSA was characterized by incorrect BMI values.
Conclusions. The mean energy intake of the surveyed patients with OSA was close to the recommended healthy level, yet its dietary structure is incorrect (Adv Clin Exp Med 2010, 19, 6, 709–719).
Key words: obstructive sleep apnea, selected nutrients, daily food rations, obese patients.
Streszczenie
Cel pracy. Ocena podaży podstawowych składników odżywczych oraz grup produktów w całodziennych racjach pokarmowych otyłych osób z rozpoznanym obturacyjnym bezdechem śródsennym. Badania przeprowadzono w grupie 22 kobiet oraz 71 mężczyzn.
Wyniki. Na podstawie analizy ilościowej wykazano duże zróżnicowanie w indywidualnej podaży energii oraz głównych składników odżywczych. Stwierdzono także niewłaściwą strukturę diet chorych na OBS pod względem procentowego udziału energii pochodzącej z białka, tłuszczu i węglowodanów. W średniej racji pokarmowej bada-nych kobiet i mężczyzn udział energii pochodzącej z tłuszczu, białka i węglowodanów wynosił odpowiednio 37; 17,5 i 46,8–50,2%. W ocenie ilościowej oszacowano także spożycie poszczególnych grup produktów spożywczych. Wykazano duży udział w diecie mięsa i jego przetworów, jaj, innych tłuszczów, a mały warzyw, owoców, produk-tów zbożowych oraz mleka i jego przetworów. Badanej grupie obliczono także wskaźnik BMI. Wśród badanych osób żadna nie charakteryzowała się prawidłowym wskaźnikiem BMI (Adv Clin Exp Med 2010, 19, 6, 709–719).
Słowa kluczowe: obturacyjny bezdech senny, składniki odżywcze, całodzienne racje pokarmowe. Adv Clin Exp Med 2010, 19, 6, 709–719
ISSN 1230-025X
ORIGINAL PAPERS
Rational nutrition is a fundamental determi-nant of health status. Understood as supplying a person with energy and all nutrients, it allows vitality to be maintained for years. It is also an indispensable element in the prevention of many chronic noninfectious diseases, including athero-sclerosis, diabetes, hypertension, obstructive sleep apnea and obesity.
In the last thirty years studies have demon-strated a close relationship between obesity and breathing disorders (dyspnea) during sleep. Epi-demiologically, the key risk factor for the obstruc-tive sleep apnea syndrome (OSA syndrome) is obesity. The occurrence of organic complications that result independently from both obesity and the apnea syndrome points to the strength of that relationship [1–3]
The incidence of sleep apnea in obese per-sons is higher than in the population as a whole. It seems to have been proven that the simultaneous occurrence of obesity and the OSA syndrome is a special risk factor in the development of arterial hypertension [4].
Obstructive sleep apnea is the most frequently occurring syndrome among breathing disorders during sleep. The recent growing interest in that disease has been mainly due to its negative impact on human health. In Poland, research on the OSA syndrome has been sparse. In one epidemiological study, the incidence of the sleep apnea syndrome was shown to be higher in men than in women between the ages of 40 and 70 years [5]. The pres-ent study was aimed at evaluating the eating habits of obese patients diagnosed with obstructive sleep apnea, with consideration given to food product groups in their daily food intake.
Material and Methods
From 2006 to 2008, the eating habits of 93 patients, including 22 women and 71 men were evaluated; all the patients had been diagnosed with OSA and were being treated at the Lower Silesian Pulmonary Center in Wrocław, Poland. Food in-take assessment was carried out on data collected using the 72-hour recall method. In the quantita-tive evaluation, use was made of the “Photo Album of Products and Dishes” elaborated at the Nation-al Food and Nutrition Institute [6]. Food rations were analyzed with “Energia v. 2” software, con-taining a database created by the authors based on “Tables of the Nutritional Value of Chosen Food Products” [7]and “The Composition and Nutritive Value of Dishes” [8], setting forth the energy value and levels of 11 nutrients (energy, total protein, plant-derived protein, animal-derived protein,
to-tal carbohydrates, dietary fiber, toto-tal fats, saturated fatty acids, monounsaturated fatty acids, polyun-saturated fatty acids, cholesterol, Keys index).
Assessment of the eating habits of the partici-pating patients was carried out using Polish rec-ommendations [9] in the weighted form, taking into account the respective percentages of women and men aged between 26 and 60 and those over 60 years of age. The authors adopted the recom-mendations of WHO [10] and national publica-tions [11] regarding the intake of fatty acids: the recommended percentage of total energy intake derived from saturated fatty acids (SFA) should be 8%; from monounsaturated fatty acids (MUFA) 11%; and from polyunsaturated fatty acids (PU-FA) 6%.
The Keys index of diet atherogenicity was cal-culated from the formula [1.35 × (2 ×%en. from SFA –%en. from PUFA) + 1.5 × √cholesterol mg/1000 kcal] [12]. The results are presented in Tables 1 and 2 in the form of mean value, median, standard deviation as well as maximal and mini-mal values. The results obtained were divided ac-cording to the percent of correspondence with the recommendations in the health-promoting model, i.e. ranges of 0–30%, 30–50%, 50–70%, 70–90%, 90–110%, 110–130% and over 130%; with the 90–110% range acknowledged as appropriate and consistent with recommendations.
Calculations of groups of food products in in-dividual diets were also performed using “Energia v. 2” software with the database described above. The patients’ consumption of groups of food prod-ucts (g/day) in the weighted form was compared with the model food rations proposed by Turlejs-ka [13], whose recommendations are presented in terms of the main products in a given group [13]. The calculations were based on the following con-version factors: 100 g of flour was assumed to cor-respond to 135 g of bread; 100 ml of milk to 10 g of aged cheese and 15 g of fresh white cheese; and 100 g of meat to 70 g of cured meat products [13].
BMI was assessed on the basis of the height and weight of the respondents.
On account of the group’s diversity, the results obtained for women and men were not subjected to statistical analyses.
Results and Discussion
disorder was observed in 59.2% of the patients; a moderate degree in 30.6%, and a mild degree in 10.2%. For 73.5% of the subjects, it was the first hospital stay linked with OSA treatment; for 22.4% of the group it had been less than six months since the last hospitalization.
In the population surveyed, 51% of the people originated from a city; 22.4% were from a town with fewer than 50,000 inhabitants; and 26.5% were from rural areas. Over half the patients (55.1%) lived with their spouses and children; the rate among men was higher (67.6%).
In terms of education, the surveyed population was diversified: 4.1% had only primary education; 22.4% had vocational education; 51.0% had sec-ondary education; and 22.4% had higher educa-tion. A majority of the women surveyed (58.3%) and close to half the men (48.6%) had secondary education.
Among the patients examined, 49% were living on a retirement pension. The majority of the wom-en (66.7%) were retiremwom-ent/social pwom-ensioners, and 25% did not work. Among the men, 21.6% were white-collar workers, and 13.5% had light physi-cal jobs. In addition, 10.8% of the male group were persons running their own small businesses.
In the case of 75.0% of the women and 91.9% of the men, OSA treatment was being conducted by means of the CPAP method – the most com-mon, non-invasive and highly effective method used to eliminate apnea, using devices that gener-ate positive air pressure in the respiratory airways. Weight reduction was recommended for all the patients.
A lack of irregularities in rest metabolism and thermogenesis observed in conjunction with OSA indicates that, apart from physiological factors, an increase in body mass since the appearance of OSA symptoms is likely to result from patients’ improper lifestyle – e.g. a syndrome of compul-sive food consumption during night awakenings, and low physical activity connected with (among other things) feeling of drowsiness and stress [14]. It may be concluded, therefore, that in this group of patients the high incidence of overweight and obesity is affected to a great extent by improper eating habits. For these patients, in the process of both losing weight and maintaining a reduced body mass, properly balancing the diet in terms of the levels of particular nutrients is of the outmost significance [15].
The study indicated that the food rations of women and men differ greatly in terms of energy supply and the levels of major nutrients. The mean energy value of the diets of women with OSA was lower than the Recommended Dietary Allowances (RDA), i.e. 73.1% (Table 1). A slightly higher
en-ergy value was found in the men’s group: 82.2% of the RDA (Table 2). An assessment of the patients’ diets in relation to the recommended norms re-vealed that only 17.8% of women and 19.8% of the men were in the correct range (90–110%) of the RDA for energy intake. In 43.7% of the women’s diets and 39.7% of the men’s, analyses revealed en-ergy deficiencies at levels from 50% to 90% of the RDA (Tables 3 and 4).
It has been claimed that persons consuming high-energy diets are especially at risk of developing overweight and obesity [16]. In the current study, an excessive energy supply – over 110% of the RDA – was observed in 12.6% of the women’s diets (Ta-ble 3) and in 31.8% of the men’s (Ta(Ta-ble 4).
Energy intake close to the current RDA (84.5%) was also demonstrated in a survey con-ducted in 2001 (the Pol–MONICA BIS study) in Warsaw and the former Tarnobrzeskie Province (Poland) [17]. The energy value of the food rations of women and men were1702 kcal and 1865.4 kcal respectively, and were similar to the findings of the current study.
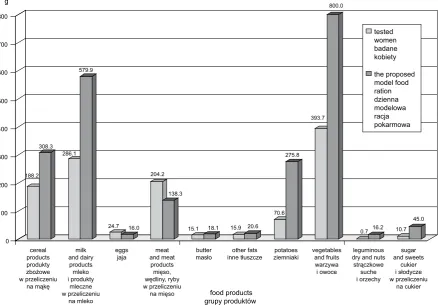
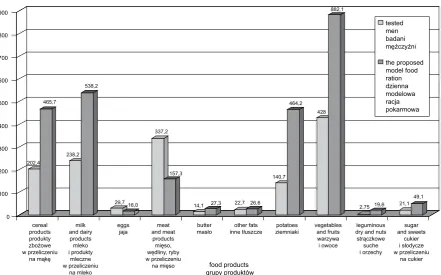
Despite the excessive supply of meat and meat products (women: 147.6% of the RDA, men: 214.4% of the RDA) and eggs (women: 154.4% of the RDA, men: 185.6% of the RDA) demonstrated in the study, the high energy value of the patients’ diets was additionally affected by a low intake of other food groups (Fig. 1 and 2).
Analyses revealed an incorrect diet structure among patients with OSA in terms of the percent-age of energy derived from protein, fats and car-bohydrates. In the case of obese people, the high contribution of energy derived from fats was espe-cially unfavorable: In both the women’s and men’s groups it was approximately 37%, as compared to the recommended level of 25%. The average diet of the men and women surveyed was also character-ized by a low level of energy from carbohydrates: 46.8–50.2%. Incorrect values were also demon-strated with respect to protein-derived energy, which was too high in both groups in the study, reaching 17.5%.
Table 3. Diets eaten by overweight and obese women diagnosed with obstructive sleep apnea (n = 22) compared to the recommended daily values of energy and nutrients
Tabela 3. Podział racji pokarmowych otyłych kobiet z rozpoznanym obturacyjnym bezdechem sennym (n = 22) na frakcje procentowej realizacji zaleceń na energię i składniki odżywcze [%]
% group 0–30 30–50 50–70 70–90 90–110 110–130 > 130 Energy [kcal]
(Wartość energetyczna [kcal]) % group 5.0 20.9 17.8 25.9 17.8 12.6 0
Total protein [g]
(Białko ogółem [g]) % group 4.2 15.0 5.0 21.7 17.5 14.2 22.4
Plant-derived protein [g]
(Białko roślinne [g]) % group 4.2 13.3 44.2 5.0 9.2 9.2 15.0
Animal-derived protein [g]
(Białko zwierzęce [g]) % group 4.2 10.0 15.0 10.0 10.0 9.2 41.6
Total carbohydrates [g]
(Węglowodany ogółem [g]) % group 10.0 37.5 14.2 21.6 8.3 4.2 4.2
Dietary fiber [g]
(Błonnik pokarmowy [g]) % group 20.0 37.7 26.7 5.2 5.2 5.2 0
Total fats [g]
(Tłuszcze ogółem [g]) % group 5.0 5.0 10.0 18.3 13.4 8.3 40.0
Saturated fatty acids [g]
(Nasycone kwasy tłuszczowe [g]) % group 0 0 10.0 9.4 9.2 22.3 49.1
Monounsaturated fatty acids [g]
(Jednonienasycone kwasy tłuszczowe [g]) % group 5.0 10.0 36.2 15.5 4.2 17.2 12.5 Polyunsaturated fatty acids [g]
(Wielonienasycone kwasy tłuszczowe [g]) % group 15.0 17.5 9.2 19.2 13.3 9.2 16.0 Cholesterol [mg]
(Cholesterol [mg]) % group 5.0 41.7 9.2 13.3 9.2 8.3 13.3
In the current study of OSA patients, analy-ses showed an excessive intake of fat among the women and men: 107.3% and 122.81% of the RDA respectively (Tables 1 and 2). Similar findings were also obtained when evaluating the patients’ food ra-tions in terms of meeting the RDA for the intake of fat (Tables 3 and 4). In 48.3% of the food rations of the women and 65.9% of the men’s, assays demon-strated an excessive supply of fat; in 40% of the food rations of women and 57.7% of the men’s, fat intake exceeded 130% of the RDA (Tables 3 and 4).
The diets of the patients studied were also char-acterized by a very high supply of saturated fatty acids (SFA). A higher intake of SFA was found in the women’s group: 129.3% of the RDA (Table 1). Among the men, the intake of saturated fatty acids was slightly lower, accounting for 129% of the rec-ommended level (Table 2). The analysis of the pa-tients’ diets in relation to the RDA showed that only a negligible percentage of the women’s food rations (9.2%) were at a correct level (90–110%) of the rec-ommended dietary allowances for SFA, whereas 71.4% were at a level exceeding 110% of the RDA (Table 3). Corresponding results were recorded
in the men’s group: In 74.4% of diets, the supply of SFA was over 110% of the recommended level (Table 4). A similar intake of saturated fatty acids – i.e. from 12 to 16% of the daily energy supply – has been observed in Greece [19] and Spain [20].
Excessive intake of saturated fatty acids inten-sifies hyperinsulinemia and consequently insulin resistance and hyperglycemia, thus contributing to an increasing body mass [21].
The high supply of SFA and excessive intake of cholesterol demonstrated in the diets of patients diagnosed with OSA resulted mainly from high consumption of meat, meat products and eggs. High consumption of meat, meat products and eggs was higher in the men’s diets (214.4% of the recommended level) than in the women’s (147.6%) (Figures 1 and 2). This is undoubtedly due to the incorrect nutritional habits that often observed in Polish families as well as to a preference for high-fat meat products.
Analyses demonstrated that butter contrib-uted little to the levels of SFA and cholesterol in the diets of patients suffering from OSA (Figures 1 and 2).
The level of monounsaturated fatty acids (MUFA) in the diets of the surveyed patients was correct, accounting for 91.7% and 111.3% of the recommended levels in the case of women and men, respectively (Tables 1 and 2). However, only 4.2% of the women and 22.2% of the men were meeting the recommended allowances at a level of 90–110%, whereas in 66.7% of the women’s diets and 36.2% of the men’s the supply of MUFA was
lower than 90% of the recommended level (Tables 3 and 4).
In a work evaluating the nutritive value of diets in the Wielkopolska Province (Poland), Przysławski et al. [22] reported a similar intake of monounsaturated fatty acid as in the current study (13–14% of energy intake).
Assessments of the daily food rations of the patients with OSA demonstrated a very high di-versity in the intake of polyunsaturated fatty acids, i.e. from 3.1 to 17.3 g/day in the women’s group (Table 1) and from 1.5 to 36.6 g/day in the men’s group (Table 2). The mean intake of PUFA in the daily diet was 83.5% of the recommended level among the women and 90.7% of the recommended level among the men (Tables 1 and 2). The analysis of the diets showed that 13.3% of the women and 14.1% of the men were meeting the recommended allowances at a level of 90–110%, while 60.9% of the women and 44.9% of the men had PUFA in-take levels below 90% of the recommended level (Tables 3 and 4). In the aforementioned study of diets in the Wielkopolska Province, Przysławski et al. [22] found a similar percentage of
polyun-Table 4. Diets eaten by overweight and obese men diagnosed with obstructive sleep apnea (n = 71) compared to the recom-mended daily values of energy and nutrients
Tabela 4. Podział racji pokarmowych otyłych mężczyzn z rozpoznanym obturacyjnym bezdechem sennym (n = 71) na frak-cje procentowej realizacji zaleceń na energię i składniki odżywcze [%]
% group 0–30 30–50 50–70 70–90 90–110 110–130 > 130 Energy [kcal]
(Wartość energetyczna [kcal]) % group 2.8 5.9 17.2 22.5 19.8 21.9 9.9
Total protein [g]
(Białko ogółem [g]) % group 0 1.5 5.7 14.0 19.6 11.1 48.1
Plant-derived protein [g]
(Białko roślinne [g]) % group 8.7 29.6 36.6 12.7 5.5 1.4 5.5
Animal-derived protein [g]
(Białko zwierzęce [g]) % group 1.4 0 2.8 1.4 2.8 1.4 90.2
Total carbohydrates [g]
(Węglowodany ogółem [g]) % group 5.8 27.2 24.4 20.7 10.9 8.2 2.8
Dietary fiber [g]
(Błonnik pokarmowy [g]) % group 17.5 30.5 21.9 12.4 8.2 6.8 2.7
Total fats [g]
(Tłuszcze ogółem [g]) % group 4.3 2.9 2.8 12.8 11.3 8.2 57.7
Saturated fatty acids [g]
(Nasycone kwasy tłuszczowe [g]) % group 1.4 7.0 11.3 1.5 4.4 16.6 57.8
Monounsaturated fatty acids [g]
(Jednonienasycone kwasy tłuszczowe [g]) % group 5.8 7.1 9.5 13.8 22.2 8.4 33.2 Polyunsaturated fatty acids [g]
(Wielonienasycone kwasy tłuszczowe [g]) % group 8.6 5.6 12.5 18.2 14.1 10.1 30.9 Cholesterol [mg]
saturated fatty acids (PUFA) to the finding in the current study (4.1% and 5.2% of total energy, re-spectively).
It was observed that in the group of patients investigated, the source of MUFA and PUFA were soft margarines used for spreading on bread, and oils.
The total protein intake was found to be high among both the women and men in the study: 106.2 and 119.9% of the RDA, respectively. Only 17.5% of the women and 19.6% of the men had protein intake in the range of 90–110% of the RDA, while 33.6% of the women and 59.2% of the men exceeded 110% of the recommended level of protein (Tables 3 and 4).
In the diets of both groups the predominat-ing protein was that of animal origin – over 110% of the recommended level was found in at least 50.8–91.6% of the food rations of both women and men (Tables 3 and 4). In addition, it was observed that only 2.8% of the men in the study had animal-derived protein intake levels within the range of 90–110% of the recommended level (Table 4).
The supply of protein of plant origin in the average diet of both groups was below the
rec-ommended allowance: 87.1% of the RDA among the women (Table 1) and 99% among the men (Table 2).
The high intake of protein was attributed to the high consumption of meat, cured meat products and eggs by the surveyed patients. Simultaneous-ly, insufficient amounts of plant products in their diets – cereal products, legumes and vegetables – meant that the contribution of animal protein to the pool of total protein was substantially higher than the adopted recommended values (Figures 1 and 2).
A high supply of total protein – 86.7 g – and animal protein in particular was also observed in a study by Grygiel et al. in the daily food rations of women with visceral obesity [23]. A high protein intake has also been observed in a number of other countries, e.g. in Greece (13.2%) [19] and Brazil (14.2%) [24].
The results of the WOBASZ survey [25] exam-ining the quality of nutrition in the Polish popula-tion indicated that as few as 48.5% of women and 49.5% of men were complying with recommended allowances for the supply of energy derived from protein. The other half of the population had
pro-Fig. 1. Groups of food products in the daily food rations of overweight and obese women diagnosed with obstructive sleep apnea (n = 22) compared with the proposed model diet
Ryc. 1. Grupy produktów w racjach pokarmowych otyłych kobiet z rozpoznanym obturacyjnym bezdechem śródsennym (n = 22) w porównaniu z dzienną modelową racją pokarmową
188.2 308.3
286.1 579.9
24.7 16.0
204.2
138.3
15.1 18.1 15.9 20.6
70.6 275.8
393.7 800.0
0.7 16.2 10.7
45.0
0 100 200 300 400 500 600 700 800 g
cereal products produkty zbożowe w przeliczeniu
na mąkę
milk and dairy
products mleko i produkty
mleczne w przeliczeniu
na mleko
eggs
jaja and meatmeat
products mięso, wędliny, ryby w przeliczeniu
na mięso
butter
masło inne tłuszczeother fats ziemniakipotatoes vegetablesand fruits warzywa
i owoce
leguminous dry and nuts strączkowe
suche i orzechy
sugar and sweets
cukier i słodycze w przeliczeniu
na cukier food products
grupy produktów
tested women badane kobiety
tein intake levels that were either excessive or defi-cient. Similar protein levels were also observed in other works [26–28].
The evaluation of daily food rations of the women and men surveyed in the current study demonstrated considerable deviations from the adopted recommended allowances for carbohy-drates (Tables 1 and 2). The mean carbohydrate intake in the diets of the women and men were 58.3–61,1% of the recommended level. In addi-tion, it was found that in 83.3% of the women’s diets and 78.1% of the men’s, the level of carbohy-drates was below 90% of the recommended dietary allowances (Tables 3 and 4).
It was found that the insufficient supply of carbohydrates was accompanied by an inadequate intake of dietary fiber (Tables 1 and 2). Among the women, the average dietary fiber intake was at 58.8% of the recommended level, and the fiber intake levels of 37.7% of them were 30–50% of the RDA (Table 3). Higher fiber intake was found in diets of men: The average was 60.7% of the recom-mended level, and 8.2% of them had fiber intake levels within the correct range of 90–110% of the RDA (Table 4). The low levels of carbohydrates and dietary fiber in the food rations of the patients with OSA was observed to result from low
con-sumption of cereals, fruits and vegetables, pota-toes, legumes and nuts.
In the entire surveyed population, the analyses also indicated a low intake of sugar and sweets, not exceeding 43% of the level recommended in the model daily food ration (Figs. 1 and 2).
Excessive consumption of fats, proteins and cholesterol and a simultaneously low supply of carbohydrates and dietary fiber was also observed in the diets of obese women and men aged 18–69 years surveyed in a study conducted by Ostrowska et al. [21].
Investigations point to insufficient intake of dietary fiber in practically all age groups of the Pol-ish population. This results from low consumption not only of vegetables and fruits, but also of coarse-grained cereal products, groats and legumes [29].
The survey conducted also included a deter-mination of the atherogenicity of the patients’ diets, calculated by means of the Keys index. The mean value of that index the diets of the women and men examined was higher than that recom-mended in the Recomrecom-mended Dietary Allow-ances: 42.2 among the women (127.9% of recom-mended value) and 48.4 among the men (156.1% of recommended value) (Tables 1 and 2). Other authors’ investigations confirm that the diets of
Fig. 2. Groups of food products in the daily food rations of overweight and obese men diagnosed with obstructive sleep apnea (n = 71) compared with the proposed model diet
Ryc. 2. Grupy produktów w racjach pokarmowych otyłych mężczyzn z rozpoznanym obturacyjnym bezdechem śródsennym (n = 71) w porównaniu z dzienną modelową racją pokarmową
202,4 465,7
238,2 538,2
29,7 16,0 337,2
157,3
14,1 27,3 22,7 26,6 140,7
464,2 428
882,1
2,75 19,8 21,1 49,1
0 100 200 300 400 500 600 700 800 900 g
cereal products produkty zbożowe w przeliczeniu
na mąkę
milk and dairy products mleko i produkty
mleczne w przeliczeniu
na mleko
eggs
jaja and meatmeat
products mięso, wędliny, ryby w przeliczeniu na mięso
butter
masło inne tłuszczeother fats ziemniakipotatoes vegetablesand fruits warzywa
i owoce
leguminous dry and nuts
strączkowe suche i orzechy
sugar and sweets
cukier i słodycze w przeliczeniu
na cukier food products
grupy produktów
tested men badani mężczyźni
different populations in Poland are characterized by considerable atherogenicity: The mean Keys index in the diets of women from Wrocław and Legnica was 38.5, and that of women from Kraków was 41.9. A similar tendency has been observed in diets of the Polish men [30–31].
The current study also determined BMI values for all the participating patients. BMI values indic-ative of overweight – i.e. 24.9–29.9 – were reported in 16.7% of the surveyed women and 13.5% of the men. BMI values indicative of obesity – over 29.9 – were found in 83.3% of the women and 86.5% of the men. Investigations conducted among resi-dents of Lublin, Poland, (n = 1214) found over-weight in 37.3% of the respondents and obesity in 25.6%.In a survey carried out under the CINDI WHO program amongst residents of Łódź, Po-land, overweight was reported in 30.5% and obe-sity in 9% of the respondents [32].
The authors concluded that:
1. The mean energy intake among the OSA patients surveyed in the current study was on the
border of the level in the adopted Recommended Dietary Allowances, yet its dietary structure was incorrect. Analyses demonstrated an excessive level of energy derived from fats and proteins, and a low level of energy derived from carbohydrates.
2. Analyses also demonstrated insufficient levels of plant-derived protein and dietary fiber in the patients’ daily food ration.
3. The average diet of the participants in the study was characterized by high atherogenicity resulting from excessive intake of saturated fatty acids.
4. Analyses of the participants’ diets showed a high intake of meat, meat products and eggs. The diets were also characterized by low levels of cereal products, vegetables, fruits, milk and dairy products.
5. The OSA study group is characterized by abnormal BMI values.
The experimental procedure was approved by the Commission of Bioethics at Wroclaw Medical University (KB-28/2008).
References
[1] Wolk R, Kara T, Komers VK: Sleep-disordered breathing and cardiovascular disease. Circulation 2003, 108, 9–12.
[2] Young T, Finn L, Austin D, Peterson A: Menopausal status and sleep-disordered breathing in the Wisconsin Subject Cohort Study. Am Resp Care Med 1995, 152, 1946–1949.
[3] Zieliński J, Pływaczewski R, Bednarek M: Zaburzenia oddychania w czasie snu. Wydawnictwo Lekarskie PZWL, Warszawa 2006.
[4] Regulski M: Zaburzenia oddychania w czasie snu u pacjentów z cukrzycą. Przew Lek 2003, 11/12, 11–17.
[5] Bielicki P, Byśkiniewicz K, Chazan R: Rodzinne występowanie obturacyjnego bezdechu podczas snu. Pneum Alerg Pol 2007, 75, supl. 1, 20–22.
[6] Szponar L, Wolnicka K, Rychlik E: Album fotografii produktów i potraw. IŻŻ, Warszawa 2000.
[7] Kunachowicz H, Nadolna I, Przygoda B, Iwanow K: Tabele wartości odżywczej produktów spożywczych. Prace IŻŻ, nr 85, Warszawa, 1998.
[8] Nadolna I, Kunachowicz H, Iwanow K: Potrawy – skład i wartość odżywcza. Prace IŻŻ, Warszawa, 1994.
[9] Ziemlański Ś: Normy żywienia człowieka. Fizjologiczne podstawy.PZWL, Warszawa 2001.
[10] World Health Organization, Diet, nutrition and the prevention of chronic disease. Report of joint WHO/FAO Expert Consultation. Technical Report Series, No 916, Geneva 2003.
[11] Paradowski L, Kempiński R: Nutrition and chronic diseases of developed communities. Adv Clin Exp Med 2003, 12, supl. 1, 109–116.
[12] Rywik S, Broda G: Stan zdrowia ludności Warszawy w roku 2001. Inst Kardiol, Warszawa 2002.
[13] Turlejska H, Pelznar U, Szponar L, Konecka-Maryjek E: Zasady racjonalnego żywienia – zalecane racje pokar-mowe dla wybranych grup ludności w zakładach żywienia zbiorowego. ODiDK Sp. z o.o., Gdańsk 2004.
[14] Traviss KA, Barr SI, Fleming JA, Ryan CF: Lifestyle – related weight gain in obese men with newly dignosed obstructive sleep apnea. J Am Diet Assoc 2002, 102, 5: 703–706.
[15] Ostrowska L, Stefańska E, Czapska D, Karczewski J: Ocena dziennych racji pokarmowych grupy osób z nadwagą i otyłością. Bromat Chem Toksykol 2003, 36, 2: 123–130.
[16] Niedworok E, Całyniuk B, Szczepańska E, Żurawińska T, Dul L: Struktura spożycia wybranych składników odżywczych w dwóch grupach wiekowych kobiet w aspekcie wystąpienia otyłości. Bromat Chem Toksykol 2003, supl.: 89–92.
[17] Rywik S, Broda G: Stan zdrowia ludności byłego województwa tarnobrzeskiego w roku 2001. Inst. Kardiol., Warszawa 2002.
[18] Przysławski J, Grygiel B: Estimation of nutrition manner of obese women perimenopausal and postmenopausal period. Żyw Człow Metab 2003, 30, 127–132.
[19] Moschandreas J, Kafatos A: Food and nutrient intakes of Greek (Cretan) adults. Recent data for food-based dietary guidelines in Greece. B J Nutr 1999, 81, Suppl. 2, S71–S76.
[21] Ostrowska L, Stefańska E, Czapska D, Karczewski J: Wpływ żywienia osób z nadwagą lub otyłością na ich param-etry lipidowe i gospodarkę węglowodanową. Bromat Chem Toksykol 2003, supl.: 201–206.
[22] Przysławski J, Gertig H, Bolesławska I, Duda G, Maruszewska M, Nowak J: Nutritional value of diets reconsti-tuted in laboratory of workers employed in public or private sector in the Wielkopolska region. Żyw Człow Metab 1999, 26, 99–110.
[23] Grygiel B, Przysławski J, Schlegel-Zawadzka M: Ocena poziomu spożycia białka oraz wybranych witamin z grupy B, u kobiet z otyłością wisceralną i gynoidalną. Bromat Chem Toksykol 2005, supl.: 533–537.
[24] Fraire RD, Carloso MA, Shinzato AR, Ferreira SR: Nutritional status of Japanese-Brazilian subjects: compari-sion across gender and generation. B J Nutr 2003, 89, 705–712.
[25] Waśkiewicz A, Piotrowski W, Sygnowska E, Broda G, Drygas W, Zdrojewski T, Kozakiewicz K, Tykarski A, Biela U: Quality of nutrition and health knowledge in subjects with diagnosed cardiovascular diseases in the Polish population – National Multicentre Health Survey (WOBASZ). Kardiol Pol 2008, 66, 507–513.
[26] Bronkowska M, Żechałko-Czajkowska A: Nutritional patterns of 40-year-old women from Wrocław in the aspect of the risk of Cardiovascular diseases. Part I. Intake of selected nutrients and groups of food products. Pol J Food Nutr Sci 2006, 15/56, 1, 83–90.
[27] Bronkowska M, Wyka J, Żechałko-Czajkowska A: Zastosowanie analizy skupień w ocenie sposobu żywienia i stanu zdrowia dorosłych mieszkańców Wrocławia. Ann Acad Med Siles 2006, 60, suppl. 95, 12–22.
[28] Zahorska-Markiewicz B: Otyłość. Poradnik dla lekarzy. Wydawnictwo Archi-Plus, Warszawa 2007.
[29] Przysławski J, Gertig H: Żywieniowe czynniki rozwoju niektórych chorób cywilizacyjnych. Żyw Człow Metab 1997, 24, 3, 354–365.
[30] Ilow R, Regulska-Ilow B, Szymczak J: Ocena sposobu żywienia kobiet z Legnicy i okolic. Cz. II. Ocena ilościowa. Bromat Chem Toksykol 1998, 31, 1, 55–60.
[31] Piórecka B, Jagielski P, Żwirska J, Piskorz A, Brzostek T, Schlegel-Zawadzka M: Wpływ żywienia na występowanie wybranych metabolicznych czynników ryzyka chorób układu krążenia wśród mieszkanek Krakowa. Rocz PZH 2007, 58, 1, 119–127.
[32] Kornacewicz-Jach Z, Przybycień K, Chomicz J, Pieczul-Mróz, Karwat B, Gorący J: Zagrożenie chorobami układu krążenia u kobiet. Przegl Menopauz 2003, 5, 17–26.
Address for correspondence:
Monika Bronkowska Division of Human Nutrition
Department of Food Storage and Technology
Wrocław University of Environmental and Life Sciences Norwida 25
50-375 Wrocław Poland
E-mail: [email protected]
Conflict of interest: None declared