R E V I E W
Open Access
The accuracy of emergency weight
estimation systems in children
—
a
systematic review and meta-analysis
Mike Wells
1,2*, Lara Nicole Goldstein
1and Alison Bentley
1Abstract
The safe and effective administration of fluids and medications during the management of medical emergencies in
children depends on an appropriately determined dose, based on body weight. Weight can often not be measured
in these circumstances and a convenient, quick and accurate method of weight estimation is required. Most methods
in current use are not accurate enough, but the newer length-based, habitus-modified (two-dimensional) systems have
shown significantly higher accuracy. This meta-analysis evaluated the accuracy of weight estimation systems in children.
Articles were screened for inclusion into two study arms: to determine an appropriate accuracy target for weight
estimation systems; and to evaluate the accuracy of existing systems using standard meta-analysis techniques. There was
no evidence found to support any specific goal of accuracy. Based on the findings of this study, a proposed minimum
accuracy of 70% of estimations within 10% of actual weight (PW10 > 70%), and 95% within 20% of actual weight
(PW20 > 95%) should be demonstrated by a weight estimation system before being considered to be accurate. In the
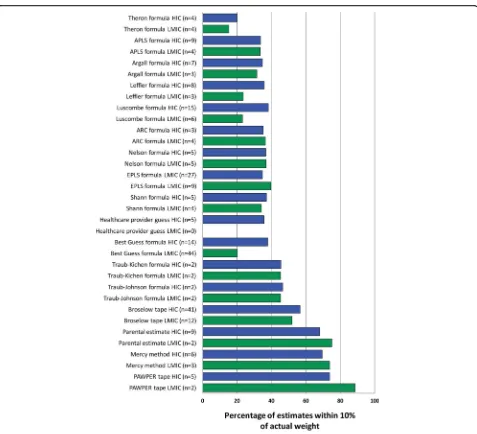
meta-analysis, the two-dimensional systems performed best. The Mercy method (PW10 70.9%, PW20 95.3%), the PAWPER
tape (PW10 78.0%, PW20 96.6%) and parental estimates (PW10 69.8%, PW20 87.1%) were the most accurate systems
investigated, with the Broselow tape (PW10 55.6%, PW20 81.2%) achieving a lesser accuracy. Age-based estimates
achieved a very low accuracy. Age- and length-based systems had a substantial difference in over- and underestimation
of weight in high-income and low- and middle-income populations. A benchmark for minimum accuracy is
recommended for weight estimation studies and a PW10 > 70% with PW20 > 95% is suggested. The Mercy method, the
PAWPER tape and parental estimates were the most accurate weight estimation systems followed by length-based and
age-based systems. The use of age-based formulas should be abandoned because of their poor accuracy.
Keywords:
Weight estimation, Broselow tape, PAWPER tape, Mercy method
Introduction
It cannot be considered to be good medical practice to
use a weight estimation system that is known to be
in-accurate [1]. When children
’
s weight cannot be
mea-sured during emergency care, an accurate, rapid
estimation of weight is needed, as the safety and
effect-iveness of emergent interventions may ultimately depend
on the accuracy of the weight estimation [2, 3]. Since
most drug doses in children are based on weight, an
ac-curate estimation of weight is important to ensure that a
correct amount of medication is administered to achieve
the desired effect, as well as to prevent the potential
complications and side-effects of overdosing [4, 5]. This
is relevant because most paediatric medication errors
occur in the Emergency Department and most cases of
resultant patient harm are related to incorrect dosing
[6
–
8].
The problem is that most contemporary methods used
to estimate children
’
s weight have been shown to lack
sufficient accuracy and consistency of performance in
different populations [9]. Most existing weight
estima-tion systems are
“
one-dimensional
”
, because a single
variable, usually age or length, is used in the weight
estimation methodology. These systems fail because a
single variable cannot adequately account for the
bio-logical variability of weight-for-age and weight-for-length
* Correspondence:mike.wells@emergencymedicine.co.za1Division of Emergency Medicine, Faculty of Health Sciences, University of
the Witwatersrand, 7 York Road, Parktown, Johannesburg 2193, South Africa
2
Postnet Suite 429, Private Bag X1510, Glenvista 2058, South Africa
[10, 11]. There is a wide variability of body habitus that
is not accounted for in these weight-estimation systems,
aggravated by the increasing levels of obesity affecting
children [12, 13]. Newer, more promising, methods are
the
“
two-dimensional
”
or dual length- and habitus-based
systems, which include two variables in the estimation
methodology: length (or a surrogate such as humerus or
ulna length) and habitus (or a surrogate such as
mid-arm circumference or waist circumference) [5, 14
–
17].
These have been shown to be much more accurate
than the older, one-dimensional systems, in many
studies [5, 15, 18
–
22].
Healthcare providers may also need more than one
ap-proach to emergency weight estimation: while parental
estimates of weight can be very accurate, parents may
not be present at the time that emergency care is
re-quired (especially in the prehospital environment) [9]. In
these situations, an evidence-based alternative system
may be required.
There has been a large amount of material published
on weight estimation in children. It would be useful to
combine the data from these studies to establish the
ac-curacy of different methodologies both within and
be-tween different populations. Since many of the same
weight estimation systems are used in populations with
very different prevalences of underweight and obese
children, it needs to be ascertained whether this impacts
on the accuracy outcomes of these systems.
In order to create an evidence-based approach to
emergency paediatric weight estimation, it is crucial to
discover which methods predict weight most accurately
and which are most appropriate for emergency use. This
will enable clinicians to decide which systems they
should incorporate into their clinical practice and will
provide some guidance to those who administer, teach
and train paediatric advanced life support on which
sys-tems are important.
The overall aim of this study was to determine which
paediatric weight estimation systems most accurately
es-timate total body weight in children. The first objective
was to determine whether there was evidence in the
lit-erature for an acceptable benchmark level of accuracy
for a weight estimation system. The second objective
was to extract and pool data on the performance of
paediatric weight estimation systems to integrate the
findings, provide a more comprehensive analysis on their
functioning and identify those systems that operated best
in diverse populations. The third objective was to
dir-ectly compare the accuracy of paediatric weight
estima-tion systems, for which paired data was available, using
pooled data and meta-analysis techniques.
Only one meta-analysis has addressed this topic, but
was limited to studies in low- and middle-income
countries [23].
Methods
This systematic review and meta-analysis followed the
PRISMA guidelines.
Search strategy
Online databases (MEDLINE, SCOPUS, Science Direct
and Google) were interrogated for eligible studies,
pub-lished between January 1983 and May 2017, using the
following search terms:
“
paediatric weight estimation
”
,
“
weight estimation children
”
and
“
Broselow tape
”
.
Cit-ation lists of reviewed papers were examined for
add-itional relevant articles. Studies in any language were
included if English translations were obtainable. To
min-imise publication bias, all studies with adequate
report-ing
were
included,
whether
full-text
articles,
dissertations, abstracts, conference presentations or
other unpublished data that had undergone some form
of peer-review.
Study selection and eligibility criteria
All studies that evaluated weight-estimation
methodolo-gies were assessed for inclusion into the study by two
separate investigators (MW and LG). Articles that
con-tained discussions on desired targets of accuracy of
weight estimation systems, or analysis of the
perform-ance of weight-estimation systems were included in the
qualitative arm of the review. Studies that presented
ori-ginal data with either accuracy data (percentage of
esti-mations within 10% of actual weight (PW10)) or bias
and precision data (mean percentage error plus an
ap-propriate indicator of variance), or both, were included
in the meta-analysis. Studies that did not include original
data, those that did not include usable data and those at
high risk of bias (see below) were excluded from the
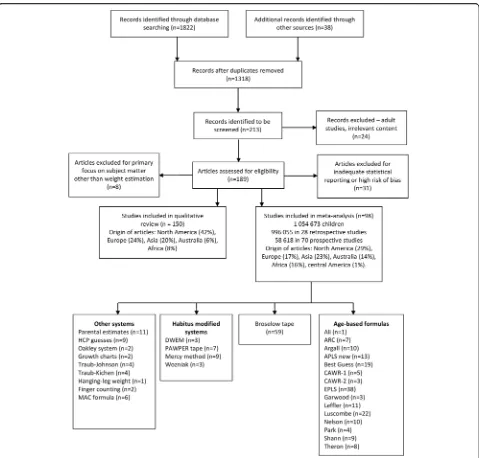
meta-analysis (see Fig. 1).
Data abstraction and analysis
Data was extracted from the included studies
independ-ently by two researchers (MW, LG), cross-checked and
confirmed. Standard statistics for meta-analysis of
method-comparison studies were used [24], with an
em-phasis on evaluating accuracy (percentage of estimations
within 10% of actual weight), bias (mean percentage
error) as well as precision (limits of agreement of
percentage error). Two methods of representing the
pooled
parametric
and
non-parametric
data
were
Many of the evaluated studies presented incomplete
data. Where it was possible, without risking bias, missing
data was imputed using standard methodologies [25].
Direct comparisons between weight estimation
sys-tems, using pooled paired data, were performed with
non-parametric techniques based on PW10 accuracy
data, where such data was available.
Subgroup analysis
There was considerable heterogeneity in the use and
composition of subgroups within the included studies.
Wherever possible, subgroup analyses that had been
per-formed in each study were included in the overall
meta-analysis. The included subgroups focused on different
age groups as previous studies have shown a difference
in weight estimation accuracy between infants (<1 year),
toddlers and pre-school children (1 to 6 years) and older
children (>6 years of age) [26].
Risk of bias within and across studies
Reporting bias was minimised by including all available
methodologically sound studies (published or not).
Methodological causes of potential bias were common
(e.g. the Broselow tape was not actually used in many
studies, but weight-estimates were generated from
length data), but these were individually assessed and
rated according to the level of risk of systematic bias.
Studies with a high risk of bias were excluded from the
meta-analysis (e.g. studies which excluded children
above or below certain weight-for-length centiles).
Sensitivity analysis
There were three large database studies among those
evaluated, with more than 100,000 children, one of
which had more than 400,000 data points [27
–
29]. The
effects of these
“
virtual
”
weight estimation studies, from
very large databases, were carefully considered to
establish any significant contribution to bias or distorted
outcomes.
Software
Statistical analysis was performed using Stata (StataCorp.
2015. Stata Statistical Software: Release 14. College
Sta-tion, TX: StataCorp LP), Graphpad Prism (GraphPad
Prism version 8.00 for Mac, GraphPad Software, La Jolla,
California, USA, www.graphpad.com) and Review
man-ager (Review Manman-ager (RevMan) [Computer program].
Version 5.3. Copenhagen: The Nordic Cochrane Centre,
The Cochrane Collaboration, 2014).
Results
Excluded studies
The most common reason for exclusion of potentially
relevant studies was incomplete data presentation (see
Fig. 1). The large database studies did not have a
signifi-cant impact on overall outcomes based on the sensitivity
analysis and were therefore not excluded from the
analysis.
Characteristics of included studies
Two-thirds of included studies evaluated multiple
weight-estimation systems and contained paired data or
made direct comparisons, while one-third evaluated only
a single system. Prospective studies accounted for the
majority of articles (70/98 (71.4%)) but a minority of
total patients (58,618/1,054,673 (5.6%)).
Table 1 provides a descriptive summary of the studies
included in both the qualitative review as well as the
meta-analysis, including the major findings and
limita-tions of each study and the risk of bias assessment for
each included study.
Benchmark accuracy for a weight estimation system
After studying the 150 identified articles, only three
arti-cles were found to propose a statistically meaningful
tar-get
for
a
weight
estimation
system:
one
article
recommended that 95% of weight estimates must fall
within 20% of actual weight and two articles suggested
that 70% of estimates must be within 10% of actual
weight
and
95% of weight estimates must fall within
20% of actual weight [11, 30, 31]. There was, however,
no evidence found upon which to base any specific
measurement analysis metric for a weight estimation
system. There was also no credible evidence found of a
tolerable weight estimation error, in terms of safety for
drug dose calculation, for an individual child.
In 90/150 articles (60.0%), there was no mention at all
of an appropriate target for weight estimation accuracy.
In 41/150 articles (27.3%) an error of < 10% was
sug-gested as appropriate; in 11/150 articles (7.3%) an error
of < 20% was advocated; in 2/150 articles (1.3%) an error
of < 30%; and in 6/150 articles (4.0%) another value or a
statistically inappropriate measure was proposed. None
of the studies included any evidence to support these
target figures. The values were selected based on clinical
significance, pragmatic limits based on generalised
thera-peutic ratios, or based on guidelines on determining
drug bioequivalence [32, 33].
Meta-analysis data on bias (trueness), precision and
accuracy of paediatric weight estimation systems
Table 2 contains a description of each of the weight
esti-mation systems reviewed, as well as any restrictions on
their use. The raw data and outcomes for each of the
weight-estimation methodologies included in the
meta-analysis are shown in Additional file 1: Table S1. From
the individual study data, it could be seen that there was
very poor within-study precision for most weight
estima-tion systems (shown by the wide limits of agreement),
with the exception of the two-dimensional methods,
which generally had precision limits of agreement of less
than ± 20%.
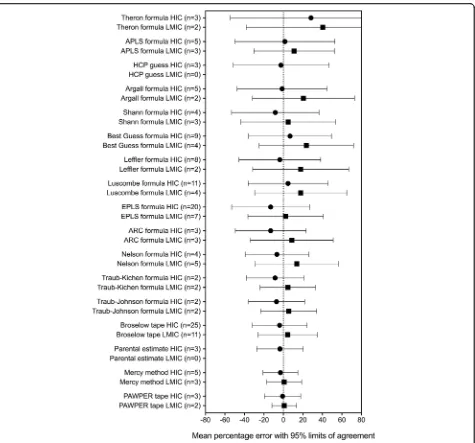
Figure 2 shows the pooled data of the bias and
preci-sion for the weight-estimation systems evaluated. The
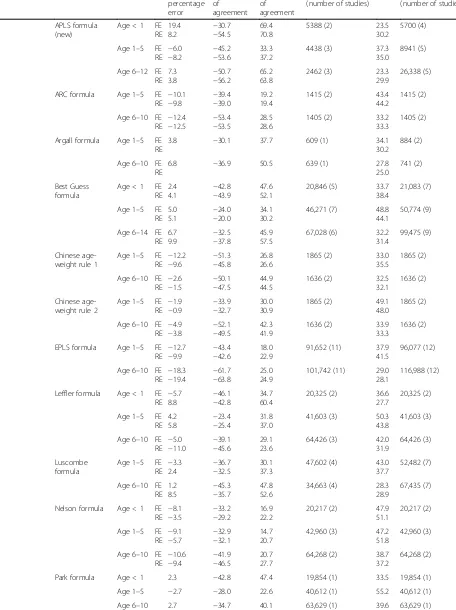
fixed effects outcomes and data for the weight
estima-tion methods not presented in Fig. 2 can be found in
Table 3. The important findings can be summarised as
follows:
There was a wide variation in the weight estimation
bias between low- and middle-income countries
(overestimation) and high-income countries
(under-estimation). This was most noticeable with the
age-based systems, less so with the length-age-based systems
and least with the two-dimensional systems, which
had virtually zero bias.
There were very wide limits of agreement for all
methods other than the PAWPER tape and the
Mercy method.
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
Traub
1983
[
69
]
>
20,000
USA
R
0
to
18
years
Formul
a
to
estimate
IBW
(Traub-Kichen
form
ula)
None
1
Lo
w
Fi
ndings:
Hei
ght
was
a
good
predictor
of
weight
;
IBW
is
onl
y
useful
for
a
han
dful
of
dru
gs;
TBW
mu
st
be
use
d
in
low
weight
-for-height
children.
Comm
ents:
Derivat
ion
st
udy
for
Tra
ub-K
ichen
formula.
IBW
pre
dicted
(act
ually
50th
centile
we
ight-f
or-lengt
h)
by
formula.
Limitations:
Inc
omp
lete
presen
tation
of
data.
Lim
ited
validat
ion
of
form
ula.
Garland
1986
[
67
]
258
USA
P
0
to
19
years
DWEM
,
weight
tab
le
<
1
0
%
*
1
,
2
Lo
w
Fi
ndings:
DWE
M
performed
best
of
me
thods
tested
.
Body
ha
bitus
accurately
ass
essed
by
evaluators.
Co
mments:
Fi
rst
eve
r
rep
ort
of
eva
luati
on
of
we
ight
estimation
syst
ems
in
the
lite
rature.
None
of
the
sy
stems
te
sted
were
very
accu
rate.
Limit
ations:
On
ly
children
up
to
170
cm
we
re
includ
ed.
Inc
omp
lete
presen
tation
of
data.
Lubit
z
1988
[
70
]
937
USA
P
0
to
12
years
Brosel
ow
tap
e
None
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
better
than
heal
thcare
provi
der
guess
es
and
similar
accuracy
to
D
WEM.
Accurac
y
o
f
Bros
elow
tape
falls
off
sharp
ly
in
children
>
2
5
kg.
Comm
ents:
Orig
inal
study
o
f
Bros
elow
tape.
Auth
ors
reco
mmend
ed
that
an
assessment
of
body
habitus
in
chi
ldren
>
2
5
kg
shoul
d
b
e
cons
idere
d.
Limitations:
No
form
al,
prospective
comparison
wit
h
oth
er
method
ologi
es
or
indi
cation
of
desired
accuracy.
Oak
ley
1988
[
71
]
–
UK
––
–
None
1
N/
A
Fi
ndings:
Re
ference
char
t
neede
d
to
aid
rapid
and
accu
rate
managemen
t.
Co
mments:
We
ight
estimation
tab
le
derived
from
average
d
boy
-girl
50
th
centi
le
weight-
for-heigh
t
(source
not
me
ntioned).
Limitations:
No
vali
dation
of
me
thodolo
gy.
Losek
1989
[
72
]
––
–
––
None
1
N/
A
Fi
ndings:
“
Body
habitus
+
height
=
accurate
w
e
ight
es
timate
”
.
Comme
nts:
Letter
claiming
superior
pe
rformanc
e
of
the
D
WEM
over
the
Broselo
w
tap
e.
No
or
iginal
dat
a.
Limitations:
No
menti
on
of
desired
accu
racy.
Haftel
1990
[
73
]
100
USA
P
2
mont
hs
to
15
years
Hangi
ng-leg
we
ight
None
1,
2
Lo
w
Fi
ndings:
Syst
em
accu
rate
in
children
>
10
kg
an
d
more
so
>
25
kg
.
Comme
nts
:
Good
res
ults
never
eva
luated
in
sub
sequent
st
udies.
Lim
itatio
ns:
Small
sample
size
.
Inc
omp
lete
presen
tation
of
data.
Hug
hes
1990
[
74
]
139
UK
P
0
to
10
years
Brosel
ow
tap
e,
healthcare
provider
gue
sses
None
1
N
/A
Fi
ndings:
Bros
elow
tape
performed
sub
stantiall
y
better
than
nurs
es
’
guess
es.
Comm
ents:
First
vali
dation
study
o
f
Bros
elow
tape
in
the
UK
.
Limitations:
Small
sam
ple
size.
Inc
omp
lete
presen
tation
of
data.
Greig
1997
[
36
]
7
5
U
K
P
0
to
1
2
years
healthcare
provider
guesses
None
1,
2
Lo
w
Fi
ndings:
Gu
esses
of
weight
are
very
inac
curate;
chi
ldren
sho
uld
be
weighed
whe
never
possible.
Comm
ents:
Auth
ors
sug
gest
that
accu
rate
we
ight
estimation
is
req
uired
for
mos
t
dru
gs
adm
inistere
d
in
emer
gency
situa
tions.
Age-based
formulas
were
wro
ngly
cons
idere
d
acce
ptabl
e.
Lim
itatio
ns:
Incomp
lete
prese
ntation
of
data,
very
small
sam
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
Leffle
r
1997
[
75
]
117
USA
P
0
to
5
years
Parent
al
esti
mates,
Leff
ler
<
10
%
†
1,
2
Lo
w
Fi
ndings:
Pare
ntal
estimate
s
pe
rforme
d
mu
ch
better
than
form
ula.
Distrau
ght
pare
nts
may
be
unreliable.
Comm
ents:
Sm
all
sample
size.
O
nly
children
<
6
years
inc
luded.
Lim
itation
s:
Over-or
undere
stim
ation
not
recorded.
Inc
omp
lete
presen
tation
of
data.
Dear
love
1999
[
76
]
50
UK
P
1
to
16
years
Parent
al
esti
mates,
Brosel
ow
tap
e,
EPLS,
Argall
<1
0
%
†
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
performed
be
st,
far
be
tter
than
pare
ntal
estimat
es
and
age
-based
form
ulas.
Comme
nts
:
The
targ
et
of
10%
accu
racy
chos
en
for
children
was
de
liberate
ly
le
ss
than
the
20%
that
the
autho
rs
cons
idered
woul
d
be
app
ropri
ate
for
adult
s.
Lim
itatio
ns:
Incomp
lete
pre
sentation
of
dat
a
an
d
sm
all
sample
size.
Goldm
an
1999
[
77
]
233
Isr
ael
P
–
Parent
al
esti
mates
<
10
%
†
1,
2
Lo
w
Fi
ndings:
Pare
nts,
es
peciall
y
mothers
,
can
accu
rately
es
timate
the
ir
children
’
s
weights.
Co
mments:
Thos
e
pare
nts
that
had
weighed
their
children
an
ave
rage
of
5
weeks
pre
viou
sly
had
the
best
resul
ts.
The
aut
hors
de
fined
highl
y
accu
rate
we
ight
estimat
ions
as
<
5
%
error,
accu
rate
as
<
10%
error
an
d
se
mi-accu
rate
as
<
20
%
error.
Lim
itation
s:
Incomp
lete
prese
ntation
of
data.
Misinte
rpret
atio
n
of
bia
s
as
indi
cative
of
accu
racy.
Harri
s
1999
[
78
]
100
USA
P
0
to
8
years
Parent
al
esti
mates,
healthcare
provider
guesses
None
1,
2
Lo
w
Fi
ndings:
We
ight
estimate
s
by
pare
nts,
nurs
es
and
doctors
we
re
sign
ificantly
unre
liable.
The
error
is
“
so
great
an
d
so
frequ
ent
that
clinical
ly
significan
t
untoward
effect
s
can
be
an
ticipated
”
.
Comme
nts:
Brosel
ow
tap
e
recom
men
ded
by
aut
hors.
Limit
ations:
Inc
omple
te
presen
tation
of
data.
Molyne
ux
1999
[
53
]
142
Malawi
P
8
mont
hs
to
5
years
Blantyre
tape,
healthcare
provider
gue
sses
<20
%
†
1,
2
Lo
w
Fi
ndings:
Hea
lthcare
provi
der
guess
es
we
re
very
inac
curate;
Bla
ntyre
tape
better
than
guess
es.
A
20%
error
cons
idere
d
an
acce
ptable
target.
Comm
ents:
Very
young
st
udy
popu
lation,
mos
tly
unde
r
5
years
.
Limitations:
Inc
omp
lete
presen
tation
of
data.
Kun
2000
[
79
]
909
Ho
ng
Ko
ng
P
0
to
12
years
Brosel
ow
tap
e
<10
%*
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
most
accurate
in
children
from
10
to
25
kg,
but
accept
able
for
all
children.
Adjustment
for
ha
bitus
would
be
advantageou
s.
Comme
nts:
Accurac
y
o
f
Bros
elow
tape
outside
of
the
10
–
25
kg
range
was
actu
ally
poo
r.
The
accu
racy
in
this
range
was
reaso
nable,
but
not
as
good
as
the
autho
rs
sugge
st.
Lim
itations:
Poo
r
interp
retat
ion
of
statist
ics.
Brosel
ow
tap
e
version
not
rep
orted.
Carrol
l
2001
[
80
]
169
UK
P
–
EPLS,
novel
method
s
None
1
N
/A
Fi
ndings:
MA
C
an
d
shoe
size
were
be
tter
indicators
of
we
ight
than
age
.
Comm
ents:
Abstra
ct.
Intere
sting
conc
ept,
frequ
ently
cited
abstract.
Limitations:
Inc
omple
te
pre
sentation
of
dat
a.
Vilke
2001
[
81
]
80
USA
P
–
Brosel
ow
tap
e,
healthcare
provider
gue
sses
<50
%
1
N/
A
Fi
ndings:
95
%
of
estimat
es
within
acceptabl
e
error
range.
Comm
ents:
Un
realistic
target
range,
wit
h
no
eviden
ce
bas
is.
Te
nfold
errors
in
dru
g
do
ses
in
10%
of
cas
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
Bros
elow
tape
more
accurate
than
guess
es.
Limit
ations:
Inc
omp
lete
presen
tation
of
data.
Black
2002
[
52
]
495
Aus
tralia
P
0
to
18
years
EPLS,
Brosel
ow
tap
e,
DWEM
,
Oakley,
TJ
,
TK
None
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
and
D
WEM
we
re
more
accu
rate
than
formulas.
These
method
s
should
be
used
if
we
ighing
not
poss
ible.
Comme
nts:
EP
LS
worst
performer
but
po
or
accu
racy
of
all
system
s.
Good
repro
ducibil
ity
of
ass
essment
of
body
habitus.
Limitations:
Inco
mplete
prese
ntation
of
dat
a.
Brosel
ow
tape
version
not
repo
rted.
Hofer
2002
[
82
]
585
Sw
itzerlan
d
R
6
mont
hs
to
11
years
Brosel
ow
tap
e
<10
%*
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
was
accu
rate
but
undere
stim
ated
we
ight
in
olde
r
chi
ldren.
Co
mments:
Nearly
25%
of
sample
ex
clud
ed
because
they
w
er
e
too
ta
ll
for
the
ta
pe.
Limitations
:
Bro
selow
ta
pe
not
ac
tually
used
an
d
ver
sion
n
ot
re
por
ted.
Incomp
let
e
pr
esenta
ti
on
of
data
.
Ueseg
i
2002
[
83
]
48
Jap
an
P
–
Healt
hcare
provider
guesses
<20
%
1,
2
Lo
w
Fi
ndings:
Do
ctors
’
guesses
o
f
children
’
s
we
ight
were
not
accu
rate
—
dru
g
dose
s
shoul
d
the
refore
be
titra
ted
in
sm
all
pae
diatric
pat
ients
.
Comme
nts:
Wide
variation
in
differ
ent
doc
tors
’
accuracy,
not
related
to
se
niority.
All
estimato
rs
were
ve
ry
inaccura
te;
w
or
st
estimations
occurr
ed
in
childr
e
n
<
2
0
kg.
Limi
tati
on
s:
Incomp
lete
p
res
entat
ion
of
d
ata;
conclusion
tha
t
underestimation
o
f
w
eight
m
ay
“
not
be
a
se
ri
o
u
s
p
rob
le
m
”
was
n
o
t
suppor
ted
b
y
the
ev
idence.
Arga
ll
2003
[
84
]
300
UK
P
1
to
10
years
EPLS,
Brosel
ow
tap
e
None
1
N/
A
Fi
ndings:
Bot
h
method
s
pe
rforme
d
poorly
and
worsen
ed
with
inc
reasing
age
.
Comm
ents:
Diff
icult
to
draw
any
conc
lusions
from
this
st
udy,
but
Broselo
w
tap
e
mar
ginally
be
tter
than
formula.
Authors
suggest
that
me
thods
of
we
ight
estimation
not
kee
ping
up
with
inc
reasing
obe
sity.
Limita
tions:
B
roselow
ta
p
e
ver
sion
not
reported.
In
co
m
plete
p
res
entat
ion
of
d
ata.
Potie
r
2003
[
85
]
––
–
–
EPLS,
Brosel
ow
tap
e
None
1
N/
A
Fi
ndings:
EPLS
“
may
”
be
losing
accuracy
with
increasing
obe
sity;
Broselo
w
tap
e
“
may
indee
d
be
”
more
accu
rate.
Comm
ents:
Min
i-PICO
analysis.
Lim
itation
s:
Limited
qua
litative
-only
evaluation.
No
com
ment
on
accept
able
de
gree
of
accuracy.
Hoh
enhaus
2004
[
86
]
––
–
–
Brosel
ow
tap
e
None
1
N/
A
Fi
ndings:
Bros
elow
tape
may
cau
se
significan
t
weight
es
timation
errors
if
used
inc
orrect
ly.
Bros
elow
tape
more
inten
ded
for
equipment
size
de
terminat
ion
than
for
we
ight
estimation
.
Limit
ations:
Bros
elow
tape
proposed
as
be
st
instrume
nt
with
mi
nimal
discuss
ion.
No
targets
for
we
ight
estimation
.
Moore
2004
[
87
]
144
USA
P
–
Brosel
ow
tap
e
None
1
N/
A
Fi
ndings:
Des
pite
using
Bros
elow
tape,
only
56%
corr
ect
me
dication
doses
delivered.
Comme
nts:
Despite
im
provi
ng
we
ight
estimation
,
the
Bros
elow
tape
did
not
decrease
me
dication
errors.
Limitations:
Inco
mplete
pre
sentation
of
dat
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho r an d date Stud y size ( N ) Count ry Des ign Patient age s Estimation techni ques evaluated Target ArmRisk of bia
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
Hashi
kawa
2007
[
32
]
1207
USA
R
0
to
12
years
Brosel
ow
tap
e
<
20
%
†
1
N
/A
Fi
ndings:
App
roximat
ely
60
%
accuracy
o
f
col
our
zone
s
as
si
gnm
e
nt
(a
ccur
at
e
dr
ug
dosi
ng).
We
ight
u
n
der
e
st
im
ate
d
in
obese
and
older
children.
Co
m
m
ents
:R
ising
p
reva
le
nce
o
f
obesity
b
la
med
for
poor
perfor
ma
nce.
Bro
selow
tape
version
200
2B.
The
average
st
udy
p
opul
at
ion
B
MI
was
1
7.
Lim
itati
ons:
Bros
elow
tape
not
actually
used
.Asse
ssment
of
correct
zone
assignmen
t
only,
weight
no
tm
e
as
u
re
d
.I
n
co
m
p
le
te
p
res
entat
ion
of
d
ata.
Im
2007
[
95
]
454
Ko
rea
P
–
Brosel
ow
tap
e
None
1
Hig
h
Fi
ndings:
Bros
elow
tape
accurate
in
children
of
nor
mal
we
ight-fo
r-lengt
h
C
o
mments:
O
nly
children
falli
ng
with
in
3rd
to
9
7
th
w
eig
h
t-for-hei
g
ht
centil
es
incl
uded
.V
ery
young
st
udy
p
opul
ati
o
n
.B
rose
low
tape
only
recommended
by
authors
for
“
no
rm
al-g
ro
w
th
”
chi
ldren
<
2
0
kg
and
<
120
cm.
Limita
tions:
Incomplete
p
re
se
nta
tion
o
f
d
at
a.
Conclusions
not
supported
by
findin
g
s.
Jang
2007
[
96
]
665
Ko
rea
R
–
Brosel
ow
tap
e
<
10
%
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
reasonabl
y
accu
rate
in
this
popu
lation,
but
le
ss
so
in
children
>
2
5
kg.
Comm
ents:
O
verall
unde
restimation
of
we
ight.
Pe
rformanc
e
not
very
goo
d
and
on
par
with
most
othe
r
studies.
Limitations:
Bros
elow
tape
not
actu
ally
used
and
version
not
reported.
Inc
omp
lete
presen
tation
of
data.
Kelly
2007
[
97
]
410
Aus
tralia
P
1
to
11
years
BG
<
20
%
1,
2
Lo
w
Fi
n
d
in
g
s:
B
G
p
e
rf
o
rm
e
d
m
o
d
e
ra
te
ly
w
e
ll,
b
u
t
o
ve
re
st
im
at
e
d
w
e
ig
ht
in
low
B
M
I
child
ren.
C
o
mments
:Mult
iple
pa
pers
on
sa
me
da
ta.
B
MI
wa
s
1
7
in
stud
y
popu
lat
ion.
Signi
fic
ant
number
of
ch
ildren
ha
d
lar
ge
er
ror
s
o
f
weight
estima
tion
.
Limita
tions:
Incomplete
p
re
senta
tion
o
f
d
at
a.
Kriese
r
2007
[
98
]
410
Aus
tralia
P
1
to
10
years
Parent
al
esti
mates,
Brosel
ow
tap
e,
BG,
Arga
ll,
EPLS
<
10
%*
1,
2
Lo
w
Fi
ndings:
Pare
ntal
estimate
s
pe
rforme
d
be
st,
followe
d
by
Bros
elow
tape.
On
ly
11
%
of
paren
ts
could
not
provi
de
an
es
timate
.
Formul
as
pe
rformed
much
worse
than
other
m
e
thods
.Com
m
ents
:M
ul
tip
le
p
ap
ers
o
n
sam
e
d
ata.
Stu
d
y
popula
tion
BMI
w
as
17.1.
Limita
tions:
B
ro
selow
tape
not
actua
lly
used.
B
ro
selow
ta
p
e
ver
sion
not
re
ported.
Incomplete
p
re
sentation
of
data.
Luscom
be
2007
[
1
]
13,988
UK
R
1
to
10
years
EPLS,
Luscom
be
None
1,
2
Lo
w
Fi
ndings:
The
aut
hors
comm
ented
that
since
few
children
with
high-acu
ity
cond
itions
are
actually
weighe
d
in
clinical
prac
tice,
we
ight
es
timation
esse
ntial.
The
EPLS
formula
sig
nificantly
undere
stimated
weight
,
which
may
lead
to
unde
r-resuscitation.
The
Lus
combe
formula
was
more
accu
rate.
Comm
ents:
Bot
h
formulas
actually
performed
poo
rly.
Limit
ations:
Inc
omple
te
presen
tation
of
data.
Mean
bia
s
used
incorrect
ly.
Luten
2007
[
99
]
––
–
–
Brosel
ow
tap
e
None
1
N
/A
Fi
ndings:
No
substan
tiation
for
se
tting
acce
ptabl
e
accuracy
of
weight
estimation
at
10%.
C
om
ments:
Editorial
commen
t;
no
e
vi
d
en
ce
p
ro
vi
d
e
d
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho r an d date Stud y size ( N ) Count ry Des ign Patient age s Estimation techni ques evaluated Target ArmRisk of bia
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
Zink
2008
[
106
]
127
USA
P
0
to
17
years
Parent
al
esti
mates,
healthcare
provider
guesses,
DWEM
,
Bros
elow
tape
None
1
Hig
h
Fi
n
d
in
g
s:
B
ro
se
lo
w
ta
p
e
an
d
D
W
EM
w
e
re
th
e
le
as
t
ac
cu
ra
te
methods.
Comments:
No
conclusion
s
ca
n
be
dra
w
n
from
this
stu
d
y
b
ecause
of
th
e
m
e
thod
o
lo
g
y.
Limi
tat
ions
:T
he
dat
a
appears
to
favour
healthcare
provider
an
d
p
arent
g
uesses,
b
u
t
the
stat
ist
ical
me
thodology
is
flawed.
Anstett
2009
[
107
]
545
Ireland
R
–
Brosel
ow
tap
e
None
1,
2
Lo
w
Fi
n
d
in
g
s:
Th
e
B
ro
se
lo
w
ta
p
e
w
as
o
ft
en
in
ac
cu
ra
te
an
d
te
n
d
ed
to
und
e
restimate
w
eight.
Comments:
A
bstract
.The
B
roselow
tap
e
actually
performed
b
etter
in
this
study
than
in
many
other
st
u
dies.
Limitations:
B
roselow
tape
version
n
ot
re
p
o
rt
ed
.
Bro
selow
ta
pe
not
ac
tually
used.
Cattamanchi
2009
[
108
]
15,000
Indi
a
P
2
mont
hs
to
12
years
Brosel
ow
tap
e
<
10
%*
1,
2
Lo
w
Fi
ndings:
The
Bros
elow
tape
performed
we
ll,
especially
in
chi
ldren
<
1
0
kg
but
undere
stimate
d
all
othe
rs,
especially
in
children
>
1
8
kg.
Comm
ents:
Abs
tract.
Ve
ry
large
prospective
st
udy.
The
autho
rs
recom
men
ded
a
new
vers
ion
of
Brosel
ow
tape
for
Indi
an
children
be
cause
of
unde
restimation
of
weight.
Limitations:
Bros
elow
tape
vers
ion
not
rep
orted.
Inco
mplete
pre
sentation
of
dat
a.
Catterm
ole
2009
[
109
]
1368
Ho
ng
Ko
ng
P
1
to
12
years
MAC,
Bros
elow
tape,
foot
lengt
h
None
1
N/
A
Fi
ndings:
Es
timate
s
of
we
ight
can
be
bas
ed
on
MAC.
A
spec
ial
colo
ur-coded
MAC
tape
could
be
produ
ced
to
aid
dru
g
dosi
ng.
The
auth
ors
reco
mmend
ed
habitus
mod
ified
use
o
f
B
roselow
ta
p
e.
C
o
mments:
Abstra
ct
.N
o
d
ata
p
resented.
Br
oselow
tape
per
formed
b
et
ter
in
you
n
ger
children,
MAC
better
in
o
ld
er
child
ren.
Limitations:
N
o
d
ata
p
re
se
ntation.
Partri
dge
2009
[
110
]
777
USA
P
0
to
20
years
Parent
al
esti
mates,
healthcare
provider
guesses
<1
0
%
†
1,
2
Lo
w
Fi
ndings:
Pare
nts
were
be
tter
than
nurs
es
at
estimating
we
ight;
nurs
es
were
very
inac
curate.
Comm
ents:
Gues
sed
we
ights
mos
t
often
undere
stim
ations.
The
lon
ger
the
time
from
last
weig
hing,
the
greater
the
error.
All
n
urses,
rega
rdless
of
tr
ai
nin
g
an
d
exper
ience,
wer
e
po
or
estimat
o
rs
.L
imita
tion
s:
Incomp
let
e
pr
esenta
ti
on
of
data
.
Paw
2009
[
111
]
791
UK
P
1
to
12
years
EPLS
None
1
Hig
h
Fi
n
d
in
g
s:
V
er
y
p
o
o
r
p
er
fo
rm
an
ce
o
f
EP
LS
fo
rm
u
la
.T
h
e
au
th
o
rs
rec
o
mmend
ed
th
e
B
ro
sel
o
w
ta
p
e
o
r
an
alter
na
tive
for
m
ul
a.
Co
mments:
Abstrac
t.
U
n
iformly
abysmal
acc
uracy
across
different
e
thnic
gr
ou
ps.
Limitations:
Incomp
let
e
p
re
senta
tion
of
da
ta
.
Sandel
l
2009
[
112
]
846
UK
P
1
to
11
years
EPLS,
age-based
estimate
s
vs.
lengt
h-based
es
timate
s
None
1,
2
Lo
w
Fi
ndings:
Leng
th-b
ased
an
d
age-base
d
system
s
are
suit
abl
e
in
emer
gencies
,
but
lengt
h-based
we
re
be
tter;
new
form
ulas
more
accurate
than
EPLS;
“
one
size
fi
ts
all
”
app
roac
h
not
like
ly
to
be
successful.
Co
mments:
Un
ique
me
thod
of
an
alysin
g
data
—
does
not
all
ow
comparisons
with
othe
r
studies
in
this
format.
Age-based
method
s
less
accurat
e
than
su
gge
sted
;b
iolog
ica
l
va
riab
ili
ty
less
in
lengt
h
-ba
se
d
than
ag
e
-ba
sed
sy
st
e
m
s.
Limitations:
Incomplete
p
res
entat
ion
of
d
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho r an d date Stud y size ( N ) Count ry Des ign Patient age s Estimation techni ques evaluated Target ArmRisk of bia
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho r an d date Stud y size ( N ) Count ry Des ign Patient age s Estimation techni ques evaluated Target ArmRisk of bia
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
Huybrec
h
ts
2011
[
123
]
275
Belg
ium
P
3
to
7
years
Parent
al
esti
mates,
pare
nt
vs.
nurse
measuremen
t
None
1
Lo
w
Fi
ndings:
Pare
ntal
estimate
s
we
re
mos
t
accu
rate
wh
en
bas
ed
on
measu
reme
nts
made
at
home
,
rather
than
ong
uesses.
Comm
ents:
Applicat
ion
to
emer
gen
cy
we
ight
es
timations
is
uncertain
as
pare
ntal
stress
may
negate
this
eff
ect.
Lim
itation
s:
Targets
we
re
es
timations
of
overw
eight
or
unde
rweight.
Incomp
lete
prese
ntation
of
data.
Kelly
2011
[
124
]
410
Aus
tralia
P
1
to
10
years
Luscom
be,
EPLS
,
Argall,
BG
<
1
0
%
*
1
,
2
Lo
w
Fi
ndings:
The
Lus
combe
form
ula
performed
best
of
all
the
form
ulas.
Comm
ents:
Study
population
BM
I
was
17.
Same
popu
lation
as
Ng
uyen
2007
and
se
veral
other
publi
cations
;
all
form
ulas
pe
rforme
d
poo
rly.
Limit
ations:
Inc
omple
te
pre
sentation
of
dat
a.
Knight
2011
[
125
]
657
USA
R
–
Brosel
ow
tap
e
None
1,
2
Lo
w
Fi
ndings:
Bros
elow
tape
performed
poo
rly,
pot
entially
le
ading
to
unde
r-resuscitation
in
all
we
ight
categories,
es
peciall
y
in
you
nger
chi
ldren.
Drug
do
ses
corr
ect
in
only
abou
t
50%
of
cases.
Consen
sus
op
inion
req
uired
whe
ther
to
use
IBW
or
TBW
during
resusci
tation.
Comm
ents:
Bros
elow
tape
2007B
.
High
inc
idenc
e
of
obe
sity
in
study
popu
lation.
Limitations:
Brosel
ow
tape
not
actu
ally
used.
Inc
omp
lete
presen
tation
of
data.
No
direct
assessment
of
accu
racy
of
weight
es
timation.
Luscom
be
2011
[
126
]
64,197
UK
R
1
to
16
years
EPLS,
Luscom
be
None
1,
2
Lo
w
Fi
ndings:
The
Lus
combe
form
ula
outpe
rforme
d
the
EPLS
form
ula.
We
ight
estimation
is
of
paramount
im
portan
ce
in
res
uscitation,
therefore
rem
embering
one
formula
be
tter
than
several.
Comme
nts:
While
the
bia
s
o
f
the
Luscombe
form
ula
was
small
er,
both
formulas
pe
rforme
d
poorly
.
Limitations:
Inc
o
mplete
pres
e
n
tation
of
data.
A
n
inappropriate
age
range
was
u
sed
for
formulas
(up
to
16
years).
Marlow
2011
[
27
]
140,31
4
UK
R
0
to
16
years
EPLS,
Argall,
L
uscom
be,
BG
<
1
0
%
*
1
,
2
Lo
w
Findings:
The
EPLS
for
mula
was
least
accura
te
of
commonly
u
sed
formul
as
.T
he
BG
an
d
Lu
scomb
e
formu
las
w
ere
very
si
mil
ar
and
the
b
est
p
erfo
rm
e
rs.
N
o
formul
as
showed
acceptable
accuracy,
however
.C
o
m
m
e
n
ts
:A
b
st
ra
ct
,w
it
h
additional
d
ata
supplied
b
y
author.
This
w
as
a
ver
y
large
re
tr
ospec
tive
d
at
ab
as
e
stud
y
wit
h
g
o
o
d
des
cri
ptiv
e
sta
tis
tics.
Limita
tions:
Some
in
complete
d
ata
.
Rosenbe
rg
2011
[
38
]
372
USA
P
0
to
14
years
healthcare
provider
guesses,
Brosel
ow
tape
<
10
%*
1,
2
Lo
w
Fi
ndings:
The
Bros
elow
tape
was
better
than
guess
es
by
doc
tors,
but
not
in
obese
chi
ldren.
Poor
ass
essment
of
habitus
b
y
d
octor
s.
IBW
suggested
as
the
best
ta
rget
for
es
timation
in
obe
se
kid
s.
Com
m
ents:
B
rose
low
tape
2
0
07B.
35
%
o
f
study
p
o
pul
ati
o
n
ob
ese
o
r
o
verwei
ght.
Mean
BMI
w
as
17.4.
It
is
a
refl
ection
o
f
h
o
w
poorl
y
the
B
ros
elow
tape
p
e
rformed
in
o
bese
ch
ildren
that
d
o
ctor
es
timates
w
ere
better;
o
ve
ra
ll
findings
of
Broselo
w
ta
pe
accura
cy
simila
r
to
other
studies.
Limitations:
In
co
m
plete
d
ata
p
re
senta
tion.
In
co
rre
ct
u
se
of
som
e
statisti
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho r an d date Stud y size ( N ) Count ry Des ign Patient age s Estimation techni ques evaluated Target ArmRisk of bia
Table
1
Studies
included
in
the
qualitative
review
and
quantitative
meta-analysis
(Continued)
Autho
r
an
d
date
Stud
y
size
(
N
)
Count
ry
Des
ign
Patient
age
s
Estimation
techni
ques
evaluated
Target
Arm
Risk of bia
s
Maj
or
fi
ndings;
com
ments
;
major
limitat
ions
acce
ptabl
e
targets
for
weight
es
timation
or
weaknesse
s
o
f
age
form
ulas.
Subjective
ass
essm
ent
of
studies
onl
y.
Meguerdician
2012
[
2
]
––
–
––
None
1
N/
A
Fi
ndings:
The
Bros
elow
tape
is
the
mos
t
consiste
nt
an
d
re
liable
tool
for
w
<