EXPERT BRIEFING PAPER 1
Intensive Care/
Case Management
David Challis and Jane Hughes
email:
[email protected]
INTENSIVE CARE/CASE MANAGEMENT
1. Definition
The origins of care or case management lie in the need for coordination of a range of support, provided from a range of sources to achieve a common goal of effective care and support. A definition of intensive care/case management (ICM) can be found in the presence of several features as shown in Figure1. This offers an approach suitable for the community-based care of vulnerable people with chronic conditions. ICM is designed for vulnerable people with complex and fluctuating needs often requiring a multi-service response rather than those with less complex needs which are often met by a single service response provided by one agency.
Figure 1: Features of Intensive Care/Case Management
Source: Challis 2003
Core tasks: case finding and screening; assessment; care planning; monitoring and review
Functions: coordination and linkage of care services
Goals: providing continuity and integrated care; increased opportunity for home-based care; make better use of resources; promote well-being of older person
Small caseloads: to permit attention to fluctuating need and risk; titrating resources to needs
Target population: long-term care needs; multiple service requirements; risk of institutional placement
Differentiating features of long-term care: intensity of involvement; breadth of services spanned; lengthy duration of involvement with older person
Multi-level response: dual function of ICM in coordinating care at user level and generate information to help inform service commissioning to develop more appropriate support
i
2. Target Populations
With its origins in North America the development of case management has been the focus of many policy discussions both in the health and social care sectors internationally over a considerable period of time. Both the terms care management and case management have been regularly used to describe this practice.
A key component of the community care reforms in the 1990s was the introduction of care management arrangements. These had the underlying aims of cost containment and promoting choice. The aim was to shift the delivery and accountability of social care away from institution based services towards care at home. Subsequently a number of initiatives have sought to promote differentiation within care management arrangements. A distinction has been made between a ‘care management approach’ for the majority of cases and ‘intensive care management’ for those cases where needs are more complex and risk greater. Recently with the emphasis on self directed support it is anticipated that different roles will develop to provide differentiated levels of support – care managers, care brokers and care navigators.
In some respects the introduction of the NHS and social care model in England mirrors that of the community care reforms in the 1990s with its origins in a move away from a reliance
on high cost acute services towards treating more patients with enduring long-term health problems in community settings. Long-term conditions (LTC) case management with its focus on patients with multiple complex needs is one of three interventions within the NHS and social care model intended to match to patients with different levels of need; the other two being disease care management for people with a single primary condition and supported self care in which patients are encouraged to manage their own condition.
3. Service Characteristics
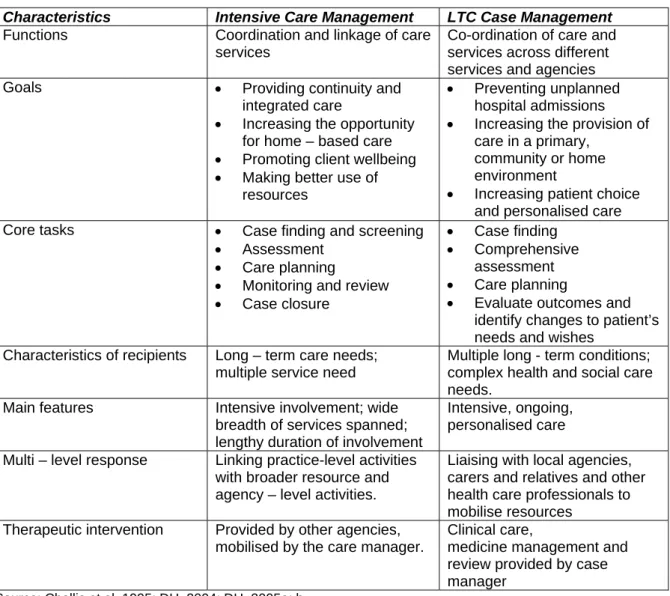
In both approaches the emphasis is on providing a coordinated link between the range of agencies and organisations delivering care and those receiving it in order to minimise the fragmentation of service provision for those with multiple health and social needs. The characteristics of both types of ICM are summarised in Figure 2. There are clear similarities in both approaches; however a distinguishing feature of LTC case management is clinical intervention by a case manger and less emphasis on securing services and review within the context of care planning.
Figure 2: Intensive Care Management and Long Term Conditions Case Management: a comparison
Characteristics Intensive Care Management LTC Case Management
Functions Coordination and linkage of care services
Co-ordination of care and services across different services and agencies Goals Providing continuity and
integrated care
Increasing the opportunity for home – based care
Promoting client wellbeing
Making better use of resources
Preventing unplanned hospital admissions
Increasing the provision of care in a primary,
community or home environment
Increasing patient choice and personalised care Core tasks Case finding and screening
Assessment
Care planning
Monitoring and review
Case closure
Case finding
Comprehensive assessment
Care planning
Evaluate outcomes and identify changes to patient’s needs and wishes
Characteristics of recipients Long – term care needs; multiple service need
Multiple long - term conditions; complex health and social care needs.
Main features Intensive involvement; wide breadth of services spanned; lengthy duration of involvement
Intensive, ongoing, personalised care Multi – level response Linking practice-level activities
with broader resource and agency – level activities.
Liaising with local agencies, carers and relatives and other health care professionals to mobilise resources
Therapeutic intervention Provided by other agencies, mobilised by the care manager.
Clinical care,
medicine management and review provided by case manager
4. Factors Associated with Positive Outcomes
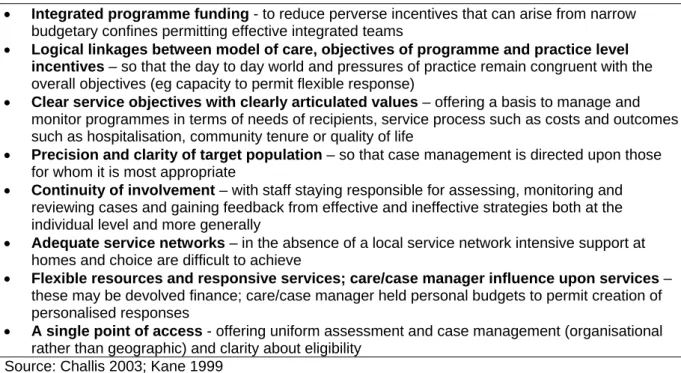
Most studies of ICM have focussed upon populations with high probability of admission or readmission to hospital or long term care settings. It is possible to infer some common elements from the findings as shown in figure 3.
Figure 3: Factors associated with positive outcomes
Integrated programme funding - to reduce perverse incentives that can arise from narrow budgetary confines permitting effective integrated teams
Logical linkages between model of care, objectives of programme and practice level incentives – so that the day to day world and pressures of practice remain congruent with the overall objectives (eg capacity to permit flexible response)
Clear service objectives with clearly articulated values – offering a basis to manage and monitor programmes in terms of needs of recipients, service process such as costs and outcomes such as hospitalisation, community tenure or quality of life
Precision and clarity of target population – so that case management is directed upon those for whom it is most appropriate
Continuity of involvement – with staff staying responsible for assessing, monitoring and reviewing cases and gaining feedback from effective and ineffective strategies both at the individual level and more generally
Adequate service networks – in the absence of a local service network intensive support at homes and choice are difficult to achieve
Flexible resources and responsive services; care/case manager influence upon services – these may be devolved finance; care/case manager held personal budgets to permit creation of personalised responses
A single point of access - offering uniform assessment and case management (organisational rather than geographic) and clarity about eligibility
Source: Challis 2003; Kane 1999
Notwithstanding these findings, it is important to identify the issue of programme fidelity. Case management programmes may develop and change as they are implemented and may thus stray from the combination of factors which contribute to successful outcomes. Managers and commissioners need therefore to view the importance of programme fidelity where the content of the intervention needs to be related to the precise goals it is designed to achieve (Challis, 2003). In the absence of this a variety of forms of case management are likely to continue to develop, not necessarily of proven efficacy.
5. Evidence Base
Findings from intensive care/case management studies have revealed that it is an approach which has a utility in a number of settings. With regard to intensive care management findings are reported from four studies conducted by the Personal Social services Research Unit.
In the social care studies, in Kent and Gateshead, intensive care management reduced the need for care home admissions of vulnerable elderly people to a significant extent. There were also marked improvements in the levels of well-being of elderly people and their carers and these were achieved at no greater cost to the social services, NHS or society as a whole (Challis and Davies, 1986; Challis et al., 2002a)
In Gateshead a pilot health and social care scheme was developed around primary care incorporating inputs from a nurse care manager and part time junior doctor also demonstrated a reduced rate of care home placement (Challis et al., 2002a).
Care managers employed by the local authority were members of a geriatric multidisciplinary team in the Darlington study. Here intensive care management demonstrated improvements in the well-being of elderly people and a lower level of carer stress were observed for those receiving this new service compared with patients in long-stay hospital care. These gains were achieved at a lower cost than was normally expended upon such patients reflecting the higher cost of hospital care compared with other institutional settings (Challis et al., 1995).
Within the Lewisham study a similar approach for older people with a diagnosis of dementia was developed in a community based service for mental health of older people by local authority care managers. Here intensive care management appeared to only have an effect of improving the probability of remaining at home in the second year of support compared with existing services and the costs were higher than for those receiving other for other forms of support. However, there was evidence of improved well being for the older people and more markedly so for the carers receiving the intensive care management support (Challis et al., 2002b, 2009).
With regard to intensive case management for long term conditions, there is less UK evidence for effectiveness, with this being a relatively new development. It would appear that although patient and carer satisfaction may improve, the evidence that case management for patients with complex long-term conditions contributes to outcomes such as reducing hospital admission, length of stay and improving patient well being is equivocal (Hutt et al., 2004; Singh, 2005). Some studies of case management interventions both in the UK and elsewhere have reported significant reductions in emergency admissions, other hospital admissions or bed days (Huws et al., 2008; Bird et al., 2007; Patrick et al., 2006; Lyon et al., 2006; Leung et al., 2004; Landi et al., 1999; Bernabei et al., 1998). However other studies including the major evaluation of the Evercare demonstration in England (Gravelle et al., 2006) and a large randomised control trial of an integrated system which included case management did not demonstrate significant reductions in inpatient care or hospital days (Béland et al., 2006). A review of nurse case management interventions and the importance of case management content can be found in Reilly et al. (2009).
6. Selected References
Béland, F., Bergman, H., Lebel, P. and Clarfield, M. (2006) A system of integrated care for older persons with disabilities in Canada: results from a randomized control trial. The Journals of Gerontology; Series A: Biological Sciences and Medical Sciences 61A, (4), 367-374.
Bernabei, R., Landi, F., Gambassi, G., Sgadari, A., Zuccala, G., Mor, V., Rubenstein, L. and Carbonin, P. (1998) Randomised trial of impact of model of integrated care and case management for older people living in the community. British Medical Journal 316, (7141), 1348-51.
Bird, S., Kurowski, W., Dickman, G. and Kronberg, I. (2007) Integrated care facilitation for older patients with complex needs reduces hospital demand. Australian Health Review 31, (3), 451-461. Challis, D. and Davies, B. (1986) Case-Management in Community Care, Gower, Aldershot Challis, D., Darton, R., Johnson, L., Stone, M. and Traske, K.(1995) Care Management and Health Care of Older People: The Darlington Community Care Project, Ashgate, Aldershot.
Challis, D., Chesterman, J., Luckett, R., Stewart, K. and Chessum, R. (2002a) Case Management in Social and Primary Health Care: The Gateshead Community Care Scheme, Ashgate, Aldershot.
5 Challis, D., von Abendorff, R., Brown, P., Chesterman, J. and Hughes, J. (2002b) Care management, dementia care and specialist mental health services: an evaluation, International Journal of Geriatric Psychiatry, 17, 4, 315-325.
Challis, D., Hughes, J., Sutcliffe, C., Von Abendorff, R., Brown, P., and Chesterman, J., (2009)
Supporting People with Dementia at Home, Ashgate, Aldershot.
Challis, D. (2003) Achieving co-ordinated and integrated care among long term care services: the role of care management, in Brodsky, J., Habib, J. and Hirschfeld, M. (eds) Key PolicyIssues in Long Term Care, World Health Organisation, Geneva.
Department of Health. (2004a) Improving Chronic Disease Management. London: Department of Health.
Department of Health. (2005a) Supporting People with Long term Conditions: Liberating the Talents of Nurses who Care for People with Long term Conditions. London: Department of Health.
Department of Health. (2005b) Supporting People with Long term Conditions: An NHS and Social Care Model to Support Local Innovation and Integration. Leeds: Department of Health.
Gravelle, H., Dusheiko, M., Sheaff, R., Sargent, P., Boaden, R., Pickard, S., Parker, S. and Roland, M. (2006) Impact of case management (Evercare) on outcomes for frail elderly patients: controlled before and after analysis of quantitative outcome data, British Medical Journal, 15 November 2006, dol: 10.1136/bmj.39020.413310.55 (abridged text, in print: BMJ 2007:334:31-4).
Hutt, R., Rosen, R. and McCauley, J. (2004) Case Managing Long- term Conditions: What Impact Does It Have in the Treatment of Older People? London: Kings Fund.
Huws, D., Cashmore, D., Newcombe, R., Roberts, C., Vincent, J. and Elwyn, G. (2008) Impact of case management by advanced practice nurses in primary care on unplanned hospital admissions: a controlled intervention study. BMC Health Services Research 8, (115), doi: 10.1186/1472-6963-8-115. Kane, R. A. (1999) Models of Long Term Care that Work, in Campbell, J.C. and Ikegami, N. (eds)
Long Term Care for Frail Older People, Springer, New York.
Landi, F., Lattanzio, F., Gambassi, G., Zuccala, G., Sgadari, A., Panfilo, M., Ruffilli, M. and Bernabei, R. (1999) A model for integrated home care of frail older patients: the Silver Network project. Aging Clinical and Experimental Research 11, (4), 262-72.
Leung, A.C., Liu, C., Chow, N.W. and Chi, I. (2004) Cost-benefit analysis of a case management project for the community-dwelling frail elderly in Hong Kong. Journal of Applied Gerontology 23, (1), 70-85.
Lyon, D., Miller, J. and Pine, K. (2006) The Castlefields integrated care model: the evidence summarised. Journal of Integrated Care,14, (1), 7-12.
Patrick, H., Roberts, R., Hutt, R., Hewitt, P., Connelly, J. and Oliver, D. (2006)Evaluation of innovations in nursing practice: report and discussion. British Journal of Nursing 15, (9), 520-523. Reilly, S., Hughes, J. and Challis, D. (2009) Case management for long-term conditions:
implementation and processes, Ageing and Society, doi:10.1017/S0144686X09990183
Singh, D. (2005) Which Staff Improve Care for People with Long-Term Conditions? A Rapid Review of the Literature. NHS Modernisation Agency and The University of Birmingham Health Service Management Centre, Birmingham, UK.