in Children
WHAT’S KNOWN ON THIS SUBJECT: Aluminum is ubiquitous and exposure is unavoidable. Adverse health effects have been associated with large exposures in workers or those with chronic kidney disease. There are no established age-specific reference ranges or toxicity data for populations of healthy children.
WHAT THIS STUDY ADDS: We demonstrate the wide variability of aluminum reference ranges in biological samples and that the ranges are not based on studies including healthy children. Further research is necessary to establish clinically relevant reference ranges for healthy children.
abstract
BACKGROUND:Some parents are requesting aluminum testing in their children with developmental issues. Although aluminum can be mea-sured in plasma, serum, or urine, there is scant scientific information about normal ranges. We sought to determine the basis for laboratory reference ranges and whether these ranges are applicable to children.
METHODS: From texts, published lists, and Internet sources, we ob-tained the names of 10 clinical laboratories that perform aluminum testing. Contact was made by telephone or e-mail, or Internet sites were viewed to obtain information regarding the establishment of aluminum reference ranges and testing methods in biological samples. Seven laboratories provided supporting literature that was reviewed regarding details of the study populations.
RESULTS:For laboratories using the atomic absorption spectrometry method, aluminum reference ranges varied from,5.41mg/L to,20 mg/L (serum),,7.00mg/L to 0 to 10mg/L (plasma) and 5 to 30mg/L (urine). For those using the inductively coupled plasma mass spectroscopy methodology, ranges varied from 0 to 6 mg/L to ,42 mg/L (serum), 0 to 10mg/L to 0 to 15mg/L (plasma), and 0 to 7mg/L to 5 to 30mg/L (urine). None of the reference ranges are known to be derived from studies of healthy children, but relied instead on small studies of adult populations, adult dialysis patients, workers, or sick children on aluminum-containing parenteral therapy.
CONCLUSIONS:Aluminum reference ranges provided by laboratories are widely divergent, may not represent“normal”ranges of a healthy population, especially children, and thus it is difficult to interpret serum or urine aluminum ranges clinically. Further studies of alumi-num in children are warranted and should be considered as part of the Centers for Disease Control and Prevention Biomonitoring Project.
Pediatrics2012;129:e142–e147
AUTHORS:Michelle Zeager, DO, MPH,a,b,c,dAlan D. Woolf,
MD, MPH,a,b,cand Rose H. Goldman, MD, MPHa,b,e,f,g
aDivision of General Pediatrics, Department of Pediatric
Environmental Health, Children’s Hospital Boston, Boston, Massachusetts;bNew England Pediatric Environmental Health Specialty Unit, Boston, Massachusetts; Departments of
c
Pediatrics andfMedicine, Harvard Medical School, Boston, Massachusetts;dHarlingen Pediatrics Associates, Harlingen, Texas;gDepartment of Environmental Health, Harvard School of Public Health, Boston, Massachusetts;eDivision of Occupational and Environmental Medicine, Cambridge Health Alliance, Cambridge, Massachusetts
KEY WORDS
aluminum, aluminum toxicity, childhood aluminum, reference range
ABBREVIATIONS
AAS—atomic absorption spectrometry ASD—autistim spectrum disorder
ICP-MS—inductively coupled plasma mass spectroscopy MRL—minimum risk level
This work and publication was supported in part by the cooperative agreement award 1U61TS000118-022 from the Agency for Toxic Substances and Disease Registry (ATSDR). Its contents are the responsibility of the authors and do not necessarily represent the official views of the Agency for Toxic Substances and Disease Registry (ATSDR). The US Environmental Protection Agency (EPA) supports the PEHSU by providing funds to ATSDR under Inter-Agency Agreement number DW-75-92301301-0. Neither EPA nor ATSDR endorse the purchase of any commercial products or services mentioned in PEHSU publications. The contents do not represent the official views of any of the clinical laboratories listed in the article.
www.pediatrics.org/cgi/doi/10.1542/peds.2010-3481
doi:10.1542/peds.2010-3481
Accepted for publication Sep 9, 2011
Address correspondence to Michelle Zeager DO, MPH, Children’s Hospital Boston, Department of General Pediatrics, 1295 Boylston Street, Suite 100, Boston, MA 02115. E-mail: michelle.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2012 by the American Academy of Pediatrics
Parents of children with developmental delays and the autism spectrum dis-order (ASD) are sometimes concerned that specific environmental contribut-ing factors, such as mercury in vaccines or toxic chemicals in foods, are the cause for their child’s delays.1,2 More
recently, parents consulting our Pediat-ric Environmental Health Specialty Unit have raised concerns about the family’s aluminum exposure and whether such exposures might have contributed to their child’s ASD. Little scientific in-formation exists on low-dose aluminum exposure and adverse health effects, particularly in children. Yet, various Internet Web sites have promoted the theory of environmental sources of aluminum as a toxin that may be as-sociated with ASD. As a result, parents of children with ASD have begun requesting testing for aluminum dur-ing visits to pediatric practitioners. The following 2 case reports illustrate this issue.
CASE REPORTS
Case 1
Parents brought their 2 ½-year-old child with pervasive developmental disorder to the Children’s Hospital Boston, Pediatric Environmental Health Center, inquiring about toxic expo-sures in the environment as possible contributing factors to the child’s de-velopmental delays. They were par-ticularly concerned about exposure to metals, namely aluminum in vacci-nations, and requested information and biological testing. The child’s subse-quently obtained 8-hour urine alumi-num level was 2mg/L, which was well within the laboratory’s reference range of 0 to 7mg/L.
Case 2
A second case presented as a tele-phone consultation regarding a 4-month-old breastfed infant with mild developmental delay. The mother had
her breast milk analyzed and the test-ing revealed an aluminum level in the 97th percentile for the laboratory’s re-ference range. She then requested an aluminum level to be checked on her child. The infant’s serum aluminum level was 17mg/L, which was above the lab-oratory’s reference range of 0 to 9mg/L; however, a 24-hour urine aluminum level was subsequently found to be 2mg/L, well below the laboratory’s ref-erence range of 5 to 30mg/L.
These case reports and additional queries from parents about testing for aluminum raise the following ques-tions. What is the basis of aluminum reference ranges provided by labora-tories? Do the reference ranges accu-rately reflect population background levels of aluminum? Can the reference ranges be applied to healthy children? If results of testing fall above the refer-ence ranges provided, does it neces-sarily represent aluminum toxicity?
The purposes of the current study are (1) to investigate the scientific basis for the reference ranges provided by US commercial laboratories measur-ing aluminum levels in bodyfluids and (2) to determine whether these refer-ence ranges are applicable or useful in evaluating children.
METHODS
United States commercial clinical lab-oratories were ascertained in a num-ber of different ways. A general Internet search by using Google Search En-gine for“aluminum reference ranges,” “lab reference ranges,” or “clinical labs in the United States” was con-ducted in January 2009 to obtain a list of those laboratories offering blood or urine aluminum levels.3Texts and
online sources that provide links to laboratories that either perform the biological testing for aluminum or had links to laboratories that collect the specimens and send them else-where for testing were also used.3,4A
telephone survey of personnel at these commercial laboratories was conducted to obtain information as to how the laboratory’s aluminum reference ranges were derived. In those cases where telephone contact could not be achieved (n= 6), the survey was conducted by electronic mail correspondence. For those commercial laboratories that could not be contacted by telephone or e-mail (n =3), information provided on the laboratory’s Internet Web site was reviewed. All data collected were analyzed with the use of descriptive statistics.
RESULTS
Reported Reference Ranges
From January 2009 until April 2009, aluminum reference ranges for serum, plasma, and 24-hour urine were ob-tained from 25 clinical laboratories throughout the United States that of-fered aluminum testing. Of the 25 lab-oratories, ten actually perform the biological testing for aluminum. The remainder send their specimens to 1 of these 10 laboratories for analysis. Table 1 provides a list of the 10 labora-tories that perform testing and also the method by which they test biological specimens for aluminum. For the labo-ratories that use the atomic absorption spectrometry (AAS) method of analy-sis, serum aluminum references ranged from,5.41mg/L to 0 to 9mg/L, and plasma references ranged from #7 mg/L to 0 to 10mg//L. Only 1 of the 10 laboratories used AAS to analyze urine; its urinary aluminum reference range was 5 to 30mg/L or 0 to 32mg/day. For laboratories that use inductively cou-pled plasma mass spectroscopy (ICP-MS) methodology, the serum references ranged from 0 to 6mg/L to,42mg/L, the plasma references ranged from 0 to 10mg/L to 0 to 15mg/L and for urine the references ranged from 0 to 7mg/L to,30mg/L or 0 to 10mg/day to 7 to 40mg/day.
Basis for Reference Ranges
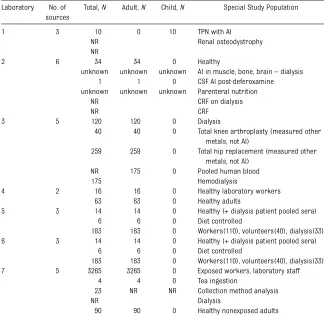
Seven of the 10 laboratories that per-form the aluminum testing revealed in-formation on the sources they used to derive the aluminum reference ranges for serum, plasma, or 24-hour urine specimens (Table 2). Limited studies were available to laboratories for de-termining aluminum reference ranges. Most of the studies cited have small sample sizes,5–7 were done in adult
patients or adult workers,5,8–13or
ex-amined the adverse effects of alumi-num in adult populations with chronic renal failure or those on dialysis,8,14–20
some of whom were getting the alumi-num in large doses through intravenous administration. None of the reported aluminum reference ranges were age specific. None referenced aluminum concentrations measured directly in healthy children. From the sources provided, we found only 1 small study looking at the urinary and plasma alu-minum levels in 10 ill children who were receiving aluminum-containing
parenteral nutrition at the time.21 The
Centers for Disease Control and Pre-vention surveillance program in bio-logical monitoring for exposure to chemicals has not yet included test-ing for aluminum; hence, population-based studies of background aluminum levels in the United States are not readily available.22In addition, a
num-ber of the studies cited did not look at aluminum in biological specimens, but analyzed the levels of other metals.23,24
DISCUSSION
Aluminum is the most abundant metal in the earth’s crust and is found natu-rally in soil, water, and air.25It can also
be found in construction and manu-facturing materials, and in waste sites, as well. It is in some cookware, pro-cessed foods, beverages, additives and preservatives, sources of drinking wa-ter, medications such as buffered as-pirin and antacids, and personal care products such as cosmetics, sunscreens, lotions, toothpaste, and antiperspirants.25
milk and infant formula and from child-hood vaccinations.25 Other sources of
aluminum exposure for children may include parenteral nutrition, dialysate, and antacid medication. The most com-mon source of exposure acom-mong all age groups is from food and beverages.26
Dietary intake for children has been estimated to be 0.7 mg/day for 6- to 11-month-olds, 4.6 mg/day for 2-year-olds, 6.5 mg/day for 6-year-2-year-olds, and 6.8 mg/day for 10-year-olds.27
Typi-cally, less than 1% of aluminum is ab-sorbed through the gastrointestinal tract, although there are circum-stances in which absorption can be enhanced.28Absorbed aluminum can
be found in the urine within hours.28
Most of what is absorbed into blood is excreted in urine within days to weeks.29 Approximately 90% of what
is excreted in the urine occurs within thefirst 48 hours.30
Aluminum salts have been added to a number of vaccines to enhance the immune response.31,32
Measles-mumps-rubella, polio, meningococcal,
in-fluenza, and rotavirus vaccines do not contain aluminum. Those containing alu-minum that are given in early childhood include all formulations of hepatitis A, hepatitis B, diphtheria-tetanus, diphthe-ria, tetanus toxoids, and acellular per-tussis alone or as a combination vaccine, Haemophilus B Conjugate Vaccine, and Pneumococcal Conjugate Vaccines. The dose of aluminum from these vaccines will vary depending on which formu-lation (manufacturer-specific) is used and which combination is given. For example, a 2-month-old child receiv-ing the recommended vaccinations for age could receive a minimum potential exposure of 0.295 mg or a maximum potential exposure of 1.2 mg of alumi-num contained within those vaccina-tions. Although this is the potential quantity delivered to the injection site,
Method Serum Reference Range
Medical University of South Carolina (MUSC)a AAS ,5.41mg/L Mayo Medical Laboratoriesa ICP-MS 0-6mg/L Quest Diagnostics, San Juan Capistrano, CAa AAS ,7mg/L
LabCorpa AAS 0-9mg/L
Quest Diagnostics Nichols Institute, Chantilly, VAa ICP-MS ,7mg/L National Medical Systemsa ICP-MS ,15mg/L Associated Regional & University Pathologists, Inc (ARUP)a ICP-MS 0-15mg/L Specialty Laboratoriesa ICP-MS ,7mg/L
Medtox Laboratory ICP-MS ,42mg/L
Method Plasma Reference Range Quest Diagnostics San Juan Capistrano, CAa AAS ,7mg/L Quest Diagnostics Nichols Institute Chantilly, VAa AAS ,7mg/L Medical University of South Carolina (MUSC)a AAS 6-7mg/L
LabCorpa AAS 0-9mg/L
Sacred Heart MC AAS 0-10mg/L
National Medical Systemsa ICP-MS ,15mg/L Associated Regional & University Pathologists, Inc (ARUP)a ICP-MS 0-15mg/L
Method 24-h Urine Reference Range Associated Regional & University Pathologists, Inc (ARUP)a ICP-MS 0-7mg/L 0-10mg/day
LabCorpa AAS 5-30mg/L 0-32mg/day
Medtox Laboratory ICP-MS ,30mg/L
Mayo Medical Laboratoriesa ICP-MS ,33mg/day Specialty Laboratoriesa ICP-MS ,36mg/day National Medical Systemsa ICP-MS 7-40mg/day Quest Diagnostics Nichols Institute Chantilly, VAa ICP-MS 5-30mg/L,36mg/day
it may not all be absorbed in 1 day from the injection site. We have not found human data noting how much of the aluminum used in vaccines is actually absorbed from intramuscular or sub-cutaneous injections, and over what time period. One small study investi-gating the fate of radiolabeled alu-minum adjuvants that were injected intramuscularly into 6 New Zealand white rabbits reported that the labeled aluminum was measurable in the blood within 1 hour, with a relatively constant absorption rate from day 2 to day 28.33
The potential vaccine dose is well be-low the minimum risk level (MRL) of 1 mg/kg per day established for alu-minum by the Agency for Toxic Sub-stances and Disease Registry.28 An
MRL is defined as an estimate of daily human exposure to a substance that is likely to be without an appreciable
risk of adverse effects (noncarcinogenic) over a specified period of time.28
De-termination of the MRL for aluminum is based on data derived from animal studies in which the potential lowest effect level is further adjusted by the application of additional uncertainty factors to account for interspecies and intraspecies differences and an added modifying factor to account for differences in bioavailability of alu-minum.28 The result is a much lower
level that would therefore be consid-ered safe.
Aluminum Toxicity
There have been reports of aluminum overload that has been associated with toxicity in humans. Some patients with chronic renal failure who have been on dialysis have developed encepha-lopathy, osteomalacia, and microcytic
anemia after exposure to larger doses of aluminum.26,28In other studies,
pre-term infants receiving prolonged stan-dard aluminum-containing parenteral nutrition had impaired neurologic de-velopment.34It also has been reported
that children with renal insufficiency on aluminum-containing phosphate-binding medications have developed osteomalacia and encephalopathy.35
It is not clear, however, if these re-ported effects in the ill children were causally related to aluminum or to the other underlying medical conditions or other factors. There is currently a lack of data to support a correlation between aluminum exposure doses, alu-minum levels measured in biological samples, and adverse clinical out-comes.28
Laboratory Reference Ranges
Reference values are established as guidelines to identify those who may have an increased exposure to a par-ticular environmental substance in com-parison with general population levels.36
However, levels reported above back-ground population reference ranges are not necessarily reflective of an ex-posure level expected to cause adverse health effects. Some reference ranges address toxicity and are based on dose-response data for the purpose of keeping population (or worker) ex-posures below those levels to avoid toxicity. In the case of aluminum, there are limited toxicity and dose-response data in humans, and MRLs (as noted above) are primarily based on animal data.28In addition, appropriate
age-based reference ranges in healthy populations are lacking. Aluminum concentrations that exceed reference ranges may not imply toxicity or indi-cate excessive exposure to aluminum.
Additional problems with measuring aluminum are accuracy, reliability, and reproducibility of the results. Because aluminum is ubiquitous, extreme care
TABLE 2 Sources From Which Aluminum References Ranges Were Derived for Seven of the Laboratories That Perform Aluminum Testing
Laboratory No. of sources
Total,N Adult,N Child,N Special Study Population
1 3 10 0 10 TPN with Al
NR Renal osteodystrophy NR
2 6 34 34 0 Healthy
unknown unknown unknown Al in muscle, bone, brain–dialysis 1 1 0 CSF Al post-deferoxamine unknown unknown unknown Parenteral nutrition
NR CRF on dialysis
NR CRF
3 5 120 120 0 Dialysis
40 40 0 Total knee arthroplasty (measured other metals, not Al)
259 259 0 Total hip replacement (measured other metals, not Al)
NR 175 0 Pooled human blood
175 Hemodialysis
4 2 16 16 0 Healthy laboratory workers 63 63 0 Healthy adults
5 3 14 14 0 Healthy (+ dialysis patient pooled sera) 6 6 0 Diet controlled
183 183 0 Workers(110), volunteers(40), dialysis(33) 6 3 14 14 0 Healthy (+ dialysis patient pooled sera)
6 6 0 Diet controlled
183 183 0 Workers(110), volunteers(40), dialysis(33) 7 5 3265 3265 0 Exposed workers, laboratory staff
4 4 0 Tea ingestion
23 NR NR Collection method analysis
NR Dialysis
90 90 0 Healthy nonexposed adults
Al, aluminum;CRF, chronic renal failure;CSF, cerebrospinalfluid;N, the number of subjects in the study;NR, not reported; TPN, total parenteral nutrition
In addition, the timing of collection has to be considered, especially when ver-ifying the results of a test, because there are circadian rhythm changes in aluminum levels in healthy individuals. Levels tend to be higher in the morn-ing and lowest in the early evenmorn-ing.37
Diets vary widely among individuals, and food, beverages, or medications consumed within hours to days of bio-logical testing can influence the re-sults.26,28If a test needs to be repeated
because the result exceeds a given ref-erence range, it would need to be col-lected in a similar manner, at the same time of day, and analyzed by the same laboratory to provide any reliable com-parison.
Because our study was stimulated by cases involving urine and serum alu-minum tests in children, and because assessment of aluminum in hair is not
include inquiries to standard commer-cial laboratories concerning hair anal-ysis reference ranges. Hair analanal-ysis results for aluminum are not men-tioned in reliable references concern-ing biomonitorconcern-ing.28,38 Nevertheless, a
laboratory that does nontraditional testing for multiple“hair toxic elements” does include aluminum in the list of 30 elements tested (www.doctorsdata. com/repository.asp?id=1271), but the basis or the meaning of the reference levels provided are not clear.39Seidel
et al (2001) sent split samples of hair to 6 laboratories and found the anal-ysis of multiple elements to be un-reliable.40
CONCLUSIONS
In summary, our study found signifi -cant interlaboratory variability in the
the same method of analysis was used. In addition, the sources for deriving the reference ranges were limited and not derived from any studies of healthy children. There is currently a lack of data to support a correlation between aluminum exposure doses, aluminum levels measured in biological samples, and adverse clinical outcomes.28As a
result, it is difficult to provide mean-ingful interpretation to aluminum urine or blood monitoring results and to make clinical decisions based on the results. Therefore, clinicians should use discretion in making the decision to order a biological test for aluminum. Further research is needed to establish normal reference ranges for healthy children, and aluminum should be con-sidered for testing in the Centers for Disease Control and Prevention’s Bio-monitoring Project.
REFERENCES
1. Harrington J, Rosen L, Garnecho A. Parental perceptions and use of complementary and alternative medicine practices for children with autistic spectrum disorder in private practice. J Dev Behav Pediatr. 2006;27(2):S156–S161
2. Harrington JW, Patrick PA, Edwards KS, Brand DA. Parental beliefs about autism: implications for the treating physician. Au-tism. 2006;10(5):452–462
3. Martindale J. Laboratory tests, diagnostics & protocols center. In: Martindale’s The Ref-erence Desk. 1994-2009. Available at: http:// infotree.library.ohiou.edu/scripts/redirect. html?id=672. Accessed June 30, 2011
4. Bush C. Evaluating Aluminum Exposure: In-formation for Health Care Providers. Lans-ing, MI: State of Michigan Department of Community Health; 2004: 7
5. Gorsky JE, Dietz AA, Spencer H, Osis D. Metabolic balance of aluminum studied in six men.Clin Chem. 1979;25(10):1739–1743
6. Wu J, Zhou CY, Wong MK, Lee HK, Ong CN. Urine levels of aluminum after drinking tea. Biol Trace Elem Res. 1997;57(3):271–280
7. Ellenberg R, King AL, Sica DA, Posner M, Savory J. Cerebrospinal fluid aluminum
levels following deferoxamine.Am J Kidney Dis. 1990;16(2):157–159
8. Valentin H, Preusser P, Schaller KH. [The analyses of aluminum in serum and urine for monitoring of exposed persons (author’s transl)].Int Arch Occup Environ Health. 1976; 38(1):1–17
9. Valkonen S, Aitio A. Analysis of aluminum in serum and urine for the biomonitoring of occupational exposure.Sci Total Environ. 1997;199(1-2):103–110
10. White MA. A comparison of inductively coupled plasma mass spectrometry with electrothermal atomic absorption spec-trophotometry for the determination of trace elements in blood and urine from non occupationally exposed populations. J Trace Elem Med Biol. 1999;13(1-2):93–101
11. Ericson SP, McHalsky ML, Rabinow BE, et al. Sampling and analysis techniques for monitoring serum for trace elements.Clin Chem. 1986;32(7):1350–1356
12. Wang ST, Pizzolato S, Demshar HP. Alumi-num levels in normal human serum and urine as determined by Zeeman atomic ab-sorption spectrometry.J Anal Toxicol. 1991; 15(2):66–70
13. Chappuis P, Poupon J, Rousselet F. A se-quential and simple determination of zinc, copper and aluminium in blood samples by inductively coupled plasma atomic emis-sion spectrometry.Clin Chim Acta. 1992;206 (3):155–165
14. McCarthy JT, Milliner DS, Kurtz SB, Johnson WJ, Moyer TP. Interpretation of serum alu-minum values in dialysis patients. Am J Clin Pathol. 1986;86(5):629–636
15. Pierides AM, Edwards WG, Jr,Cullum UX, Jr, McCall JT, Ellis HA. Hemodialysis encepha-lopathy with osteomalacic fractures and mus-cle weakness.Kidney Int. 1980;18(1):115–124
16. Alderman FR, Gitelman HJ. Improved elec-trothermal determination of aluminum in serum by atomic absorption spectroscopy. Clin Chem. 1980;26(2):258–260
17. Soldado Cabezuelo AB, Blanco González E, Sanz-Medel A. Quantitative studies of alu-minium binding species in human uremic serum by fast protein liquid chromatog-raphy coupled with electrothermal atomic absorption spectrometry. Analyst (Lond). 1997;122(6):573–577
aluminum intoxication.N Engl J Med. 1976; 294(4):184–188
19. Wills MR, Savory J. Aluminum and chronic renal failure: sources, absorption, transport, and toxicity.Crit Rev Clin Lab Sci. 1989;27(1): 59–107
20. Tzamaloukas AH. Diagnosis and manage-ment of bone disorders in chronic renal failure and dialyzed patients. Med Clin North Am. 1990;74(4):961–974
21. Advenier E, Landry C, Colomb V, et al. Alu-minum contamination of parenteral nutri-tion and aluminum loading in children on long-term parenteral nutrition. J Pediatr Gastroenterol Nutr. 2003;36(4):448–453
22. CDC. Fourth National Report on Human Exposure to Environmental Chemicals. Atlanta, GA: Centers for Disease Control and Prevention; 2009.
23. Liu T-K, Liu S-H, Chang C-H, Yang RS. Con-centration of metal elements in the blood and urine in the patients with cementless total knee arthroplasty.Tohoku J Exp Med. 1998;185(4):253–262
24. Lhotka C, Szekeres T, Steffan I, Zhuber K, Zweymüller K. Four-year study of cobalt and chromium blood levels in patients managed with two different metal-on-metal total hip replacements.J Orthop Res. 2003; 21(2):189–195
25. Public Health Statement: Aluminum. Atlanta, GA: Agency for Toxic Substances and Dis-ease Registry; 2006. Available at: www.atsdr.
cdc.gov/toxprofiles/tp22-c1-b.pdf. Accessed September 1, 2011
26. Becaria A, Campbell A, Bondy SC. Aluminum as a toxicant.Toxicol Ind Health. 2002;18(7): 309–320
27. Pennington JA, Schoen SA. Estimates of di-etary exposure to aluminium. Food Addit Contam. 1995;12(1):119–128
28. Toxilogical Profile for Aluminum. Atlanta, GA; Agency for Toxic Substances and Dis-ease; 2008. Available at: www.atsdr.cdc.gov/ toxprofiles/TP.asp?id=191&tid=34. Accessed September 1, 2011
29. Priest ND. The biological behaviour and bioavailability of aluminium in man, with special reference to studies employing aluminium-26 as a tracer: review and study update.J Environ Monit. 2004;6(5):375–403
30. Jouhanneau P, Raisbeck GM, Yiou F, Lacour B, Banide H, Drüeke TB. Gastrointestinal absorption, tissue retention, and urinary excretion of dietary aluminum in rats de-termined by using26Al.Clin Chem. 1997;43(6 pt 1):1023–1028
31. Baylor NW, Egan W, Richman P. Aluminum salts in vaccines—US perspective.Vaccine. 2002;20(suppl 3):S18–S23
32. Offit PA, Jew RK. Addressing parents’ con-cerns: do vaccines contain harmful preser-vatives, adjuvants, additives, or residuals? Pediatrics. 2003;112(6 pt 1):1394–1397
33. Flarend RE, Hem SL, White JL, et al. In vivo absorption of aluminium-containing vaccine
adjuvants using 26Al.Vaccine. 1997;15(12-13):1314–1318
34. Bishop NJ, Morley R, Day JP, Lucas A. Alu-minum neurotoxicity in preterm infants receiving intravenous-feeding solutions. N Engl J Med. 1997;336(22):1557–1561
35. Aluminum toxicity in infants and children. American Academy of Pediatrics, Commit-tee on Nutrition.Pediatrics. 1996;97(3):413– 416
36. Ewers U, Krause C, Schulz C, Wilhelm M. Reference values and human biological monitoring values for environmental toxins. Report on the work and recommendations of the Commission on Human Biological Monitoring of the German Federal Envi-ronmental Agency.Int Arch Occup Environ Health. 1999;72(4):255–260
37. Tietz NW, ed.Clinical Guide to Laboratory Tests. 3rd ed. Philadelphia: W.B. Saunders; 1995.
38. Lauwerys RR, Hoet P. Industrial chemical exposures. In:Guidelines for Biological Mon-itoring. 3rd ed. Boca Raton, FL: CRC Press; 2001
39. Hair toxic element exposure profile. St. Charles, IL: Doctor’s Data, Inc.; 2011. www.doctorsdata. com/repository.asp?id=1271. Accessed June 23, 2011.
40. Seidel S, Kreutzer R, Smith D, McNeel S, Gilliss D. Assessment of commercial labo-ratories performing hair mineral analysis. JAMA. 2001;285(1):67–72
DOI: 10.1542/peds.2010-3481 originally published online December 5, 2011;
2012;129;e142
Pediatrics
Services
Updated Information &
http://pediatrics.aappublications.org/content/129/1/e142 including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/129/1/e142#BIBL This article cites 32 articles, 6 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/toxicology_sub
Toxicology
http://www.aappublications.org/cgi/collection/pharmacology_sub
Pharmacology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
DOI: 10.1542/peds.2010-3481 originally published online December 5, 2011;
2012;129;e142
Pediatrics
Michelle Zeager, Alan D. Woolf and Rose H. Goldman
Wide Variation in Reference Values for Aluminum Levels in Children
http://pediatrics.aappublications.org/content/129/1/e142
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.