ContentslistsavailableatScienceDirect
European
Journal
of
Radiology
jo u r n al ho me p a g e : w w w . e l s e v i e r . c o m / l o c a t e / e j r a d
Lung
nodule
detection
performance
in
five
observers
on
computed
tomography
(CT)
with
adaptive
iterative
dose
reduction
using
three-dimensional
processing
(AIDR
3D)
in
a
Japanese
multicenter
study:
Comparison
between
ultra-low-dose
CT
and
low-dose
CT
by
receiver-operating
characteristic
analysis
Yukihiro
Nagatani
a,∗,
Masashi
Takahashi
a,
Kiyoshi
Murata
a,
Mitsuru
Ikeda
b,
Tsuneo
Yamashiro
c,
Tetsuhiro
Miyara
c,d,
Hisanobu
Koyama
e,
Mitsuhiro
Koyama
f,
Yukihisa
Sato
g,h,
Hiroshi
Moriya
i,
Satoshi
Noma
j,
Noriyuki
Tomiyama
g,
Yoshiharu
Ohno
e,
Sadayuki
Murayama
c,
for
the
investigators
of
ACTIve
study
group
aDepartmentofRadiology,ShigaUniversityofMedicalScience,Otsu520-2192,Shiga,Japan
bDepartmentofRadiologicalandMedicalLaboratoryScience,NagoyaUniversityGraduateSchoolofMedicine,Nagoya461-8673,Aichi,Japan cDepartmentofRadiology,GraduateSchoolofMedicalScience,UniversityoftheRyukyus,Nishihara903-0215,Okinawa,Japan
dDepartmentofRadiology,OkinawaPrefecturalYaeyamaHospital,Ishigaki907-0022,Okinawa,Japan eDepartmentofRadiology,KobeUniversityGraduateSchoolofMedicine,Kobe650-0017,Hyogo,Japan fDepartmentofRadiology,OsakaMedicalCollege,Takatsuki569-8686,Osaka,Japan
gDepartmentofRadiology,OsakaUniversityGraduateSchoolofMedicine,Suita565-0871,Osaka,Japan
hDepartmentofRadiology,OsakaMedicalCenterofCancerandCardiovascularDiseases,Osaka537-8511,Osaka,Japan iDepartmentofRadiology,OharaGeneralHospital,Fukushima960-8611,Japan
jDepartmentofRadiology,TenriHospital,Tenri632-8552,Nara,Japan
a
r
t
i
c
l
e
i
n
f
o
Articlehistory:
Received17December2014 Receivedinrevisedform3March2015 Accepted8March2015
Keywords:
Computedtomography Chest
Ultra-lowdosescanning Adaptiveiterativedosereduction Imagequality
a
b
s
t
r
a
c
t
Purpose:Tocomparelungnoduledetectionperformance(LNDP)incomputedtomography(CT)with adaptiveiterativedosereductionusingthreedimensionalprocessing(AIDR3D)betweenultra-lowdose CT(ULDCT)andlowdoseCT(LDCT).
Materialsandmethods:ThiswaspartoftheArea-detectorComputedTomographyfortheInvestigation ofThoracicDiseases(ACTIve)Study,amulticenterresearchprojectbeingconductedinJapan. Institu-tionalReviewBoardapprovedthisstudyandinformedconsentwasobtained.Eighty-threesubjects (bodymassindex,23.3±3.2)underwentchestCTat6institutionsusingidenticalscannersand pro-tocols.Inasinglevisit,eachsubjectwasscannedusingdifferenttubecurrents:240,120and20mA(3.52, 1.74and0.29mSv,respectively).AxialCTimageswith2-mmthickness/incrementwerereconstructed usingAIDR3D.Standardofreference(SOR)wasdeterminedbasedonCTimagesat240mAbyconsensus readingof2board-certificatedradiologistsastothepresenceoflungnoduleswiththelongestdiameter (LD)ofmorethan3mm.Another5radiologistsindependentlyassessedandrecordedpresence/absence oflungnodulesandtheirlocationsbycontinuously-distributedratinginCTimagesat20mA(ULDCT) and120mA(LDCT).Receiver-operatingcharacteristic(ROC)analysiswasusedtoevaluateLNDPofboth methodsintotalandalsoinsubgroupsclassifiedbyLD(>4,6and8mm)andnodularcharacteristics (solidandgroundglassnodules).
Results:ForSOR,161solidand60groundglassnoduleswereidentified.NosignificantdifferenceinLNDP forentiresolidnoduleswasdemonstratedbetweenbothmethods,asareaunderROCcurve(AUC)was 0.844±0.017inULDCTand0.876±0.026inLDCT(p=0.057).ForgroundglassnoduleswithLD8mm ormore,LNDPwassimilarbetweenbothmethods,asAUC0.899±0.038inULDCTand0.941±0.030in LDCT.(p=0.144).
∗Correspondingauthor.Tel.:+81775643885.
E-mailaddress:[email protected](Y.Nagatani). http://dx.doi.org/10.1016/j.ejrad.2015.03.012
0720-048X/© 2015The Authors.Publishedby Elsevier Ireland Ltd.This is anopen accessarticle underthe CC BY-NC-NDlicense(http://creativecommons.org/ licenses/by-nc-nd/4.0/).
Conclusion:ULDCTusingAIDR3Dwithanequivalentradiationdosetochestx-raycouldhavecomparable LNDPtoLDCTwithAIDR3Dexceptforsmallergroundglassnodulesincaseswithnormalrangebody habitus.
©2015TheAuthors.PublishedbyElsevierIrelandLtd.ThisisanopenaccessarticleundertheCC BY-NC-NDlicense(http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
NationalLungScreening Trial(NLST)had demonstrated that screeningwiththeuseoflow-dosecomputedtomography(LDCT) reduceslung cancer mortality ratecompared withchest X-ray
[1].TheguidelinerecentlyissuedbytheAmericanCancerSociety recommendstheinitialscreeningwithlow-doseCTforapparently healthycurrentandformersmokerswithintheagerange of55 to74years[2].However,carcinogenesisisastochasticinfluenceof radiation,anditsprobabilityincreaseswitheffectiveradiationdose andfurtherreductionoftheradiationdosewithoutlosingimage qualitywouldbedesirable[3,4].
Imagenoiseisinverselyincreasedwithradiationdose reduc-tion. To overcome this dilemma, various image reconstruction kernelsand filtershavebeendevelopedinconjunctionwith fil-tered backprojection (FBP).However, standard FBP algorithms havemajordeficitsrelatedtonoisereductionbecausetheydonot considercertainopticalchaindetails[5,6].Indeed,these recons-tructionsyield a significant increase of image noise in case of excessivedosereduction[7].Iterativereconstructionalgorithms, suchas SinogramAffirmedIterativeReconstruction bySiemens Healthcare[8,9]andModelBasedIterativeReconstruction(MBIR) byGEHealthcare[10,11]provideimageswithlessnoisecompared withfilteredbackprojectionalgorithmregardlessofthenecessary longerimagereconstructiontime[12,13].
Adaptive Iterative Dose Reduction using Three Dimensional Processing(AIDR3D)byToshibaMedicalSystemstakesaccount ofelectricalnoiseandphotonnumbertoestimateprojectionnoise inLDCTanditsadvantagehasbeenalsorecognizedforchestCT.
[14–16].Wedemonstrated inapreviousprospectivestudythat scanswithAIDR3Dat60mA(0.63mSv)weresuperioror equiv-alent tothose withoutAIDR at 120mA (1.26mSv) in terms of imagequalityforvariouspatternsoflungdiseasesincluding bron-chiolitisand diffuselung disease[17].Greater reduction ofthe radiationdosecanbealsorealizedforthepurposeoflungnodule detection.Itispresumedthatultra-low-doseCT(ULDCT)usinga radiationdoselevelequivalenttochestX-raywithiterative recon-structiontechniquecouldpreservenodulardetectabilityonchest CTimagesandrepresentanalternativescreeningmethodoflung cancer.ULDCTwithMBIR(0.20mSv)showeddetectionsensitivity comparabletoLDCTwithadaptiveiterativereconstruction,with respecttopulmonarynodulesincludingrelativelylargernon-solid nodules,whichmeansizeis8.0mmingroundglassnodulesand 11.3mminpart-solidnodules[18].Tothebestofourknowledge,no prospectivemulti-centerclinicalstudiesassessingthediagnostic performanceofULDCTusingAIDR3Dincludingsub-groups analy-sesbasedonthenodularsizeandcharacteristicswithconsiderable nodulenumbershavebeenperformed.
Thepurposeofthisstudyistocomparelungnoduledetectability (LND)withAIDR3DbetweenULDCT(20mA)andLDCT(120mA)in thetotalstudypopulationandsub-groupsclassifiedbythenodular longestdiameter(>4mm,>6mmand>8mm)andnodular charac-teristics(solidandgroundglassnodules).
2. Materialsandmethods
ThisstudywasconductedaspartoftheArea-detectorComputed TomographyfortheInvestigationof ThoracicDiseases(ACTIve) Study, an ongoing multi-center research project in Japan. The
researchcommitteeofthestudyprojectoutlinedandapprovedour studyprotocols.TheInstitutionalReviewBoardofeachinstitution approvedthisstudy,andwritteninformedconsentwasobtained fromalltheparticipants.
2.1. Studypopulations
From December 2012 to March 2013, a total of 112 sub-jectswereinitiallyenrolledinthisstudyatsixinstitutions:Kobe University,OharaGeneralHospital,OsakaUniversity,Tenri Hos-pital,ShigaUniversity of MedicalScience andUniversity ofthe Ryukyus.Twenty-ninepatientswereexcludedduetovarious rea-sons;finally,83subjectswereevaluatedinthisstudy,including42 femalesand41males,withameanageof63.9±12.0years(Fig.1). 2.2. Imagedataacquisition
During a singlevisit each, the 83 subjects underwent plain 64 chest CT (64-row helical mode) using identical 320-row MDCTscanners(AquilionONE,ToshibaMedicalSystems,Otawara, Tochigi,Japan).Eachsubjectwasscannedthreetimesusing dif-ferenttubecurrents(240,120and20mA)withthesamerotation time(0.35s).Thus,aneffectivetubecurrentforpatientexposureof 84,42and7mAswasobtainedusingthisshortrotationtime. Scan-ningfieldofview(FOV)wasselectedfromtwosettingsonthebasis ofthepatients’bodyhabitus,400mm(large)and320(medium). Otherscanningandreconstructionparameterswerefixed:tube voltage=120kVp;collimation=0.5mm;beampitch=0.828 (heli-cal pitch 53) and reconstruction kernel: FC52. Scan data were convertedtoCTimagesusingAIDR3D,and3CTserieswithAIDR3D weremadeforeachpatient.TheAIDR3Dmodedidnotrequire addi-tionalprocessingtime;thus,CTimagesacquiredwithAIDR3Dwere createdassoonasdatascanningwascompleted.All249CTseries (3series×83subjects)wereanonymizedandstoredina worksta-tionviewerconnectedtotheCTconsole.CTscansobtainedat20mA and120mAwithAIDR3DweredefinedasULDCTandLDCT, respec-tively.InadditiontoLDCTandULDCT,imagesat240mAwithAIDR 3DwerealsoobtainedtobeusedfortheSORofthepresenceof pul-monarynodulesinthisstudy.Itisbecausesummedradiationdoses inthethreeCTserieswaslowerthanthestandardradiationdose usedduringsinglechestCTexaminationbeforetheintroduction ofthe320-row CTscannerin anyof6 institutionsthat partici-patedthisstudy,andalsobecausethesummedradiationdosewas smallerthantheguidancelevelforabdominalCTprovidedby Inter-nationalAtomicEnergyAgencybasedontherecommendationsof theInternationalCommissiononRadiologicalProtection[19].
CT dose index volumes (CTDIvol) weredefined by patients’ proportion.Theeffectivedosewasretrospectivelycalculatedby multiplyingthedose-lengthproductvaluesbasedonCTDIvolbya factorof0.017[20].
2.3. Objectivemeasurementinthelungfield
AllquantitativeanalyseswereperformedusingImageJ soft-ware,Version1.43(RasbandW.S.,ImageJ,U.S.NationalInstitute of Health, Bethesda, Maryland, USA, http://rsb.info.nih.gov/ij/, 1997–2008)onapersonalcomputerbyasingleboard-certificated radiologist(Y.N.with13yearsofexperience).Becausethe mea-surements should be done at comparable regions in the lung
Fig.1. Flowchartofstudypopulation.
field,the3CTscanswithAIDR3DandCTscanat20mAwithout AIDR3Dweredisplayedsimultaneouslyinaside-by-sidefashion. Therefore,this observerwasawareofthescanningprotocolfor eachimagedata.Objectiveimagenoise(i.e,standard deviation) wasmeasuredattheleveloflungapics,carina,inferiorpulmonary veinsandlungbases.Thus,1328ROImeasurements(4series×4 levels×83patients)weretotallyperformed(Fig.2).
2.4. Noduledetectionstudy
Five board-certificated radiologists (M.K, T.Y, H.K, T.M. and Y.S., with 16, 11, 11, 10, and 10 years of experience, respec-tively)independently assessedULDCT and LDCTimagesforthe presence/absence of non-calcifiedpulmonary nodulesincluding ground-glass nodules. These observers were instructed that CT imagesincludedcasesbothwithnodules andwithoutand that caseswithmultiplenodules(lessthan10) wereincluded.They wereblindedtothescanningprotocolsandthepatients’clinical informationandwereallowedtoadjustthewindowlevel accord-ingtotheirindividualpreference andtochangetheimagesize. Theseobserverswereaskedtomarkthepulmonarynodulesthat metthethreecriteriaonthemonitor:(1)thelongestdiameter(LD) of3mmormore;(2)anaspectratiooflessthan3;and(3)theratio ofheighttobaseof1ormoreinapleura-basedlesion(Fig.3),by puttingthecursorbesidethedetectednodulesandrecordingthe confidencelevelforitsexistencebyacontinuousratingscale.They werealsoallowedtomeasurethenodularsizeonthemonitor. Priorto thereading experiment, theobservers were instructed
toignoreabnormal findings thatare notin apparently nodular shapes,ifany,suchasconsolidationandbronchiectasis.Toreduce systematicbiasforeachobserver,ULDCTandLDCTimageswere randomly sorted into two reading sessions so that the images for eachcase appeared onlyoncein each session(forexample, iftheLDCTimagesobtainedforacasewereinthefirstsession, thecorrespondingULDCT imagesforthesamecasewereinthe second).Standardofreference(SOR)ofthepulmonarynoduleswas determinedbasedonimagesobtainedat240mAwithAIDR3Dby theconsensusreadingsofanother2board-certificatedradiologists (M.T.andK.M.,with29and34yearsofexperience,respectively) whodidnotparticipateinthedetectionstudy.Thetotalreading timeduringthereadingsessionwasrecordedforeachreader.
To estimate intra-observer variability of the continuously-distributedrating scalesonULDCTimages, ULDCTimagesin20 casesselectedarbitrarilyasthedistributionofnodularsizeand characteristics(solidorgroundglassnodules)issimilartothatin thetotalstudypopulation:23solidnodulesand7groundglass nod-uleswereincluded,3caseshadnonodulesand8caseshadtwoor morenodules,wereevaluatedbyfivereaderstwotimes,separated byanintervalofmorethanayear.Theintra-observervariancewas evaluatedbySpearmancorrelationcoefficientfortheratingscales onidenticalimages.
2.5. Statisticalanalyses
Thelocationofthenoduledetectedbyeachobserverwas com-paredwiththatofSOR.Then,theobserver’sdetectionwasclassified
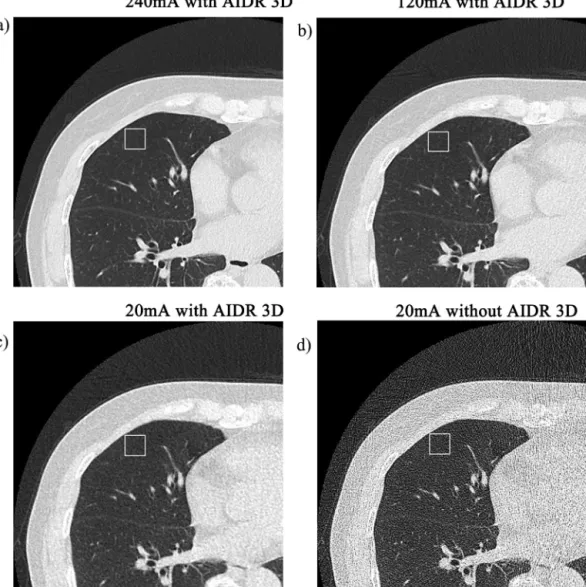
Fig.2. Thisisanexampleofobjectiveimagenoisemeasurementinthelevelofrightinferiorpulmonaryvein(71-year-oldwoman).First,imagedatacorrespondingtothis levelweredeterminedoneachscanseries.Second,15mm-quadrangularregionsofinterest(ROI)(whitesquares)weresetontherightparenchymabasedonanatomical landmarksuchasvesselbifurcations.ROIswerecarefullyplacedbytheobservertoavoidpulmonarybronchiandvessels.MeasuredstandarddeviationsinROIlocatedinthe rightmiddlelobeonCTobtainedat240mAwithAIDR3D(a),LDCT(b),ULDCT(c)andCTobtainedat20mAwithoutAIDR3D(d)were37.6,51.0,61.8and232.3Hounsfield ofUnit,respectively.Inthemeasurementofthisobjectiveimagenoise,parenchymaoftheleftlungwasnotmeasured,becauseofunreliablityinmeasurementassociated withpresumedcardiacmotion.
asatruepositive,iftheclosestdistancebetweenthedetected nod-uleanditsnearestSORnodulewaslessthantheLDoftheSOR nodule,anditwasafalsepositiveifnot.Forconvenience,incasethe markingsrecognizedasfalsepositiveswerelocatedintheidentical pulmonarysub-segmentastheSOR,themarkingswereregarded tobelocatedinadifferentsub-segmentfromthesub-segmentin whichtheSORexisted.
ThenoduledetectionperformancebetweenULDCTandLDCT was compared in total as well as in each subgroup classified according to the LD (>4mm, >6mm and >8mm) and nodular characteristics(solidandnon-solid),usingreceiver-operating char-acteristics(ROC)analysis.Asanindexofobserverperformance, weusedtheareaundertheROCcurve(AUC),whichwas calcu-latedbythetrapezoidalrule.Weperformedtheanalysisofvariance
Table1
Objectiveimagenoise.
AIDR3D FBP
240mA 120mA(LDCT) 20mA(ULDCT) 20mA
Objectiveimagenoise(Hounsfieldofunit)
Lungapics 86.4±18.0 95.8±18.8 88.2±14.4 620.7±209.3*
Carina 55.3±12.7 64.5±13.7 74.2±10.9 313.0±118.5*
Inferiorpulmonaryvein 57.9±14.9 65.2±13.7 75.4±12.8 293.6±113.9*
Lungbase 88.2±25.0 99.0±23.5 99.3±25.3 440.2±145.6*
CTAV:computedtomographyattenuationvalue,AIDR3D:adaptiveiterativedosereductionusingthree-dimensionalprocessing,FBP:filteredbackprojection,LDCT:low dosecomputedtomography,ULDCT:ultralowdosecomputedtomography.
Fig.3. Schemeofthethreecriteriametbyincludedpulmonarynodulesinthe detec-tionstudy:(a)thelongestdiameterofapulmonarynodule,representedasadotted line,is3mmormore;(b)theaspectratio,theratioofthelongestdiameterof pul-monarynodule(A)totheshortestdiameterofthepulmonarynodule(B),islessthan 3;and(c)theheightofapleura-basedpulmonarynoduleisgreaterthanthebaseof thenodule.
(ANOVA)ofpseudovaluesofAUCcomputedbythejackknife anal-ysismethodproposedbyDorfmanetal.[21],whichisdesignated theDorfman–Berbaum–Metzmethod.Sensitivityandpositive pre-dictivevalue(PPV)werecomparedbetweenULDCTandLDCTusing Wilcoxonrankedsigntestonasub-segmentbasis.
Asadditionalanalyseswithrespecttotheinfluenceof body habitusonimagesonULDCT,Spearmanrankcorrelationanalysis were performed to assess the correlations of objective image noisewithbody massindex(BMI),and comparisonsamongthe 4seriesbothinobjectiveimagenoisewereperformedusingone wayfactorial analysisof variance. Whenthis test waspositive,
Turkey–Kramertestforpairwisecomparisonsamongthe4series wasapplied.Sensitivitywerecomparedin2sub-groupsclassified accordingtothethresholdvalueof25inBMIbetweenULDCTand LDCTusingWilcoxonrankedsigntestonasub-segmentbasis.
3. Results
3.1. Radiationdoseassessment
TheCTDIvolsettingsfor240mA,120mAand20mAwere5.7,2.8 and0.5mGy,respectively,in46patientswithsmallerandmedium proportionand5.1,2.6and0.4mGy,respectively,in37patients withlargerproportion.Meandose-lengthproductvaluesfor240, 120and20mAwere207.3,102.1and17.0mGy/cm,respectively. Meaneffectivedosesfor240,120and20mAwere3.524,1,736and 0.289mSv,respectively.
3.2. Objectivemeasurementinthelungfield
Atallmeasuredlevels,objectiveimagenoiseonULDCTwas sig-nificantlyless thanthatonCT scansat20mAwithoutAIDR3D (p<0.05).Inthe3CTscanswithAIDR3D,ahighertubecurrentyield lessobjectiveimagenoiseatthelevelofcarina,inferiorpulmonary veinandlungbase(Table1).
Objective image noise correlated positively with BMI at all measuredlevelsonCTscansat20mAwithoutAIDR.(p<0.05) Coef-ficientcorrelationsincreasedasthedistanceofmeasuredlevelfrom thelungapices.Significantcorrelationswerenotobservedinany CTscanwithAIDR3DexceptforCTscansat240mAwithAIDR3D atbothlevelofcarinaandinferiorpulmonaryveinandLDCTatthe levelofcarina(Table2).
3.3. Noduledetectionstudy
AstheSOR,161solidnodulesand60ground-glassnoduleswere identified,withthenumberofnodulesperpatientrangingfrom1 to9.Theaveragenumberofnodulesperpatientswas3.0.The min-imumandmaximumLDswere3.0and25.5mm,respectively,with ameanLDof6.25mm.ThemeanLDsofsolidnodulesand ground-glassnoduleswere5.71and7.63mm,respectively(Table3).
Thenodule detectionperformance ofLDCTwassignificantly betterthanthatofULDCTforallpulmonarynodules,astheAUC was0.845±0.017inULDCTand0.886±0.024inLDCT(p=0.012), whereas the PPV in ULDCT wasrather similar to that in LDCT (p=0.08).Therewasastatisticallysignificantinter-observer vari-ance in the nodule detection performance among five readers (p<0.001).Thetotalreadingtimeduringthereadingsessionwas 10.2±2.5h(range,7–14h)(Table4).
No statistically significant difference in the nodule detec-tion performance wasdemonstrated for solid nodules between ULDCTandLDCT,irrespectiveofthenodularLD,astheAUCwas 0.844±0.017inULDCTand0.876±0.026inLDCT(p=0.057).The sensitivitywasequivalentbetweenULDCTandLDCTintheentire solidnodules(p=0.08)(Table5).ULDCTdemonstratedcomparable sensitivitytoLDCTforthesolidnodules,inthesubgroupwithBMI of25ormore(p=0.074)aswellasthatwithBMIoflessthan25 (p=0.225)(Table6).
Whenconfinedtotheground-glassnodules,theAUCwasrather similarbetweenULDCT(0.899±0.038)andLDCT(0.941±0.030) fornoduleswithLDvaluesof8mmormore(p=0.144).However, fornoduleswithLD<8mm,ULDCTshowedasignificantlysmaller AUCandlowersensitivitycomparedwithLDCT(Table7).
In terms of intra-observer variance for the continuously-distributed rating scales in 30 pulmonary nodules on ULDCT images,theSpearmancorrelationcoefficientsofthefivereaders were0.641forreader-1(p<0.001),0.762forreader-2(p<0.001),
Table2
Correlationsofobjectiveimagenoisewithbodymassindex.
AIDR3D FBP 240mA 120mA(LDCT) 20mA(ULDCT) 20mA Lungapics 0.162 0.211 0.037 0.409 (NS) (NS) (NS) (p<0.001) Carina 0.266 0.291 0.169 0.458 (p=0.015) (p=0.008) (NS) (p<0.001)
Inferiorpulmonaryvein 0.280 0.202 0.088 0.564
(p=0.010) (NS) (NS) (p<0.001)
Lungbase 0.171 −0.077 −0.142 0.576
(NS) (NS) (NS) (p<0.001)
AIDR3D:adaptiveiterativedosereductionusingthree-dimensionalprocessing,FBP:filteredbackprojection,LDCT:lowdosecomputedtomography,ULDCT:ultralowdose computedtomography,NS:notsignificant.
0.559forreader-3(p=0.001),0.645forreader-4(p<0.001),and
0.652for reader-5 (p<0.001), and these indicated rather small
intra-observervariances.
4. Discussion
In this study, ULDCT (0.289mSv) demonstrated comparable
lung noduledetectionperformance of the161solid nodulesto
LDCT(1.736mSv)irrespectiveoftheLD(Fig.4).Amean
sensitiv-ityofULDCT wasacceptable(70.3%)and60patients(72%)with BMIvaluebetween18.5and25wereclassifiedasstandardbody habitusbythecategorizationcriteriaoftheWorldHealth Organiza-tion.UsingULDCT(0.17mSv),Yamadaetal.hasreportedthatMBIR wassuperiortoFBPinnoduledetection[22].Inanotherprevious study,ULDCTwithMBIR(0.20mSv)hasshowncomparable sensi-tivityfor55solidnodules(≥4mm)(meanvalue:66.5%)toLDCT (0.92mSv)withiterativereconstruction[18].Eveninsmallersolid nodules(<4mm),whicharerecommendedtobefollowedupat12 monthsfromtheinitialCTforhigh-riskpatientsaccordingtothe statementfromtheFleischnerSociety[23],thisstudyrevealedthat ULDCThadadiagnosticperformanceequivalenttoLDCT.The effec-tivedoseofULDCT(0.289mSv)isabout2×thatofastandardPAand LateralchestX-ray[24,25].Consideringthataverageeffectivedose ofNationalLungScreeningTrial(1.4mSv)almostcorrespondedto thatofLDCTinthisstudy(1.736mSv)[26],ULDCTmayrepresent alessinvasivealternativescreeningmodalityforsolidnodulesin caseswithstandardbodyhabitus.Moreover,detectionsensitivity forsolidnodulesinULDCT(meanvalue62.8%)wascomparableto LDCTalsoinoverweightorobesesub-group(BMI≥25).Objective imagenoiseofthelungparenchymadidnotcorrelatewithBMI inULDCT.Therefore,ULDCTmayhavepotentialtobesolid nod-ulescreeningmethodirrespectiveofthebodyhabitus.Toconcrete theseresults,afurtherstudyincludingmoreoverweightorobese casesmayberequired.
HighlevelsofPPV,equivalenttoLDCT,weredemonstratedin ULDCTinthis study,whichisanotheradvantageofULDCT asa screeningtoolforpulmonarynodules.Forallidentifiedpulmonary nodules,PPVin ULDCT (meanvalue 78.7%)tendedtoberather higherthaninLDCTinfourreaders.Thisparadoxicalphenomenon couldbeexplainedbythefollowingreasons.InULDCT,some nod-uleslookedhighlightedincontrasttoobscurednormalperipheral lungstructures,(Fig.5)andsomefaintshadowsfalselyrecognized asnodulesinLDCTwereremovedintheimage-noise differentia-tionprocesswithAIDR3DinULDCT.(Fig.6)Lessorcomparable objectiveimagenoiseshowninthelungapexandbaseinULDCT comparedwithLDCTcouldreflectthisparadoxicalphenomenon. Furthermore,aquantummottledpixelatedappearancereportedin ULDCTimageswithMBIR[27,28]wasnotapparentinULDCTinthis study.Nonetheless,reader3showedamuchlowerPPVinULDCT thantheother4readers,andthetotalreadingtimeofreader3was
thelongest.Actually,manynodule-likeshadowsdetectedbyreader 3weremostlyleftunmarkedbytheother4readers.These nodule-likeshadowsweremisjudgedastruelesionsinULDCTbyblurring branchingstructuressuchasvesselbifurcationswhichcouldbe recognizedcorrectlyinLDCT,however,theirbordersareindistinct evenwithdetailedobservation.Therefore,theycaneasilybe recog-nizedasfalse–positivelesionsbylessfamiliaritywithULDCTimage (Fig.7).
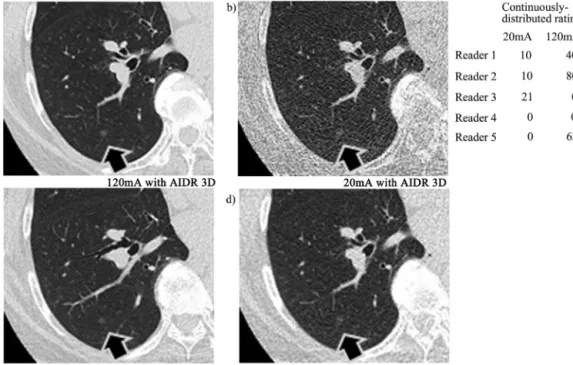
Regardinggroundglassnodules,thelungnoduledetection per-formanceinULDCTwasinferiortothatinLDCTinnoduleswith LDof8mmorless.(Figs.8and9)Onthecontrary,someprevious studiesreportedthatULDCTwithMBIR(0.16–0.2mSv)hadthelung noduledetectionperformanceforgroundglassnodules compara-bletoLDCTwithiterativereconstruction(0.92mSv)orstandard doseCT(11.2mSv)[18,29].However,thedetectionsensitivityfor groundglassnodulesinULDCTwithMBIR(65.5%)[18]was simi-lartothatinthisstudy(68.5%),andthemeansizeofgroundglass nodulesinULDCTwithMBIR(9.24mm)[18]waslargerthanLD ofgroundglassnodulesinthisstudy(7.63mm).Therefore, effec-tivedoseelevationshouldbedesirableforacquiringlungnodule detectionperformanceforrelativelysmallerGGNswitha diam-eter of 5mm or more, which is recommended to be followed accordingtotheguidelineforground-glassnodulemanagement bytheFleischnerSociety[30].Toconcludethisissue,furtherstudy withagreaternumberofground-glassnodulesisrequired;there isanotherresearchprojectbeingconductedintheACTIvestudy groupstoassessthesesubjects.
Table3
Distributionofthenumberoflungnodulesperpatientandsizedistributionoflung nodule.
Distributionofthenumberoflungnodulesperpatient
Thenumberoflungnodulesperpatient Patientnumber
0 10 1 36 2 17 3 11 Morethan4 9 Total 83
Sizedistributionoflungnodules
LD(mm) SN GGN total <4 48 9 57 4–6 74 22 96 6–8 19 10 29 >8 20 19 39 Total 161 60 221
Table4
ComparisonofLNDPbetweenULDCTandLDCTintotallungnodules.
Reader areaunderROCcurve sensitivity(n=221) PPV Readingtime(h)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader1 0.854 0.894 71.95(159) 80.54(178) 81.12 76.72 12 Reader2 0.849 0.904 70.59(156) 81.45(180) 91.18 87.38 9 Reader3 0.853 0.876 74.66(165) 78.73(174) 48.25 49.57 14 Reader4 0.793 0.808 59.72(132) 62.44(138) 83.44 74.33 7 Reader5 0.874 0.947 75.57(167) 90.50(200) 89.30 87.72 9 Significant(p=0.012) Significant(p=0.043) NS(p=0.080)
LNDP:lungnoduledetectionperformance,ULDCT:ultralowdosecomputedtomographyobtainedat20mA,LDCT:lowdosecomputedtomographyobtainedat120mA, ROC:receiveroperatingcharacteristics,PPV:positivepredictivevalue,NS:nosignificant,Numbershowninparenthesesinsensitivitystandsfornodulenumberdetectedby eachof5readers.
Table5
ComparisonofLNDPbetweenULDCTandLDCTinsolidnodules. AreaunderROCcurve
Reader Totalsolidnodules Morethan4mm Morethan6mm
(n=161) (n=113) (n=39)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader1 0.848 0.892 0.913 0.947 0.986 0.956 Reader2 0.855 0.896 0.899 0.913 0.934 0.920 Reader3 0.856 0.864 0.894 0.887 0.960 0.947 Reader4 0.790 0.790 0.813 0.821 0.894 0.880 Reader5 0.872 0.937 0.912 0.949 0.934 0.960 NS(p=0.057) NS(p=0.148) NS(p=0.654) Sensitivity
Reader Totalsolidnodules Morethan4mm Morethan6mm
(n=161) (n=113) (n=39)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader1 69.57(112) 78.88(127) 82.30(93) 90.27(102) 97.44(38) 92.31(36) Reader2 71.43(115) 79.50(128) 80.53(91) 83.19(94) 87.18(34) 84.62(33) Reader3 74.53(120) 75.78(122) 79.65(90) 78.76(89) 92.31(36) 89.74(35) Reader4 60.87(98) 60.25(97) 63.72(72) 65.49(74) 79.49(31) 76.92(30) Reader5 75.16(121) 88.82(143) 83.19(94) 90.27(102) 87.18(34) 92.31(36) NS(p=0.080) NS(p=0.080) NS(p=0.414)
LNDP:lungnoduledetectionperformance,ULDCT:ultralowdosecomputedtomographyobtainedat20mA,LDCT:lowdosecomputedtomographyobtainedat120mA, ROC:receiveroperatingcharacteristics,NS:nosignificant,Numbershowninparenthesesinsensitivitystandsfornodulenumberdetectedbyeachof5readers.
Table6
ComparisonofsensitivitybetweenULDCTandLDCTin2sub-groupsclassifiedaccordingtothethresholdof25inBMI. Bodymassindexoflessthan25
Reader Total(n=168) solidnodule(n=124) ground-glassnodule(n=44)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader-1 73.21(123) 81.55(137) 72.58(90) 79.84(99) 75.00(33) 86.36(38) Reader-2 73.81(124) 79.76(134) 75.80(94) 77.42(96) 68.19(30) 86.36(38) Reader-3 75.60(127) 80.36(135) 74.19(92) 76.61(95) 79.55(35) 90.91(40) Reader-4 61.90(104) 61.31(103) 62.90(78) 57.26(71) 59.09(26) 72.73(32) Reader-5 76.79(129) 91.67(154) 77.42(96) 90.32(112) 75.00(33) 95.46(42) NS(p=0.080) NS(p=0.225) Significant(p=0.043) Bodymassindexof25ormore
Reader Total(n=53) Solidnodule(n=37) Ground-glassnodule(n=16)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader-1 67.92(36) 77.36(41) 59.46(22) 75.68(28) 87.50(14) 81.25(13) Reader-2 60.38(32) 86.80(46) 56.76(21) 86.49(32) 68.75(11) 87.5(14) Reader-3 71.70(38) 73.58(39) 75.68(28) 72.98(27) 62.50(10) 75.00(12) Reader-4 52.83(28) 66.04(35) 54.06(20) 70.27(26) 50.00(8) 56.25(9) Reader-5 71.70(38) 86.79(46) 67.57(25) 83.79(31) 81.25(13) 93.75(15) Significant(p=0.043) NS(p=0.074) NS(p=0.078)
ULDCT:ultralowdosecomputedtomographyobtainedat20mA,LDCT:lowdosecomputedtomographyobtainedat120mA,NS:nosignificant,Numbershowninparentheses standsfornodulenumberdetectedbyeachof5readers.
Table7
ComparisonofLNDPbetweenULDCTandLDCTinGGNs. AreaunderROCcurve
Reader TotalGGNs Morethan6mm Morethan8mm
(n=60) (n=29) (n=19)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader-1 0.868 0.898 0.962 0.979 0.946 0.972 Reader-2 0.834 0.922 0.930 0.999 0.894 0.998 Reader-3 0.845 0.907 0.913 0.965 0.894 0.973 Reader-4 0.799 0.854 0.878 0.895 0.868 0.868 Reader-5 0.882 0.973 0.913 0.999 0.894 0.894 Significant(p=0.001) Significant(p=0.031) NS(p=0.144) Sensitivity
Reader TotalGGNs Morethan6mm Morethan8mm
(n=60) (n=29) (n=19)
ULDCT LDCT ULDCT LDCT ULDCT LDCT
Reader-1 78.33(47) 85.00(51) 93.10(27) 96.55(28) 89.47(17) 94.74(18) Reader-2 68.33(41) 86.67(52) 86.21(25) 100.00(29) 78.95(15) 100.00(19) Reader-3 75.00(45) 86.67(52) 82.76(24) 93.10(27) 78.95(95) 94.74(18) Reader-4 56.67(34) 68.33(41) 75.86(21) 79.31(23) 73.68(14) 73.68(14) Reader-5 76.67(46) 95.00(57) 82.76(24) 100.00(29) 78.95(15) 100.00(19) Significant(p=0.043) Significant(p=0.042) NS(p=0.066)
LNDP:lungnoduledetectionperformance,GGN:ground-glassnodule,ULDCT:ultralowdosecomputedtomographyobtainedat20mA,LDCT:lowdosecomputedtomography obtainedat120mA,ROC:receiveroperatingcharacteristics,NS:nosignificant,numbershowninparenthesesinsensitivitystandsfornodulenumberdetectedbyeachof5 readers.
Thereare several limitations in this study. First, qualitative
imageassessmentfortheimagenoisewasnotanalyzedbecause
thisstudymainlyfocusedontheLNDbyULDCT withAIDR3D.
Second, although this research was conducted as multi-center
trial,thestudypopulationinthisstudywasrelativelysmall,and
furtherstudieswithmorepatientsasdescribedabovearerequired
to enhance these preliminary results. Third, the readers could
recognizetheradiationdosesoftheimagestosomeextentdueto
theimagedatesetsbeinggenerallydifferentinappearanceeven
inablindfashion.Thismaybeapotentialcauseofreadingbias.
Fourth,theresultsobtainedusingonlyaniterativereconstruction
techniquedevelopedbyasinglevendorinthisstudymaynotbe
adaptable to similar iterative reconstruction methods available
fromothermanufacturer.Furtherstudywillbeneededtocompare
the merit of iterative reconstruction technique from multiple
vendorsforfuturelungnodulescreeninginULDCT.Fifth,although
the2radiologistswhodidnotparticipateinthedetectionstudy
usedmeasurement toolcarefullyonthemonitorfor measuring
theLD ofsmallernodules, asnecessary, todeterminetheSOR,
and the automated nodule measurement tool was not used.
Fig.4.Trans-axialimagesattherightlowerlobeina68-year-oldwomanwithabodymassindexof30.8.Asmallersolidnodulewiththelongestdiameterof4.0mm identifiedintherightlowerlobe(blackarrow)inCTobtainedat240mAwithAIDR3D(a)isapparentlyrecognizedinULDCT(d)aswellasinLDCT(c),ascontinuously distributedratingsinULDCTweresimilartothoseinLDCTinall5observers.ThissmallersolidnodulecanbesimilarlydetectedinCTobtainedat20mAwithoutAIDR3D(b).
Fig.5. Trans-axialimagesattherightlowerlobeina71-year-oldwomanwithabodymassindexof21.9.Asmallerground-glassnodulewiththelongestdiameterof 4.2mmidentifiedintherightlowerlobe(blackarrow)inCTobtainedat240mAwithAIDR3D(a)appearsratherhighlighted,mainlythankstovaguenormalperipheral lungstructuressuchassmallervessels,inULDCT(d).ContinuouslydistributedratingsinULDCTwerehigherthanthoseinLDCT(c)in3observers.InCTobtainedat20mA withoutAIDR3D(b),imagenoiseisprominentinsomeregionscomparedwithULDCT.
Therefore, the LD measuredin this study might be sometimes
inaccurate.However,suchmeasuringerrorispresumedtobetoo
smallto affectthe comparabilityin ULDCT to LDCTasto solid
nodule detection. Moreover, as a relevant issue, the influence
oftheuseof lowdoseanditerativereconstructionmethods on
the automated-measured nodule volume was not analyzed in
thisstudyandhastobeassessedasanotherstudyinthefuture.
Sixth, we did not evaluate LND by using maximum intensity
projection(MIP)thickslabimages,whichcanbeusefulespecially
forpulmonarysolidnoduleinULCT.TheusefulnessofMIPimages
for theimprovement of LND hastobe examinedin thefuture
study.
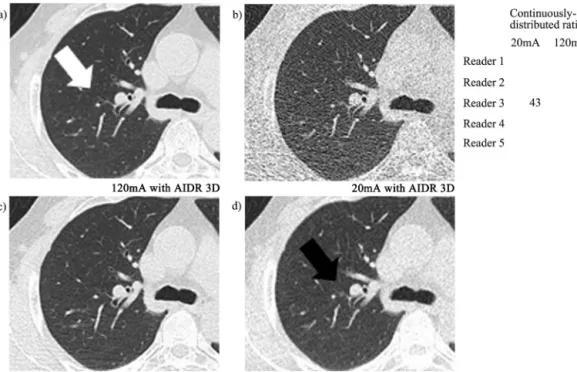
Fig.6. Trans-axialimagesattherightupperlobeinan80-year-oldmanwithabodymassindexof19.8.Faintground-glassnodularshadowseemstoexistinLDCT(black arrow)andwasmarkedbytworeaders(c).InCTobtainedat240mAwithAIDR3D(a),obviousvesselstructurecanbedetectedsuperimposedonanill-definedslight attenuatedarea(whitearrow).InULDCT(d),thisslightattenuatedareaisindistinctandundifferentiatedwiththecircumferentiallungfield(grayarrow).Thisfalse–positive lesionisalsonotapparentinCTobtainedat20mAwithoutAIDR3Dbygettingunifiedwithpatchy-distributedimagenoise(b).
Fig.7. Trans-axialimagesattherightupperlobeinan83-year-oldmanwithabodymassindexof22.0.Anill-definednodule-likeshadowseemstoexistinULDCT(black arrow)andwasmarkedbyareader(d).Thisnodule-likeshadowisnotapparentinCTobtainedat240mAwithAIDR3D(a)aswellasinLDCT(c),andthelocationofthe nodule-likeshadowinULDCTcorrespondstoperipheralpulmonaryvesselbifurcationinthese2images(whitearrow).Thisfalse–positivelesionisalsonotapparentinCT obtainedat20mAwithoutAIDR3Dbygettingunifiedwithpatchy-distributedimagenoise(b).
Inconclusion,thisstudydemonstratedthatULDCTusingAIDR
3Dwitharadiationdoseequivalenttothatofconventionalchest
X-raycouldhavecomparableLNDtoLDCTwithAIDR3D,except
insmallernon-solidnodules,indicatingthatULDCTwithAIDR3D
haspotentialforuseinlungsolidnodulescreeningforcaseswith
normalrangebodyhabitus.
Roleofthefundingsource
ThisstudywasconductedaspartoftheArea-detector
Com-puted Tomography for the Investigation of Thoracic Diseases
(ACTIve)study,anongoingmulti-centerresearchprojectinJapan.
Each of the eight institutions: Ohara General Hospital, Osaka
Fig.8.Trans-axialimagesattherightupperlobeina57-year-oldwomanwithabodymassindexof23.4.Asmallerground-glassnodulewiththelongestdiameterof4.0mm identifiedintherightupperlobe(blackarrow)inCTobtainedat240mAwithAIDR3D(a)isindistinctinCTobtainedat20mAwithoutAIDR3D(b)byreducedsignal-to-noise ratio,presumablyduetoradiationdosedeficiency.AIDR3Dimprovesthisdisadvantage,andthissmallernon-solidnodulewaseasilydetectedinULDCT(d)aswellasin LDCT(c),ascontinuouslydistributedratingsinULDCTweresimilartothoseinLDCTinall5observers.
Fig.9.Trans-axialimagesattherightlowerlobeina62-year-oldmanwithabodymassindexof29.1.Asmallersolidnodulewiththelongestdiameterof5.0mmidentified intherightlowerlobe(blackarrow)inCTobtainedat240mAwithAIDR3D(a)wasmoredifficulttodetectinULDCT(d)thaninLDCT(c).Continuouslydistributedratingsin ULDCTwerelowerthanthoseinLDCTin3observers.Thissmallernon-solidnoduleinULDCTwithoutAIDR3DismoreobscurethaninCTobtainedat20mAwithoutAIDR 3D(b).
MedicalCollege,OsakaUniversity,KobeUniversity,TenriHospital,
Okayama University, University of the Ryukyusand Shiga
Uni-versityofMedicalSciencereceivesaresearchgrantfromToshiba
MedicalSystems.However,thefunderhadnoroleinstudydesign,
datacollectionandanalysis,decisiontopublish,orpreparationof
themanuscript.Anyothercompetinginterests,suchas
employ-ment,consultancy,patents,productsindevelopment,ormarketed
products,donotexistregardingthismanuscript.
TheACTIvestudygroup
The ACTIve study group currently consists of the following
institutions:OharaGeneralHospital,Fukushima,Fukushima,Japan
(HiroshiMoriya,M.D., PhD., Kotaro Sakuma M.D.); Osaka
Med-ical College, Takatsuki, Osaka, Japan (Mitsuhiro Koyama, M.D.,
PhD.);OsakaUniversity,Suita,Osaka,Japan(OsamuHonda,M.D.,
PhD., Noriyuki Tomiyama, M.D., PhD.); Kobe University, Kobe,
Hyogo, Japan (Hisanobu Koyama, M.D., PhD., Yoshiharu Ohno,
M.D.,PhD., KazuroSugimura, M.D.);TenriHospital,Tenri,Nara,
Japan(RyoSakamoto,M.D.,Yuko NishimotoM.D.,PhD., Satoshi
Noma,M.D.,PhD.);OkayamaUniversity,Okayama,Okayama,Japan
(Katsuya Kato, M.D., PhD.); University of the Ryukyus,
Nishi-hara,Okinawa,Japan(TetsuhiroMiyara,M.D.,TsuneoYamashiro,
M.D., Hisashi Kamiya, M.D., Ayano Kamiya,M.D., Yuko Tanaka,
M.S.,SadayukiMurayama,M.D.,PhD.);ShigaUniversityof
Medi-calScience,Otsu,Shiga,Japan(YukihiroNagatani,M.D.,Norihisa
Nitta,M.D.PhD.,MasashiTakahashi,M.D.,KiyoshiMurata,M.D.,
PhD.).
Acknowledgement
The authors acknowledge the great assistance of Mr
Shin-suke Tsukagoshi and Mr Hiroyasu Inokawa (Toshiba Medical
SystemsCorporation) fortheirtechnicalsupportand important
suggestions.
References
[1]The National Lung Screening Trial Research Team. Reduced lung-cancer mortalitywith low-dosecomputed tomography screening.NEngl JMed 2011;365:395–409.
[2]WenderR,FonthamET,BarreraJrE,etal.AmericanCancerSocietylungcancer screeningguidelines.CACancerJClin2013;62(2):107–17.
[3]BrennerDJ.Radiationriskspotentiallyassociatedwithlow-doseCTscreening ofadultsmokersforlungcancer.Radiology2004;231:440–5.
[4]BachPB,MirkinJN,OliverTK,etal.BenefitsandharmsofCTscreeningforlung cancer.Asystematicreview.JAMA2012;307:2418–29.
[5]Hsieh J. Computed tomography: principles, design, artifacts, and recent advances.1sted.Bellingham,Washington:SPIEPress;2003.
[6]Prakash P, Kalra MK, Digumarthy SR, et al. Radiation dose reduction withchestcomputedtomographyusingadaptivestatisticaliterative recon-structiontechnique: initialexperience.J ComputAssistTomogr2010;34: 40–5.
[7]XuJ,MaheshM,TsuiBM.IsiterativereconstructionreadyforMDCT?JAmColl Radiol2009;6:274–6.
[8]PontanaF,PagniezJ,DuhamelA,etal.Reduced-doselow-voltagechestCT angiographywithsinogram-affirmediterativereconstructionversus standard-dosefilteredbackprojection.Radiology2013;267(2):609–18.
[9]WilleminkMJ,deJongPA,LeinerT,deHeerLM,NievelsteinRA,etal. Iter-ativereconstructiontechniquesforcomputedtomography.Part1:Technical principles.EurRadiol2013;23:1623–31.
[10]SinghS,KalraMK,GilmanMD,etal.Adaptivestatisticaliterativereconstruction techniqueforradiationdosereductioninchestCT:apilotstudy.Radiology 2011;259(2):565–73.
[11]Vardhanabhuti V, Loader RJ, Mitchell GR, Riordan RD, Roobottom CA. Imagequality assessment ofstandard- and low-dose chest CTusing fil-teredbackprojection,adaptivestatisticaliterativereconstruction,andnovel model-basediterativereconstructionalgorithms.AmJRoentgenol2013;200: 545–52.
[12]PontanaF,PagniezJ,FlohrT,etal.Chestcomputedtomographyusingiterative reconstructionvsfilteredbackprojection.Part1.Evaluationofimagenoise reductionin32patients.EurRadiol2011;21:627–35.
[13]PontanaF,DuhamelA,PagniezJ,etal.Chestcomputedtomographyusing itera-tivereconstructionvsfilteredbackprojection.Part2.Imagequalityoflow-dose CTexaminationin80patients.EurRadiol2011;21:636–43.
[14]YangZ, Zamyatin AA, Akino N. Effective data-domain noise and streak reductionfor X-ray CT.In:KachlriessM,Rafecas M,editors. 11th Inter-national meeting on fully three-dimensional image reconstruction in radiologyandnuclearmedicine.2011(Fully3DWebsite)www.fully3rd.org/ 2011/Fully3D2011Proceedings.pdf(accessedJune4,2012).
[15]FunabashiN,IrieR,AibaM,MorimotoR,KabashimaT,etal. Adaptive-iterative-dose-reduction 3D with multisector-reconstruction method in 320-slice CTmaymaintainaccurate-measurementoftheAgatston-calcium-scoreof
severe-calcificationevenathigherpulsating-beatsandlowtube-currentin vitro.IntJCardiol2013;168:601–3.
[16]JuriH,MatsukiM,ItouY,InadaY,NakaiG,etal.Initialexperiencewithadaptive iterativedosereduction3Dtoreduceradiationdoseincomputedtomographic urography.JComputAssistTomogr2013;37:52–7.
[17]YamashiroT,MiyaraT,HondaO,etal.Adaptiveiterativedosereductionusing threedimensionalprocessing(AIDR3D)improveschestCTimagequalityand reducesradiationexposure.PLoSONE2014;9(8):e105735(Aug25). [18]KatsuraM,MatsudaI,AkahaneM,etal.Model-basediterative
reconstruc-tiontechniqueforultralow-dosechestCT:comparisonofpulmonarynodule detectabilitywiththeadaptivestatisticaliterativereconstructiontechnique. InvestRadiol2013;48:206212.
[19]IAEA.Internationalbasicsafetystandardsforprotectionagainstionizing radi-ationsandforthesafetyofradiationsources.In:IAEAsafetyseries,no.115-I. Vienna:IAEA;1994.
[20]ShrimptonPC,HillierMC,LewisMA,DunnM.NationalsurveyofdosesfromCT intheUK:2003.BrJRadiol2006;79(948):968–80.
[21]DorfmanDD,BerbaumKS,MetzCE.Receiveroperatingcharacteristicrating analysis:generalizationtothepopulationofreadersandpatientswiththe jackknifemethod.InvestRadiol1992;27:723–31.
[22]YamadaY,JinzakiM,TanamiY,etal.Model-basediterativereconstruction techniqueforultralow-dosecomputedtomographyofthelung:apilotstudy. InvestRadiol2012;47:482–9.
[23]MacMahonH,AustinJH,GamsuG,etal.Guidelinesformanagementofsmall pulmonarynodulesdetectedonCTscans:astatementfromtheFleishner Soci-ety.Radiology2005;237:395–400.
[24]ServomaaA,TapiovaaraM.OrgandosecalculationinmedicalXray examina-tionsbytheprogramPCXMC.RadiatProtDosimetry1998;80:213–9. [25]ICRP.The2007recommendationsoftheInternationalCommissionon
Radio-logicalProtection.ICRPpublication103.AnnICRP2007;37:1–332.
[26]LarkeFJ,KrugerRL,CagnonCH,etal.Estimatedradiationdoseassociatedwith low-dosechestCTofaverage-sizeparticipantsintheNationalLungScreening Trial.AJRAmJRoentgenol2011;197:1165–9.
[27]SinghS,KalraMK,HsiehJ,etal.AbdominalCT:comparisonofadaptive statis-ticaliterativeandfilteredbackprojectionreconstructiontechnique.Radiology 2010;257:373–83.
[28]PrakashP,KalraMK,KambadakoneAK,etal.ReducingabdominalCTradiation dosewithadaptivestatisticaliterativereconstructiontechnique.InvestRadiol 2010;45:202–10.
[29]Neroladaki A,BotsikasD, BoudabbousS,etal. Computedtomographyof thechestwithmodel-basediterativereconstructionusingaradiation expo-suresimilartochestX-rayexamination:preliminaryobservations.EurRadiol 2013;23:360–6.
[30]NaidichDP,BankierAA,MacMahonH,etal.Recommendationsforthe man-agementofsubsolidpulmonarynodulesdetectedatCT:astatementfromthe FleischnerSociety.Radiology2013;266:304–17.