Comparative Study between
the Role of Medial LCP and
Anterolateral LCP in the
Management of Fractures of
Distal Tibia
INTRODUCTION
As the civilisation proceeds towards industrialisation more and more acci-dents have been experienced. In almost all over the world, the incidence of road traffic and industrial accidents are growing up, resulting in fracture of various bones of body. Leg bones fracture are most common among them because it is the most distal part of the body and actively involves in loco-motive system. Out of all the leg bones fracture, a significant number of cases are of distal tibia which are generally comminuted in nature and are unstable. As these fractures occur in proximity of the weight bearing surface of ankle joint, a slight maladjustment in inclination of ankle joint may lead to permanent disability.
Vinod Nair, Satish Uchale,
Prafulla Govind Herode, Aabhijeet Shroff, Krishan Yadav*
Department of Orthopaedics, Dr. D.Y. Patil Medical College, Pimpri, Pune, Maharashtra
Address reprint requests to *Dr. Krishan Yadav, Department of Orthopaedics, Dr. D.Y. Patil Medical College, Pimpri, Pune, Maharashtra, India Article citation: Nair V, Uchale S, Herode
PG, Shroff A, Yadav K. Comparative study between the role of medial LCP and anterolateral LCP in the management of fractures of distal tibia. J Pharm Biomed Sci2016;06(02):115–120. Available at www.jpbms.info Statement of originality of work: The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and that each author believes that the manuscript represents honest and original work.
Sources of funding: None.
Competing interest / Conflict of interest:
The author(s) have no competing interests for financial support, publication of this research, patents, and royalties through this collaborative research. All authors were equally involved in discussed research work. There is no financial conflict with the subject matter discussed in the manuscript.
Disclaimer: Any views expressed in this paper are those of the authors and do not reflect the official policy or position of the Department of Defense.
NLM Title J Pharm Biomed Sci CODEN JPBSCT
2230-7885 ISSN No
ABSTRACT
Background As the civilisation proceeds towards industrialisation more and more accidents have been experienced. In almost all over the world, the incidence of road traffic and industrial accidents are growing up, resulting in fracture of various bones of body. Leg bones fracture are very common because it is the most distal part of the body and is actively involved in locomotive system. Out of all the leg bones fracture, a signif-icant number of cases are of distal tibia which are generally comminuted in nature and are unstable. As these fractures occur in proximity of weight bearing surface of ankle joint, a slight maladjustment in inclination of ankle joint may lead to permanent disability. Besides closed reduction with casting many osteosynthesis techniques can be used for these fracture such open reduction and internal fixation with locking plate, external fixa-tion with or without limited internal fixafixa-tion, intra-medullary nailing. Two types of LCP can be used in the management of fractures of distal one third of tibia i.e. medial LCP and the newer anterolateral LCP.
Aims and Objectives To study the management of fractures of distal tibia using medial LCP and anterolateral LCP and to assess and compare the end results of above proce-dure in terms of benefits and complications.
Materials and Methods This is a prospective randomised study from December 2013 to December 2015 for management of distal tibia fractures treated by medial LCP and Anterolateral LCP.
Results Study was performed on 50 patients out of which 25 were treated by medial LCP and 25 by anterolateral LCP. In study it was seen that medial and anterolateral plating duration of surgery, time of appearance of callus, and time for full weight bear-ing of patient were almost same but infection rate and hardware problem was lower in anterolateral plating.
Conclusion The objective is to obtain anatomic realignment of the joint surface while providing enough stability to allow early motion. This should be accomplished using techniques that minimise osseous and soft tissue devascularisation in the hopes of decreasing the complications resulting from treatment.
KEYWORDS distal tibia fractures, internal fixation, open reduction, Laughansen, mortise view, anatomical reduction
Traditionally, a variety of methods of management have been described with a reportedly high rate of asso-ciated complications1–7.
Many osteosynthesis techniques can be used for these fracture such as open reduction and internal fixa-tion with locking plate, external fixafixa-tion with or with-out limited internal fixation and intra-medullary nailing. All these techniques have their pros and cons, also, there is no consensus concerning the management of these fractures.
Open reduction and internal fixation: To obtain maximal mechanical stability in order to achieve pri-mary (endosteal) bone healing, exact anatomical reduc-tion and strict rigid fixareduc-tion were emphasised in the beginning. This however can rarely be obtained without significant dissection of the fracture and the surround-ing soft tissues. Well-known complications like infec-tion and delayed or non-union are frequently attributed to the devitalisation of bony fragments and additional damage to the soft tissues.
In order to improve fracture healing, more “biologi-cal” methods have been developed over the last decades, trying to lessen the surgical dissection, preserving the blood supply to the bony fragments and containing at least partially the fracture hematoma.
The emphasis now lies on indirect reduction, axial alignment and stable fixation without disturbing the fracture environment and thus preserving most of the vascularisation and fracture haematoma, containing all necessary growth factors for bony healing. There has been an increasing trend towards the use of the lock-ing compression plate (LCP) for fracture fixation. The device allows the screws to lock to the plate, therefore creating a stable, fixed angle device. Precise anatomical contour of this plate is no longer necessary because the plate does not need to be pressed on the bone to achieve stability, thus preventing the loss of primary reduction of fracture fragments caused by inadequate contouring of the plate.
Two types of LCP can be used in the management of fractures of distal one third of tibia i.e. medial LCP and the newer anterolateral LCP3,8,9.
Limited literature exists, comparing methods of treatment of distal tibia fractures. Locking and compres-sion plates are well accepted and effective methods, but are historically related to some complications such as infections, wound complications and implant promi-nence particularly with medial plating.
MATERIALS AND METHODS
The present study was conducted on 50 cases of ankle fracture treated by open reduction and internal fixation by medial LCP and anterolateral LCP in adults (≥21 years). Study was conducted in the Department of Orthopedics, in a tertiary care teaching hospital from December 2013 to December 2015. The maximum follow up was for 24 months and minimum was 2 months with average
follow up of 10 months. All the patients were treated as indoor patients. A written informed consent was obtained before surgery. All the patients were selected on the basis of patients having distal tibia fracture without distal neurovascular injury. Patients having foot injury in same limb and proximal tibia fracture were excluded from our study.
Initial management and resuscitation
After receiving patients in emergency, their vital parame-ters were checked. Thorough examination of the patient was done to rule out any associated chest, abdomen and head injury. A good quality of X-ray both AP and LAT view were taken. After establishment of an intravenous line, fluid replacement was done according to patient’s vital parameters and in case of open fracture bleeding was controlled by pressure bandage and G.T. slab was applied. A tetanus prophylaxis (in case of open injury) and intravenous antibiotic and analgesic were given. Once patient was settled from acute injury then we decide to go for definitive fracture management. This study involved total 50 patients. Open injuries were clas-sified by the Gustilo and Anderson method and closed injuries via the Tscherne classification. Wounds associ-ated with open fractures were managed initially by stan-dard debridement and irrigation.
Injured limb was immobilised with posterior below knee plaster slab. Once the patient was stabilised and all associated injury managed, patient was sent for radio-logical examination. Roentgenogram of injured limb [tibia-fibula with ankle anterio-posterior (AP), lateral and mortice views] were taken. Roentgenogram of knee was also taken to rule out other associated injury like fracture of upper third fibula. Fractures were then classified using Ruedi and Allgower system. If required, computerised tomography (CT) scan was taken for intra-articular extension.
Operative procedure
Open reduction and internal fixation to achieve anatom-ical reduction and strict rigid fixation with medial LCP and anterolateral LCP was done. (Figs. 1–8).
RESULTS
The present study was aimed at assessing the outcomes of fracture of distal tibia treated by either medial LCP or with anterolateral LCP.
The study was performed in a total of 50 patients. Of these, 25 patients were allotted in each group i.e. Group A and Group B.
GROUP A is designated for patients those are oper-ated with distal tibia Medial LCP.
GROUP B is designated for patients those are oper-ated with distal tibia Anterolateral LCP.
Fig. 1 Incision for medial LCP plating. Fig. 2 Open reduction and internal fixation with medial LCP.
Fig. 3 Medial LCP plating by MIPO technique. Fig. 4 X-ray view of medial LCP.
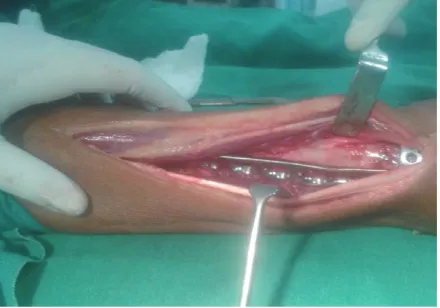
Fig. 5 Incision for anterolateral LCP plating. Fig. 6 Open reduction and internal fixation with anterolateral LCP.
In this study in group A 76% male patients and 24% female patients and in group B 84% males and 16% females participated (Table 1).
Most of the patients, 80% in group A and 84% in group B in our study were between 18 and 60 years, probably because this age group is involved in outdoor activities. Mean age for Group A was 44 years and for Group B was 43.08 years (Table 2).
Maximum cases were caused by road traffic accidents indicating this fracture is high velocity type trauma associated with significant soft tissue injury. Other causative factors were fall on ground and slip from vehicle (Tables 3, 4).
Table 1 Gender incidence.
Gender
Group A Group B No. of
cases % No. of cases %
Male 19 76% 21 84%
Female 6 24% 4 16%
Total 25 100% 25 100%
Fig. 8 Anterolateral LCP plating with MIPO technique.
Fig. 7 X-ray view of anterolateral LCP.
Table 2 Age incidence.
Age in years
Group A Group B No. of
cases % No. of cases %
18–40 12 48% 11 44%
41–60 8 32% 10 40%
Above 60 5 20% 4 16%
25 100% 25 100%
Table 3 Mode of injury.
Mode of injury
Group A Group B No. of
cases % No. of cases %
RTA 16 64% 18 72%
Fall 9 36% 7 28%
Total 25 100% 25 100%
Table 4 Nature of fracture.
Nature
Group A Group B No. of
patients % patientsNo. of %
Close fractures 19 76% 17 68%
Open fractures 6 24% 8 32%
Total 25 100% 25 100%
Table 5 Duration between injury and surgery.
Duration in days
Group A Group B No. of
patients % patientsNo. of %
<5 4 16% 3 12%
5–10 16 64% 18 72%
>10 5 20% 4 16%
Total 25 100% 25 100%
according to Gustilo Anderson classification. Open injuries involved in our study were grade type I only (Table 4).
In our study, most of the patients i. e. 64% in group A and 72% in group B were operated between 5 and 10 days after the injury allowing some time for swelling to subside (Table 5).
Most of the patients i. e. 76% in Group A and 72% in Group B were operated by MIPPO compared to only 24% in Group A and 28% in Group B for open reduction and internal fixation (Table 6).
On taking X-rays during follow up of included patients starting of radiological union was observed carefully by looking for bridging callus, haziness of fracture line (Table 7). Appearance of callus took average time of around 12 weeks in both groups.
Table 8 Time taken for full weight bearing.
Time taken for full wt bearing
Group A Group B No. of
patients % patientsNo. of %
10–15 weeks 6 24% 8 32%
16–20 weeks 16 64% 16 64%
21–25 weeks 3 12% 1 4%
Total 25 25
Average mean time
17.6 weeks
16.9 weeks
P value - 0. 526.
Table 9 Superficial skin infection.
Superficial skin infection patients No. of %
Medial LCP group 6 24%
Anterolateral LCP group 1 4%
P value - 0.042.
Table 10 Symptomatic hardware.
Symptomatic hardware No. of patients %
Medial LCP group 10 40%
Anterolateral LCP group 1 4%
P value - 0.002.
Table 6 Technique used for surgery.
Technique used for surgery
Group A Group B No. of
patients % patientsNo. of % Open
reduction 6 24% 7 28%
MIPPO 19 76% 18 72%
Total 25 100% 25 100%
Table 7 Time taken for appearance of callus on X rays.
Time
Group A Group B No. of
patients % patientsNo. of % Less than
10 weeks 5 20% 6 24%
11–15
weeks 17 68% 18 72%
16–20
weeks 3 12% 1 4%
Total 25 100% 25 100%
Average mean time
12.4 weeks
11.6 weeks
P value - 0.801.
By the process of weight bearing we believed that it would promote secondary bone healing.
Complications
Intraoperative complications: There were no cases with intraoperative complications in both the groups.
Postoperative complications: The postoperative com pli cations are listed below.
Superficial skin infection was more common in medial plating group accounting for 24% infection
rate. It was only 4% in anterolateral plating group (Table 9).
Symptomatic hardware was much more common in Medial LCP group i. e. 40% cases as compared to antero-lateral LCP group i. e. only 4% cases (Table 10).
Ankle stiffness: Only two patients in medial LCP group and one patient in anterolateral LCP group had ankle stiffness. It was probably due to the incompliance of the patient to the advised physiotherapy regimen. Ankle stiffness ranged from restriction of ankle move-ment by 20–40 degrees. P value by statistical calculation was 0.552 which is not significant.
DISCUSSION
Distal tibia fractures can be treated surgically by both medial LCP and anterolateral LCP depending on the type of fracture and the surgeon’s opinion. The question of whether which surgery should be used for distal tibia fractures remains controversial. The goal of operative treatment is to obtain anatomic realignment of the joint surface while providing enough stability to allow early motion. This should be accomplished using techniques that minimize osseous and soft tissue devascularisation in the hopes of decreasing the complications resulting from treatment.
Small clinical outcome studies have been conducted and operative techniques are well described, but the biomechanical consequences of these distinct plate applications are not well understood3,9–12.
Both of these techniues have their pros and cons so it is entirely the surgeon’s decision regarding which tech-nique to use.
SUMMARY AND CONCLUSION
reduction/MIPPO technique and half were treated with anterolateral locking and compression plate using open reduction/MIPPO technique.
• All patients achieved union at the end of study. The mean time for fracture union was 25.4 weeks with medial plating group and 24.04 weeks with anterolateral plating group.
• The average time for appearance of callus formation on X-ray was comparable in both the groups. In medial plating group callus appeared at an average of 12.4 weeks and in anterolateral plating group, callus appeared at 11.6 weeks.
• The average time for full weight bearing was com-parable in both the groups. In medial plating group it was 17.6 weeks and anterolateral plating group, average time for full weight bearing was 16.9 weeks.
• Out of 25 patients in medial plating group, 6 patients showed superficial skin infection, 10 patients complained of hardware prominence and pain at medial malleolus, 6 patients had skin necrosis with subsequent exposure of implant and 2 patients had ankle stiffness.
• Out of 25 patients with anterolateral plating group, one patient had superficial skin infection, one had complains of hardware prominence, one had skin necrosis with implant exposure and one had ankle stiffness.
• None of the patients in both the groups had non union.
• Out of 25 patients in medial plating group, 10 patients had excellent OMAS score and 15 had good OMAS score at final follow up. Out of 25 patients in anterolateral plating group, 12 patients had excel-lent OMAS score and 13 patients had Good OMAS score. The average OMAS score for Group A was 86 and for Group B, it was 87.8.
• By the analysis of the data collected in our study, we conclude that most of the cases of distal tibia fractures can be treated by either medial locking and compression plate or anterolateral locking and compression plate. Both had similar outcome in terms of fracture union, time for weight bearing, and functional outcome. However anterolateral locking and compression plate is associated with much lower complication rates.
• Due to the small numbers of patients involved in our study, we cannot draw any definitive con-clusions from our preliminary results but view them as a valuable basis for future studies. With larger number of patients and with longer follow up, it seems that treatment of distal tibia fractures with anterolateral locking and compression plates having much lower complication rates would prove to be a feasible and worthwhile method of stabilisation.
REFERENCES
1. Bone L, Stegemann P, McNamara K, Seibel R. External fixation of severely comminuted and open tibial pilon fractures. Clin Orthop Relat Res. 1993;292:101–7.
2. McFerran MA, Smith SW, Boulas HJ, Schwartz HS. Complications encountered in the treatment of pilon fractures. J Orthop Trauma. 1992;6(2):195–200.
3. Oh CW, Kyung HS, Park IH, Kim PT, Ihn JC. Distal tibia metaphy seal fractures treated by percutaneous plate osteosynthesis. Clin Orthop Relat Res. 2003;408:286–91.
4. Teeny SM, Wiss DA. Open reduction and internal fixation of tibial plafond fractures: variables contributing to poor results and complications. Clin Orthop Relat Res. 1993;292:108–17. 5. Thordarson DB. Complications after treatment of tibial pilon
fractures: prevention and management strategies. J Am Acad Orthop Surg. 2000;8(4):253–65.
6. Watson JT, Moed BR, Karges DE, Cramer KE. Pilon fractures: treatment protocol based on severity of soft tissue injury. Clin Orthop Relat Res. 2000;375:78–90.
7. Wolinsky P, Lee M. The distal approach for anterolateral plate fixation of the tibia: an anatomic study. J Orthop Trauma. 2008;22(6):404–7.
8. Collinge C, Sanders R, DiPasquale T. Treatment of complex tibial periarticular fractures using percutaneous techniques. Clin Orthop Relat Res. 2000;375:69–77.
9. Helfet DL, Shonnard PY, Levine D, Borrelli J Jr. Minimally inva sive plate osteosynthesis of distal fractures of the tibia. Injury. 1997;28(Suppl 1):A42–A47.
10. Redfern DJ, Syed SU, Davies SJ. Fractures of the distal tibia: min imally invasive plate osteosynthesis. Injury. 2004;35(6):615–20. 11. Shon OJ, Park CH. Minimally invasive plate osteosynthesis of
distal tibial fractures: a comparison of medial and lateral plating. J Orthop Sci. 2012;17(5):562–6.