Prevalence, Stability, and Predictors of Clinically Significant Behavior
Problems in Low Birth Weight Children at 3, 5, and 8 Years of Age
Ronald F. Gray, MB, ChB, MPH; Alka Indurkhya, PhD; and Marie C. McCormick, MD, ScD
ABSTRACT. Objectives. To examine the prevalence, stability, and predictors of clinically significant behavior problems in 869 preterm low birth weight (LBW) infants at 3, 5, and 8 years of age.
Methods. A prospective cohort study was conducted. Clinically significant behavior problems were assessed using dichotomized total problem Child Behavior Checklist scores in LBW children at ages 3, 5, and 8 years. Baseline sociodemographic and obstetric data were col-lected. Maternal General Health Questionnaire per-formed at 40 weeks’ gestation was dichotomized at a score of 12 to give a measure of maternal psychological distress. Prevalence and stability of behavior problems at ages 3, 5, and 8 were determined and potential predictors of behavior problems at age 3, 5, and 8 were examined using multiple logistic regression.
Results. Prevalence of behavior problems remained at⬃20% at 3, 5, and 8 years. Stability of behavior prob-lems between different ages was⬃50%. Significant be-havior problems at ages 3, 5, and 8 were predicted by maternal psychological distress at 40 weeks (odds ratio [OR]: 1.59; 95% confidence interval [CI]: 1.21–2.09), ma-ternal cigarette smoking during pregnancy (OR: 1.57; 95% CI: 1.20 –2.04), Hispanic ethnicity (OR: 2.00; 95% CI: 1.24 – 3.24), and maternal age (OR: 0.97; 95% CI: 0.94 – 0.99).
Conclusions. This sample had double the prevalence of behavior problems expected in the general child pop-ulation. These problems showed stability over time. Cig-arette smoking in pregnancy, maternal psychological dis-tress at 40 weeks’ gestation, maternal age, and Hispanic ethnicity all were significant predictors of the develop-ment of behavior problems from ages 3 to 8. These find-ings have implications for health policies on smoking and postnatal depression.Pediatrics2004;114:736–743; in-fant, premature, low birth weight, Child Behavior Check-list, prevalence, stability, outcome predictors.
ABBREVIATIONS. LBW, low birth weight; IHDP, Infant Health and Development Program; GHQ, General Health Questionnaire; CBCL, Child Behavior Checklist; OR, odds ratio; CI, confidence interval.
P
reterm low birth weight (LBW) infants are at an increased risk for the subsequent develop-ment of both cognitive and behavioral prob-lems in childhood.1,2These problems haveimplica-tions for school performance3 and later life.4
Although the factors that affect cognitive develop-ment in this group have been examined extensively, less attention has been paid to the factors that affect behavior.
LBW infants have higher average scores on mea-sures of problem behavior than control subjects1and
are more likely to have clinically significant behavior disorders.5In particular, there is a well-documented
association between prematurity and later develop-ment of attention-deficit/hyperactivity disorder.6
Al-though the prevalence of behavior disorders in LBW infants has been established in the short term, few studies have examined stability of behavior disor-ders in these children in the longer term. Two studies that have reported that 40% to 50% of LBW children with significant behavior problems continue to dis-play them 3 years later.5,7
As with cognitive development in LBW infants, the development of child behavioral problems is known to be influenced by a number of environmen-tal factors,8,9 but many of the existing follow-up
studies of LBW children have reported on relatively few predictors of outcome other than gender, ethnic-ity, and socioeconomic status. This may be in part because they have included small populations from single sites. These studies generally have not identi-fied factors during pregnancy or the neonatal period that might be modified to reduce the risk of behavior problems, but this is important if we want to im-prove the content of early intervention programs. Therefore, there is an urgent need for studies on preterm LBW children that 1) recruit from multiple sites and in larger numbers, 2) measure prevalence of child behavior problems in a clinically meaningful way across pre- and midschool periods, and 3) con-sider a wide range of potential predictors of out-come, particularly predictors that are potentially modifiable through intervention.
The present study had 3 objectives: 1) to establish the prevalence of clinically significant behavior prob-lems in a sample of preterm LBW infants at 3, 5, and 8 years of age; 2) to determine the stability of clini-cally significant behavior problems between 3 and 8 years of age; and 3) to identify potentially modifiable factors during pregnancy or the neonatal period that might be altered to reduce the risk for behavior
prob-From the Department of Maternal and Child Health, Harvard School of Public Health, Boston, Massachusetts.
Accepted for publication Apr 26, 2004. DOI: 10.1542/peds.2003-1150-L
Reprint requests to (R.F.G.) National Perinatal Epidemiology Unit, Institute of Health Sciences, University of Oxford, Old Road, Headington, Oxford OX3 7LF, United Kingdom. E-mail: ron.gray@perinatal-epidemiology. oxford.ac.uk
lems. To address these objectives, we relied on data collected for those who participated in the Infant Health and Development Program (IHDP).10–12
METHODS Study Sample and Design
The IHDP was a multisite, randomized, controlled trial of the effect of early childhood support and education from birth to age 3 years corrected for duration of gestation on the social, emotional, and cognitive outcomes in LBW premature infants. Subject selec-tion and method of the IHDP is described fully elsewhere.13
Briefly, infants were eligible when they were born preterm (⬍37 weeks’ gestation) and weighed⬍2500 g at birth. A total of 985 participating mother– child dyads were recruited at 8 sites in the United States between January 7, 1985, and October 9, 1985. One third of the group were randomly assigned to the intervention and compared with the remainder, who received routine follow-up only. The study design included stratification by birth weight: one third of the sample weighed between 2001 and 2500 g, and two thirds weighed 2000 g or less. The intervention group was pro-vided with both home-visiting services and center-based child care from birth to age 3, corrected for gestational age.
Measures
Baseline data were collected by interview at entry to the trial, maternal self-reported mental health was measured using the 12-item General Health Questionnaire (GHQ)14at 40 weeks,
ges-tation and parent-reported behavior problems in the child were assessed at age 3 using the Child Behavior Checklist for Ages 2 to 3 (CBCL/2–3)15and at ages 5 and 8 using the CBCL/4 –18.16
CBCL/2–3
The CBCL/2–3 lists various types of behavior and emotional problems that occur in children aged 2 and 3 years. Each of 99 problem items is scored 0⫽not true, 1⫽somewhat or sometimes true, and 2⫽very true or often true, based on the preceding 2 months. Scores on each item are summed to give a raw total problems score. Higher scores indicate more behavior problems. A suggested cutoff point dichotomizes “clinical” and “normal”
groups and has been shown to discriminate efficiently between children who are referred to mental health services and nonre-ferred children.15
CBCL/4 –18
The CBCL/4 –18 is a widely used, parent-completed checklist that identifies various types of behavior and emotional problems that occur in children aged 4 and above. Each of 118 problem items is scored 0⫽not true, 1⫽somewhat or sometimes true, and 2⫽ very true or often true, based on the preceding 6 months. Scores on each item are summed to give a raw total problems score. Higher scores indicate more behavior problems. Gender-specific cutoff points dichotomize clinical and normal groups and have been shown to discriminate efficiently between children who are re-ferred to mental health services and nonrere-ferred children.16
Fifty-four of the problem items are common to both the CBCL/2–3 and the CBCL/4 –18.
GHQ
The 12-item GHQ has been used to screen for short-term changes in mental health in a number of large-scale, community-based surveys as well as in clinical studies. The respondent as-sesses her present state compared with her usual state by answer-ing 12 items on a 4-point scale: better than usual, same as usual, worse than usual, much worse than usual. We use a cutoff point of 12 to dichotomize a group with significant psychological dis-tress from a normal group.14
Baseline Measures
Baseline measures of interest in predicting child behavior prob-lems were identified. These included marital status and living arrangement, trimester of first prenatal care, alcohol consumption during pregnancy, cigarette consumption during pregnancy, ges-tational age at birth as defined using the Ballard method,17and the
child’s birth order. In keeping with previous work13on the IHDP,
we also included the more established risk factors of child gender, race/ethnicity, birth weight, neonatal health,18 maternal age at
birth, and level of education. Treatment group assignment was included to adjust for any potential treatment effect. The catego-rizations of these variables are summarized in Table 1.
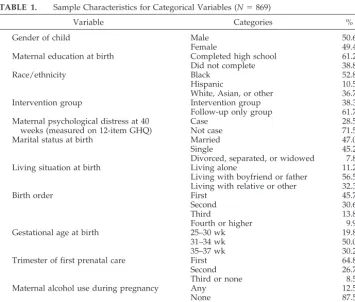
TABLE 1. Sample Characteristics for Categorical Variables (N⫽869)
Variable Categories %
Gender of child Male 50.6
Female 49.4
Maternal education at birth Completed high school 61.2
Did not complete 38.8
Race/ethnicity Black 52.8
Hispanic 10.5
White, Asian, or other 36.7
Intervention group Intervention group 38.3
Follow-up only group 61.7
Maternal psychological distress at 40 weeks (measured on 12-item GHQ)
Case 28.5
Not case 71.5
Marital status at birth Married 47.0
Single 45.2
Divorced, separated, or widowed 7.8
Living situation at birth Living alone 11.2
Living with boyfriend or father 56.5 Living with relative or other 32.3
Birth order First 45.7
Second 30.6
Third 13.8
Fourth or higher 9.9
Gestational age at birth 25–30 wk 19.8
31–34 wk 50.0
35–37 wk 30.2
Trimester of first prenatal care First 64.8
Second 26.7
Third or none 8.5
Maternal alcohol use during pregnancy Any 12.5
None 87.5
Maternal cigarette use during pregnancy Any 33.1
Statistical Analysis
All of the categorical variables were treated as nominal vari-ables and dummy coded. The unadjusted prevalence of being in the clinical group at each age (3, 5, and 8) was determined. The prevalence stratified by birth weight and each of the categorical variables was then derived. Then the percentages that remained in the clinical and normal groups at ages 5 and 8 were computed. Next, using a logit model, the odds ratios (ORs) of being in the clinical group at ages 5 and 8, conditional on being in the clinical group at ages 3 and 5, were determined.
Finally, alternating multiple logistic regression19,20was used to
model the outcome (clinical vs normal group assignment on the CBCL/2–3 and the CBCL/4 –18 from ages 3 through 8) as a function of the baseline measures and GHQ. This method is ap-propriate with repeated observations when the responses at each time point may be correlated. It gives more conservative estimates of confidence intervals (CIs) than ordinary logistic regression. The method uses the data on all 869 subjects (not just data on the 804 with complete data). The longitudinal element of time is incorpo-rated into this model using age of testing (3, 5, and 8 years) as an additional covariate dummy coded to make age 3 the baseline. SAS 8.221was used for the analysis. The full main effects logistic
regression model included 2 sets of predictor variables. The first set was site of randomization, gender of child, race/ethnicity of child, maternal education, maternal age, birth weight, neonatal health index, and treatment group assignment. These variables were kept in a reduced model to be consistent with previous analyses in this sample. The second set of predictor variables was marital status, maternal psychological distress at 40 weeks’ gesta-tion, living arrangement, trimester of first prenatal care, alcohol consumption during pregnancy, cigarette consumption during pregnancy, gestational age at birth, birth order, and age at testing. If these variables did not contribute significantly to the model, then they could be dropped.
The IHDP was approved by both local and national Human Subjects Committees. This analysis has been approved by the Harvard School of Public Health Human Subjects Committee.
RESULTS Description of Sample
Of the 985 subjects who were randomly allocated to intervention or follow-up only, data were com-plete at 3 years of age on 869. These form the popu-lation for this study. Complete outcome data at all 3 time points were present on 804 (92.5%) of the 869 children.
Comparison of the 869 subjects with 116 excluded because of incomplete data showed no significant differences in gender (2 ⬍0.01, P ⫽ .96, df ⫽ 1),
race/ethnicity (2⫽0.44,P⫽.80,df⫽2), site (2⫽
7.37,P⫽.39,df⫽7), treatment group assignment (2
⬍0.01,P⫽.94,df⫽1), marital status (2⫽1.78,P⫽
.41,df⫽2), maternal age (ttestP⫽.46), birth weight (ttestP⫽.49), or Neonatal Health Index (ttestP⫽ .09). However, there was a significant difference for maternal education (2⫽4.58,P⫽.03,df⫽1): 49.1%
of mothers with missing data did not complete high school compared with 38.8% of those who did.
The characteristics of the sample for the categorical variables are shown in Table 1. The mean birth weight for the sample was 1799.1 g (standard devi-ation: 453 g), and the mean maternal age at time of birth was 24.8 years (standard deviation: 6 years).
Prevalence
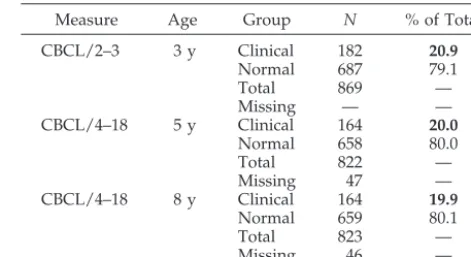
Table 2 shows estimates of point prevalence at each age. Consistent with the way the instrument is normed and scored, the results show no significant variation in point prevalence over time: 20.9% (95%
CI: 18.2–23.6) at age 3, 20.0% (95% CI: 17.2–22.7) at age 5, and 19.9% (95% CI: 17.2–22.7) at age 8.
Table 3 shows prevalence at each age of testing stratified by the 2 birth weight strata and by the categorical variables. The prevalence did not seem to be influenced by birth weight at any age. At age 3, prevalence was significantly increased in children whose mother did not complete high school com-pared with those whose mother did and in children whose mother either did not attend at all for prenatal care or did not attend until the third trimester. These differences were no longer apparent by ages 5 and 8. Children of mothers with psychological distress at 40 weeks’ gestation and children of lone mothers had a consistently higher prevalence between ages 3 and 8 of clinically significant behavior problems, but this difference was statistically significant only at age 5. Similarly, children of mothers who smoked during pregnancy showed a consistently increased preva-lence of clinically significant behavior problems, but this difference was statistically significant only at age 8. Children of Hispanic mothers had a consistently higher prevalence rate than mothers with white or black ethnicity, and children of divorced single or widowed mothers also showed higher prevalence rates.
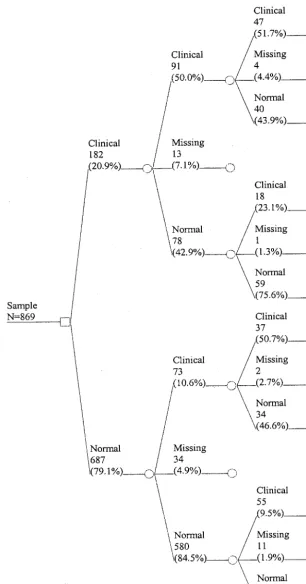
Stability
Figure 1 shows both numbers and proportions of the sample in the clinical and normal groups at ages 3, 5, and 8 years. A total of 311 (35.8%) of the 869 subjects were in the clinical group on at least 1 occa-sion. Of the 182 children in the clinical group at age 3, 50.0% remained in the clinical group at age 5, and 51.7% of the group who were in the clinical group at both ages 3 and 5 remained in the clinical group at age 8. However, these 47 subjects, who were in the clinical group at all ages (3, 5, and 8), made up only 5.4% of the entire sample of 869.
If a child was in the clinical group at age 3, then that child was 9.27 (95% CI: 6.29 –13.67) times more likely to be in the clinical group at age 5 than a child who was in the normal group at age 3 and 4.17 (95% CI: 2.87– 6.06) times more likely at age 8 to be in the clinical group. If a child was in the clinical group at age 5, then that child was 8.91 (95% CI: 6.00 –13.24)
TABLE 2. Numbers Categorized as Being in the Clinical and Normal Groups at Each Age on the CBCL/2–3 and the CBCL/4 – 18, Shown as a Percentage of the Total
Measure Age Group N % of Total
CBCL/2–3 3 y Clinical 182 20.9
Normal 687 79.1
Total 869 —
Missing — —
CBCL/4–18 5 y Clinical 164 20.0
Normal 658 80.0
Total 822 —
Missing 47 —
CBCL/4–18 8 y Clinical 164 19.9
Normal 659 80.1
Total 823 —
Missing 46 —
times more likely to be in the clinical group at age 8 than a child who was in the normal group at age 5. Finally, if a child was in the clinical group at both age 3 and age 5, then that child was 6.48 (95% CI: 4.06 – 10.35) times more likely to be in the clinical group at age 8 than those in the clinical group at 1 time point and in the normal group at another or in the normal group at both time points.
Predictors
After fitting a full main effects model, age at test-ing, marital status, living situation, trimester of first prenatal care, birth order, gestational age, and alco-hol during pregnancy were shown to have no signif-icant effects; therefore, these variables were removed in a reduced model. The reduced model included the
following variables: site of randomization, gender of child, race/ethnicity of child, maternal education, maternal age, birth weight, neonatal health index, treatment group assignment, maternal psychological distress, and cigarette consumption during preg-nancy.
The effects of birth weight and neonatal health were not significant in the model. Sociodemographic variables, effects of treatment assignment, and sig-nificant predictors are presented as ORs. These re-sults show that after adjustment, the average odds of being in the clinical as opposed to the normal group at ages 3, 5, and 8 were significantly and indepen-dently predicted by 4 baseline characteristics: mater-nal psychological distress at 40 weeks, matermater-nal cig-arette smoking during pregnancy, Hispanic
TABLE 3. Point Prevalence by Categorical Variables and Age at Testing
VARIABLE Point Prevalence
3 Years 5 Years 8 Years
Overall prevalence 20.9 (18.2–23.6) 20.0 (17.2–22.7) 19.9 (17.2–22.7)
Birth weight
2001–2500 g 20.9 (16.5–25.4) 18.5 (14.1–23.0) 19.6 (15.1–24.1)
ⱕ2000 g 21.0 (17.6–24.4) 20.8 (17.4–24.3) 20.2 (16.8–23.6)
Gender of child
Male 20.8 (17.0–24.6) 20.7 (16.8–24.6) 22.2 (18.2–26.3)
Female 21.2 (17.4–25.0) 19.3 (15.5–23.1) 17.7 (14.0–21.4)
Maternal education at birth
Completed high school 16.4 (13.3–19.5) 18.3 (14.9–21.6) 18.2 (14.9–21.6)
Did not complete 28.2 (23.4–33.0) 22.8 (18.2–27.5) 22.8 (18.2–27.5)
Race/ethnicity
Black 23.8 (19.9–27.7) 18.1 (14.5–21.7) 19.9 (16.2–23.6)
Hispanic 28.6 (19.3–37.9) 34.2 (23.9–44.5) 24.4 (15.1–33.7)
White, Asian, or other 14.8 (10.9–18.7) 18.9 (14.5–23.3) 18.9 (14.5–23.3)
Intervention group 17.8 (13.7–21.9) 16.5 (12.4–20.6) 19.9 (15.5–24.3)
Follow-up only group 23.0 (19.4–26.6) 22.1 (18.5–25.7) 24.4 (15.1–33.7)
Maternal psychological distress
Case 25.9 (20.4–31.3) 27.7 (21.9–33.5) 25.7 (20.1–31.3)
Not case 19.1 (16.0–22.1) 17.1 (14.0–20.1) 17.8 (14.7–20.8)
Marital status at birth
Married 16.2 (12.7–19.8) 16.3 (12.6–20.0) 17.1 (13.3–20.8)
Single 24.0 (19.8–28.2) 21.8 (17.6–26.0) 22.0 (17.8–26.2)
Divorced, separated, or widowed 32.4 (21.3–43.5) 33.4 (21.1–45.6) 26.4 (14.9–37.8) Living situation at birth
Living alone 25.8 (17.1–34.5) 34.1 (24.2–44.0) 29.6 (20.1–39.1)
Living with boyfriend or father 18.0 (14.6–21.4) 18.1 (14.7–21.6) 17.3 (13.9–20.7) Living with relative or other 24.6 (19.6–26.6) 18.6 (13.9–23.3) 21.6 (16.6–26.5) Birth order
First 20.5 (16.5–24.4) 16.8 (13.1–20.6) 20.0 (16.0–24.0)
Second 21.9 (16.9–26.8) 20.7 (15.8–25.7) 20.1 (15.2–25.0)
Third 22.5 (15.1–30.0) 26.2 (17.9–34.5) 18.4 (11.1–25.7)
Fourth or higher 18.7 (10.4–26.9) 24.1 (14.7–33.5) 21.6 (12.5–30.6)
Gestational age at birth
25–30 wk 23.3 (17.0–29.6) 20.4 (14.3–26.5) 19.1 (13.0–25.1)
31–34 wk 19.8 (16.1–23.6) 19.9 (16.0–23.8) 20.9 (17.0–24.8)
35–37 wk 21.4 (16.5–26.4) 19.9 (14.9–24.9) 19.1 (14.2–24.0)
Trimester of first prenatal care
First 17.5 (14.3–20.6) 19.0 (15.7–22.3) 17.8 (14.6–21.1)
Second 26.3 (20.7–32.0) 23.4 (17.7–29.1) 24.2 (18.5–30.0)
Third or none 31.1 (20.6–41.7) 17.2 (8.4–26.0) 23.6 (13.5–33.7)
Maternal alcohol use during pregnancy
Any 17.5 (10.4–24.6) 14.9 (8.0–21.8) 22.0 (13.9–30.2)
None 21.5 (18.6–24.4) 20.7 (17.8–23.7) 19.7 (16.8–22.6)
Maternal cigarette use during pregnancy
Any 26.1 (21.0–31.2) 22.5 (17.5–27.4) 26.9 (21.6–32.2)
None 18.5 (15.3–21.6) 18.8 (15.5–22.0) 16.6 (13.5–19.7)
ethnicity, and maternal age. Controlling for other variables, the odds of a child’s being in the clinical as opposed to the normal group were 59% higher in children whose mother had psychological distress at 40 weeks, 57% higher in children whose mother
smoked during pregnancy, and doubled in Hispanic children compared with children in the white or other group. The odds were reduced by ⬃3% for each year of increase in maternal age. This means that the risk was nearly halved in a mother aged 33
at birth compared with a mother aged 16 at birth. The results of fitting the reduced model are shown in Table 4.
DISCUSSION
Our first objective was to establish the prevalence of clinically significant behavior problems. We found that the prevalence of behavior problems in this sam-ple of preterm LBW children remained at⬃20% at 3, 5, and 8 years of age.
The prevalence of clinically significant behavior problems using the dichotomized total problems scores on the CBCL/2–3 and CBCL/4 –18 was twice the 10% prevalence expected in normative popula-tion samples, suggesting that, on average, prematu-rity and LBW double the risk of behavior problems. This is supported by another study showing that LBW children were twice as likely as normal birth weight children to have clinically significant behav-ior problem scores.22Additional support comes from
a random effects meta analysis of 6 case-control stud-ies.1This study reported a relative risk of 2.64 for the
development of attention-deficit/hyperactivity dis-order in LBW children compared with normal birth weight control subjects. The higher prevalence of clinically significant behavior problems in children of smokers, Hispanic mothers, and those with psy-chological distress at 40 weeks’ gestational age was reflected in the multivariate model.
Our second objective was to establish the stability of clinically significant behavior problems. We found that once these problems had developed, they showed moderate stability over time. This stability is greater between time periods 2 or 3 years apart than over the interval of 3 to 8 years. The stability in the short term is consistent with the literature.5
Our third objective was to identify which sociode-mographic and obstetric characteristics of the mother and the child at the time of the birth were indepen-dent predictors of clinically significant behavior problems at ages 3, 5, and 8. Maternal smoking dur-ing pregnancy, maternal age at time of birth, and being Hispanic as opposed to white race/ethnicity were significant predictors of behavior problems at 3, 5, and 8. These results for significant predictors are consistent with the existing literature. Longer estab-lished predictors of child behavior problems such as gender, birth weight, gestational age, and neonatal
health were not significant predictors of outcome when included in the multivariate model. These pre-dictors might well have been significant in a different sample of predominantly very low or extremely low birth weight infants.
The predictive value of maternal age independent of socioeconomic status is in keeping with previous reports.23The finding that Hispanic children were at
double the risk of clinically significant behavior problems is consistent with previous work24
show-ing higher risk in Puerto Rican children for behav-ioral and developmental disorders, but very little research has been done in this area for preterm LBW children.25
We identified 2 modifiable factors: maternal psy-chological distress and maternal cigarette smoking during pregnancy. The marked effects of maternal psychological distress are in keeping with the litera-ture suggesting that maternal distress modifies the relationship between mother and infant at a number of levels and in a reciprocal manner to increase the risk of behavior problems and other psychiatric dis-orders.26 The persistence of this effect, arising from
maternal psychological distress at 40 weeks’ gesta-tion, has not to our knowledge been demonstrated before in preterm LBW children. It may reflect long-term impairment of the mother– child relationship arising from maternal psychological distress at 40 weeks’ gestation. However, it seems more likely that the maternal psychological distress at 40 weeks’ ges-tation represents a snapshot of recurrent or chronic maternal psychological distress or even unmeasured or residual confounders reflecting underlying mater-nal vulnerability. The association of smoking during pregnancy and increased risk of behavior problems also, to our knowledge, has not been shown before in a preterm LBW cohort. Smoking and postnatal de-pression are frequently found together and may rep-resent part of a pattern of risk factors found in asso-ciation with social deprivation, which in turn is also associated with increased risk of child behavior problems. However, this study controlled for mater-nal education as a proxy for social deprivation, and the smoking effect was independent of the effect of psychological distress. Therefore, the association of child behavior problems with smoking may repre-sent a real teratogenic effect as has been shown in other recent work27 on term infants. If so, then this
TABLE 4. Results of Fitting the Reduced Alternating Logistic Regression Model
Variable Comparison OR Upper
95% CI
Lower 95% CI
Gender of child Female vs male 0.92 0.71 1.19
Race/ethnicity Black vs white or other 1.34 0.93 1.93
Hispanic vs white or other 2.00* 1.24 3.24
Maternal age (For an increase in age of 1 year) 0.97* 0.94 0.99
Maternal education Did not complete vs completed high school 1.26 0.93 1.71
Treatment group assignment Randomized to follow-up only vs. intervention 1.26 0.97 1.64
Maternal psychological distress at 40 weeks (measured on 12-item GHQ)
Case vs not case 1.59† 1.21 2.09
Maternal cigarette smoking in pregnancy Any vs none 1.57† 1.20 2.04
Adjusted ORs of being in the clinical and normal groups at ages 3, 5, and 8 on the CBCL/2–3 and the CBCL/4 –18 are shown for the sociodemographic variables, effects of treatment assignment, and significant predictors. Significant effects are marked.
finding adds to the increasing body of literature showing an association between maternal smoking during pregnancy and later behavioral problems in children after controlling for birth weight.28
There are a number of limitations in this study. First, the cohort was born 17 years ago, when the mortality of very low birth weight infants was con-siderably higher than it is now.29A second limitation
is that cigarette smoking during pregnancy was as-sessed by maternal recall with no independent vali-dation performed (eg, measuring cotinine levels). However, this would not have been possible given that recruitment was not until after the birth. Moth-ers may not have reported smoking if they did, but it seems unlikely that they would report smoking if they did not smoke. Failure to detect maternal smok-ing would lead to a misclassification error, which might have diluted the relationship of smoking with behavior, but we still obtained a relationship. A third limitation is that outcome data were available only on 869 of the 985 involved in the IHDP. Those moth-ers for whom data were not available were less likely to have completed high school and therefore may have been at increased risk for child behavioral prob-lems. This means that the prevalence rates found in the study may be underestimates. Another limitation of maternal report on child behavior problems is that depressed mothers may be more likely to rate their children as more disturbed. This may have biased the analysis.
The study has a number of implications for clinical practice. First, it suggests that greater attention be paid to maternal smoking during pregnancy. Smok-ing cessation programs are worthwhile in any event: a recent systematic review30concluded that smoking
cessation programs in pregnancy reduce smoking, LBW, and preterm birth. Our results suggest that additional benefits may accrue. Also, assessment of maternal mood with widely used screening ques-tionnaires such as the Edinburgh Postnatal Depres-sion Scale31should be performed while the infant is
in the neonatal intensive care unit. Appropriate in-tervention could reduce maternal morbidity as well as reduce the risk of later child behavior problems. We suggest interpreting the increased risk for behav-ior problems in Hispanic children compared with the white (and black) population with caution. The num-bers involved were small, and Hispanic mothers may have had a lower threshold for reporting behavior problems than the other ethnic groups in this study. In summary, in a sample of 869 preterm LBW children who were recruited at 8 US sites and fol-lowed up to age 8, we found a prevalence of clini-cally significant behavior problems approximately double what might be expected in the general pop-ulation. We found that these problems showed mod-erate stability once they developed. Finally, we have identified 2 potentially modifiable factors for which interventions might reduce the risk of behavior prob-lems: cigarette smoking in pregnancy and maternal psychological distress at 40 weeks’ gestation.
Recent follow-up studies of LBW children in ado-lescence and young adulthood have found catch-up growth, a reduction in acute health problems,32and
a lower rate of drug and alcohol misuse4compared
with control subjects. These findings are not fully understood and suggest the need for additional work. Data collection on phase 4 of the IHDP is currently in progress (the participating children are now 18 years of age) and hopefully will shed some light on these interesting findings.
ACKNOWLEDGMENTS
This study was partially supported by funds from the Robert Wood Johnson Foundation (I.D. 039543) and the National Insti-tutes of Health (MH01880). Dr Gray is supported by The Com-monwealth Fund, a New York City– based private independent foundation. The views presented here are those of the authors and not necessarily those of The Commonwealth Fund and its director, officers, or staff.
Related work from this study has been presented in abstract form at the Pediatric Academic Societies’ Annual Meeting; May 3– 6, 2003; Seattle, WA (Pediatr Res.2003;53:351A, 460A).
We thank Dr S. Buka for comments on an earlier draft and the 2 anonymous reviewers for helpful comments.
REFERENCES
1. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis.JAMA.2002;288:728 –737
2. Buka SL, Lipsett LP, Tsuang MT. Emotional and behavioral develop-ment of low birthweight infants. In: Friedman SL, Sigman MD, eds.The Psychological Development of Low Birthweight Children. Norwood, NJ: Ablex Publishing; 1992:187–214
3. Klebanov PK, Brooks-Gunn J, McCormick MC. School achievement and failure in very low birth weight children.J Dev Behav Pediatr.1994;15: 248 –256
4. Hack M, Flannery DJ, Schluchter M, Cartar L, Borawski E, Klein N. Outcomes in young adulthood for very-low-birth-weight infants.
N Engl J Med.2002;346:149 –157
5. Rose SA, Feldman JF, Rose SL, Wallace IF, McCarton C. Behavior problems at 3 and 6 years—prevalence and continuity in full terms and pre-terms.Dev Psychopathol.1992;4:361–374
6. Botting N, Powls A, Cooke RW, Marlow N. Attention deficit hyperac-tivity disorders and other psychiatric outcomes in very low birthweight children at 12 years.J Child Psychol Psychiatry.1997;38:931–941 7. Miller M, Bowen JR, Gibson FL, Hand PJ, Ungerer JA. Behaviour
problems in extremely low birthweight children at 5 and 8 years of age.
Child Care Health Dev.2001;27:569 –581
8. Miceli PJ, Goeke-Morey MC, Whitman TL, Kolberg KS, Miller-Loncar C, White RD. Brief report: birth status, medical complications, and social environment: individual differences in development of preterm, very low birth weight infants.J Pediatr Psychol.2000;25:353–358
9. McCarton C. Behavioral outcomes in low birth weight infants. Pediat-rics.1998;102(suppl E):1293–1297
10. McCormick MC, McCarton C, Tonascia J, Brooks-Gunn J. Early educa-tional intervention for very low birth weight infants: results from the Infant Health and Development Program.J Pediatr.1993;123:527–533 11. Brooks-Gunn J , McCarton CM, Casey PH, et al. Early intervention in
low-birth-weight premature infants. Results through age 5 years from the Infant Health and Development Program. JAMA. 1994;272: 1257–1262
12. McCarton CM, Brooks-Gunn J, Wallace IF, et al. Results at age 8 years of early intervention for low-birth-weight premature infants. The Infant Health and Development Program.JAMA.1997;277:126 –132 13. McCormick MC, McCarton C, Brooks-Gunn J, Belt P, Gross RT. The
Infant Health and Development Program: interim summary.J Dev Behav Pediatr.1998;19:359 –370
14. Goldberg D, Williams P.A User’s Guide to the General Health Question-naire. Windsor, United Kingdom: NFER-Nelson; 1988
15. Achenbach T.Manual for the Child Behavior Checklist/2-3 and 1992 Profile. Burlington, VT: University of Vermont Department of Psychiatry; 1992 16. Achenbach T.Manual for the Child Behaviour Checklist/4-18 and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychi-atry; 1991
19. Carey V, Zeger SL, Diggle PJ. Modeling multivariate binary data with alternating logistic regression.Biometrika.1991;80:517–526
20. Lipsitz SR, Laird NM, Harrington DP. Generalized estimating equations for correlated binary data: using the odds ratio as a measure of associ-ation.Biometrika.1991;78:153–160
21. SAS Institute.SAS/STAT User’s guide, Version 8.0. Cary, NC: SAS Insti-tute Inc; 2000
22. McCormick MC, Workman-Daniels K, Brooks-Gunn J. The behavioral and emotional well-being of school-age children with different birth weights.Pediatrics.1996;97:18 –25
23. Orlebeke JF, Knol DL, Boomsma DI, Verhulst FC. Frequency of parental report of problem behavior in children decreases with increasing ma-ternal age at delivery.Psychol Rep.1998;82:395– 404
24. Arcia E, Keyes L, Gallagher JJ. Indicators of developmental and func-tional status of Mexican-American and Puerto Rican children.J Dev Behav Pediatr.1994;15:27–33
25. Flores G, Fuentes-Afflick E, Barbot O, et al. The health of Latino children: urgent priorities, unanswered questions, and a research agenda.JAMA.2002;288:82–90
26. Campbell S.Behavior Problems in Preschool Children: Clinical and Devel-opmental Issues. 2nd ed. New York, NY: The Guilford Press; 2002
27. Law KL, Stroud LR, LaGasse LL, Niaura R, Liu J, Lester BM. Smoking during pregnancy and newborn neurobehavior. Pediatrics. 2003; 111(suppl):1318 –1323
28. Wakschlag LS, Pickett KE, Cook E Jr, Benowitz NL, Leventhal BL. Maternal smoking during pregnancy and severe antisocial behavior in offspring: a review.Am J Public Health.2002;92:966 –974
29. Lemons JA et al. Very low birth weight outcomes of the National Institute of Child health and human development neonatal research network, January 1995 through December 1996. NICHD Neonatal Re-search Network.Pediatrics.2001;107(1). Available at: www.pediatrics. org/cgi/content/full/107/1/e1
30. Lumley J, Oliver S, Waters E. Interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst Rev. 2000;(2): CD001055
31. Cox JL, Holden JM, Sagovsky R. Detection of postnatal depression. Development of the 10-item Edinburgh Postnatal Depression Scale.Br J Psychiatry.1987;150:782–786
32. Saigal S, Stoskopf BL, Streiner DL, Burrows E. Physical growth and current health status of infants who were of extremely low birth weight and controls at adolescence.Pediatrics.2001;108:407– 415
HOW TO FIND THE LATEST ON RESULTS OF CLINICAL TRIALS
“The current push to require drug companies to disclose their unpublished clinical trials could unleash a flood of new information for doctors and patients. But in the meantime, there is already a growing effort by medical publishers, scientific groups, and government agencies aimed at helping people find and interpret clinical-trials results online. To find clinical-trial results:
• Clinicaltrials.gov: Lists more than 10,000 trials, with links to completed studies • Cancer.gov: Lists open cancer trials; links to latest results with easy-to-read
summaries
• Centerwatch.com: Lists over 41,000 active studies, and summarizes completed trials
• Trialscentral.org: Links to summaries of evidence from trials around the world.”
Landro L.Wall Street Journal. June 17, 2004
DOI: 10.1542/peds.2003-1150-L
2004;114;736
Pediatrics
Ronald F. Gray, Alka Indurkhya and Marie C. McCormick
in Low Birth Weight Children at 3, 5, and 8 Years of Age
Prevalence, Stability, and Predictors of Clinically Significant Behavior Problems
Services
Updated Information &
http://pediatrics.aappublications.org/content/114/3/736 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/114/3/736#BIBL This article cites 23 articles, 3 of which you can access for free at:
Subspecialty Collections
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior Developmental/Behavioral Pediatrics
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2003-1150-L
2004;114;736
Pediatrics
Ronald F. Gray, Alka Indurkhya and Marie C. McCormick
in Low Birth Weight Children at 3, 5, and 8 Years of Age
Prevalence, Stability, and Predictors of Clinically Significant Behavior Problems
http://pediatrics.aappublications.org/content/114/3/736
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.