Behavior Change Techniques to Create Safe Dates for Teens:
Applying the BCTTv1 to the Safe Dates Curriculum
Carly Bess Cannoy
Health Policy and Management
University of North Carolina at Chapel Hill
Background: Teen dating violence (TDV) is a prevalent, but preventable, public health problem in the United States with severe and long-lasting health effects on victims.* Poor conflict
management skills, acceptance of dating abuse norms, and gender stereotyping behaviors have been identified as contributing to TDV perpetration and victimization. The Behavior Change Technique Taxonomy (BCTTv1) can be used to code health behavior interventions and discover which basic elements of interventions bring about behavior change in participants.
Program Description: The Safe Dates program consists of nine in-person classroom sessions, a play, and poster contest. The program was developed and evaluated in the 1990s in Johnston County, North Carolina. Participants included eighth and ninth grade students. The Safe Dates curriculum approaches all participants, regardless of gender, as potential perpetrators and victims of TDV.
Research Questions: How do mediator variables described in the Safe Datestheoretical model relate to specific activities in the Safe Datescurriculum? How does the Behavior Change
Technique (BCT) Taxonomy (BCTTv1) apply to specific activities in the Safe Datescurriculum? Are there patterns in the application of BCTs to mediator variables and mediator variable
effectiveness?
Methods: This study is a qualitative program evaluation, involving the application of the BCTTv1 to the Safe Dates curriculum and utilizing results from previous evaluations. Findings: BCT use between effective and ineffective mediator variables did not differ on frequency or other quantitative descriptions. However, effective mediator variables were more often targeted in combination and across the curriculum. Additionally, they were more often targeted with BCTs from group five, “natural consequences,” emphasizing the importance of behavior change. Lastly, BCTs 8.1 and 11.4 were used to complement other BCTs related to knowledge with behavior practice of wanted (8.1) and unwanted (11.4) behaviors.
Implications: While the findings of this study are unique to the Safe Dates curriculum, they could be considered in the creation of new TDV prevention programs, updates to the Safe Dates curriculum, or included in later larger studies of BCT use in TDV prevention programming. These findings are an early indication that frequency of BCT use may not be important for effectiveness. However, strategic use of BCTs targeting multiple mediator variables across a curriculum and with reinforcement through both knowledge and behavior practice may be more important for program effectiveness.
Introduction
Teen dating violence (TDV) is a prevalent, but preventable, public health problem
affecting as many as 1 in 9 female teens, 1 in 13 male teens (Kann et al., 2016), and even more
among teens with other gender identities (Dank et al., 2014). The Centers for Disease Control
and Prevention (CDC) defines TDV as physical, sexual, psychological, and/or emotional
aggressions, including stalking, that happen between current or former dating relationship
partners. TDV can occur in-person or through electronic means and is also known as dating
abuse (CDC, 2018).TDV has severe impacts, including increasing risk for suicidal ideation and
later interpersonal violence (IPV) victimization among both male and female victims during
young adulthood (Exner et al., 2013).More generally, IPV is associated with life-long adverse
health outcomes, including, but not limited to, heart disease (Black & Breiding, 2008),
depression, posttraumatic stress disorder (PTSD) (Warsaw et al., 2009), and health risk behaviors
like binge drinking (Exner et al, 2013).
This project will examine how one TDV prevention program, Safe Dates, is effective
through assessing the linkages between mediator variables, activities, and behavior change
techniques (BCTs). Safe Dates is a TDV prevention program for middle and high school
students, consisting of nine in-person sessions, a play, poster contest, and materials for parents
(Foshee et al., 2004). The underlying theoretical model used for Safe Dates utilizes school
activities, particularly the nine in-person sessions, to change mediating variables in TDV.
Mediator variables represent intermediate skills, knowledge, or beliefs which contribute to
behavior change and outcomes of interest. Primary prevention mediator variables include dating
abuse norms, gender stereotypes, and conflict management skills. Secondary prevention
mediator variables include awareness of services and belief in a need for help (Foshee et al.,
stereotypes, and improvement in conflict management skills should lead to primary prevention
and increasing the belief in a need for help should lead to help seeking and secondary prevention
(Foshee et al., 1996). This project will link specific activities in the Safe Dates curriculum to the
primary and secondary prevention mediating variables in the Safe Dates theoretical model
(Foshee et al., 1998).
Challenges arise when communicating the structure and effectiveness of health behavior
interventions, like Safe Dates. To facilitate communication and collaboration, the Behavior
Change Technique Taxonomy (BCTTv1) was developed to classify the “active ingredients that
bring about behavior change” within behavior change interventions (Michie et al., 2013).This
project will apply the BCTTv1 to the Safe Dates curriculum and determine how many and which
Behavior Change Techniques (BCTs) are applied to activities. Early evaluations of Safe Dates
demonstrated positive effects on some mediating variables, including decreasing gender
stereotyping and changing dating abuse norms, along with decreases in violence perpetration.
Mediation analyses were used to suggest that changes in mediator variables, particularly gender
stereotyping and dating abuse norms, led to the decrease in perpetration. However, positive
effects were not shown for all mediator variables identified in the Safe Dates theoretical model
(Foshee et al., 1998).
The linking of mediator variables from the theoretical model to activities in the
curriculum, followed by the application of the BCTTv1 to those activities, provides an
opportunity to compare the use of BCTs within the Safe Dates curriculum. This project will
explore all mediator variables identified in the Safe Dates theoretical model, determining if
different patterns exist between BCTs used for mediator variables with demonstrated positive
accounted for an effective TDV prevention program, Safe Dates, through the application of the
BCTTv1, which could facilitate communication with other health behavior intervention
programs. A potential follow-up project is the exploration of how other effective TDV
prevention programs, such as Real Consentor It’s Your Game, Keep it Real, utilize BCTs.
Through the application of the BCTTv1 to these programs, as well as Safe Dates, comparisons
and contrasts between use of BCTs and program effectiveness could provide insights on best
practices.
Research Questions
1. How do mediator variables described in the Safe Datestheoretical model relate to
specific activities in the Safe Datescurriculum?
2. How does the Behavior Change Technique (BCT) Taxonomy (BCTTv1) apply to specific
activities in the Safe Datescurriculum?
3. Do, and if so how, patterns in the application of BCTs to mediator variables differ
between effective and ineffective variables?
Literature Review
This literature review begins by describing teen dating violence (TDV) and TDV
prevention programs. Then, the role of gender stereotypes, dating abuse norms, and conflict
management in TDV will be described. The challenges of reporting health behavior
interventions, like Safe Dates, will also be addressed before the review ends with a description of
the Behavior Change Technique Taxonomy’s (BCTTv1) development and previous applications
to interventions similar to Safe Dates.
The Centers for Disease Control and Prevention (CDC) defines teen dating violence
(TDV) as a form of intimate partner violence (IPV), between teens in close relationships. TDV
can include physical and sexual violence, stalking, and psychological aggressions, both in person
or electronically (Breiding et al., 2015). Actions like sexting without consent or posting private
sexual pictures on social media, while often not thought of as TDV, are in fact forms of
non-physical violence and may develop into other forms of violence (“Preventing Teen Dating
Violence,” 2017).
TDV is prevalent; the 2015 Youth Risk Behavior Survey found a 9.6% prevalence of
physical dating violence victimization among students, with over 1 in 9 female and 1 in 13 male
students reporting victimization. Further, a 10.6% prevalence of sexual violence victimization
among students was found, with over 1 in 7 female and 1 in 19 male students reporting
victimization (CDC, 2016). Similar physical and sexual dating violence prevalence measures
were found in 2013, 10.3% for physical and 10.4% for sexual dating violence (CDC, 2014).
From 1999 to 2011 the YRBS included only a generalized dating violence question, combining
both physical and sexual violence, but showed stable prevalence of dating violence, between 8.8
and 9.4% among both male and female students (CDC, 2012).
TDV has severe and life-long effects; multiple longitudinal studies have found a
wide-range of negative health outcomes for those victimized by TDV. For example, there is evidence
that psychological TDV increases alcohol use and marijuana use among females, while physical
TDV increases cigarette use (Foshee et al., 2013) and revictimization during the first year of
college(Smith et al., 2003). Other studies have found victimization increases depression among
both female and male victims while increasing other high-risk behaviors, such as antisocial and
have found an increase in antisocial and suicidal behavior among male victims, as well as female
victims (Exner-Cortens et al., 2013). Regardless of these discrepancies in longitudinal studies,
there is clear evidence through cross-sectional studies that exposure to intimate partner violence
(IPV), including TDV, is associated with negative health outcomes, even though causality cannot
be determined. For example, the Behavioral Risk Factor Surveillance System (BRFSS) in 2005,
found that female victims of IPV were 1.7 times as likely to have arthritis and heart disease
compared to females not victimized, 1.8 times for stroke, and 1.5 times for use of disability
equipment. Male victims were found to have increased odds as well, but to a lesser extent than
female victims. These findings support a general link between IPV and negative health
outcomes, from chronic diseases to gastrointestinal disorders (CDC, 2008).
TDV Prevention Programs
Due to the prevalence of TDV and severity of TDV’s long-term effects, numerous
prevention programs have been developed to prevent TDV. A 2014 review of IPV and sexual
violence (SV) prevention programs for adolescents around the world identified 61 interventions
which varied in approach, rigor of evaluation, and effectiveness. The most common approach
was school-based programs, with 31 in total (though 10 were based in universities), with
community-based programs the next most common (16 interventions). Only five programs
(including Safe Dates) were evaluated in a rigorous manner, defined as a randomized control
trial. The review found that school-based and community-based interventions were most
effective and many included an emphasis on increasing gender-equitable norms, similar to Safe
Dates (Lundgren & Amin, 2015). An earlier review of primary and secondary TDV prevention
programs found a similar emphasis on gender-equitable norms (Cornelius & Resseguie, 2007) as
evaluation, programs often included an element to promote gender equity, conflict management,
and awareness of resources for victims (though not perpetrators). The evaluation data that were
available indicated promise for the development of effective TDV prevention programs
(Cornelius & Resseguie, 2007).
Conflict Management Skills and Violence Prevention
Scholars have hypothesized that conflict management skills are more important within TDV
prevention than larger IPV prevention due to less developed interpersonal skills among
adolescents. Poor conflict management skills are known to relate to victimization for female
teens and conflict management skill building has been suggested as important to include in TDV
prevention programs (Bonache et al., 2017). Additionally, poor conflict management skills are a
known risk factor for TDV perpetuation (Cohen et al., 2018). TDV prevention programs often
incorporate conflict management skill building; one literature review found that many programs
incorporated conflict management and resolution into their theoretical models and curriculums
(Cornelius & Resseguie, 2007). In reviews of TDV prevention programs, conflict management
skill building (also commonly identified as nonviolent conflict resolution) is consistently
presented as part of generally effective programs. However, specific information on the
effectiveness of conflict management, within programs, is not usually identified (Lundgren &
Amin, 2015; Hickman et al., 2004).
Dating Violence Norms
Gender inequitable norms as well as TDV norms are commonly included in TDV prevention
programs. Gender inequitable norms will be further addressed in the next session of this
literature review. While commonly present together in prevention programs, TDV norms are
by gender inequitable norms (Lundgren & Amin, 2015; Storer et al., 2016). For example,
Coaching Boys into Men is effective in changing participants’ acceptance of TDV: participants
were less likely to perpetuate TDV and to accept their peers’ TDV (through either ignoring or
encouraging behavior). However, participants were not less likely to accept gender inequitable
norms. Therefore, while TDV norms and acceptability of TDV were affected by this prevention
program, gender equity was not (Miller et al., 2013). It is important for prevention programs to
include both TDV norms and gender stereotyping elements, to address the related, but distinct,
social norms around TDV and gender equity.
Gender, Stereotypes, and Violence
Gender stereotyping is a specific behavior that can be targeted in TDV prevention
programs, acting as an individual and relationship-level proxy for larger systems of gender
norms in communities and society. While feminist scholars disagree on the validity of framing
violence, specifically against women, as a result of a patriarchy, there is agreement that a
hierarchal system of gendered power is inherently related to IPV, including TDV (Hunnicutt,
2009). The inherent link between gender and violence is posited to be due to gender norms, the
expectations for expressing stereotypical femininity and masculinity at a societal level and
subsequent gender stereotyping that occurs at an individual and interpersonal level (Barker et al.,
2010). Gender stereotyping, within heterosexual relationships, can be as simple as a belief that
young women are trying to manipulate their partners or that young men want sex more than their
partners. These behaviors have been known to be associated with TDV and that association was
quantified nearly two decades ago (Foshee et al., 2001).
As gender norms and gender stereotyping are linked to violence, they are becoming
review of 58 health promotion programs (including violence prevention programs) for men and
boys found that those addressing gender norms and stereotypes were more effective than those
which took a gender-neutral approach (Barker et al., 2010). For TDV, pressure to conform to
gender stereotypes, and their related gender inequities, are directly related to both perpetuation
and victimization (Adelman & Sang Hea Kil, 2007). However, related to feminist reluctance to
apply a patriarchal framework to violence, the associations between gender stereotypes and
perpetuation and victimization should not be interpreted as meaning only men can perpetrate
violence and only women can be victimized by violence. Instead, the relationship between gender and violence is much more complex and related to female perpetuation, male
victimization, and the experiences of gender non-binary folks (Hunnicutt, 2009). Even so,
scholars have cautioned against distancing violence prevention from issues of gender inequity
(Reed et al., 2010). It is within this nuanced context that gender stereotyping components are
included in violence prevention programs, such as Safe Dates.
Health Behaviors and Reporting Guidelines
Interventions, such as Safe Dates, attempt to change complex health beliefs and
behaviors, like gender stereotyping. The communication of how these interventions are effective
and what components contribute to that effectiveness is challenging. To establish general
reporting guidelines for randomized controlled trials, the Consolidated Standards of Reporting
Trials (CONSORT) statement was developed in the 1990s (Moher et al., 2001). Behavioral
health specialists quickly recognized the need for additional guidelines to communicate the
effectiveness and structure of behavioral interventions. Additions to the CONSORT statement
were proposed in 2003 (Davidson et al., 2003) and an extension of the CONSORT statement was
CONSORT checklist and expansion of 11 other items on the checklist to provide more relevant
information for behavioral (and other nonpharmalogic) interventions (Boutron et al., 2008). Yet,
this extension only called for the description of components of behavioral interventions and their
delivery. It provided no specific guidance on how to describe components(Michie et al., 2013).
The lack of specific guidance on how to describe components of behavioral interventions
caused significant problems for intervention replication, reporting, and systematic reviewing.
Because of the absence of detailed information on components, researchers and implementers of
interventions often felt uncertainty and confusion in their attempts to replicate programs.
Additionally, systematic reviewers were unable to compare interventions without creating their
own system for classification of components. For these reasons, a taxonomy to be used across
behavioral change interventions became necessary and was developed (Michie et al., 2013).
BCTTv1 and Relevant Previous Applications
Due to the challenges described above, a taxonomy was developed to describe the
specific components of behavioral interventions. This taxonomy’s current form, the Behavior
Change Technique (BCT) Taxonomy (BCTTv1), includes 93 BCTs hierarchically organized into
16 groups. BCTs are informally defined as the “active ingredients” of behavioral interventions;
they are formally defined as “observable, replicable, and irreducible components of an
intervention designed to alter or redirect causal processes that regulate behavior.” For example,
one grouping within the BCTTv1 is “goals and planning” and there are nine BCTs within the
group. These BCTs range from goal setting focused on a specific behavior to behavioral
contracts (e.g., signing a contract with another person to adhere to the goal set of eating a fruit
and vegetable every day). The creators of BCTTv1 identified five potential benefits from the
the CONSORT statement and included improved opportunity for accurate replication and
implementation of interventions, more accurate systematic reviews of interventions, and the
opportunity for possible linkage of BCTs and theories of behavior change (Michie et al., 2013).
The BCTTv1 has been applied to over 400 behavioral intervention programs, including
interventions targeting adolescent sexual health. The BCTTv1 was retroactively applied to a
school-based program to promote sexual wellness through condom use(Hill & Abraham, 2008),
a community-based sexual health program in southern rural communities focused on delaying
sexual activity (Murry et al., 2011), and a film-based program designed for adolescent males to
prevent unintended pregnancies (Aventin et al., 2015). These programs were retroactively coded
with the BCTTv1 as part of the Theories and Techniques of Behavior Change Project (Michie &
Johnston, 2012). The application of the BCTTv1 allowed for the identification of BCTs used in
the programs and thus to how the program achieved their intervention effect. Similar to the
previous applications, this project will retroactively apply the BCTTv1 to an adolescent health
intervention, Safe Dates.
Program Description
The Safe Dates Project involved the development and evaluation of Safe Dates to
establish evidence for the effectiveness of a TDV prevention program, which was lacking in the
1990s. Safe Dates, acknowledging that both males and females perpetuate and are victimized by
TDV, approaches all participants as potential perpetuators as well as potential victims. The
curriculum has both primary and secondary prevention goals, achieved through a school
intervention of nine classroom sessions, a play, and a poster contest along with community
interventions including parent materials. Primary prevention was expected to occur through
management skills. Through changing of norms related to dating abuse and gender role
expectations related to gender stereotyping, a decrease in TDV was expected. The theoretical
basis for secondary prevention, precaution adoption theory, emphasized the need for victims to
believe they need help as well as believe that an action will actually provide help. Belief in a
need for help was expected to be influenced by stereotypes of abusive relationships and causes of
violence, so Safe Dates targeted abuse stereotypes, labeling of abuse, and causes of violence
along with addressing perceptions of seriousness of and susceptibility to TDV to increase
participant beliefs in a need for help. Further, increasing awareness of resources and the
expectation that resources will be helpful were expected to create secondary prevention through
increasing both the belief in needing help and help-seeking behaviors (Foshee, 1996).
The initial evaluation of Safe Datestook place in Johnston County, North Carolina,
among 14 schools and included 1,171 students in the eighth and ninth grades. Safe Dates was
implemented in the 1994-1995 school year, with initial follow-up in the spring of 1995 and
another follow-up in the spring of 1996. A matched-pairs, at the school level, randomized control
design was used in the study with each pair randomized to treatment (Safe Dates and community
intervention) or to control (community intervention only). Results of the evaluation generally
appeared promising. Specifically, schools receiving the treatment reported significantly less
average psychological abuse, sexual violence, and violence against current participants than
control schools. Primary prevention was demonstrated with less psychological abuse being
initiated during the study period among those exposed to the school interventions than those not.
Secondary prevention was also demonstrated through increased awareness of resources among
the treatment schools compared to the control schools. Mediation analyses were completed to
participant behavior. The analyses showed that changing norms related to dating violence,
decreasing gender stereotyping, and increasing awareness of services were likely the mediating
variables contributing most to changes in participant behavior (Foshee et al., 1998).
Subsequent evaluations of Safe Dates demonstrated effectiveness in TDV prevention and
changing some mediator variables. The one-year follow-up found that the behavior changes
effects shown in the one-month follow-up were no longer present. However, the changes in
cognitive mediating variables continued, particularly among participants who had experienced
TDV before the initial program(Foshee et al., 2000). Due to the lack of behavioral change at the
one-year follow-up, a Safe Dates booster (newsletter and phone call from health educator) was
developed and implemented among 135 participants from the original treatment group. Four
years after the original implementation, Safe Dates participants reported less physical and sexual
dating violence perpetration and victimization with equal effectiveness for male and female
participants. However, the booster was not shown to be effective (Foshee et al., 2004). Lastly,
another evaluation of data from Safe Dates participants collected 1 month, 1, 2, 3, and 4 years
after implementation showed significant effects on mediating variables of dating violence norms
and gender-role norms. Dating violence prevention was demonstrated through significantly less
moderate physical dating violence victimization among Safe Dates participants and some
reduction in sexual violence victimization among Safe Dates participants (Foshee et al., 2005).
Methods
This study is a qualitative program evaluation of Safe Dates. The BCTTv1 will be
applied to the Safe Dates curriculum and theoretical exercises completed to understand how
elements of the Safe Dates theoretical model relate to program activities, mediator variable
effectiveness, and BCT use.
The Safe Dates curriculum is the primary data source and activities within the curriculum
will be coded with the BCTTv1 to produce data for this project. Additionally, the theoretical
model for Safe Dates (Figure 1 in Foshee et al., 1998) will be used to tie activities, BCTs, and
mediator variables. Secondary data analysis, related to the effectiveness of various mediator
variables, will use data from the original evaluation of Safe Dates (Foshee et al., 1998).
Analysis Methods
BCTTv1 training
The researcher will complete the BCTTv1 training online before coding the Safe Dates
curriculum. Online training consists of six multi-part educational sessions and two assessments.
Coders trained to use the BCTTv1 have been found to have competence and reliability in
accurately applying the BCTTv1 (Abraham et al., 2015; Wood et al., 2015).
Linking mediating factors to specific activities
The theoretical model for Safe Dates is shown below (Foshee et al., 1998). The Safe
Dates program is assumed to work through mediator variables, such as gender stereotyping, to
achieve both primary and secondary prevention. There is evidence of differing effectiveness
between mediator variables and the effectiveness of mediator variables will be determined with
data from the original evaluation of Safe Dates from Foshee et al. (1998). Mediator variables
found to have significant effects in the treatment group at follow-up will be considered
“effective” for this project (the results from Foshee et al., 1998, are included as Appendix A).
For the gender stereotyping and belief in need for help mediating variables, impact was
determined by the researcher at the variable level (i.e. gender stereotyping, belief in need for
help). For the norms and conflict management skills, however, impact was not determined at the
variable level but at more nuanced sub-levels. Norms consists of four sub-levels, including
management skills consists of constructive communication, destructive communication,
constructive anger response, and destructive anger response. For the purpose of this project, if at
least three of four sub-levels of the dating abuse norms or conflict management skills mediator
variables are found to have significant effects, then the entire mediator variable will be
considered “effective.” Therefore, it is necessary to know which parts of the curriculum target
which mediator variables. To tie activities and mediator variables, both activity description, from
the Safe Dates curriculum, and content will be considered. Notably, some activities may target
multiple mediator variables and this will be indicated in the results, along with activity names
and BCTs used.
Safe Dates Theoretical Model (Foshee et al., 1998)
Applying BCTTv1 to specific activities
The BCTTv1 provides detailed definitions for 93 BCTs, organized into 16 groups
(Michie et al., 2013). The developers of the BCTTv1, and the BCTTv1 training program, also
developed an app which contains definitions and examples for all 93 BCTs. To code the Safe
Dates curriculum with the BCTTv1, all activities, directions, and suggested questions will be
read and relevant BCTs, both groupings and individual BCTs, recorded. Additionally, a coding
findings section and Appendix B (Michie et al., 2013). The frequency of BCT groupings in the
Safe Dates curriculum will be reported as well as the frequency of most of the BCTs used (other
BCTs are included in the Appendix B). Tables will be used to organize not only activities,
targeted mediator variables, and present BCTs but also report, for each mediator variable, the
most common individual BCTs, BCT groups, and proportion of activities including at least one
BCT. The table will include all activities which might target a mediator variable, even if the
variable is not the primary target of the activity. For example, if an activity targets both dating
abuse norms and conflict management skills, the BCTs used will be recorded for both mediator
variables. Additionally, when creating proportions of activities including at least one BCT, all
activities targeting the mediator variable will be considered. This is important as activities with
the mediator variable as a secondary target are likely still influencing participants.
Patterns among effective and ineffective mediator variables
The final step of this analysis will involve linking BCT use and mediator variable
effectiveness, to identify overarching patterns. To identify patterns between the effective and
ineffective mediator variables and BCT use, a synthesis table, based on a synthesis table used in
a systematic review of BCTs in sexual health interventions, will be used (De Vasconcelos et al.,
2018). This synthesis will include measures for the variety of BCTs used in activities targeting
mediator variables, by including a count of unique BCTs used in all activities targeting a given
mediator variable. The range of BCT use in activities will also be included, that is a measure of
the least number of BCTs used in an activity to the highest number of BCTs used in an activity
targeting a given mediator variable. Additionally, a short (up to three) list of the BCTs most
frequently used for each mediator variable will be included. Lastly, a measure of the frequency
of BCTs per activity for a given mediator variable will be included. This measure will only
due to the extent of activities targeting multiple mediator variables—to the point of every
mediator having nearly the same frequency when many activities are included in the calculations
for multiple variables. From the synthesis table, patterns in the use of BCTs among both the
effective and ineffective mediator variables will be induced. To supplement the information in
the synthesis table, more detailed information about the targeting of mediator variables across the
curriculum and more details of BCT use in each activity may be taken from Findings’ Table 1.
Findings
Connecting Activities, Mediator Variables, and BCTs
Connecting Activities and Mediator Variables
Using the descriptions of mediator variables from Foshee et al. (1996) and the instructor
directions as well as script to be read to participants, mediator variables addressed by each
activity were determined. Activities which addressed standards for acceptable behavior, usually
directly in dating relationships, were recorded as relating to the dating abuse norm mediator
variable. Activities which addressed gender stereotyping, through educating participants on
stereotypes and how to identify them in their behavior, were recorded as relating the gender
stereotyping mediator variable. Activities which addressed conflict management skills, including
participants exploring their past anger responses, were connected with the conflict management
skills mediator variable. Lastly, activities which related to educating participants about support
resources, emphasized the impact these resources could have, or provided participants with
practice and skills to communicate about resources were recorded as addressing belief in the
need for help mediator variable.
Some activities addressed multiple mediators, shown in Table 1. The bolded “X”
norms mediator variable was addressed in the most activities; about half of the activities
addressed another mediator variable as primary target but also included elements of dating abuse
norms. For example, in Session 5, the activity “Michele’s Story” tells the story of Michele who
is in a relationship with Greg. Greg becomes jealous when Michele talks to other boys, yells at
her, and has even hit her once. But Michele describes that he also write her love letters and can
be insecure and vulnerable. The activity asks participants to identify what “red flags” they see as
Michele’s friend and then practice responding to the situation. Primarily, this activity is
reinforcing for participants that they can identify when friends need help and that they can
effectively help them, so the primary mediator variable recorded was a belief in the need for
help. However, this activity also addresses dating abuse norms by providing specific examples of
what is not acceptable in a relationship - emotional and physical violence along with some
manipulation - and stresses to participants they can identify this elements, so dating abuse norms
were also recorded as being addressed as a secondary target.
Connecting Activities and BCTs
The BCTTv1 was used to identify BCTs in the Safe Dates curriculum. Most activities did
include at least one BCT, specifically 30 of 41 activities. Ten of the activities included more than
one BCT, with only two activities including three BCTs and a single activity including four
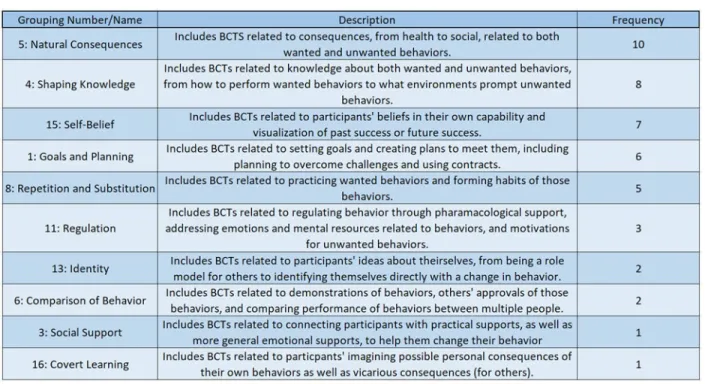
BCTs. BCT groupings from the BCTTv1 and identified within the Safe Dates curriculum are
shown in Table 2. The most commonly used groupings of BCTs included group five, “natural
consequences,” and group four, “shaping knowledge,” with ten and eight BCTs used from each
group respectively. Group five BCTs were largely coded in activities which emphasized the
coded in activities addressing conflict management skills, by providing participants with
instructions on how to handle their anger and conflict. Additionally, group four BCTs were
coded in activities which helped participants recognize situations that triggered their or others’
anger responses.
Table 2: BCT Grouping Descriptions and Frequency
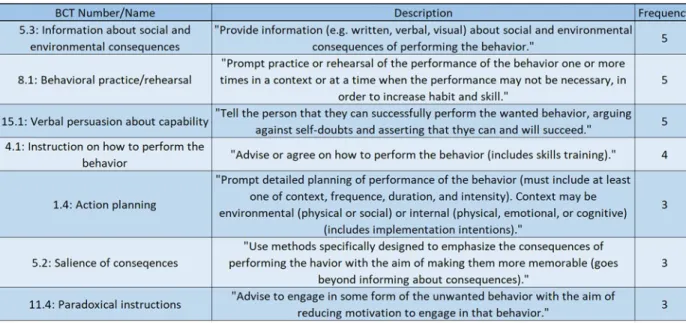
The most commonly used individual BCTs included 5.3, “information about social and
environmental consequences;” 8.1, “behavioral practice;” and 15.1, “verbal persuasion about
capability” (Table 3). BCT 5.3 was coded in activities which emphasized the consequences that
dating abuse and genders stereotyping behaviors can have on participants and their relationships.
BCT 8.1 was used in activities addressing conflict management skills and a belief in the need for
help; specifically, BCT 8.1 was coded in activities which allowed participants to practice their
conflict management skills and talking to both partners in unhealthy or abusive relationships
about resources available to them. BCT 15.1 was coded in the conclusions of multiple sessions
and adopt behavior changes. For example, in Session 8, the conclusion includes (emphasis
added):
“Anger is controllable. You can choose the actions you take when you’re angry. You can teach yourself to do things that reduce your anger without hurting others. Controlling your anger is easier when you recognize what makes you angry, when you can identify
your own physical and psychological cues to anger, and when you have a plan to deal
with anger.”
Table 3: BCT Description and Frequency
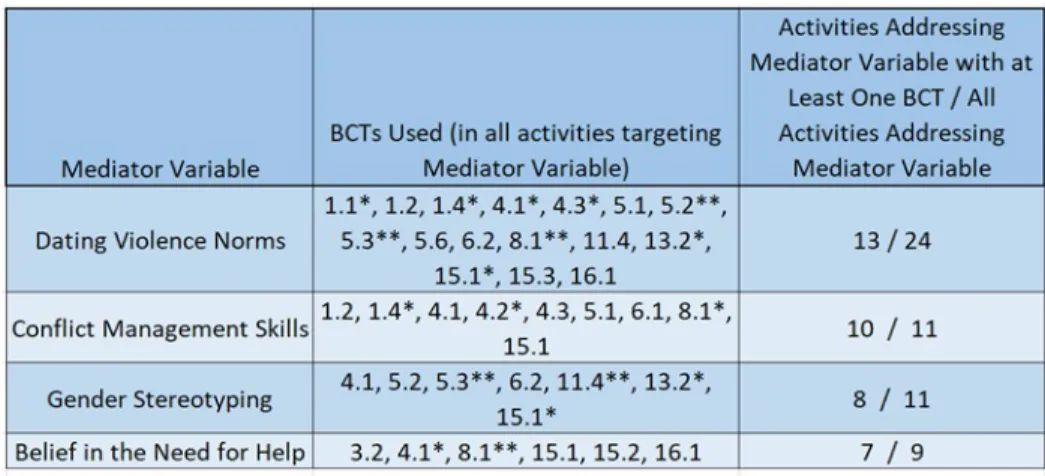
Linking Activities, BCTs, and Mediator Variables
BCTs used in activities targeting each mediator variable is shown in Table 5 below.
Additionally, the table shows how many activities targeted each mediator variable.
Dating Violence Norms
This mediator variable was the most commonly addressed in the activities, being targeted
in 24 out of 41 activities. Over the 24 activities, 13 included at least one BCT. The most common
and group one, “goals and planning.” Outside of those two groupings of BCTs, BCT 8.1,
“behavioral practice” was used three times to address dating violence norms.
Conflict Management Skills
This mediator variable was addressed in 11 activities, with all but one activity including
at least one BCT. The most common grouping of BCTs used to address conflict management
skills was group four, “shaping knowledge.” Specifically, activities included BCTs that
instructed participants how to perform behaviors (like anger management) and prompted
participants to consider what situations and emotions predicted anger responses for them.
Gender Stereotyping
Gender stereotyping was addressed in the same number of activities as conflict
management skills (11). However, only eight of the eleven activities included at least one BCT.
The most commonly used BCT grouping was group five, “natural consequences,” which was
also one of the commonly used groupings in activities addressing dating violence norms. The
two most common BCTs were 5.3, “information about social and environmental consequences,”
and 11.4, “paradoxical instructions.” BCT 5.3 was coded for activities which emphasized the
impact gender stereotyping can have both participants and their relationships. BCT 11.4 was
coded for multiple activities which instructed participants to exaggerate their gender stereotyping
behaviors.
Belief in the Need for Help
This mediator variable was addressed in the least number of activities, nine, but most of
those activities did include at least one BCT. There was a relatively, large amount of variation in
the BCTs present in the activities. Only two BCTs were present from the same grouping, group
to perform the behavior,” were the only BCTs coded more than once in the activities addressing
a belief in the need for help.
Table 5: Mediator Variables, BCTs, and Activities
Differences in BCTs between Effective and Ineffective Mediators
The effectiveness of mediator variables was determined by using evaluation data from
Foshee et al. (1998). Specifically, gender stereotyping and a belief in the need for help both were
found to have significant effects in the treatment group at follow-up. Data were not reported at
the variable level for dating abuse norms but all sub-levels of dating abuse norms (prescribed and
proscribed norms, positive and negative consequences) were found to have significant effects in
the treatment group at follow-up. Conflict management skills was also reported with sub-levels,
but only two of the four sub-levels were found to have significant effects at follow-up.
Therefore, conflict management skills was not considered to be effective.
The first measure in Table 6, number of BCTs identified, identifies variation in BCT use
within activities addressing a given mediator variable. For example, among the activities
addressing dating abuse norms, 16 different BCTs were used. For conflict management skills, the
ineffective mediator variable, 9 different BCTs were used. While fewer BCTs were used to target
management skills than the other two effective mediator variables, gender stereotyping and the
belief in a need for help. The frequency of BCT use in each activity, measured by the average
number of BCTs in the activities with a given mediator variable as the primary target, shows a
similar trend as BCT variation. The ineffective mediator variable, conflict management skills,
has a slightly higher frequency of BCTs than two of the effective mediator variables but less than
the other. With all the average number of BCTs between 1.1 and 1.3, all mediator variables are
relatively close together in this measurement.
All the mediator variables were addressed by activities with a similar range in low to high
BCT frequency. Specifically, all the mediator variables were targeted by some activities without
any BCTs and therefore had the same low BCT frequency of zero
. Some differences do appear between the most frequently used BCTs among the
effective and ineffective mediator variables. Two of the effective mediator variables shared use
of group five, “natural consequences,” BCTs. However, two of the effective mediator variables
and the ineffective variable also share use of BCT 8.1, “behavioral practice.”
Table 6: BCTs, Frequency, and Effectiveness
Discussion
The Safe Dates curriculum effectively changes behaviors and knowledge related to three
mediator variables in the theoretical model: dating abuse norms, gender stereotyping, and a
belief in the need for help. However, Safe Dates has less effectively changed behaviors among
model (Foshee et al., 1998). The BCTTv1 can help researchers understand how Safe Dates targets mediator variables, both effectively and ineffectively, to change participant behavior. The
application of the BCTTv1 to the Safe Dates curriculum, and comparing BCT use in effective
and ineffective mediator variables, provided the basis for three findings in BCT use and
effectiveness within Safe Dates. First, frequency of BCT use does not relate to mediator variable
effectiveness. Second, connectedness between mediator variables, activities, and BCTs is related
to effectiveness. Connectedness, within this study, is related to how some activities, and the
BCTs used within them, targeted multiple mediator variables. Additionally, connectedness is
related to how some mediator variables were targeted across the curriculum, instead of in a few
isolated sessions and activities. Third, the combination of using BCTs related to knowledge
followed by BCTs related to behavior practice was associated with effectiveness.
The application of the BCTTv1 to the Safe Dates curriculum did not demonstrate that
higher frequency of BCTs was associated with mediator variable effectiveness. Activities
primarily targeting the ineffective mediator variable (conflict management skills) generally had
the same number of BCTs as the activities primarily targeting the effective mediator variables
(see “BCT Frequency per Activity” in Table 6). Additionally, the ineffective mediator variable’s
variation in BCT use was within the range of variations for the three effective mediator variables
(see “Number of BCTs Identified” in Table 6). While the frequency and variation of BCT use
did not differ between effective and ineffective mediator variables, there were other differences
in BCT use.
Effective mediator variables shared many sessions, activities, and BCTs, while the
ineffective mediator variable, conflict management skills, was more isolated in the curriculum.
these activities targeted another mediator variable (dating abuse norms in all three).
Consequently, two sessions and eleven activities of Safe Dates targeted conflict management
skills, without much inclusion of other mediator variables while outside of those two sessions,
conflict management skills were not targeted. Among effective mediator variables, dating abuse
norms were targeted in all nine sessions while gender stereotyping and a belief in the need for
help were both targeted in three sessions. Further, the activities targeting the effective mediator
variables often targeted another mediator variable; specifically, eight of the eleven activities
targeting gender stereotyping targeted dating abuse norms and five of the nine activities targeting
a belief in the need for help targeted dating abuse norms as well.
A contrast of two activities, “Stereotyping Leads to Abuse” and “Defusing Anger,”
illustrates the difference between the effective and ineffective mediator variables. Specifically,
the contrast highlights how multiple variables are targeted together in activities and with BCTs
for the effective variables. “Stereotyping Leads to Abuse,” in session 6, targeted two effective
mediator variables, gender stereotyping and dating abuse norms. The activity consisted of two
scenarios explicitly tying gender stereotyping behaviors to dating abuse and exploring the role
that norms play by including bystanders who do not intervene. BCTs 5.2, “salience of
consequences,” and 5.3, “information about social and environmental consequences,” are used to
highlight the consequences of gender stereotyping behavior (i.e. dating abuse) and the
importance of changing that behavior. Additionally, the activity is preceded by two and followed
by another activity which targets gender stereotyping with BCTs related practice of behaviors
(specifically BCT 11.4 and exaggeration of unwanted behaviors).
In contrast, “Defusing Anger,” in session 7, is one of the few activities which targeted
variables, BCTs 1.4, “action planning,” and 4.3, “re-attribution” were used. First, dating abuse
norms are targeted by re-attributing violence from uncontrollable anger to mishandling of anger
(BCT 4.3): “Many teenagers who have been abusive to their dating partner claim that they were so angry, it was uncontrollable…Anger, however, is never uncontrollable.” Participants are then asked to think about what they could do when they realize they are or are becoming angry and
before they become violent (BCT 1.4). In contrast to effective mediator variables, BCTs
regarding knowledge were not reinforced elsewhere in the curriculum through behavior practice,
connected to other mediator variables, or had an emphasis on consequences and importance of
behavior change.
Conflict management skills was largely targeted by BCT group four, “shaping
knowledge,” with little behavior practice or emphasis on consequences of behavior. Specifically,
behavior practice (BCT 8.1) was coded only twice (“Role-Playing Communication Skills,”
Session 8: “Conclusion”). Notably, one of the activities only prompted behavior practice after
the session but did not ensure the practice was completed. With a single use of a group five BCT,
“natural consequences,” participants may have not understood the importance of changing
conflict management behaviors. In contrast, all the effective mediator variables were targeted in
at least three activities with behavior practice BCTs. Dating abuse norms and a belief in the need
for help were targeted with BCT 8.1, “behavior practice/rehearsal,” while gender stereotyping
was targeted with BCT 11.4, “paradoxical instructions.” Behavior practice related to providing
help to friends could increase participant self-efficacy and lead to changes in a belief for help as
well as actual help-seeking. Similarly, paradoxical instructions to perform gender stereotyping
appear particular useful in helping participants identify behaviors they may not perceive
increased with the use of activities targeting multiple mediator variables across the curriculum,
along with a combination of BCTs related to knowledge preceded or followed by BCTs related
to behavior practice.
Comparing the results of this study to other literature regarding BCTs in health behavior
interventions is challenging. The primary challenge is the lack of literature regarding BCT use in
TDV prevention programs. However, there has been widespread application of the BCTTv1 to
physical activity and sedentary behaviors interventions targeting adolescents. Two systematic
reviews of interventions have utilized the BCTTv1 to understand the role of BCTs in program
effectiveness. Both reviews drew conclusions affirming the positive relationship between
quantity of BCTs and program effectiveness, in contrast to this study’s conclusion that quantity
of BCTs within Safe Dates did not show a pattern between effective and ineffective mediator
variables. Notably, one review did use “quality” ratings as a proxy for effectiveness, considering
elements such as app “aesthetic” as well as the evidence base for their intervention (Schoeppe et
al., 2017). Regarding specific the use of BCTs, BCT 5.3 (“information about social and
environmental consequences”) was found in all effective interventions in one systematic review
(Hynynen et al., 2016). BCT 5.3 was identified five times within Safe Dates and only in
activities targeting effective mediator variables. The efficacy of BCT 5.3, particularly in
interventions targeting adolescents, might be a useful research topic in the future.
This study had a few limitations. The study had only one coder due to resource
constraints. However, the coder did complete the BCTTv1 training and coders trained have been
found to have competence and reliability in accurately applying the BCTTv1 (Abraham et al.,
2015; Wood et al., 2015). Additionally, the researcher retroactively coded the Safe Dates
certain activities or sessions; but, retroactive coding is common among applications of the
BCTTv1. The results are specific to the Safe Dates curriculum and should not be applied to other
TDV prevention curriculums without a careful application of the BCTTv1 and study of
theoretical models and effectiveness from previous evaluations. However, with the careful study
of other TDV prevention curriculums and application of the BCTTv1, best practices for
curriculums could be found.
The application of the BCTTv1 to the Safe Dates curriculum provided three overarching
findings related to BCT use. First, frequency of BCT use is not related to mediator variable
effectiveness. However, connectedness between mediator variables, activities, and BCTs is
related to effectiveness along with the combination of using BCTs related to knowledge followed
by BCTs related to behavior practice. A continuation of this research, with other TDV prevention
programs, could lead to the identification of best practices for BCT use within TDV prevention
and improve TDV prevention programming. While programs are often known to be effective in
changing behaviors or mediating variables, how programs do so is generally less well-known. BCTs provide an opportunity to identify the elements of curricula which influence behavior
change and provide a common system to be used across programs. The author hopes this study
Appendix A
Foshee et al., 1998 Results
Treatment and Control Group Comparisons of Mediating Variables and at Baseline and Follow-Up in the Full, Primary, and Secondary Prevention Samples, North Carolina, 1994/1995 (n=14)
Appendix B
Additional BCT Descriptions
References
Abraham, C., Wood, C. E., Johnston, M., Francis, J., Hardeman, W., Richardson, M., & Michie, S. (2015). Reliability of Identification of Behavior Change Techniques in Intervention Descriptions. Annals of Behavioral Medicine, 49(6), 885–900. https://doi.org/10.1007/s12160-015-9727-y
Adelman, M., & Sang Hea Kil. (2007). Dating Conflicts: Rethinking Dating Violence and Youth Conflict. Violence Against Women, 13(12), 1296–1318. https://doi.org/10.1177/1077801207310800
Aventin, Á., Lohan, M., O’Halloran, P., & Henderson, M. (2015). Design and development of a film-based intervention about teenage men and unintended pregnancy: Applying the Medical Research Council framework in practice. Evaluation and Program Planning, 49, 19–30. https://doi.org/10.1016/j.evalprogplan.2014.11.003
Barker, G., Ricardo, C., Nascimento, M., Olukoya, A., & Santos, C. (2010). Questioning gender norms with men to improve health outcomes: Evidence of impact. Global Public Health, 5(5), 539–553.
https://doi.org/10.1080/17441690902942464
Black, M & Breiding M (2008). Adverse Health Conditions and Health Risk Behaviors Associated with Intimate Partner Violence—United States, 2005. MMWR. Volume 57(5), 113-117.
Bonache, H., Gonzalez-Mendez, R., & Krahé, B. (2017). Romantic Attachment, Conflict Resolution Styles, and Teen Dating Violence Victimization. Journal of Youth and Adolescence, 46(9), 1905–1917.
https://doi.org/10.1007/s10964-017-0635-2
Boutron, I., Moher, D., Altman, D. G., Schulz, K. F., Ravaud, P., & for the CONSORT Group. (2008). Extending the CONSORT Statement to Randomized Trials of Nonpharmacologic Treatment: Explanation and Elaboration. Annals of Internal Medicine, 148(4), 295. https://doi.org/10.7326/0003-4819-148-4-200802190-00008
Breiding, M. J., Basile, K. C., Smith, S. G., Black, M. C., & Mahendra, R. (2015). Intimate partner violence surveillance uniform definitions and recommended data elements. Atlanta, GA: Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. Adverse health Conditions and Health Risk Behaviors Associated with
Intimate Partner Violence--United States, 2005. MMWR 2008;57(No. 5):[113-117].
Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance--United States, 2011. MMWR 2012;61(SS04):[1-62].
Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance--United States, 2013. MMWR 2014;63(SS04):[1-172].
Centers for Disease Control and Prevention. Youth Risk Behavior Surveillance--United States, 2015. MMWR 2016;65(SS06):[1-180].
Cohen, J. R., Shorey, R. C., Menon, S. V., & Temple, J. R. (2018). Predicting Teen Dating Violence Perpetration. Pediatrics, 141(4), e20172790. https://doi.org/10.1542/peds.2017-2790
Cornelius, T. L., & Resseguie, N. (2007). Primary and secondary prevention programs for dating violence: A review of the literature. Aggression and Violent Behavior, 12(3), 364–375. https://doi.org/10.1016/j.avb.2006.09.006
Dank, M, Lachman, P, Zweig, J, et al (2014). Dating Violence Experiences of Lesbian, Gay, Bisexual, and Transgender Youth. Journal of Youth and Adolescence 43(5), 846-857.
Davidson, K. W., Goldstein, M., Kaplan, R. M., Kaufmann, P. G., Knatterud, G. L., Orleans, C. T., Whitlock, E. P. (2003). Evidence-based behavioral medicine: What is it and how do we achieve it? Annals of Behavioral Medicine, 26(3), 161–171. https://doi.org/10.1207/S15324796ABM2603_01
De Vasconcelos, S., Toskin, I., Cooper, B., Chollier, M., Stephenson, R., Blondeel, K., & Kiarie, J. (2018). Behaviour change techniques in brief interventions to prevent HIV, STI and unintended pregnancies: A systematic review. PLoS ONE, 13(9). https://doi.org/10.1371/journal.pone.0204088
Hickman, L. J., Jaycox, L. H., & Aronoff, J. (2004). Dating Violence among Adolescents: Prevalence, Gender Distribution, and Prevention Program Effectiveness. Trauma, Violence, & Abuse, 5(2), 123–142. https://doi.org/10.1177/1524838003262332
Hill, C. A., & Abraham, C. (2008). School-based, randomised controlled trial of an evidence-based condom promotion leaflet. Psychology & Health, 23(1), 41–56. https://doi.org/10.1080/08870440701619726
Hunnicutt, G. (2009). Varieties of Patriarchy and Violence Against Women: Resurrecting “Patriarchy” as a Theoretical Tool. Violence Against Women, 15(5), 553–573. https://doi.org/10.1177/1077801208331246
Hynynen, S.-T., van Stralen, M. M., Sniehotta, F. F., Araújo-Soares, V., Hardeman, W., Chinapaw, M. J. M., Hankonen, N. (2016). A systematic review of school-based interventions targeting physical activity and sedentary behaviour among older adolescents. International Review of Sport and Exercise Psychology, 9(1), 22–44.
https://doi.org/10.1080/1750984X.2015.1081706
Foshee, V, & Langwick, S (2004). Safe Dates: An Adolescent Dating Abuse Prevention Curriculum. Center City, Minnesota: Hazeldon Foundation.
Foshee, V. A., Linder, G. F., Bauman, K. E., & Langwick, S. A. (1996). The Safe Dates Project: Theoretical Basis, Evaluation Design, and Selected Baseline Findings. Retrieved October 16, 2018, from https://www.ajpmonline.org/ article/S0749-3797(18)30235-6/pdf
Foshee, V. A., Bauman, K. E., Arriaga, X. B., Helms, R. W., Koch, G. G., & Linder, G. F. (1998). An evaluation of Safe Dates, an adolescent dating violence prevention program. American Journal of Public Health, 88(1), 45–50. Foshee, V. A., Bauman, K. E., Greene, W. F., Koch, G. G., Linder, G. F., & MacDougall, J. E. (2000). The Safe Dates
program: 1-year follow-up results. American Journal of Public Health, 90(10), 1619–1622.
Foshee, V. A., Linder, F., MacDougall, J. E., & Bangdiwala, S. (2001). Gender Differences in the Longitudinal Predictors of Adolescent Dating Violence. Preventive Medicine, 32(2), 128–141. https://doi.org/10.1006/pmed.2000.0793 Foshee, V. A., Bauman, K. E., Ennett, S. T., Linder, G. F., Benefield, T., & Suchindran, C. (2004). Assessing the
Long-Term Effects of the Safe Dates Program and a Booster in Preventing and Reducing Adolescent Dating Violence Victimization and Perpetration. American Journal of Public Health, 94(4), 619–624.
Foshee, V. A., Bauman, K. E., Ennett, S. T., Suchindran, C., Benefield, T., & Linder, G. F. (2005). Assessing the Effects of the Dating Violence Prevention Program “Safe Dates” Using Random CoefficientRegression Modeling. Prevention Science, 6(3), 245–258. https://doi.org/10.1007/s11121-005-0007-0
Foshee, V. A., Reyes, H. L. M., Gottfredson, N. C., Chang, L.-Y., & Ennett, S. T. (2013). A longitudinal examination of psychological, behavioral, academic, and relationship consequences of dating abuse victimization among a primarily rural sample of adolescents. The Journal of Adolescent Health : Official Publication of the Society for Adolescent Medicine, 53(6). https://doi.org/10.1016/j.jadohealth.2013.06.016
Foshee, V, Reyes, L, Agnew-Brune, C, Simon, T, Vagi, K, Lee, R, & Suchindran, C (2014). The effects of the evidence-based Safe Dates dating abuse prevention program on other youth violence outcomes. Prevention Science, 15(6), 907-916.
Kann, L, McManus, T, Harris, W, Shanklin, S, Flint, K, Hawkins, J, et al (2016). Youth risk behavior surveillance--United States, 2015. MMWR Surveillance Summaries. Volume 65 (No. SS-6), 1-174.
Lundgren, R., & Amin, A. (2015). Addressing Intimate Partner Violence and Sexual Violence Among Adolescents: Emerging Evidence of Effectiveness. Journal of Adolescent Health, 56(1), S42–S50.
https://doi.org/10.1016/j.jadohealth.2014.08.012
Michie, S., & Johnston, M. (2012). Theories and techniques of behaviour change: Developing a cumulative science of behaviour change. Health Psychology Review, 6, 1–6. https://doi.org/10.1080/17437199.2012.654964
Michie, S., Richardson, M., Johnston, M., Abraham, C., Francis, J., Hardeman, W., Wood, C. E. (2013). The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions. Annals of Behavioral Medicine, 46(1), 81–95.
https://doi.org/10.1007/s12160-013-9486-6
Miller, E., Tancredi, D. J., McCauley, H. L., Decker, M. R., Virata, M. C. D., Anderson, H. A., Silverman, J. G. (2013). One-Year Follow-Up of a Coach-Delivered Dating Violence Prevention Program: A Cluster Randomized Controlled Trial. American Journal of Preventive Medicine, 45(1), 108–112. https://doi.org/10.1016/j.amepre.2013.03.007 Moher, D., Schulz, K. F., & Altman, D. G. (2001). The CONSORT statement: revised recommendations for improving the
quality of reports of parallel group randomized trials. BMC Medical Research Methodology, 1, 2. https://doi.org/10.1186/1471-2288-1-2
Murry, V. M., Berkel, C., Chen, Y., Brody, G. H., Gibbons, F. X., & Gerrard, M. (2011). Intervention Induced Changes on Parenting Practices, Youth Self-Pride and Sexual Norms to Reduce HIV-Related Behaviors Among Rural African American Youths. Journal of Youth and Adolescence, 40(9), 1147–1163. https://doi.org/10.1007/s10964-011-9642-x
“Preventing Teen Dating Violence,” (2017). Atlanta, GA: Centers for Disease Control and Prevention.
Reed, E., Raj, A., Miller, E., & Silverman, J. G. (2010). Losing the “Gender” in Gender-Based Violence: The Missteps of Research on Dating and Intimate Partner Violence. Violence Against Women, 16(3), 348–354.
https://doi.org/10.1177/1077801209361127
Roberts, T. A., Klein, J. D., & Fisher, S. (2003). Longitudinal Effect of Intimate Partner Abuse on High-Risk Behavior Among Adolescents. Archives of Pediatrics & Adolescent Medicine, 157(9), 875–881.
https://doi.org/10.1001/archpedi.157.9.875
Schoeppe, S., Alley, S., Rebar, A. L., Hayman, M., Bray, N. A., Van Lippevelde, W., Vandelanotte, C. (2017). Apps to improve diet, physical activity and sedentary behaviour in children and adolescents: a review of quality, features and behaviour change techniques. The International Journal of Behavioral Nutrition and Physical Activity, 14.
Smith, P. H., White, J. W., & Holland, L. J. (2003). A Longitudinal Perspective on Dating Violence Among Adolescent and College-Age Women. American Journal of Public Health, 93(7), 1104–1109.
Storer, H. L., Casey, E., & Herrenkohl, T. (2016). Efficacy of Bystander Programs to Prevent Dating Abuse Among Youth and Young Adults: A Review of the Literature. Trauma, Violence, & Abuse, 17(3), 256–269.
https://doi.org/10.1177/1524838015584361
Warsaw, C, Brashler, P, & Gil, J (2009). Mental health consequences of intimate partner violence. In Mitchell & Anglin (Eds.), Intimate partner violence: a health-based perspective. New York: Oxford University Press.