Weight in Overweight Adolescents
WHAT’S KNOWN ON THIS SUBJECT: The prevalence of
overweight and obesity in adolescents has risen in recent years. Previous measures of weight misperception have ranged from 20% to 40% in overweight patients. Some studies have revealed positive and negative effects of overweight perception.
WHAT THIS STUDY ADDS: We provide recent, nationally representative information on the prevalence of weight
misperception in overweight adolescents in the United States and its relationship to demographic characteristics and weight-related behaviors, assisting clinicians in their individualized counseling efforts with overweight and obese patients.
abstract
OBJECTIVE:The goal of this study was to examine weight misperception among overweight adolescents in recent years and compare the demo-graphic characteristics and weight-related behaviors of overweight ado-lescents who accurately and inaccurately perceive their weight status.
METHODS:We used data from the nationally representative Youth Risk Behavior Surveillance System, collected every 2 years from 1999 through 2007. On the basis of self-reported height and weight, BMI percentile for age and sex was calculated. Overweight and obese respondents (BMIⱖ 85th percentile) were classified into 2 groups: (1) misperceivers (weight perception “about right” or “underweight”) or (2) accurate perceivers (weight perception “overweight”). We examined the proportion of misper-ceivers at each time point. Using the 2007 data, we compared demographic characteristics and weight-related behaviors of accurate perceivers and misperceivers with bivariate and multivariate analyses.
RESULTS:Among overweight adolescents, the overall proportion of mis-perceivers ranged between 29% and 33% from 1999 through 2007. In 2007, 23% of overweight girls and 40% of overweight boys were misperceivers (P
⬍ .001). Both male and female accurate perceivers were significantly more likely than misperceivers to report trying to maintain or lose weight, exercising for weight control, and eating less for weight control. Adjusting for age, race/ethnicity, and BMI percentile, no significant differences in unhealthy weight-related behaviors were found between accurate perceiv-ers and misperceivperceiv-ers in boys or girls. Male accurate perceivperceiv-ers were significantly less likely to report achieving recommended levels of fruit and vegetable intake and physical activity.
CONCLUSIONS:Nearly 3 in 10 overweight adolescents do not consider themselves overweight. Those with an accurate weight perception re-ported some healthy weight-related behaviors but not higher levels of unhealthy weight-related behaviors. With the substantial prevalence of weight misperception, clinicians should consider their patients’ perceived weight status when pursuing patient-centered counseling of overweight adolescents.Pediatrics2010;125:e452–e458
AUTHORS:Nicholas Murphy Edwards, MD,aSandra
Pettingell, PhD,band Iris Wagman Borowsky, MD, PhDa
aDivision of General Pediatrics, Department of Pediatrics, and bCenter for Adolescent Nursing, School of Nursing, University of
Minnesota, Minneapolis, Minnesota
KEY WORDS
adolescent, BMI, obesity, perception, self-assessment
ABBREVIATIONS
CDC—Centers for Disease Control and Prevention YRBS—Youth Risk Behavior Survey
FV—fruit and vegetable PA—physical activity OR— odds ratio CI— confidence interval
The views in this article are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
www.pediatrics.org/cgi/doi/10.1542/peds.2009-0185
doi:10.1542/peds.2009-0185
Accepted for publication Sep 2, 2009
Address correspondence to Nicholas Murphy Edwards, MD, University of Minnesota, Department of Pediatrics, Division of General Pediatrics, 717 Delaware St SE, 3rd Floor West, Minneapolis, MN 55414. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2010 by the American Academy of Pediatrics
The prevalence of overweight among children and adolescents has risen in recent years and has become a focus of public health efforts nationally.1 Thirty years ago, the prevalence of overweight and obesity (BMI ⱖ 85th percentile) in the pediatric population was⬃15%; in 2003–2004 it was more than 30%.2Recent studies indicate the upward trend may be stabilizing over the previous few years.3 There are many acute and chronic comorbidities associated with overweight and obe-sity; for instance, higher BMI during childhood is significantly associated with higher coronary heart disease risk in adulthood.4
Despite the increase in overweight prevalence and the increased atten-tion by government organizaatten-tions and the media on the public health prob-lem of obesity, studies have revealed that many overweight adolescents do not recognize their own overweight status. For example, Goodman et al5 ex-amined data from 1994 to 1995 and found that for nearly 40% of obese ad-olescents, neither the adolescent nor their parent recognized the adoles-cent’s obesity. Brener et al6found that 20% of overweight participants in a convenience sample of adolescents re-ported they were underweight; more recently, Standley et al7found that 26% of overweight adolescents in a sample in London did not accurately perceive their weight status. In addition, sex and racial/ethnic disparities exist in adolescents around the issue of weight perception.6,8
Assessing recognition of the problem is a key component of patient-centered counseling. These counseling meth-ods, such as motivational interviewing, have been efficacious9and have been recommended when addressing over-weight in the clinical setting.10,11 Al-though overweight among adolescents has increased over the previous de-cade, the recognition of overweight
status among adolescents in the United States during this time period is unclear.
It is unclear how weight misperception relates to weight-related behaviors in overweight adolescents; most re-search thus far has focused on behav-iors in all overweight adolescents12 and all adolescents who perceive themselves as overweight.13Shi et al13 found nearly twice as many adoles-cents who perceive themselves as overweight reported dieting in the pre-vious year compared with those who perceived themselves as normal. Infor-mation about weight-related behav-iors in overweight misperceivers may be useful for clinicians in their coun-seling efforts; for example, if an over-weight adolescent reports he or she is normal or underweight, the clinician may consider assessing weight-related behaviors and matching coun-seling efforts to patients’ self-efficacy.
The purpose of this study was to exam-ine within overweight adolescents the (1) proportion of misperceivers (those who do not assess themselves as overweight) over time and (2) demo-graphic characteristics and weight-related behaviors of accurate perceiv-ers compared with misperceivperceiv-ers. We examined weight self-perception in overweight adolescents by using na-tionally representative data collected every 2 years from 1999 to 2007. The weight-related behaviors compared among accurate perceivers and mis-perceivers in 2007 included both healthy and unhealthy practices.
METHODS
Study Population and Design
The Centers for Disease Control and Prevention (CDC) national Youth Risk Behavior Survey (YRBS) is a biennial nationally representative survey of students in 9th through 12th grade.14 Self-report of height and weight was added in 1999. For this study, data
from the 1999 through 2007 surveys were used to describe perception ac-curacy over a range of years. Analysis of demographic characteristics and weight-related behaviors was con-ducted on data from the 2007 survey.
Survey administration was approved by the CDC’s institutional review board and secondary analysis was approved by the University of Minnesota’s insti-tutional review board. A 3-stage clus-ter sample design produced a nation-ally representative sample of students in grades 9 to 12 who attend public and private schools. Oversampling of black and Hispanic students was performed to enable separate analysis.14
The surveys were completed voluntar-ily with the permission of schools and parents. Surveys were self-administered with the guidance of trained data collectors during 1 class period, and no identifying information was recorded. The numbers of partici-pants were 15 349 in 1999, 13 601 in 2001, 15 214 in 2003, 13 917 in 2005, and 14 041 in 2007. The overall re-sponse rates (school rere-sponse rate multiplied by the participant response rate) were 66% in 1999, 63% in 2001, 67% in 2003, 67% in 2005, and 68% in 2007.15–19
Measures
Survey questions pertaining to height, weight, age, sex, race/ethnicity, weight perception, and weight-related behav-iors were used. BMI was calculated by converting the self-report of height in feet and inches and weight in pounds to metric units and by using the stan-dard formula (weight in kg/m2). We used a program available from the CDC to estimate BMI percentiles, which ac-counts for age and sex.20Age in months was used to obtain the BMI percentiles, estimated by taking the age in years recorded on the survey, multiplying by 12, and adding 6. Implausible BMI
BMI percentile categories were as-signed according to the 2000 growth charts as follows: ⬎95th percentile, obese; 85th to 95th percentile, over-weight; 5th to 85th percentile, normal; and ⬍5th percentile, underweight.21 The present study included only re-spondents who were classified as overweight or obese (BMIⱖ85th per-centile), collectively referred to in this article as “overweight.”
Self-perception of weight was mea-sured by asking the question, “How do you describe your weight?” Response options included “very overweight,” “slightly overweight,” “about the right weight,” “slightly underweight,” and “very underweight.” To aid in analysis, response options were collapsed into 2 categories: (1) overweight (includes “very” and “slightly”) and (2) about right or underweight (includes “very” and “slightly”). Using these 2 weight perception categories, overweight re-spondents who described themselves as overweight were classified as accu-rate perceivers; overweight respon-dents who described themselves as about right or underweight were clas-sified as misperceivers.
Grade level was described by 4 catego-ries (grades 9 –12). Sex was classified as male or female by asking “What is your sex?” Race/ethnicity was ascer-tained by asking 2 questions: (1) “Are you Hispanic or Latino? (yes or no)”; and (2) “What is your race?” Possible classifications were American Indian or Alaska Native, Asian, black or Afri-can AmeriAfri-can (non-Hispanic), Hispanic or Latino, Native Hawaiian or other Pacific Islander, white (non-Hispanic), multiple-Hispanic, or multiple–non-Hispanic. To maintain sufficient num-bers of participants in each category, categories were collapsed into the fol-lowing: black or African American
Weight control behaviors were as-sessed with several questions. Partici-pants were asked, “which of the follow-ing are you tryfollow-ing to do about your weight?” Possible responses were, “lose weight,” “gain weight,” “stay the same weight,” or “I am not trying to do anything about my weight.” Questions about behaviors used in the previous 30 days to lose weight or to keep from gaining weight were, did you “exer-cise,” “eat less food, fewer calories, or foods low in fat,” “go without eating for 24 hours or more (also called fast-ing),” “take any diet pills, powders, or liquids without a doctor’s advice,” or “vomit or take laxatives?” Possible re-sponses were “yes” or “no.”
Other weight-related activities ana-lyzed were fruit and vegetable (FV) in-take (percentage of students who ate FVsⱖ5 times per day during the previ-ous 7 days), mild physical activity (PA) (percentage of students who partici-pated in PA that did not make them sweat or breathe hard for ⱖ30 min-utes or more onⱖ5 days of the previ-ous 7 days), and moderate-to-vigorprevi-ous PA (percentage of students who exer-cised or participated in PA that made them sweat and breathe hard forⱖ20 minutes onⱖ3 of the previous 7 days). These thresholds are consistent with goals and recommendations pub-lished by the US government.22–25
Analysis
Statistical analyses were performed by using Stata 9.2 (StataCorp, College Station, TX). An␣level of .05 was used to indicate statistical significance and all tests were 2-sided. All analyses were performed on weighted data to reflect a nationally representative sample and controlled for the cluster sampling design. We examined the pro-portions of overweight participants with weight misperception at each of
acteristics and behaviors of accu-rate perceivers and misperceivers, cross tabulations were examined by using2tests for categorical variables andt tests for continuous variables. Weight-related behaviors of accurate perceivers were compared with mis-perceivers by using multivariate logis-tic regression, adjusting for age, race/ ethnicity, and BMI percentile, and stratifying by sex. On the basis of pre-vious evidence of sex differences in weight perception, stratification by sex was performed.5,6
RESULTS
The number of participants available for analysis in 1999, 2001, 2003, 2005, and 2007 were 14 388, 12 501, 13 504, 12 989, and 12 853, respectively. The proportion of participants at ⱖ85th percentile in each of the years studied were 25% in 1999, 24% in 2001, 27% in 2003, 29% in 2005, and 29% in 2007.
Weight Misperception in 1999 –2007
From 1999 through 2007, the propor-tion of overweight adolescents who misperceived their weight ranged from 29% to 33%. In 1999, 30.6% of overweight adolescents were misper-ceivers. Subsequently, the proportion of misperceivers was 30.7% in 2001, 31.2% in 2003, 29.3% in 2005, and 32.8% in 2007. Specifically in 2007, 0.8% of overweight respondents described themselves as “very underweight,” 1.7% as “slightly underweight,” 30% as “about the right weight,” 56% as “slightly overweight,” and 12% as “very overweight.”
Demographic Characteristics in 2007
weight status (P⫽.12). Among male respondents, 40.2% were misperceiv-ers, whereas 22.6% of female respon-dents inaccurately perceived their weight status (P⬍.001; Table 1). Over 4 in 10 African American respondents (45.2%) were misperceivers, whereas 28.2% of white respondents were mis-perceivers (P ⬍ .001). Significantly more Hispanic respondents were mis-perceivers (34.7%) compared with white respondents (P⫽ .02). Signifi-cantly more African American respon-dents were misperceivers compared with Hispanic respondents (P⫽.009) and respondents of other races/eth-nicities (32%;P⬍.001). The proportion of respondents of other races/ethnic-ities who were misperceivers did not dif-fer significantly from white respondents or Hispanic respondents.
Weight-Related Characteristics and Behaviors in 2007
The mean BMI percentile of the accu-rate perceivers was 95% (SE: 0.13), which was significantly higher com-pared with the misperceivers, who had a BMI percentile of 92% (SE: 0.12) (P⬍
.001). In bivariate analyses, the propor-tion of accurate perceivers reporting engaging in most of the weight-related behaviors assessed was significantly higher than the proportion of misper-ceivers engaging in these activities (Table 2). Significantly fewer accurate perceivers reported achieving remended levels of FV intake and PA com-pared with misperceivers.
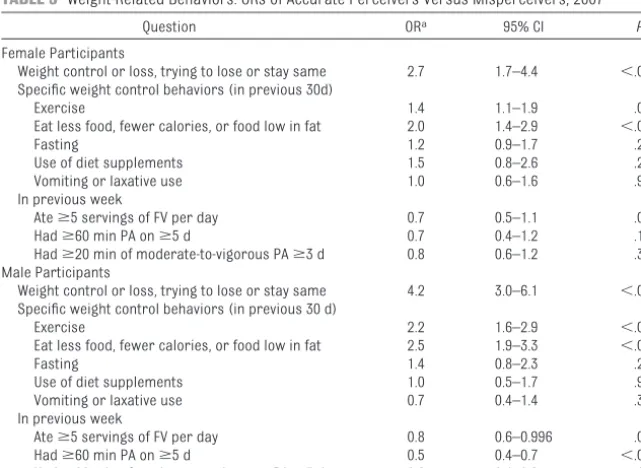
Table 3 contains measures from the adjusted model of weight-related be-haviors among overweight adoles-cents who accurately perceive and misperceive their weight status. When compared with misperceivers, accu-rate perceivers of both sexes had sig-nificantly higher odds of engaging in several weight-related behaviors, ad-justing for age, race/ethnicity, and BMI percentile. Among female participants,
accurate perceivers had nearly 3 times the odds of trying to lose weight or stay the same weight when
com-pared with misperceivers (odds ratio [OR]: 2.7 [95% confidence interval (CI): 1.7– 4.4]). Among male respondents
TABLE 1 Demographic Characteristics: Accurate Perceivers Versus Misperceivers, 2007 Characteristic Accurate Perceivers
(N⫽2479),n(%)a
Misperceivers (N⫽1208),n(%)a
P
Sex ⬍.001
Female 1206 (77.4) 352 (22.6) —
Male 1274 (59.8) 856 (40.2) —
Race/ethnicity
African American 382 (54.8) 314 (45.2) ⬍.001
Hispanic 238 (65.3) 126 (34.7) .02
Other 420 (67.8) 200 (32.2) .10
White 1402 (71.8) 550 (28.2) Referent
aAll counts and percentages are weighted.
TABLE 2 Weight-Related Behaviors: Misperceivers Versus Accurate Perceivers, 2007
Behavior Accurate Perceivers
(N⫽2478), %
Misperceivers (N⫽1204), %
P
Weight-related behaviors, % in each group reporting behavior
Weight control or loss, trying to lose or stay same 91 70 ⬍.001
Exercisea 81 69 ⬍.001
Eat less food, fewer calories, or food low in fata 66 40 ⬍.001
Fastinga 18 12 ⬍.001
Use of diet supplementsa 10 6 .02
Vomiting or laxative usea 6 4 .04
In the previous week
Ateⱖ5 servings FV per day 20 26 ⬍.001
Hadⱖ60 min PA onⱖ5 d 26 44 ⬍.001
Hadⱖ20 min of moderate-to-vigorous PAⱖ3 d 59 73 ⬍.001
Proportions reported are unadjusted.
aUsed in previous 30 days to lose weight or prevent weight gain.
TABLE 3 Weight-Related Behaviors: ORs of Accurate Perceivers Versus Misperceivers, 2007
Question ORa 95% CI P
Female Participants
Weight control or loss, trying to lose or stay same 2.7 1.7–4.4 ⬍.001 Specific weight control behaviors (in previous 30d)
Exercise 1.4 1.1–1.9 .01
Eat less food, fewer calories, or food low in fat 2.0 1.4–2.9 ⬍.001
Fasting 1.2 0.9–1.7 .25
Use of diet supplements 1.5 0.8–2.6 .20
Vomiting or laxative use 1.0 0.6–1.6 .95
In previous week
Ateⱖ5 servings of FV per day 0.7 0.5–1.1 .08
Hadⱖ60 min PA onⱖ5 d 0.7 0.4–1.2 .16
Hadⱖ20 min of moderate-to-vigorous PAⱖ3 d 0.8 0.6–1.2 .31 Male Participants
Weight control or loss, trying to lose or stay same 4.2 3.0–6.1 ⬍.001 Specific weight control behaviors (in previous 30 d)
Exercise 2.2 1.6–2.9 ⬍.001
Eat less food, fewer calories, or food low in fat 2.5 1.9–3.3 ⬍.001
Fasting 1.4 0.8–2.3 .24
Use of diet supplements 1.0 0.5–1.7 .90
Vomiting or laxative use 0.7 0.4–1.4 .33
In previous week
Ateⱖ5 servings of FV per day 0.8 0.6–0.996 .046
Hadⱖ60 min PA onⱖ5 d 0.5 0.4–0.7 ⬍.001
Hadⱖ20 min of moderate-to-vigorous PAⱖ3 d 0.6 0.4–0.9 .02
ORs reported are from a logistic regression model, adjusting for age, race/ethnicity, and BMI percentile.
aValues represent odds of accurate perceivers responding affirmatively relative to odds of misperceivers responding
affirmatively.
attempting weight maintenance or weight loss compared with misper-ceivers (OR: 4.2 [95% CI: 3.0 – 6.1]). Both male and female accurate per-ceivers had significantly higher odds of exercising and eating less to lose or maintain weight compared with misperceivers. Weight perception accuracy was not significantly asso-ciated with fasting, using diet supple-ments, vomiting, or using laxatives for weight control among overweight adolescents.
Male accurate perceivers had signifi-cantly lower odds of reporting rec-ommended levels of FV intake and PA in the week before the survey admin-istration. Among female accurate perceivers compared with female misperceivers, there was no signifi-cant difference in the odds of report-ing recommended levels of FV intake and PA.
DISCUSSION
In this nationally representative sam-ple of overweight adolescents, we found that the proportion of over-weight adolescents who were misper-ceivers (reported they are “about right” or “underweight”) was substan-tial, ranging from 29% to 33% from 1999 through 2007. Significantly more male respondents were misperceivers compared with female respondents. In addition, both female and male accu-rate perceivers had significantly higher odds of reporting some healthy weight-related behaviors compared with misperceivers, after adjusting for age, race/ethnicity, and BMI percen-tile.
Our finding that nearly 1 in 3 over-weight adolescents misperceives their weight coincides with previous find-ings. In previous studies of adoles-cents, the proportion of misperceivers ranged from 20% to 40%,5–7,13and
re-32% in the years 1988 –1994 to 38% in the years 1999 –2004.26There may be opposing influences on weight percep-tion in children. Some factors could de-crease misperception: childhood over-weight and obesity is perceived as a serious problem,27 and exposure to weight-related media is positively as-sociated with weight-related behav-iors in adolescent girls.28However, in some populations overweight percep-tion is associated with psychological distress29; this may provide a disincen-tive for developing an overweight per-ception. There is also evidence that de-spite increasing weight in the general population, recent improvements have been reported in body image in adolescents.30
We found that overweight male adoles-cents were more likely to be misper-ceivers compared with overweight fe-male adolescents. The authors of previous studies investigating weight misperception in adolescents have also found higher rates of mispercep-tion among overweight boys compared with overweight girls.5,6Wardle et al31 reported gender differences in weight perception in a study of university stu-dents from several countries, such as a pattern of underestimation of weight in men. Investigators have explored various possible explanations for these differences. Field et al32 found gender differences in influences on weight-related concerns (eg, parental opinion about a child’s weight affects weight concerns more in girls than in boys), and comparing one’s own body with images found in the media (media body comparison) has been demon-strated to mediate effects on body dis-satisfaction among adolescent girls but not adolescent boys.33
In our study, African American and Hispanic respondents were signifi-cantly more likely to be
misperceiv-other research finding race/ethnic-ity differences in weight percep-tion.7,34Neumark-Sztainer et al8found that adolescent girls who were African American reported fewer weight-related concerns compared with ado-lescent girls who were white. Signifi-cant differences in BMI for age exist across races/ethnicities, with higher rates of obesity found in some groups of Mexican American and black youth compared with white children and ad-olescents.3If health disparities are to be eliminated, we need to better un-derstand how these differences in per-ception may disturb progress toward reducing overweight and obesity.
After adjusting for age, race/ethnicity, and BMI percentile, we found that over-weight accurate perceivers of both sexes had significantly higher odds of reporting several healthy weight-related behaviors, whereas the odds of reporting some unhealthy weight-related behaviors were not signifi-cantly higher among accurate perceiv-ers. The authors of other studies of adolescents have linked unhealthy weight-related behaviors with over-weight12and overweight perception,13 but these studies did not focus on over-weight misperceivers. Accurate per-ception of overweight status was not without its downsides. Accurate per-ceivers were less likely to report rec-ommended levels of PA and FV intake. This is consistent with studies in adults,35but Shi et al13did not find that FV intake differed by weight percep-tion. One potential explanation for the difference in FV intake is that accurate perceivers may be eating less overall, although these differences need to be replicated before any major conclu-sions can be reached.
more accurate than self-report and are preferred, although self-reported data are valuable when no directly measured source is available.36Many studies have revealed that bias occurs in self-report compared with direct measures of height and weight, mostly overestimation of height and underes-timation of weight.36,37The authors of a study measuring the reliability of the height and weight self-report in YRBS found the questions to be highly reli-able, with high correlation between self-reported values and measured values, although with overestimation of height by an average of 2.7 in, and underestimation of weight by an aver-age of 3.5 lb.38If the potential misclas-sification is nondifferential, this bias could result in underestimation of weight misperception in our sample because the misperceivers had a lower mean BMI percentile compared with those with accurate weight per-ception. Additional studies on the topic of weight perception disparity in ado-lescents should explore these relation-ships by using objective measure-ments of height and weight when possible.
Another study limitation is the unavail-ability of a socioeconomic status marker in the YRBS. Thus,
socioeco-nomic status remains a potential con-founder. In addition, because height and weight questions were not intro-duced until 1999, the data used to cal-culate the proportion of overweight adolescents who are misperceivers is limited to 1999 through 2007. Thus, the present study does not assess misper-ception before 1999, when the rise in prevalence of overweight in children began.39
The findings in this study have impor-tant implications for clinical practice. Our findings that a substantial propor-tion of overweight adolescents do not recognize they are overweight is a re-minder to clinicians that a variety of counseling strategies, such as patient-centered counseling and motivational interviewing, will be needed to combat overweight and obesity.11 Misperceiv-ers may need counseling directed at recognition of the problem; the find-ings that accurate perceivers did not have significantly higher levels of un-healthy weight-related behaviors after adjustment for age, race/ethnicity, and BMI percentile provide some support that increased recognition may not be harmful. In addition, the findings of higher levels of some healthy weight-related behaviors in accurate perceiv-ers provide support to the hypothesis
that recognition of one’s own over-weight status may carry some benefit. However, on the basis of the findings that some accurate perceivers were less likely to achieve recommended levels of FV intake and PA, clinicians need to remain focused on educating their overweight and obese patients on healthy lifestyle choices.
CONCLUSIONS
The data presented in this study high-light the substantial weight misper-ception that exists in overweight ado-lescents. Accurate weight perception is associated with several healthy weight-related behaviors. Clinicians should individualize their approach to their overweight patients, depending on the patients’ recognition of the problem.
ACKNOWLEDGMENTS
The authors were supported in part by the Adolescent Health Protection Program (School of Nursing, Univer-sity of Minnesota) grant number T01-DP000112 (Principal Investiga-tor: Bearinger) from the CDC.
We thank the fellows, faculty, and staff in the Department of Pediatrics and School of Nursing, University of Minnesota for their assistance.
REFERENCES
1. Centers for Disease Control and Preven-tion. DATA2010: The healthy people 2010 database. Available at: http://wonder. cdc.gov/data2010. Accessed August 29, 2009
2. Ogden CL, Yanovski SZ, Carroll MD, Flegal KM. The epidemiology of obesity. Gastroen-terology.2007;132(6):2087–2102
3. Ogden CL, Carroll MD, Flegal KM. High body mass index for age among US children and adolescents, 2003–2006. JAMA. 2008; 299(20):2401–2405
4. Baker JL, Olsen LW, Sorensen TIA. Childhood body mass index and the risk of coronary heart disease in adulthood.N Engl J Med. 2007;357(23):2329 –2337
5. Goodman E, Hinden BR, Khandelwal S. Accu-racy of teen and parental reports of obesity
and body mass index.Pediatrics. 2000; 106(1 pt 1):52–58
6. Brener ND, Eaton DK, Lowry R, McManus T. The association between weight perception and BMI among high school students.Obes Res.2004;12(11):1866 –1874
7. Standley R, Sullivan V, Wardle J. Self-perceived weight in adolescents: over-estimation or under-over-estimation?Body Im-age.2009;6(1):56 –59
8. Neumark-Sztainer D, Croll J, Story M, Han-nan PJ, French SA, Perry C. Ethnic/racial dif-ferences in weight-related concerns and behaviors among adolescent girls and boys: findings from project EAT.J Psycho-som Res.2002;53(5):963–974
9. Burke BL, Arkowitz H, Menchola M. The effi-cacy of motivational interviewing: a
meta-analysis of controlled clinical trials.J Con-sult Clin Psychol.2003;71(5):843– 861
10. Resnicow K, Davis R, Rollnick S. Motivational interviewing for pediatric obesity: concep-tual issues and evidence review.J Am Diet Assoc.2006;106(12):2024 –2033
11. Barlow SE; Expert Committee. Expert com-mittee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report.Pediatrics.2007; 120(suppl 4):S164 –S192
12. Boutelle K, Neumark-Sztainer D, Story M, Resnick M. Weight control behaviors among obese, overweight, and nonoverweight ado-lescents. J Pediatr Psychol.2002;27(6): 531–540
13. Shi Z, Lien N, Nirmal Kumar B,
10(3):298 –305
14. Brener ND, Kann L, Kinchen SA, et al. Meth-odology of the youth risk behavior surveil-lance system.MMWR Recomm Rep.2004; 53(RR-12):1–13
15. Kann L, Kinchen SA, Williams BI, et al. Youth risk behavior surveillance: United States, 1999.MMWR CDC Surveill Summ. 2000; 49(5):1–32
16. Grunbaum JA, Kann L, Kinchen S, et al. Youth risk behavior surveillance: United States, 2003.MMWR Surveill Summ.2004; 53(2):1–96
17. Grunbaum JA, Kann L, Kinchen SA, et al. Youth risk behavior surveillance: United States, 2001.MMWR Surveill Summ.2002; 51(4):1– 62
18. Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance: United States, 2005. MMWR Surveill Summ.2006;55(5):1–108
19. Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance: United States, 2007. MMWR Surveill Summ.2008;57(4):1–131
20. Centers for Disease Control and Prevention. A SAS program for the CDC growth charts. Available at: www.cdc.gov/nccdphp/dnpa/ growthcharts/resources/sas.htm. Accessed August 29, 2009
21. Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growth charts: United States. Adv Data.2000;8(314):1–27
22. US Department of Health and Human Ser-vices.2008 Physical Activity Guidelines for Americans. Hyattsville, MD: US Department of Health and Human Services; 2008. Avail-able at: www.health.gov/paguidelines. Ac-cessed August 29, 2009
23. US Department of Health and Human Ser-vices.Dietary Guidelines for Americans.
cessed August 29, 2009
24. US Department of Health and Human Ser-vices. Objective 22. In:Healthy People 2010. Washington, DC: US Department of Health and Human Services; 2000. Available at: www.healthypeople.gov/Document/HTML/ Volume2/22Physical.htm. Accessed August 29, 2009
25. US Department of Health and Human Ser-vices. Objective 19. In:Healthy People 2010. Washington, DC: US Department of Health and Human Services; 2000. Available at: www.healthypeople.gov/Document/HTML/ Volume2/19Nutrition.htm. Accessed August 29, 2009
26. Johnson-Taylor WL, Fisher RA, Hubbard VS, Starke-Reed P, Eggers PS. The change in weight perception of weight status among the overweight: comparison of NHANES III (1988 –1994) and 1999 –2004 NHANES.Int J Behav Nutr Phys Act.2008;5:9
27. Evans WD, Finkelstein EA, Kamerow DB, Renaud JM. Public perceptions of childhood obesity.Am J Prev Med.2005;28(1):26 –32 28. Field AE, Cheung L, Wolf AM, Herzog DB,
Gort-maker SL, Colditz GA. Exposure to the mass media and weight concerns among girls. Pediatrics. 1999;103(3). Available at: www.pediatrics.org/cgi/content/full/103/3/ e36
29. Atlantis E, Ball K. Association between weight perception and psychological dis-tress.Int J Obes (Lond).2008;32(4):715–721
30. Cash TF, Morrow JA, Hrabosky JI, Perry AA. How has body image changed? A cross-sectional investigation of college women and men from 1983 to 2001.J Consult Clin Psychol.2004;72(6):1081–1089
31. Wardle J, Haase AM, Steptoe A. Body image and weight control in young adults:
interna-32. Field AE, Camargo CA, Jr, Taylor CB, Berkey CS, Roberts SB, Colditz GA. Peer, parent, and media influences on the development of weight concerns and frequent dieting among preadolescent and adolescent girls and boys.Pediatrics.2001;107(1):54 – 60
33. van den Berg P, Paxton SJ, Keery H, Wall M, Guo J, Neumark-Sztainer D. Body dissatis-faction and body comparison with media images in males and females.Body Image. 2007;4(3):257–268
34. Strauss RS. Self-reported weight status and dieting in a cross-sectional sample of young adolescents: national health and nutrition examination survey III.Arch Pediatr Adolesc Med.1999;153(7):741–747
35. Atlantis E, Barnes EH, Ball K. Weight status and perception barriers to healthy physical activity and diet behavior.Int J Obes (Lond). 2008;32(2):343–352
36. Sherry B, Jefferds ME, Grummer-Strawn LM. Accuracy of adolescent self-report of height and weight in assessing overweight status: a literature review.Arch Pediatr Adolesc Med.2007;161(12):1154 –1161
37. Gorber SC, Tremblay M, Moher D, Gorber B. A comparison of direct versus self-report measures for assessing height, weight and body mass index: a systematic review.Obes Rev.2007;8(4):307–326
38. Brener ND, Mcmanus T, Galuska DA, Lowry R, Wechsler H. Reliability and validity of self-reported height and weight among high school students.J Adolesc Health.2003; 32(4):281–287
DOI: 10.1542/peds.2009-0185 originally published online February 8, 2010;
2010;125;e452
Pediatrics
Nicholas Murphy Edwards, Sandra Pettingell and Iris Wagman Borowsky
Adolescents
Where Perception Meets Reality: Self-Perception of Weight in Overweight
Services
Updated Information &
http://pediatrics.aappublications.org/content/125/3/e452 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/125/3/e452#BIBL This article cites 31 articles, 3 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/obesity_new_sub
Obesity
icine_sub
http://www.aappublications.org/cgi/collection/adolescent_health:med
Adolescent Health/Medicine
http://www.aappublications.org/cgi/collection/endocrinology_sub
Endocrinology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2009-0185 originally published online February 8, 2010;
2010;125;e452
Pediatrics
Nicholas Murphy Edwards, Sandra Pettingell and Iris Wagman Borowsky
http://pediatrics.aappublications.org/content/125/3/e452
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.