Parents’ Experiences of Expanded Newborn Screening
Evaluations
WHAT’S KNOWN ON THIS SUBJECT: The referral and evaluation of an infant for an abnormal newborn screening result is highly distressing for families. Screening for more metabolic disorders has increased infant referrals, but little is known about parents’ experiences of expanded screening evaluations.
WHAT THIS STUDY ADDS: Parents provided a description of the challenges they encountered during the evaluation of their infants. New approaches to care are suggested to help alleviate some of parents’ distress. Comprehensive strategies for follow-up are needed for infants with equivocal diagnostic results.
abstract
OBJECTIVE:Abnormal results of newborn screening for common met-abolic diseases are known to create substantial distress for parents. We explored parents’ perceptions during diagnostic evaluations for newer disorders that are less well understood.
METHODS:Thirty families completed 48 open-ended interviews before and/or after parents received confirmatory test results for their in-fants. Qualitative content analysis was used to analyze the data.
RESULTS:Parents were shocked by the notification of the abnormal test result. Their urgent and often frustrating searches for information dominated the early phase of the screening process. Treatment center personnel were mainly informative and reassuring, but waiting for results exacerbated parents’ distress. Equivocal results from diagnos-tic testing created uncertainties for parents regarding their infants’ long-term health. After counseling, some parents reported inaccurate ideas about the disorders despite exposure to large amounts of infor-mation. Regardless of the challenges and anxieties of the evaluation, nearly every parent thought newborn screening was an important pro-gram for infant health.
CONCLUSIONS:The evaluation of a newborn for an abnormal screen-ing result was highly stressful for parents. To help reduce parents’ distress, improvements in communications and clinical services are needed. Recommendations of useful Internet sites and discussions of this information may benefit parents. Tailoring counseling to meet the needs of culturally and educationally diverse families is needed. Fam-ilies and infants with equivocal results are a new group of patients who merit comprehensive clinical follow-up.Pediatrics2011;128:53–61
AUTHORS:Jane M. DeLuca, PhD, RN, CPNP,aMargaret H.
Kearney, PhD, RN,aSally A. Norton, PhD, RN,aand
Georgianne L. Arnold, MDb
aSchool of Nursing, University of Rochester, Rochester, New
York; andbDivision of Medical Genetics, University of Pittsburgh,
School of Medicine, Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania
KEY WORDS
metabolic disorders, inborn errors of metabolism, primary health care, genetics, newborn screening, public health, qualitative research
Dr DeLuca conceived the study design, collected the data, and analyzed and interpreted the study data and drafted, revised, and approved the final version of the article; Dr Kearney co-conceived the study design and analyzed and interpreted the study data, contributed content to the draft version, and critiqued and approved the final version of the article; Dr Norton contributed to the study design and interpretation of study data, and contributed content to the draft version, and critiqued and approved the final version for publication; and Dr Arnold contributed to data collection and analysis and critiqued and approved the final version for publication.
www.pediatrics.org/cgi/doi/10.1542/peds.2010-3413 doi:10.1542/peds.2010-3413
Accepted for publication Mar 16, 2011
Address correspondence to Jane M. DeLuca, PhD, RN, CPNP, University of Rochester, School of Nursing, 601 Elmwood Ave, Box SON, Rochester, NY 14642. E-mail: [email protected]. edu
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2011 by the American Academy of Pediatrics
Nearly all of the ⬎4 million infants born in the United States each year will undergo newborn screening tests.1 Statewide newborn screening pro-grams began in the mid-1960s. A lim-ited number of disorders were added over the years until the introduction of tandem mass spectrometry. This tech-nology altered the landscape of screening, extending it to disorders about which little may be known and prognostic communication may have limited evidentiary support.2 In 2010, the Secretary’s Advisory Committee on Heritable Disorders in Newborns and Children recommended screening for 30 core disorders, with 26 others de-tectable through differential diagno-sis.3,4 Larger numbers of infants are now referred for screening evalua-tions, many with false-positive re-sults.5–7This has increased the work-loads of clinicians and laboratories,8 and the pace will accelerate as new disorders are added to screening pan-els.9–13 The pathologic significance of some new metabolic conditions, such as short-chain acyl-coenzyme A dehy-drogenase deficiency and others, is unclear.14–16Identification of equivocal biochemical findings or genetic vari-ants can complicate the diagnostic process.17,18These uncertainties pose conundrums to clinicians and parents alike.19
Extensive research has been con-ducted to examine the technical as-pects of expanded screening, but there have been fewer reports on parents’ responses to these screening evalua-tions. Earlier research for common disorders established that parents were shocked by the notification of an abnormal screening result for their in-fants.20,21 Parents of infants with ab-normal cystic fibrosis screening re-sults reported substantial distress while waiting for sweat-test appoint-ments for possible diagnosis.22 This distress often resolved after they
re-ceived negative results, but some par-ents were uncertain of the meaning of carrier status for their infants and re-productive implications for them-selves.23–26 In expanded screening for metabolic disorders, parents of in-fants with false-positive results re-ported increased stress and long-lasting concerns for their infants’ health,27but a later study found that these apprehensions did not lead to creased use of health services for in-fants.28 Parents reported a lack of information on what to expect if their infant was referred for abnormal re-sults and suggested that more educa-tion about screening was needed.29 Most previous studies of parents’ re-sponses to screening relied on their retrospective recall of screening events, sometimes months and years after the screening evaluations took place. The purpose of the present qual-itative study was to create a descrip-tion of parents’ experiences of their in-fants’ evaluations for rare metabolic disorders as they unfolded in real time.
METHODS
The Newborn Screening Process
Different states and regions use a va-riety of protocols in administering newborn screening programs.30 In New York, universal newborn screen-ing is mandatory; however, parents may refuse on religious grounds.31 Screening samples are collected from infants in the first 24 to 48 hours of life and sent to the state laboratory for analysis. Public health law mandates that parents are informed of the pur-pose of newborn screening, and par-ent education is recognized as an im-portant part of the process.31For the metabolic treatment centers selected for our study, the state laboratories notified centers and primary provid-ers of critically abnormal values by telephone and faxed them the name of
the disorder, the abnormal values, and family contact information. Members of the treatment center team and the primary providers often discussed cases by telephone before contacting families, but the primary providers typically made the first call to parents to discuss the results. Infants were evaluated at the treatment centers within 1 week of the notification or un-derwent an emergent evaluation if ill or if they screened positive for severe disorders. Blood and urine samples for confirmatory diagnostic testing were obtained from the infants after the treatment center visit. Depending on the type of testing, results were available from 24 hours to 4 weeks af-ter the evaluation.
Design, Sample, and Recruitment
back-grounds might yield distinctive expe-riences of the phenomenon.32,33
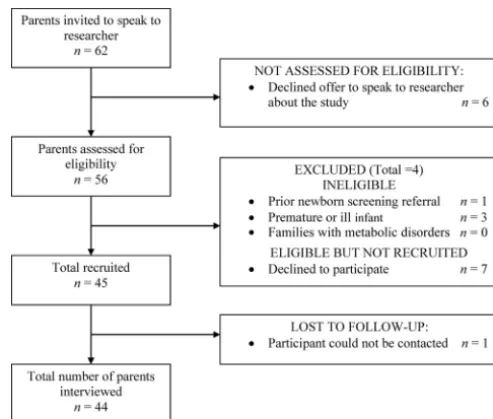
Thirty families (44 parents) of infants referred for 12 of the newer metabolic disorders from the expanded screen-ing panel34participated in the study. At last study contact, 9 infants had con-firmed positive diagnoses and 8 in-fants received negative results. Thirteen infants had equivocal confir-matory results. Equivocal results in-cluded persistently abnormal bio-chemical metabolites (eg, prolonged elevated tyrosine), molecular variants of uncertain significance (eg, isovaleric acidemia “newborn screening” variant), and enzyme deficiencies of uncertain clinical risk (eg, galactocerebrosidase deficiency [Krabbe disease]).
Data Collection
After providing informed consent, 14 couples and 16 solo mothers were interviewed. Forty-eight semistruc-tured open-ended interviews lasting up to 1 hour were conducted by tele-phone (43%) or in person (57%), ac-cording to parent preference, in which parents were asked to de-scribe their reactions to the screen-ing referral and evaluation (Table 1). The first interview was conducted 1 to 2 weeks after infants were evaluated at the treatment centers but before parents received results of confirma-tory testing. The second interview was conducted up to 4 weeks after receiv-ing confirmatory results. If confirma-tory results were returned to parents
before the first interview could be con-ducted, a single comprehensive inter-view was performed (Table 2). An equal number of parents of infants from each of the diagnostic categories (positive, negative, or equivocal) par-ticipated in single interviews. A total of 48 interviews were completed. Each parent received a $10 gift card per in-terview. All interviews were audiore-corded with a digital recorder and transcribed by Dr DeLuca. Transcripts were reviewed for accuracy and loaded into ATLAS.ti 5.0 (Scientific Soft-ware Development GmbH, Berlin, Ger-many) for data management.35
Data Analysis
Qualitative content analysis was used to develop a clinically useful summary of parents’ reports.36Blocks of inter-view text were labeled by codes to characterize parents’ statements. When this process was complete, the codes were merged into larger cate-gory labels that encapsulated the sample’s shared responses to sa-lient screening events. Participant enrollment continued until the satu-ration of data in the key categories was achieved.37 Emblematic verba-tim statements from parents were identified and used to represent par-ents’ characteristic responses to screening evaluation processes.
The qualitative validity38of the find-ings was tested in several ways. Re-peated contact through 2 interviews (60% of the sample) yielded rich data as parents became more com-fortable with the researcher. The de-pendability of analytic decisions was strengthened by reviewing emerging results regularly with experienced peers. Preliminary study results were endorsed when presented to 5 newborn screening parents, 2 metabolic providers and 1 pediat-ric provider, and at 2 national conferences.
FIGURE 1
Diagram of parent recruitment.
TABLE 1 Types of Parent Interviews and Knowledge of Screening
Sample n %
Types of parent interviews
No. of couples interviewed 14 46
No. of sole parents (mothers only) interviewed 16 54 No. of interviews conducted per family
1 12 40
2 18 60
Parents had sufficient knowledge of newborn screening before referral of infant
No 37 84
RESULTS
Demographic Characteristics
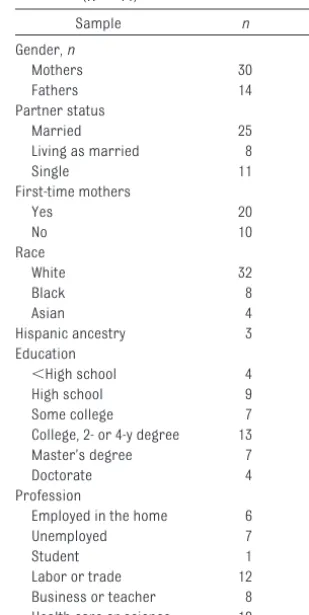
Table 3 describes the characteristics of the parent participants in the study. Fifty-seven percent of parents were married, and fathers represented 32% of the sample. The majority of mothers (67%) were first-time parents. Non-white parents comprised 27% of the sample, and 7% claimed Hispanic an-cestry. Education ranged from non– high school graduates to doctorate de-grees; the largest group (30%) had 2- or 4-year college degrees. Twenty-three percent of parents were em-ployed in science or health care professions.
Parent Response to the Initial Call
Parents spoke of their first response to the call of the positive result as a feeling of shock, as if a death occurred:
“I couldn’t even comprehend anything that she said. I couldn’t even function at the moment she was telling me.” Ac-cording to another parent: “I was shocked, I hadn’t heard of anything like this.” Only 16% of parents stated they had adequate knowledge of newborn screening before the referral of their infants. Many parents had not heard of newborn screening, or if they knew the term, they did not know its mean-ing. Parents often did not remember receiving screening information or teaching before the referral or only vaguely recalled the heel-stick procedure.
Parents’ first concern was to under-stand the metabolic disorder in ques-tion, but nearly 100% had never heard of the disorder before. Many parents felt that their providers did not have sufficient information for them at the
time of the initial call: “She [doctor] made it very clear she was not familiar with this condition at all. She wasn’t really sure what it was or anything.” Few parents felt that their providers were sufficiently knowledgeable about the disorders to adequately explain the conditions. Providers often de-ferred to the metabolic treatment cen-ter to provide detailed information to parents. Parents wanted their infants evaluated at the treatment centers as soon as possible, but appointment times could be several days to 1 week after the notification.
Internet Use
Some parents turned to the Internet for information: “We were furiously looking on the Internet trying to figure out what this is!” Some parents were cautioned by providers not to access the Internet because the information could be upsetting. Most parents ac-TABLE 2 Interview Guide
First interview
Receiving and reacting to news of positive screen result
What did you think about when you found out that you had to have your baby checked out because of the newborn blood test?
Experiences of evaluation at the metabolic treatment center
Can you describe what has happened so far in the follow-up for the newborn blood test; what has this been like?
What kinds of things did you talk about? Perspectives on follow-up and awaiting results
What are your concerns while you wait for the blood/urine test results? Are you doing anything different for your baby because of the clinic visit? Have you talked with anyone about the follow-up for the newborn blood test?
What did you talk about?
Did you look for information on about the newborn blood test or the condition your baby might have?
Is there anything you want to tell me about your experiences thus far that I haven’t asked you about? Second interview
Responses to results of diagnostic evaluation
What do you think about the blood (and/or urine) test results? How do you think this will (or will not) affect your baby’s health? Views on the newborn screening evaluation process before and after results
What did you think was helpful or upsetting about the newborn blood testing? Prompts
Initial contact with the person who spoke to you about the newborn blood testing Care and treatment at the clinic visit
Waiting for test results
Understanding of disorder, test results, and implications
Is there anything you want to tell me about your experiences thus far that I haven’t asked you about? How has your thinking changed about the newborn blood test from the beginning when you found
you had to have the baby checked out to now?
If confirmatory results were returned to parents before interview 1 was conducted, a single interview was conducting, combining the first and second interview questions
TABLE 3 Parent Demographic Characteristics (N⫽44)
Sample n %
Gender,n
Mothers 30 68
Fathers 14 32
Partner status
Married 25 57
Living as married 8 18
Single 11 25
First-time mothers
Yes 20 67
No 10 33
Race
White 32 73
Black 8 18
Asian 4 9
Hispanic ancestry 3 7 Education
⬍High school 4 9
High school 9 20
Some college 7 16 College, 2- or 4-y degree 13 30 Master’s degree 7 16
Doctorate 4 9
Profession
Employed in the home 6 14
Unemployed 7 16
Student 1 2
cessed it anyway, and many were frightened by what they found. “You look on the Internet and look up the disease and that was just scary!” Par-ents were dismayed by the complexity of medical terms and lack of treatment information. Only 1 of 4 parents, mainly those with higher education, were satisfied with their search results. Several parents accessed primary research articles, and 1 parent con-tacted a nationally recognized re-searcher. A few parents did not access the Internet: “Sometimes too much in-formation can be hurtful in a sense. We just didn’t want to expose ourselves.”
Metabolic Treatment Center Visit
Parents were anxious before the treat-ment center visit, but many were re-lieved by it. One parent said: “Her [doc-tor’s] expertise in dealing with [the disorder] over the years really set our hearts and minds at ease.” According to another parent: “It actually helped us a lot because it helped us under-stand.” Most parents valued the ample time for questions and discussion. Some parents appreciated technical discussions about genes and metabo-lites: “We felt like we had a better un-derstanding. We knew the effects, if he had [disorder]. We just didn’t know what the treatment was like. She was really good about answering our ques-tions about the treatment.”
Other parents found the clinicians’ personal qualities important: “They treated us like humans, not just as a number, and talked to us in ways we would understand.” In a few in-stances, clinicians indicated to par-ents it was unlikely the infant was affected, which offered them relief even though they had to wait for con-firmatory results.
Some parents were uncomfortable or overwhelmed by information in the visit. Two mothers had postoperative pain but did not want to shift the focus
of the visit from their infants to them-selves. Several parents of infants with likely positive diagnoses, although sat-isfied with the visits overall, felt the cli-nicians lacked empathy during the dis-cussions: “She was presenting the facts. She was trying to get us to un-derstand, but some of them were pre-sented in a way that had a little scare tactic to it. I don’t think she meant to do it that way, just the way it came across.”
Parents who were young, ethnic mi-norities, or had limited education de-scribed more difficulty in their interac-tions with the metabolic clinic staff: “Because the way they were talking at first, they said he got it, and they were talking like he had it . . . how can he have it if the tests not been run yet?” Also, “It was kind of like ‘wham bam, thank you mam.’ Information wasn’t provided. Like they came and got infor-mation from us but kind of like re-turned and never gave it back.”
Waiting for Test Results
Waiting for confirmatory results was highly stressful. Many parents were consumed by thoughts about the dis-order: “It is always in the back of my mind . . . eating me from the inside out.” Another stated: “It’s kind of just like a waiting game now, wondering if, or what if something happens.” A num-ber of parents were instructed by met-abolic clinic personnel to monitor in-fants for symptoms such as diarrhea or lethargy, which could indicate met-abolic decompensation. This created additional uncertainty for new par-ents. Experienced parents also felt in-secure and second-guessed their abil-ities to recognize illness symptoms: “It was hard for me to determine if it was a throw up or a spit up. Now I feel like I want to wake him up and make sure he isn’t lethargic. I was just nervous, am I going to know what it looks like for a baby to be lethargic versus just
sleep-ing all the time, you know, and also the throwing up thing.”
Parents of infants with expected pos-itive diagnoses had frequent contact by telephone with the treatment cen-ter during this period, but other par-ents did not speak to treatment cen-ter personnel unless they called to report symptoms: “Because we know as parents that doctors are busy, nurses are busy. We feel like we are burdening you, bothering you during the day.”
Parents received the news of confir-matory results by telephone from the treatment center. Parents of infants with negative results were ecstatic: “It’s like you were locked in some-where forever and now you are free!” Parents of affected infants were re-signed to the diagnosis: “I did wish it came back that he was negative for it, but it’s the truth, so I sort of have to live with that.”
Equivocal Results
Parents of infants with equivocal re-sults were relieved that a severe disor-der was not diagnosed but were un-sure of the implications of the findings and some worried about potential long-term health issues for their in-fants: “Because it seems like no matter how much testing they do, something doesn’t show up or something new shows up, you know it’s not just a solid thing.” Another stated: “I felt a little confused, they don’t really know a whole lot about [the disorder], I guess because they kind of left it. Well of all the people they’ve researched nothing has happened but something could happen. So it kind of leaves it wide open. I wonder if something is going to happen later on.”
in-fant’s risk or need for treatment or until the diagnosis could be ruled out.
Parents’ Views on Newborn Screening
Despite the stress of the screening evaluation process, most parents ex-pressed unshakable faith in the merits of newborn screening: “It is probably one of the best things that could be done for the health of a child!” Almost every parent in the study believed that newborn screening was an important program that preserved the health of infants through early identification and treatment of disorders: “You know, some people playing devil’s ad-vocate could say, ‘Well, now you’ve gone through all this and it came to nothing, was it worth it?’ I would say 100 times, yes, because I would always err on the side of being cautious, and I would want to know about something before it happened.”
Three parents were less enthusiastic about screening. One couple objected to screening for rare disorders about which little was known. A parent of an infant with a disorder that might not be clinically significant was distraught over her son’s diagnosis. Living with a potential illness, she explained: “Me, I want him to have a normal life. Right now he isn’t getting it.”
At the time of the final interview, sev-eral parents from each diagnostic out-come group—particularly those who were younger, with less formal educa-tion, or were underserved minorities— had inaccurate information about the disorder or results. Most parents un-derstood the concept of recessive in-heritance, but a few thought the disor-ders were inherited through only 1 parent. Two parents believed the dis-order stemmed from problems of di-gestion. Several parents of infants with negative results thought there might be long-term health implications for their infants.
DISCUSSION
Only a limited number of parents in our study reported having adequate un-derstanding of newborn screening be-fore the referral of their infants, which was consistent with previous re-search.39,40 Reasonable knowledge of the screening process is important for the ethical treatment of families in mandatory screening programs. It may also help reduce parents’ anxiet-ies if they know what to expect if their infants are referred for evaluation. Screening programs recommend that screening education occurs before de-livery41 and parents preferred this,39 but some parents felt that education could be provided in the nursery set-ting if timed for when they were recep-tive to teaching.40Diverse health ser-vice providers are charged with educating parents about screening, but studies indicate that providers were less likely to discuss screening with parents if they did not see it as part of their professional responsibili-ties or if they were less confident of their screening knowledge.42,43 Provid-ing education about newborn screen-ing in high school health and science classes could be a way to introduce the concept of screening to young persons and future parents.
When parents were notified about the abnormality, many felt their providers lacked sufficient information and knowledge about the disorder. Previ-ous literature reported that primary providers had limited knowledge of the screening disorders44and discom-fort discussing results with parents due to lack of knowledge of the newer conditions.45Discussing difficult news is challenging46,47 and may be even more daunting when information is de-livered by telephone.48Training provid-ers to increase their confidence in communicating difficult news may be helpful for these discussions. Alterna-tive models for delivering initial
screening news could be explored to include conference or tandem
tele-phone calls from primary providers and metabolic specialists to provide parents with expert information and support at the time of the referral. Fu-ture studies might determine if pro-grams providing pediatricians and parents with information by fax or e-mail can improve knowledge deficits
and help decrease parents’ distress.
The metabolic clinic visit was benefi-cial for most parents in the study but less so for younger, disadvantaged,
and nonwhite parents. From the per-spective of these parents, providers did not connect with them and the counseling did not fit their informa-tion needs. Cultural orientainforma-tion, educa-tion attainment, and historical influ-ences may affect acceptance and trust of genetically oriented medical
information.49Strategies for culturally sensitive, educationally appropriate counseling are needed. Parents of in-fants who were likely to have positive test results perceived providers as in-sensitive during discussions of screening results. This was echoed in
studies of parents’ experiences of ab-normal prenatal ultrasound counsel-ing,50,51during which some parents felt distanced from providers if they fo-cused on the medical management of the fetus without addressing parents’ needs.51
Parents accessed the Internet but were warned by providers that it could be disturbing. It was not known if par-ents brought information back to pro-viders for discussion. The Internet is increasingly used for health
discussion, and correcting potential inaccuracies in Internet information.
The magnitude of parents’ distress while waiting for infants’ confirmatory test results should not be underesti-mated. Every means should be sought for a quick return of results. Parents, including experienced parents, had difficulty distinguishing metabolic de-compensation from normal newborn behaviors. Parents require sufficient instruction to develop skills to assess their infants for these symptoms. Tele-phone follow-up with all parents dur-ing the waitdur-ing period provides an op-portunity to assess infants’ well-being and address potential educational needs.
As in other screening studies, some parents did not retain accurate infor-mation about the disorders from their discussions with specialty providers, but it was surprising it occurred so soon after they received extensive counseling. Reinforcing parents’ knowledge at case closure and cor-recting misinformation can help guar-antee that parents have adequate un-derstanding of the disorder and its implications. Written information can be provided for parents’ reference.
In previous studies of public opinions of newborn screening programs, indi-viduals approved of screening for well-characterized, treatable disorders. Some also supported screening of con-ditions with less definitive treatments, as well as late-onset and untreatable disorders.55–57The majority of parents in the current study approved of ex-panded newborn screening. However, screening for less well-characterized disorders, about which little is known or that have treatments of limited effi-cacy, may intensify parents’ distress. Rigorous evaluation of candidate dis-orders for screening panels, as well as carefully conducted outcomes studies for disorders currently screened for but that are of uncertain significance,
can help identify disorders that are un-suitable or warrant removal from new-born screening panels.4,14,58
Parents of infants with equivocal re-sults were unsure of the implications of these findings and worried about the health of their infants. Similarly, in a study of parents and equivocal cystic fibrosis results, diagnostic uncertain-ties catalyzed long-term worries about their infants’ health.59However, it was also noted that parents can adjust to these uncertainties over time, espe-cially if infants continue to grow and develop normally.19,59The problems of disorders of uncertain significance and of equivocal diagnostic testing might be addressed, at least in part, by some of the current regional and na-tionally funded projects for long-term follow-up registries.60Pooling of clini-cal data can help in understanding the implications of equivocal and variant findings for infants’ health.61,62 These data may contribute to the develop-ment of consensus practice guide-lines, such as those established by the Cystic Fibrosis Foundation for interme-diate results.63 Understanding the challenges and issues these families face should be considered when plan-ning for long-term follow-up of their infants.
Our study has several potential limita-tions. Interviews were restricted to parents from selected treatment cen-ters in New York. Screening practices differ in other states and regions. Sam-ple size was adequate for qualitative inquiry, but the small numbers of par-ents in diagnostic or demographic subgroups precluded finer compari-sons. Infants with equivocal results comprised the largest group in the study. Equivocal results are not rou-tinely tracked at this stage of the screening process in New York and other state newborn screening pro-grams. Whether this high number rep-resented sampling variation or was
due to specifics of the screening pro-gram is unclear. A recruitment bias may account for these higher numbers despite measures to recruit parents without regard to potential infant diag-noses and before confirmatory results were known in most cases. As in many studies, participants had high educa-tion levels on average, and in this sam-ple more had health care and science backgrounds than the general popula-tion. Nonetheless, the distress of these parents was considerable despite their potentially greater comprehen-sion of the medical situation.
CONCLUSIONS
The evaluation of a newborn for an ab-normal screening result was highly stressful for parents. Several areas for future clinical research were iden-tified. Improving parents’ exposure to and their retention of newborn screen-ing education information is needed. Different methods for notifying par-ents of abnormal screening results could be examined to determine the ef-fects on parents’ distress. Studies are needed that explore provider commu-nications and counseling of culturally and educationally diverse parents. Ex-amining the long-term health of in-fants with equivocal/variant results and researching the concerns of these parents are essential. As newborn screening continues to expand and the numbers of families entering the diag-nostic evaluation process grows, the care families receive must be critically examined and continually improved.
ACKNOWLEDGMENTS
This study was funded in part by a re-search grant from the International Society of Nurses in Genetics.
REFERENCES
1. Serving the family from birth to the medical home and newborn screening. A report from the Newborn Screening Task Force convened in Washington DC, May 10 –11, 1999.Pediatrics. 2000;106(2 pt 2):383– 427 2. Marsden D, Larson C, Levy HL. Newborn
screening for metabolic disorders.J Pedi-atr. 2006;148(5):577–584
3. US Department of Health and Human Ser-vices, Health Resources and Services Ad-ministration. Advisory Committee on Heri-t a b l e D i s o r d e r s i n N e w b o r n s a n d Children. Recommended Uniform Screen-ing Panel* of the Secretary’s Advisory Com-mittee on Heritable Disorders in Newborns and Children. Available at: www.hrsa. g o v / h e r i t a b l e d i s o r d e r s c o m m i t t e e / uniformscreeningpanel.htm. Accessed Oc-tober 20, 2010
4. Calonge N, Green NS, Rinaldo P, et al, and the Advisory Committee on Heritable Disor-ders in Newborn and Children. Committee report: method for evaluating conditions nominated for population-based screening of newborns and children.Genet Med. 2010; 12(3):153–159
5. Howell RR. The high price of false positives.
Mol Genet Metab. 2006;87(3):180 –183 6. Kwon C, Farrell PM. The magnitude and
challenge of false-positive newborn screen-ing test results.Arch Pediatr Adolesc Med. 2000;154(7):714 –718
7. Tarini BA, Christakis DA, Welch HG. State newborn screening in the tandem mass spectrometry era: more tests, more false-positive results.Pediatrics. 2006;118(2): 448 – 456
8. Hubbard HB. Expanded newborn screening for genetic and metabolic disorders: mod-eling costs and outcomes.Nurs Econ. 2007; 25(6):345–352
9. Coffee B, Keith K, Albizua I, et al. Incidence of fragile X syndrome by newborn screening for methylated FMR1 DNA.Am J Hum Genet. 2009;85(4):503–514
10. Comeau AM, Hale JE, Pai SY, et al. Guidelines for implementation of population-based newborn screening for severe combined immunodeficiency. J Inherit Metab Dis. 2010;33(suppl 2):S273–S278
11. Dajnoki A, Mühl A, Fekete G, et al. Newborn screening for Pompe disease by measuring acid alpha-glucosidase activity using tan-dem mass spectrometry.Clin Chem. 2008; 54(10):1624 –1629
12. Dajnoki A, Fekete G, Keutzer J, et al. Newborn screening for Fabry disease by measuring GLA activity using tandem mass
spectrome-try. Clin Chim Acta. 2010;411(19 –20): 1428 –1431
13. Duffner PK, Caviness VS Jr, Erbe RW, et al. The long-term outcomes of presymptomatic infants transplanted for Krabbe disease: re-port of the workshop held on July 11 and 12, 2008, Holiday Valley, New York.Genet Med. 2009;11(6):450 – 454
14. Waisbren SE, Levy HL, Noble M, et al. Short-chain acyl-CoA dehydrogenase (SCAD) deficiency: an examination of the medical and neurodevelopmental characteristics of 14 cases identified through newborn screening or clinical symptoms.Mol Genet Metab. 2008;95(1–2):39 – 45
15. Alexander D, van Dyck PC. A vision of the future of newborn screening. Pediatrics. 2006;117(5 pt 2):S350 –S354
16. van Maldegem BT, Duran M, Wanders RJ, et al. Clinical, biochemical, and genetic heter-ogeneity in short-chain acyl-coenzyme A de-hydrogenase deficiency.JAMA. 2006;296(8): 943–952
17. Arnold GL, Saavedra-Matiz CA, Galvin-Parton PA, et al. Lack of genotype-phenotype corre-lations and outcome in MCAD deficiency di-agnosed by newborn screening in New York State.Mol Genet Metab. 2010;99(3):263–268 18. Wilcken B. Expanded newborn screening: reducing harm, assessing benefit.J Inherit Metab Dis. 2010;33(suppl 2):S205–S210 19. Timmermans S, Buchbinder M.
Patients-in-waiting: living between sickness and health in the genomics era.J Health Soc Behav. 2010;51(4):408 – 423
20. Hewlett J, Waisbren SE. A review of the psy-chosocial effects of false-positive results on parents and current communication prac-tices in newborn screening.J Inherit Metab Dis. 2006;29(5):677– 682
21. Locock L, Kai J. Parents’ experiences of universal screening for haemoglobin disorders: implications for practice in a new genetics era. Br J Gen Pract. 2008; 58(548):161–168
22. Tluczek A, Koscik RL, Farrell PM, Rock MJ. Psychosocial risk associated with newborn screening for cystic fibrosis: parents’ expe-riences while awaiting the sweat-test ap-p o i n t m e n t . P e d i a t r i c s. 2 0 0 5 ; 1 1 5 ( 6 ) : 1692–1703
23. Lang CW, McColley SA, Lester LA, Ross LF. Parental understanding of newborn screening for cystic fibrosis after a nega-tive sweat-test. Pediatrics. 2011;127(2): 276 –283
24. Cavanagh L, Compton CJ, Tluczek A, Brown RL, Farrell PM. Long-term evaluation of
ge-netic counseling following false-positive newborn screen for cystic fibrosis.J Genet Couns. 2009;19(2):199 –210
25. Beucher J, Leray E, Deneuville E, et al. Psy-chological effects of false-positive results in cystic fibrosis newborn screening: a two-year follow-up. J Pediatr. 2010;156(5): 771–776
26. Ciske DJ, Haavisto A, Laxova A, Rock LZ, Far-rell PM. Genetic counseling and neonatal screening for cystic fibrosis: an assess-ment of the communication process. Pedi-atrics. 2001;107(4):699 –705
27. Waisbren SE, Albers S, Amato S, et al. Effect of expanded newborn screening for bio-chemical genetic disorders on child out-comes and parental stress.JAMA. 2003; 290(19):2564 –2572
28. Lipstein EA, Perin JM, Waisbren SE, Prosser LA. Impact of false-positive newborn meta-bolic screening on early health care utiliza-tion.Genet Med. 2009;11(10):716 –721 29. Morrison DR, Clayton EW. False positive
newborn screening results are not always benign.Public Health Genomics. 2011;14(3): 173–177
30. American Academy of Pediatrics Newborn Screening Authority Committee. Newborn screening expands: recommendations for pediatricians and medical homes— implications for the system.Pediatrics. 2008;121(1):192–217
31. New York State Department of Health. New-born Screening in New York State: A Guide for Health Professionals.Albany, NY: New-born Screening Program, Wadsworth Center; 2003
32. Sandelowski M. Whatever happened to qual-itative description?Res Nurs Health. 2000; 23(4):334 –340
33. Maxwell J.Qualitative Design. Thousand Oaks, CA: Sage Publications;1996
34. New York State Department of Health, New York State Wadsworth Center. Newborn Screening Program. Available at: www. wadsworth.org/newborn/babhealth.htm. Accessed January 15, 2011
35. Muhr T.Users’ Manual for ATLAS.ti [com-puter program]. Version 5.0. Berlin, Germany: Scientific Software Development GmbH
36. Miles B, Huberman A.Qualitative Data Anal-ysis.Thousand Oaks, CA: Sage Publications; 1994
37. Morse J. Determining sample size.Qual Health Res. 2000;10(1):3–5
39. Davis TC, Humiston SG, Arnold CL, et al. Rec-ommendations for effective newborn screening communication: results of focus groups with parents, providers, and ex-p e r t s . P e d i a t r i c s. 2 0 0 6 ; 1 7 ( 5 p t 2 ) : S326 –S340
40. Tluczek A, Orland KM, Nick SW, Brown RL. Newborn screening: an appeal for improved parent education.J Perinat Neonatal Nurs. 2009;23(4):326 –334
41. Kemper AR, Fant KE, Clark SJ. Informing par-ents about newborn screening. Public Health Nurs. 2005;22(4):332–338
42. Hayeems RZ, Miller FA, Little J, et al. Inform-ing parents about expanded newborn screening: influences on provider involve-ment.Pediatrics. 2009;124(3):950 –958 43. Faulkner LA, Feuchtbaum LB, Graham S,
Bol-stad JP, Cunningham GC. The newborn screening educational gap: what prenatal providers do compared with what is ex-pected.Am J Obstet Gynecol. 2006;194(1): 131–137
44. Gennaccaro M, Waisbren SE, Marsden D. The knowledge gap in expanded newborn screening: survey results from paediatri-cians in Massachusetts.J Inherit Metab Dis. 2005;28(6):819 – 824
45. Kemper AR, Uren RL, Moseley KL, Clark SJ. Primary care physicians’ attitudes regard-ing follow-up care for children with positive newborn screening results. Pediatrics. 2006;118(5):1836 –1841
46. Harrison ME, Walling A. What do we know about giving bad news? A review.Clin Pedi-atr (Phila). 2010;49(7):619 – 626
47. Horwitz N, Ellis J. Paediatric SpR’s experi-ences of breaking bad news.Child Care Health Dev. 2007;33(5):625– 630
48. Ngo-Metzger Q. Breaking bad news over the phone.Am Fam Physician. 2009;80(5):520 49. Catz DS, Green NS, Tobin JN, et al. Attitudes
about genetics in underserved, culturally diverse populations. Community Genet. 2005;8(3):161–172
50. Lalor JG, Devane D, Begley CM. Unexpected diagnosis of fetal abnormality: women’s en-counters with caregivers.Birth. 2007;34(1): 80 – 88
51. Larssen AK, Svalenius EC, Lundqvist A, Lund-qvist A, Dykes AK. Parents’ experiences of an abnormal ultrasound examination— vacillating between emotional confusion and sense of reality.BMC. Repro Health. 2010;7:1–10. Available at: www.reproductive-health-journal.com/content/7/1/10. Ac-cessed January 13, 2010
52. The Harris Poll. “Cybercondriacs” on the Rise? Those who go online for healthcare information continues to increase. August 4, 2010. Available at: www.harrisinteractive. com/vault/HI-Harris-Poll-Cyberchondriacs-2010-08-04.pdf. Accessed October 20, 2010 53. Imes RS, Bylund CL, Sabee CM, Routsong TR,
Sanford AA. Patients’ reasons for refraining from discussing internet health informa-tion with their healthcare providers.Health Commun. 2008;23(6):538 –547
54. Ahmad F, Hudak PL, Bercovitz K, Hollenberg E, Levinson W. Are physicians ready for pa-tients with Internet-based health informa-tion?J Med Internet Res. 2006;8(3):e22 55. Plass AM, van El CG, Pieters T, Cornel MC.
Neo-natal screening for treatable and untreatable disorders: prospective parents’ opinions.
Pediatrics. 2010;25(1). Available at: www. pediatrics.org/cgi/content/full/25/1/e99 56. Lipstein EA, Nabi E, Perrin JM, Luff D,
Brown-ing MF, Kuhithau KA. Parents’ decision-making in newborn screening: opinions,
choices, and information needs.Pediatrics. 2010;126(4):696 –704
57. Hasegawa LE, Fergus KA, Ojeda N, Au SM. Parental attitudes toward ethical and social issues surrounding the expansion of new-born screening using new technologies.
Public Health Genomics. 2010; In press 58. Stadler SC, Polanetz R, Maier EM, et al.
New-born screening for 3-methylcrotonyl-CoA carboxylase deficiency: population hetero-geneity of MCCA and MCCB mutation and im-pact on risk assessment.Hum Mutat. 2006; 27(8):748 –759
59. Tluczek A, Chevalier McKechnie A, Lynam PA. When the cystic fibrosis label does not fit: a modified uncertainty theory. Qual Health Res. 2010;20(2):209 –223
60. Berry SA, Lloyd-Puryear MA, Watson MS. Long-term follow-up of newborn screening patients. Genet Med. 2010;12(12 suppl): S267–S268
61. Wright E, Van Hove JL, Thomas J, Mountain States Metabolic Consortium. Mountain States Genetics Regional Collaborative Cen-ter’s Metabolic Newborn Screening Long-term Follow-up Study: a collaborative multi-site approach to newborn screening outcomes research.Genet Med. 2010;12(12 suppl):S228 –S241
62. Botkin JR, Anderson R, Staes C, Longo N. De-veloping a National Registry for conditions identifiable through newborn screening.
Genet Med. 2009;11(3):176 –182
DOI: 10.1542/peds.2010-3413 originally published online June 27, 2011;
2011;128;53
Pediatrics
Jane M. DeLuca, Margaret H. Kearney, Sally A. Norton and Georgianne L. Arnold
Parents' Experiences of Expanded Newborn Screening Evaluations
Services
Updated Information &
http://pediatrics.aappublications.org/content/128/1/53
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/128/1/53#BIBL
This article cites 53 articles, 10 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/genetics_sub
Genetics
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
ub
http://www.aappublications.org/cgi/collection/metabolic_disorders_s
Metabolic Disorders
http://www.aappublications.org/cgi/collection/endocrinology_sub
Endocrinology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2010-3413 originally published online June 27, 2011;
http://pediatrics.aappublications.org/content/128/1/53
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.