Pulmonary Function in
Primary Pulmonary Hypertension
Xing-Guo Sun, MD, James E. Hansen, MD, Ronald J. Oudiz, MD, FACC, Karlman Wasserman, PHD, MD
Torrance, California
OBJECTIVES The study was done to ascertain the degree to which abnormalities in resting lung function correlate with the disease severity of patients with primary pulmonary hypertension (PPH).
BACKGROUND Patients with PPH are often difficult to diagnose until several years after the onset of symptoms. Despite the seriousness of the disorder, the diagnosis of PPH is often delayed because it is unsuspected and requires invasive measurements. Although PPH often causes abnormalities in resting lung function, these abnormalities have not been shown to be statistically significant when correlated with other measures of PPH severity.
METHODS Resting lung mechanics and diffusing capacity for carbon monoxide DLCOwere assessed in 79 patients whose findings conformed to the classical diagnostic criteria of PPH and who had no evidence of secondary causes of pulmonary hypertension. These findings were correlated with severity of disease as assessed by cardiac catheterization, New York Heart Association (NYHA) class, and cardiopulmonary exercise testing.
RESULTS When PPH patients were first evaluated at our referral clinic, the DLCOand lung volumes were decreased in approximately three-quarters and one-half, respectively. The decreases in DLCO, and to a lesser extent lung volumes, correlated significantly with decreases in peak oxygen uptake (reflecting maximum cardiac output), peak oxygen pulse (reflecting maximum stroke volume), and anaerobic threshold (reflecting sustainable exercise capacity) and higher NYHA class.
CONCLUSIONS Patients with PPH commonly have abnormalities in lung mechanics and DLCOlevels that correlate significantly with disease severity. These measurements can be useful in evaluating patients with unexplained dyspnea and fatigue. (J Am Coll Cardiol 2003;41:1028 –35) © 2003 by the American College of Cardiology Foundation
Primary pulmonary hypertension (PPH) is a rare, life-threatening illness that is typically diagnosed a year or more after patients become symptomatic (1–4). It begins with alterations to the pulmonary arterioles and capillaries that lead to increased pulmonary vascular resistance, right ventricular hypertrophy and/or dilation, decreased systemic and pulmo-nary perfusion, and an increase in dead-space ventilation. Both the increased ventilatory requirement and the decreased cardiac output response to exercise contribute to the predominant symptoms of exercise dyspnea and fatigue (5,6), symptoms common to many disorders, either organic or functional. Unfortunately, most patients with PPH are diagnosed in advanced stages of their disease, when the mean survival rate is less than three years without treatment (5,6). Because of the lack of distinctive physical, radiographic, and electrocardio-graphic findings in PPH, cardiac catheterization is required to establish and confirm the diagnosis (5,7).
Several studies (6–12) have found that simple, noninvasive lung function measurements, especially the gas transfer index or diffusing capacity for carbon monoxide (DLCO), can also be abnormal in PPH patients. This is not surprising considering that the pathology of PPH primarily involves the small pulmonary arteries and capillaries, and that the DLCO is
dependent on the access and transfer of inhaled carbon monoxide to the hemoglobin in the pulmonary capillaries. However, none of the above studies have shown significant correlations of DLCO with the severity of the disease as measured by New York Heart Association (NYHA) class, resting hemodynamic measurements, or cardiopulmonary ex-ercise test (CPET) parameters. The CPET can be safely performed in PPH patients to: 1) detect patterns of gas exchange abnormalities that are typical of PPH, 2) quantify disease severity, and 3) identify the presence of right-to-left shunting (2,3,13,14). Specifically, the severity of PPH has been shown to be correlated with several CPET parameters, includ-ing peak O2uptake (maximal aerobic capacity), peak O2pulse, and anaerobic threshold (maximal sustainable exercise level) (2). We hypothesized that the DLCO, and perhaps other lung function measurements, would be significantly correlated with the severity of PPH assessed in other ways. Thus, in 79 patients with well-documented diagnoses of PPH and 20 control subjects, resting lung function measurements (includ-ing spirometric, lung volume, and DLCOvalues) were corre-lated with CPET parameters, resting hemodynamic variables (measured during cardiac catheterization), and NYHA symp-tom class.
METHODS
Subjects. After we obtained Human Subjects Committee approval, the resting lung function and CPET measure-ments of 79 consecutive patients referred for such tests with From the Division of Respiratory and Critical Care Physiology and Medicine and
Division of Cardiology, Department of Medicine, Research and Education Institute, Harbor–UCLA Medical Center, Torrance, California. Supported, in part, by the American Heart Association.
Manuscript received May 31, 2002; revised manuscript received November 16, 2002, accepted December 4, 2002.
well-documented diagnoses of PPH seen between 1996 and 2001 in our PPH clinic were analyzed. The diagnosis of PPH was based on clinical and laboratory data, including cardiac catheterization, according to currently accepted diagnostic criteria (4). Many patients had used appetite suppressants. Secondary causes of pulmonary hypertension, such as portal hypertension, interstitial lung disease, throm-boembolic, and infectious diseases were excluded by history, physical examination, cardiac catheterization, ventilation/ perfusion scans, and computerized tomography. All pa-tients’ diagnoses were made or confirmed by the PPH referral clinic cardiologist in charge, who also assigned the NYHA class independently of CPET and resting lung function data. The patients were nonsmokers at the time of study; most had never smoked. This report includes only the first lung function and exercise test measurements made after referral to our PPH clinic, nearly always prior to the initiation of pulmonary vasodilator therapy.
For comparison purposes, the CPET and resting lung function data of 20 sedentary age- and gender-matched control individuals, without detectable cardiorespiratory disorders, were measured during the same time period and analyzed.
Resting lung function measurements. Each patient un-derwent resting measurements of forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), maximum voluntary ventilation (MVV), DLCO and effective alveolar volume (VA⬘) using standard equipment and methodology meeting American Thoracic Society standards (15,16). To-tal lung capacity (TLC) was assessed by multiple breath nitrogen washout or plethysmographic measurements (17,18) in 41 patients.
CPET measurements. On the same day as resting lung function testing, each patient underwent CPET after famil-iarization with the exercise apparatus. The exercise protocol consisted of a progressively increasing work rate test to maximum tolerance on an electromagnetically braked cycle ergometer (2,3,12). Gas exchange was measured using the MedGrapics (St. Paul, Minnesota) CPET equipment that calculated heart rate, ventilation, CO2 output, O2 uptake, and other gas exchange variables, breath-by-breath (2,3,19). From these data, peak O2uptake, anaerobic threshold, peak O2pulse, and other parameters were analyzed by standard techniques (2,3,19 –22).
Calculation of percent predicted values. All resting lung function and CPET values were reported in absolute terms and normalized to percent of predicted (%pred). Predicted spirometry values were calculated using accepted equations for Caucasians, Hispanics, and Blacks (23), with Asian values considered equal to Blacks (24). Predicted DLCOand VA⬘were calculated using nonsmoker equations for sians and Hispanics (25); and 0.93 and 0.88 of the Cauca-sian values for ACauca-sian and Black adult patients, respectively (26). Separate predicting equations were used for those under age 20 (27). Predicted DLCOvalues were corrected for measured hemoglobin concentration (28). All predicted values of CPET parameters were calculated as previously reported (2,3,19,29).
Abbreviations and Acronyms
CPET ⫽cardiopulmonary exercise test
DLCO ⫽diffusing capacity of the lung for carbon
monoxide or gas transfer index FEV1 ⫽forced expiratory volume in 1 second
FVC ⫽forced vital capacity
MVV ⫽maximum voluntary ventilation NYHA⫽New York Heart Association %pred ⫽percent predicted
PPH ⫽primary pulmonary hypertension TLC ⫽total lung capacity
VA⬘ ⫽effective alveolar volume
Table 1. Demographics and Cardiopulmonary Exercise Testing Parameters in PPH Patients and Control Subjects PPH Patients (nⴝ79) Control Subjects (nⴝ20) Age (yrs) 44⫾13 45⫾12 Gender (F/M) 71/8 15/5 Height (cm) 164⫾9 169⫾9 Weight (kg) 73⫾18 81⫾24
Body mass index (kg/m2) 27⫾6 28⫾8
Hemoglobin (g/dl) 14.9⫾2.0* 13.6⫾1.5
NYHA class 2.7⫾0.6 —
mPAP (mm Hg) 60⫾18 —
Peak O2uptake, l/min (%pred) 0.78⫾0.26 (45⫾13)‡ 1.87⫾0.48 (97⫾18)
Peak work rate, W (%pred) 47⫾24 (37⫾17)‡ 151⫾45 (104⫾24) Anaerobic threshold, l/min (%pred) 0.59⫾0.18 (59⫾15)‡ 0.98⫾0.20 (89⫾14) Peak O2pulse, ml/beat (%pred) 5.9⫾1.9 (69⫾17)‡ 12.0⫾3.2 (108⫾16)
Peak heart rate, beats/min (%pred) 133⫾21 (76⫾11)† 156⫾16 (89⫾8) Peak ventilation, l/min (%MVV) 43⫾15 (47⫾13)* 72⫾19 (58⫾10) Values are expressed as mean⫾SD and percentage of measured to predicted values (%pred).
*p⬍0.05, †p⬍0.001, ‡p⬍0.0001, vs. controls using unpairedttest.
mPAP⫽mean pulmonary artery pressure; %MVV⫽percentage of maximum voluntary ventilation; NYHA class⫽New York Heart Association heart failure classification; PPH⫽primary pulmonary hypertension; %pred⫽percent predicted
Statistical analyses. Parameters were expressed as mean⫾ SD, except where specifically noted. Individual values within two-tailed 95% confidence limits were considered normal. The Student-Newman-Keuls tests were performed for the repeated-measures analyses of variance. Individual linear regression analyses were performed. Pearson
correla-tion coefficients were performed for all pulmonary funccorrela-tion and exercise values, which were normally distributed, whereas Spearman rank correlation coefficients were per-formed for NYHA class. To ascertain the relative signifi-cance of resting lung function parameters to CPET param-eters, multicollinearity analyses were done. Stepwise regression with forward selection and backward elimination was used, eliminating variables with an alpha of p⬎ 0.05.
RESULTS
Demographics of PPH patients and controls. The female-to-male ratio of the PPH patients in this study was 9:1 (Table 1). The control population, by design, had a similar female-to-male ratio. The resting lung function and CPET parameters of the control group were within normal limits (Tables 1 and 2). Using arabic numerals to grade NYHA class, the PPH patients both had an average NYHA class of 2.7. The hemoglobin concentration in the PPH group was significantly higher than the controls.
All individuals completed their CPET studies without incident or untoward effects. Nearly all patients stopped exercise because of dyspnea and/or leg fatigue; uncom-monly, patients noted palpitations or lightheadedness. The magnitude of the absolute and percent of predicted peak O2 uptake, and all of the other measured parameters of cardio-vascular function and ventilatory efficiency was strikingly abnormal, and similar to those seen in a smaller group of PPH patients previously reported (2).
Resting lung function. Mean FVC (80 %pred), FEV1(79 %pred), and VA⬘ (83 %pred) showed mild, albeit highly significant reductions (p⬍0.001 to p⬍0.0001) in the PPH group (Table 2), with values ranging from 46% to 118%, 40% to 121%, and 55% to 126 %pred, respectively. Approximately half of the FVC measurements, as well as the FEV1, VA⬘, and TLC values, were below 80 %pred, a level approximating the lower limit of normal (Fig. 1, upper). The FEV1/FVC was 98
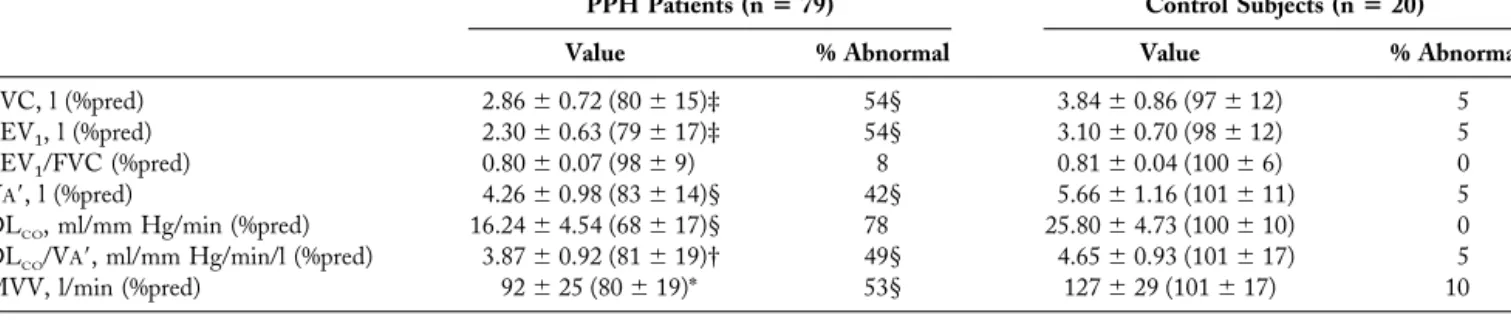
⫾9 %pred (Table 2 and Fig. 2, upper left), providing evidence that airway obstruction is unusual in patients with PPH. In contrast, the proportional reductions in FEV1 and FVC indicate that a restrictive ventilatory defect was common (Table 2). In Figure 2, the regression lines (solid lines) of Table 2. Resting Lung Function in PPH Patients and Control Subjects
PPH Patients (nⴝ79) Control Subjects (nⴝ20)
Value % Abnormal Value % Abnormal
FVC, l (%pred) 2.86⫾0.72 (80⫾15)‡ 54§ 3.84⫾0.86 (97⫾12) 5 FEV1, l (%pred) 2.30⫾0.63 (79⫾17)‡ 54§ 3.10⫾0.70 (98⫾12) 5 FEV1/FVC (%pred) 0.80⫾0.07 (98⫾9) 8 0.81⫾0.04 (100⫾6) 0 VA⬘, l (%pred) 4.26⫾0.98 (83⫾14)§ 42§ 5.66⫾1.16 (101⫾11) 5 DLCO, ml/mm Hg/min (%pred) 16.24⫾4.54 (68⫾17)§ 78 25.80⫾4.73 (100⫾10) 0 DLCO/VA⬘, ml/mm Hg/min/l (%pred) 3.87⫾0.92 (81⫾19)† 49§ 4.65⫾0.93 (101⫾17) 5 MVV, l/min (%pred) 92⫾25 (80⫾19)* 53§ 127⫾29 (101⫾17) 10
Values are expressed as mean⫾SD and percentage of measured to predicted values (%pred). *p⬍0.05, †p⬍0.01, ‡p⬍0.001, §p⬍0.0001, vs. controls using unpairedttest or chi-square test.
DLCO⫽gas transfer index or diffusing capacity for carbon monoxide; FEV1⫽forced expiratory volume in 1 second; FVC⫽forced vital capacity; MVV⫽maximum voluntary ventilation; VA⬘ ⫽effective alveolar volume. Other abbreviations as in Table 1.
Figure 1. Distribution of values for forced vital capacity (FVC)(upper)
and gas transfer index or diffusing capacity for carbon monoxide (DLCO)
(lower)in 79 primary pulmonary hypertension (PPH) patients(lines from upper left to lower right)and 20 normal controls(lines from lower left to upper right). Values are divided by deciles of percent predicted (%pred). For these measurements, all individuals below 80% of predicted are below the normal 95% confidence limits. Approximately 50% of the PPH patients have a reduced FVC and 75% have a reduced DLCO.
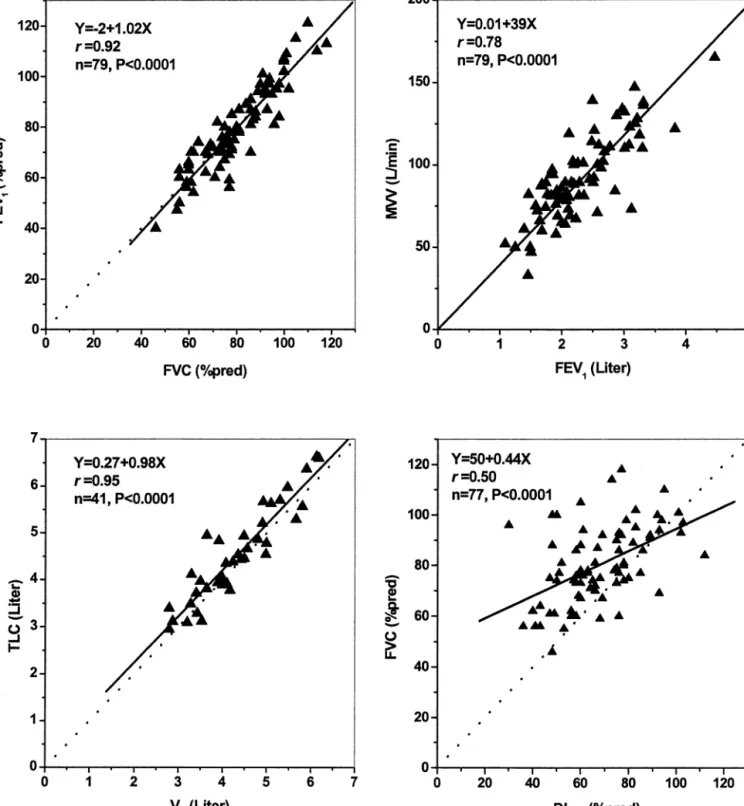
FEV1-versus-FVC and VA⬘-versus-TLC had nonsignificant intercepts (p ⬎ 0.05 vs. 0) and similar slopes to the line of identity (dotted lines, p⬎0.05). The ratio of directly measured MVV to the FEV1was 39 ⫾ 9 (Fig. 2, upper right). This
MVV/FEV1ratio is similar to that found in the control group and in patients with obstructive lung disease, but lower than that found in patients with interstitial lung disease (19).
Only two patients could not perform the necessary Figure 2. Correlation of resting lung function measurements in 79 primary pulmonary hypertension (PPH) patients. Eachsymbolindicates an individual PPH patient.Upper left:Values are percent predicted (%pred) for FVC and FEV1;upper right:absolute values for FEV1and MVV;lower left:absolute
values for alveolar volume determined from single breath dilution of inert gas (VA⬘) and TLC determined by body plethysmography or N2washout method; andlower right:%pred values for DLCOand FVC. The mean⫾SD of their sample ratio values are: FEV1/FVC⫽0.99⫾0.09, MVV/FEV1⫽39⫾
7, and VA⬘/TLC⫽0.96⫾0.03.Solid linesare the regressions lines for the data;dotted linesare the lines of identity. DLCO⫽gas transfer index; FEV1
⫽forced expiratory volume in 1 s; FVC⫽forced vital capacity; MVV⫽maximum voluntary ventilation; TLC⫽total lung capacity; VA⬘ ⫽effective alveolar volume.
maneuvers for measurement of DLCO and VA⬘. In slightly over three-fourths of the remaining PPH patients, the DLCOvalues were below 80% of predicted, that is, the lower limit of normal (Fig. 1, lower) and generally reduced to a greater extent than the FVC (Fig. 2, lower right). The mean DLCOwas 68⫾17 %pred (p⬍0.0001) with a range of 32% to 114%pred (Table 2 and Fig. 2, lower right). Method-ologically, when a patient has a good inspiratory volume (at least 90% of the vital capacity) during the single breath maneuver required for the DLCOmeasurement and a normal hemoglobin concentration (as did these PPH patients), a reduced DLCO can be due only to a real reduction in pulmonary alveolar capillary bed or maldistribution of ven-tilation to the alveoli during the single breath maneuver, or both. The near equality of VA⬘and TLC, (VA⬘/TLC⫽96
⫾ 3%, Fig. 2, lower left) demonstrate that maldistribution of ventilation does not account for the low DLCO.
In contrast to the PPH patients who, on average, dem-onstrated mild restriction and moderate loss of diffusing capacity (Fig. 1 and 2), the resting lung function measure-ments in the controls were rarely outside of the 95% confidence limits for normal subjects (Table 2 and Fig. 1). Despite the frequency of dyspnea as a symptom and the reduced FVC, FEV1, and MVV in the PPH patients, the ratio of peak exercise ventilation to MVV was significantly lower than that of the controls (Table 1), indicating that the decreased ventilatory capacity of the PPH group (Table 2) did not appear to limit their maximal exercise capacity.
Correlations of resting lung function to CPET, NYHA class, and resting cardiac catheterization measurements.
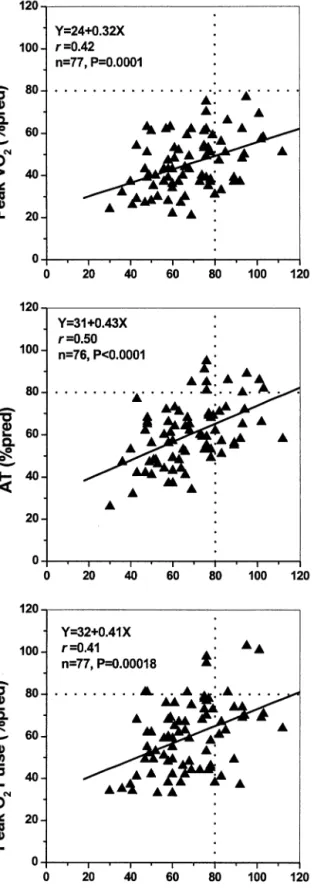
Because patients and controls varied in age, gender, and size, and because all correlations were higher using %pred than with absolute values, only %pred values are used to establish correlation (Table 3). The DLCOwas most highly correlated with peak O2uptake (peak O2uptake ⫽ 24 ⫹ 0.32 ⫻DLCO,r ⫽ 0.42, SD⫽12, n ⫽77, p⫽ 0.0001), anaerobic threshold (anaerobic threshold⫽ 31 ⫹ 0.43 ⫻ DLCO,r⫽0.50, SD⫽13, n⫽76, p⬍0.0001), and peak O2pulse (peak O2pulse⫽32⫹ 0.41⫻DLCO,r⫽ 0.41, SD ⫽ 16, n ⫽ 77, p ⫽ 0.0002), although DLCO also correlated significantly with peak work rate and NYHA class. The relationships of %pred peak O2uptake, anaerobic threshold, and peak O2 pulse to DLCO are shown for the
PPH patients as shown in Figure 3. Although other PFT parameters (FVC, FEV1, MVV, and VA⬘) correlated sig-nificantly with many CPET parameters and NYHA class, the highestrvalues and most significant p values were those for DLCO. There were no significant correlations of any resting lung function parameter with resting mean pulmo-nary artery pressure, cardiac output, pulmopulmo-nary vascular resistance, or other values obtained during right heart catheterization.
Multicollinearity regression analysis of resting lung function and CPET measurements of aerobic function.
Using all resting lung function factors for stepwise regres-sion analysis, the only significant independent factor that was a determinant for peak O2uptake, anaerobic threshold, or peak O2 pulse was DLCO (Fig. 3). The equations were similar to the equations derived using simple regression correlation.
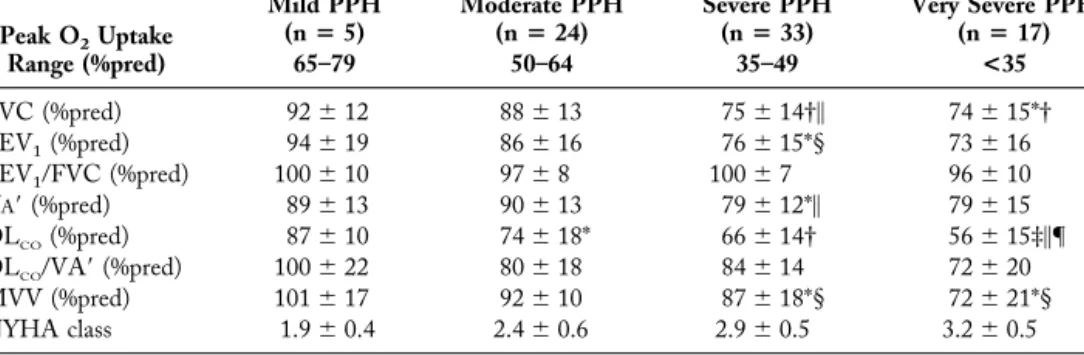
Physiologic severity. The PPH patients were divided into four categories of severity (Table 4) according to their %pred peak O2 uptake: 1) mild, 65 to 79 %pred; 2) moderate, 50 to 64 %pred; 3) severe, 35 to 49 %pred; and 4) very severe,⬍35 %pred, as was done in a previous analysis of CPET in PPH patients (2). Clearly shown is the tendency to a progressive decrease in the resting lung function measures, especially DLCO, as the severity of PPH increases, using either %pred peak O2 uptake or NYHA class (p⬍0.05 to p⬍ 0.001).
DISCUSSION
Resting lung function correlates with PPH severity. The objective of this study was to determine whether the pattern of abnormality in resting lung function is related to NYHA symptom class, resting hemodynamics, and CPET-based disease severity in patients with PPH. To minimize con-founding factors due to differences in age, gender, or size, our analysis is primarily based on %pred values. Although the study was limited because disease duration and follow-up were not considered in the analysis, the data in Table 4 suggest that the severity of the disease, estimated by either NYHA classification or CPET, parallels the abnor-mality of some resting lung function tests at the time of the patient’s referrals (not necessarily initial diagnoses) to the Table 3. Pearson Correlation Coefficients Relating Resting Lung Function Parameters to CPET
and NYHA Class in PPH Patients
Resting Lung Function and CPET Parameters
FVC (%pred) FEV1 (%pred) VAⴕ (%pred) DLCO (%pred) DLCO/VAⴕ (%pred) MVV (%pred)
Peak O2uptake (%pred) 0.34† 0.33† 0.32† 0.42§ 0.20* 0.31†
Anaerobic threshold (%pred) 0.33† 0.31† 0.31† 0.50§ 0.28† 0.27†
Peak O2pulse (%pred) 0.27† 0.26* 0.18 0.41§ 0.32† 0.19
Peak work rate (%pred) 0.29† 0.31† 0.34† 0.35‡ 0.1 0.30†
Peak ventilation (%MVV) ⫺0.14 ⫺0.24* 0.08 0.03 ⫺0.07 ⫺0.35†
Peak heart rate (%pred) 0.17 0.17 0.27† 0.06 ⫺0.20* 0.23*
NYHA class ⫺0.20* ⫺0.20* ⫺0.33† ⫺0.27† ⫺0.04 ⫺0.1
*p⬍0.05, †p⬍0.01, ‡p⬍0.001, §p⬍0.0001. Abbreviations as in Tables 1 and 2.
PPH clinic. These resting lung function findings are mod-erate reductions in DLCO and mild, albeit statistically significant, reductions in FVC, FEV1, MVV, TLC, and VA⬘. Conversely, airway obstruction and maldistribution of ventilation are uncommon.
Restriction, as evidenced by reductions in FEV1, FVC, VA⬘, TLC, and DLCO have been reported in other series (6,10,30) of patients with PPH, but the degree and propor-tion of patients with these abnormalities are generally larger in our study. Because reference values derived from normal populations have a large variance for FVC and TLC, the finding of a VA⬘within normal limits in 58% of the PPH patients does not exclude a developing restrictive process in some patients, as sequential measurements were not made. However, any developing restrictive process, per se, is not a likely explanation for the exercise dyspnea of our PPH patients since, at peak exercise, PPH patients had both a lower ratio of ventilation relative to their resting MVV and a proportionally larger breathing reserve than did our control population. In addition, their symptoms were gen-erally well out of proportion to their degree of ventilatory restriction.
The finding that the VA⬘ measured by a single breath averaged 96% of the TLC measured by plethysmography or nitrogen washout, with a standard deviation of only 3%, is strong evidence against maldistribution of ventilation in the PPH patients. If maldistribution of ventilation were part of PPH, the TLC would have been considerably higher than the VA⬘ In comparing resting lung function values in a normal population, ratio values have a much lower coeffi-cient of variation than do absolute values (31). Therefore, the nearly universally normal FEV1/FVC ratio (Fig. 1) indicates that obstructive airways disease was uncommonly present in our patients with PPH. The fact that the FEV1/FVC was rarely increased and that the overall MVV-to-FEV1ratio was not appreciably or significantly increased over the normal value of 40 (Fig. 2) is evidence against lung fibrosis with increased elastic recoil, as is commonly found in patients with interstitial lung disease (19). These resting lung function findings fit with those from other reports in PPH patients (6 – 8,10), except that prior reports did not find significant correlations between resting lung function and disease severity.
Probable causes of reduction in DLCO. Importantly, the
overall reduction in mean resting DLCOin most of our PPH patients (Figs. 1 and 2, Table 2) strongly suggests that, even at rest, pulmonary capillary blood volume was reduced. This reduction fits the pathological findings typical of PPH, described by Meyrick and Reid (32)—that is, musculariza-tion of smaller, more peripheral pulmonary arteries, medial thickening of the muscular arteries, intimal thickening, and a reduction in peripheral vascular bed. The possible effect of smoking causing the low DLCO, values in the eight men in this study was investigated because the prediction equations of Miller et al. (25) indicate a reduction in DLCO in men, but not women, smokers. For these eight men, the DLCO
Figure 3. Correlations and regression equations for gas transfer index (DLCO) versus three cardiopulmonary exercise test parameters of aerobic
function (upper⫽peak O2uptake;middle⫽anaerobic threshold; lower
⫽ peak O2 pulse) in primary pulmonary hypertension (PPH) patients.
Eachsymbolindicates an individual PPH patient. All values and equations are in units of % predicted (%pred).Dotted linesapproximate the 95% confidence limits of controls.
were 77%, 75%, and 65% of predicted in the three never-smokers and 68%, 66%, 63%, 53%, and 49% in the ex-smokers. Using Miller’s predicting equations (25) for men smoking one and a half packs per day (though none of these five men had smoked this heavily), their % predicted DLCOall remained abnormal, increasing an average of 9%. Thus, smoking was unlikely to be more than a minor factor in the overall reduction in DLCOin this study. The reduc-tion in DLCO cannot be attributed to maldistribution of ventilation, because the VA⬘ (measured concurrently with the DLCOduring 10-s breathholding at full inspiration) was approximately 96% of the separately measured TLC. Hence, all the study findings support the concept that the reduced DLCO in PPH patients must be attributable to a reduction in perfused pulmonary capillary bed rather than maldistribution of ventilation or anemia. Furthermore, the lung function findings in this study do not fit the pattern found in patients with interstitial lung disease and secondary pulmonary hypertension, as in such patients the restriction tends to be more severe, with the FEV1/FVC and MVV/ FEV1ratios abnormally increased (10,19).
Possible causes of restriction. What are the possible causes of lung restriction in PPH? The PPH patients were not more overweight than the controls or general popula-tion, and no evidence was observed for chest wall disease, lung fibrosis, pleural effusions, or left ventricular failure in these patients. Patients with severe left ventricular failure commonly have lung restriction (32–34), but following heart transplant, the TLC may increase by 400 to 1,000 ml, presumably due to the fact that the transplanted heart is smaller (34). We conjecture that cardiomegaly with right ventricular hypertrophy and dilation may account for some of the reduction in lung volume in the PPH patients. Additionally, because lung expansion depends on the dis-tensibility (compliance) of all lung tissues including the pulmonary vasculature, loss of the normal distensibility of the smaller arteries radiating out into the lung periphery may be an important factor causing lung restriction in these patients.
Clinical implications. The positive correlations of the DLCO, FVC, FEV1, and VA⬘ values with multiple CPET
parameters and NYHA class support the hypothesis that a close relationship exists between the processes that causes each to become abnormal (Table 4, Fig. 3). However, the greater proportional reduction in DLCOthan in FVC (Fig. 2) and TLC in our PPH patients supports the findings that the primary pathological process involves the blood vessels of the lungs. These simple, safe, and patient-friendly resting lung function measurements can be clinically useful in suspecting (but not excluding) the diagnosis of PPH in patients who have unexplained dyspnea on exertion. Whether or not they are useful in following the course of the disease remains to be seen.
Reprint requests and correspondence: Dr. James E. Hansen, St. John’s Cardiovascular Research Center, 1124 West Carson Street, Box 405, Torrance, California 90509-2910. E-mail: jimandbev@ cox.net.
REFERENCES
1. Rubin LJ. Current concepts: primary pulmonary hypertension. N Engl J Med 1997;336:111–7.
2. Sun XG, Hansen JE, Oudiz RJ, Wasserman K. Exercise pathophys-iology in patients with primary pulmonary hypertension. Circulation 2001;104:429 –35.
3. Sun XG, Hansen JE, Oudiz RJ, Wasserman K. Gas exchange detection of exercise-induced right-to-left shunt in patients with primary pulmonary hypertension. Circulation 2002;105:54 –60. 4. Rich S. Executive summary from the World Symposium on primary
pulmonary hypertension 1998. World Health Organization Web site. Available at: www.who.int/ncd/cvd/pph.html. Accessed February 19, 2001.
5. Rubin LJ. Clinical diagnosis of pulmonary vascular disease. In: Cagle PT, editor. Diagnostic Pulmonary Pathology. New York, NY: Marcel Dekker, 2000:429 –36.
6. Rich S, Dantzker DR, Ayres SM, et al. Primary pulmonary hyperten-sion. A national prospective study. Ann Intern Med 1987;107:216 –23. 7. D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med 1991;115:343–9.
8. Steenhuis LH, Groen HJM, Koeter GH, van der Mark ThW. Diffusion capacity and haemodynamics in primary and chronic throm-boembolic pulmonary hypertension. Eur Respir J 2000;16:276 –81. 9. Kindman LA, Vagelos RH, Willson K, Prikazky L, Fowler M.
Abnormalities of pulmonary function in patients with congestive heart failure, and reversal with ipratropium bromide. Am J Cardiol 1994; 73:258 –62.
Table 4. Resting Lung Function in PPH Patients Grouped by Severity of Reduction in Peak ˙VO2 Peak O2Uptake Range (%pred) Mild PPH (nⴝ5) Moderate PPH (nⴝ24) Severe PPH (nⴝ33) Very Severe PPH (nⴝ17) 65–79 50–64 35–49 <35 FVC (%pred) 92⫾12 88⫾13 75⫾14†㛳 74⫾15*† FEV1(%pred) 94⫾19 86⫾16 76⫾15*§ 73⫾16 FEV1/FVC (%pred) 100⫾10 97⫾8 100⫾7 96⫾10 VA⬘(%pred) 89⫾13 90⫾13 79⫾12*㛳 79⫾15 DLCO(%pred) 87⫾10 74⫾18* 66⫾14† 56⫾15‡㛳¶ DLCO/VA⬘(%pred) 100⫾22 80⫾18 84⫾14 72⫾20 MVV (%pred) 101⫾17 92⫾10 87⫾18*§ 72⫾21*§ NYHA class 1.9⫾0.4 2.4⫾0.6 2.9⫾0.5 3.2⫾0.5
*p⬍0.05, †p⬍0.01, ‡p⬍0.001 vs. mild PPH. §p⬍0.05,㛳p⬍0.01 vs. moderate PPH. ¶p⬍0.05 vs. severe PPH using repeated analysis of variance.
10. Riley MS, Po´rsza´sz J, Engelen MPK, Wasserman K. Gas exchange response to continuous incremental cycle ergometry exercise in primary pulmonary hypertension in humans. Eur J Appl Physiol 2000;83:63– 70.
11. D’Alonzo GE, Bower JS, Dantzker DR. Differentiation of patients with primary and thromboembolic pulmonary hypertension. Chest 1984;85:457–64.
12. D’Alonzo GE, Gianotti LA, Pohil RL, et al. Comparison of progres-sive exercise performance of normal subjects and patients with primary pulmonary hypertension. Chest 1987;92:57–62.
13. Wensel R, Opitz CF, Ewert R, Bruch L, Kleber FX. Effects of iloprost inhalation on xercise capacity and ventilatory efficiency in patients with primary pulmonary hypertension. Circulation 2000;101:2388 –92. 14. Wax D, Garofano R, Barst RJ. Effects of long-term infusion of
prostacyclin on exercise performance in patients with primary pulmo-nary hypertension. Chest 1999;116:914 –20.
15. American Thoracic Society. Standardization of spirometry (1994 update ATS statement). Am J Respir Crit Care Med 1995;152:1107–36. 16. American Thoracic Society. Single-breath carbon monoxide
diffus-ing capacity (transfer factor). Recommendations for a standard technique—1995 update. Am J Respir Crit Care Med 1995;152: 2185–98.
17. Crapo RO, Morris AH, Clayton PD, Nixon CR. Lung volumes in healthy nonsmoking adults. Bull Euro Physiopath Resp 1982;18:419 – 25.
18. Hyatt RE, Scanlon PD, Nakamura M. Interpretation of Pulmonary Function Tests: A Practical Guide. Philadelphia, PA: Lippincott Williams & Wilkins, 1997.
19. Wasserman K, Hansen JE, Sue DY, Casaburi R, Whipp BJ. Principles of the Exercise Testing and Interpretation. 3rd ed. Baltimore, MD: Lippincott Williams & Wilkins, 1999:65–93, 144 –162.
20. Beaver WL, Wasserman K, Whipp BJ. A new method for detecting the anaerobic threshold by gas exchange. J Appl Physiol 1986;60: 2020 –7.
21. Metra M, Dei Cas L, Panina G, et al. Exercise hyperventilation in chronic congestive heart failure, and its relation to functional capacity and hemodynamics. Am J Cardiol 1992;70:622–8.
22. Sietsema KE, Daly JA, Wasserman K. Early dynamics of O2uptake
and heart rate as affected by exercise rate. J Appl Physiol 1989;67: 2535–41.
23. Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med 1999;159:179 –87.
24. Seltzer CC, Siegelaub AB, Friedman GD, Collen MF. Differences in pulmonary function related to smoking habits and race. Am Rev Respir Dis 1974;110:598 –608.
25. Miller A, Thornton JC, Warshaw R, Anderson H, Teirstein AS, Selikoff IJ. Single breath diffusing capacity in a representative sample of the population of Michigan, a large industrial state: predicted values, lower limits of normal, and frequencies of abnormality by smoking history. Am Rev Respir Dis 1983;127:270 –7.
26. American Thoracic Society (Medical Section of the American Lung Association). Lung function testing: selection of preference values and interpretative strategies. Am Rev Respir Dis 1991;144:1202–18. 27. Polgar C, Promodhat V. Pulmonary Function in Children:
Tech-niques and Standards. Philadelphia, PA: WB Saunders, 1971:254. 28. Clark EH, Woods RL, Hughes JMB. Effect of blood transfusion on
the carbon monoxide transfer factor of lung in man. Clin Sci Mol Med 1978;54:627–31.
29. Hansen JE, Sue DY, Wasserman K. Predicted values for clinical exercise testing. Am Rev Respir Dis 1984;129:S49 –55.
30. Phipps B, Wang G, Chang CHJ, Dunn M. Unexplained severe pulmonary hypertension in the old age group. Chest 1983;84:399 – 402.
31. Hansen JE, Sue DY. Resolution of the differences in reference FEV1/FVC values. Respir Ther 1983;13:51–9.
32. Meyrick B, Reid L. Pulmonary hypertension. Anatomic and physio-logic correlates. Clin Chest Med 1983;4:199 –217.
33. Naum CC, Sciurba FC, Rogers RM. Pulmonary function abnormal-ities in chronic severe cardiomyopathy preceding cardiac transplanta-tion. Am Rev Respir Dis 1992;145:1334 –8.
34. Hosenpud JD, Stibolt TA, Atwal K, Shelley D. Abnormal pulmonary function specifically related to congestive heart failure: comparison of patients before and after cardiac transplantation. Am J Med 1990;88: 493–6.