Emergency Transportation
Technology Opportunity Assessment
Prepared for the Merck for Mothers Program
February 2012 M A IL ING A D DR E S S PO Box 900922 Seattle, WA 98109 USA A D DR E SS 2201 Westlake Avenue Suite 200
Seattle, WA, USA
TEL
:
206.285.3500FAX
:
206.285.6619 www.path.orgCopyright © 2013, Program for Appropriate Technology in Health (PATH). All rights reserved. Cover photo credit: PATH/Gabe Bienczycki.
1
Emergency Transportation
Summary
Modes of transportation for women who need to reach a health facility in an obstetric emergency vary in safety, comfort, and speed. Emergency transportation includes motorized vehicles (cars, motorbikes), bicycles, animals, and boats and must be able to traverse roads, non-road terrain, and water. To improve health outcomes, women need access to efficient transportation options in low-resource settings.
Statement of Need
While most pregnancies and births are uneventful, all pregnancies are at risk. Around 15% of all pregnant women develop a potentially life-threatening complication that calls for skilled care and some will require a major obstetrical intervention to survive.1 About 1,000 women die from pregnancy- or childbirth-related complications around the world every day; of these, 99% occur in low-resource countries.2 Improving maternal health is one of the eight United Nations Millennium Development Goals (MDGs) adopted by the international community in 2000. The fifth MDG is to achieve a 75% reduction in maternal mortality between 1990 and 2015. Emergency obstetric care (EmOC),* access to family planning, and skilled attendance at birth are three key interventions that have been implemented globally to reduce maternal mortality. EmOC is a package of medical interventions that has been developed to treat the five direct obstetric complications—obstetric hemorrhage, obstructed labor, septicemia, hypertensive disorders in pregnancy, and unsafe abortion—that cause 75% of maternal deaths. However, in spite of global efforts to reduce mortality, the World Health Organization reports that the global maternal mortality ratio (i.e., the number of maternal deaths per 100,000 live births) declined by only 2.3% per year between 1990 and 2008.2 This is far from the annual decline of 5.5% required to achieve the fifth MDG.
In settings where maternal mortality is highest, three crucial delays are directly associated with elevated rates of maternal mortality. These are: (1) delay in seeking health care, (2) delay in reaching a health facility, and (3) delay in obtaining appropriate care upon reaching a health facility. To improve obstetric outcomes, a woman must recognize that she is experiencing an obstetric emergency, her family must be supportive of her seeking care at a health facility, she must be able to access transportation and be successfully transported to the appropriate health facility, and she must receive the care that she needs.3 The second delay is a direct consequence of transportation systems that are poor, nonexistent, or expensive—or a combination of these three. For instance, in Tanzania, 61% of women said that they could not deliver in a facility because it was too far away, while 44% of women indicated that they had no means to reach a facility.4 In rural Zimbabwe, 28% of all maternal deaths have been attributed to an
* The medical interventions of EmOC include antibiotics, cesarean operations, blood transfusions, anticonvulsants/antihypertensive drugs, uterotonic drugs, manual removal of the placenta and placental fragments/repair of genital lacerations, assisted vaginal delivery, and safe abortion care (either postabortion care or the complete package for abortion care).
2
inability to access transportation from one’s home to a health facility.5
Among the indigenous
communities of Cambodia, lack of transportation was cited as the second most important barrier (after lack of money) to accessing care at health centers.6
Most households, especially in rural areas, do not possess a personal vehicle, thereby necessitating their reliance on public transportation or shared means of transportation for transferring women to health facilities. Problems exist with both public and shared transportation options, including lack of fuel, absence of motorized vehicles at night or during quiet days (e.g., non-market days), refusal of car/bus drivers to carry pregnant women for fear of their vehicles being stained by blood, lack of funds to pay the cost of transportation, artificially increased fees for emergency transport, and the poor quality or absence of roads.7 In many cases, the women are forced to walk or be carried to the nearest health facility.3 These problems are further exacerbated when a woman needs to be transported to a heath facility for EmOC since the critical time window for ensuring that the woman is able to survive complications during childbirth is only a few hours. This is a particularly worrisome situation in countries such as Mali, Haiti, and the Central African Republic where over 40% of rural women live more than 15 kilometers from the nearest health center able to assist with deliveries. In countries with particularly poor roads and
transportation, such as Sierra Leone, this may translate into anywhere between 3 and 24 hours to reach a hospital.7
Unfortunately, there is no single “silver bullet” technology that can solve the issue of transport for women experiencing an obstetric emergency. Each setting is unique given widespread variations in the
availability of certain modes of transportation, the geography of the area, the condition of roads, and the ability of the community to pay for a particular mode of transportation. Therefore, any emergency transport system needs to be developed within the broader context of health systems with robust early warning and referral mechanisms. The early warning and referral mechanisms would need to include means of emergency transportation that currently exist in a particular setting as well as innovative means of transportation that could be easily introduced and maintained in a sustainable manner.
Additionally, the three delays cannot be viewed in isolation since addressing one delay does not
necessarily imply that the other delays will be automatically addressed. It is, therefore, essential that any strategies to improve transportation for obstetric emergencies also address the need for early recognition of obstetric problems, sensitizing families and communities about the importance of seeking care in a timely way, and improving the quality of obstetric care.
Technology Solutions Landscape
A landscape of the literature and programmatic evidence shows that a variety of means of transportation have been used to transport women for accessing EmOC—either from the community to the first-line health care facility or from the latter to the hospital. 7,8The mode of transportation used is usually a
3
function of two broad variables: access to motorized transport and access to roads. The landscape of transportation options is summarized in Table 1 below.
Table 1. Emergency transportation options.
Access to motorized transport
No or little access to motorized transport
Access to an all-weather motorable road
Medical ambulance, taxi, bus, shared vehicle, motorcycle ambulance, private vehicle (usually tractor).
Bicycle ambulance, animal cart, rickshaw, padded seat on an animal, canoe, maternity waiting home.
Access to seasonal roads
Motorboat, all-wheel drive (AWD) vehicle, tractor, airplane, maternity waiting home.
Animal cart, padded seat on an animal, canoe, maternity waiting home.
No access to roads Motorboat, airplane, AWD vehicle,
maternity waiting home.
Canoe, padded seat on an animal, maternity waiting home.
Communities with access to all-weather motorable roads Access to motorized transport
Motorized transport is generally the best way to transport women. Motorized means of transportation are usually comfortable and able to offer privacy, able to cover long distances relatively quickly, and can accommodate family members of the woman requiring transportation. Communities with access to motorable roads and motorized transport have utilized modern ambulances, taxis, public transport, shared vehicles, motorcycle ambulances, and tractors to transport women.
Robust, modern, motorized ambulances are the best way to transport women. The use of ambulances has been scaled up in low-resource settings, including India, where a public-private partnership aims to provide one ambulance for every 100,000 people.9 However, the system has certain limitations including a reliance on sustained government funding and continued slow penetration into rural, remote areas. Moreover, while dedicated ambulances have been used to transport women from communities to health facilities in low-resource settings, they are more likely to be found at health facilities, where these ambulances are used to refer women to hospitals in case women face obstetric complications that cannot be treated at the health facility. Therefore, in low-resource settings, only a small percentage of women are taken to the hospital in dedicated ambulances, and most of these are women who live in urban or peri-urban settings. Some of the barriers to making ambulances more available include purchase price of the vehicle, cost and technical expertise needed to maintain and keep the vehicle in running condition, high fuel prices, and problems with fuel supply. In addition, obstetric emergencies are usually fairly rare events, which results in the ambulances often remaining idle and unused for significant amounts of time. As a result, ambulances—even if present—are expensive and often beyond the reach of ordinary, rural families living on little more than a dollar a day.
In the absence of dedicated ambulances, communities have utilized taxis, public transportation, and shared vehicles to transport women for obstetric care. Taxis are a good way to transport women, since they provide a certain degree of privacy and allow family members to accompany women. Taxis have
4
been used to transport women on an ad hoc basis all across the world—especially from the community to the facility, though they may be used for referrals to hospitals if an ambulance is not available at the facility. However, taxis are usually an expensive means of transportation, though financial barriers have been lowered by systematic strategies such as forming partnerships with taxi unions and establishing seed funds to cover transportation costs that would be paid later on (Nigeria), training taxi drivers in basic first aid (Ghana), and mapping and reaching out to vehicle operators to establish a standard fee based on distance (Nigeria). In addition to financial barriers, women using taxis to access obstetric care face cultural barriers that dissuade taxi drivers from transporting women in labor for fear of soiling their vehicles with blood. Cultural barriers have been dismantled by sensitizing taxi drivers and transport unions (Nigeria and Ghana).8
Public transport and shared vehicles are cheaper than taxis, though they do not offer the privacy of a taxi and/or ambulance. Such means of transportation are mostly used to transport women from the
communities to the health facility. Among other means of motorized transport, motorcycle ambulances (motorcycles with specially fitted sidecars) have been used with success in Malawi to reduce
transportation times, while tractors have been demonstrated as a good means of emergency transportation in Ghana, Tanzania, Tibet, and India.8 Motorcycle ambulances are, however, not particularly feasible if women need to be transported over distances greater than 30 kilometers. Moreover, they do not provide privacy to the woman being transported or allow her family members to accompany her.
No or little access to motorized transport
Communities with little or no access to motorized transport have used bicycle ambulances (trailers fitted to bicycles), animal carts, rickshaws/tricycles, animal “ambulances” (padded seats on animals), and canoes. Obviously, nonmotorized means of transport are not ideal for transporting women over long distances since they are slow and require manual effort to operate. In fact, the maximum distance that can be covered by nonmotorized means of transport is usually 5 to 20 kilometers. In addition, nonmotorized means of transport usually do not provide adequate protection of privacy or protection from
environmental elements—thereby limiting their utility to short distances. Nonmotorized means of transport are also generally unsuitable for referrals from a primary health facility to the hospital. Bicycle ambulances have often been suggested as an effective means of nonmotorized transportation (Namibia, Malawi, and Zambia); however, there have been several concerns around the lack of privacy and the inability for family members to accompany the women being transported in bicycle ambulances. Communities with no or little access to motorized transport can also make maternity waiting homes available. Maternity waiting homes are residential facilities, located near a qualified medical facility, where women can await their delivery. Some maternity waiting homes have the capacity to assist women during normal, uncomplicated births. In most cases, women are transferred to a nearby medical facility shortly before delivery or earlier should complications arise. In these homes, additional emphasis is sometimes put on education and counseling regarding pregnancy, delivery, and care of the newborn infant and family. Maternity waiting homes “bridge the geographical gap” in obstetric care and serve asa link in a larger chain of comprehensive maternity care.However, maternity waiting homes can only meet their
5
objective to reduce maternal mortality if the women they serve receive quality care in the facilities they are linked to. There is considerable variation in the organizational structures, funding, and responsibilities for upkeep of maternity waiting homes. Maternity waiting homes have been established and scaled up in several countries (e.g., Cuba, Peru, Mongolia, Zimbabwe). While maternity waiting homes have the potential to improve access to obstetric care, there are still barriers that prevent women from using a maternity waiting home including the cost for their meals, the “voluntary” financial contribution that is expected, and the inability to leave families for long periods of time.
Communities with access to seasonal roads Access to motorized transport
Communities are often connected to roads that are impassable during certain seasons—especially during the rainy season. The means of motorized transport discussed previously would probably not be able to function outside the dry season. During the season when roads become impassable, tractors and all-wheel drive (AWD) vehicles (Niger, India) could still be used to transport women to facilities. Motorboats have been used for emergency transportation in places such as coastal/riverine Bangladesh, Burma, and Ghana. Such means of transportation are probably more suited for transportation from the community to the primary health facility and not from the latter to the hospital for referrals. Airplanes have been used for emergency transportation in extremely remote places, such as Arctic Canada and Papua New Guinea. However, for the obvious reason of high costs, air transport is not a sustainable option without sustained funding from governments and/or donors. The option of traveling to maternity waiting homes a few weeks in advance of the expected delivery date is still valid for this scenario.
No or little access to motorized transport
For communities with limited access to motorized transport and all-weather roads, the options for emergency transportation during the season when roads are rendered impassable are reduced to animal carts, canoes, and padded seats on animals—none of which are particularly comfortable for a woman in labor. Moreover, these transportation options are not likely to be feasible for referrals from the facility to the hospital. Once again, traveling to a maternity waiting home is a good solution. It is possible that motorized transportation may be used to transport women from the maternity waiting home to the health facility or from the latter to the hospital for referrals.
Communities with no access to roads Access to motorized transport
For communities with no access to roads (e.g., communities in delta/estuarine, mountainous, and remote forest regions), the only motorized means of transportation would include motorboats or airplanes. AWD vehicles may work in mountainous or desert regions, but would not work in regions with soft soils and frequent barriers in the form of river crossings and dense forests. Such means of transportation are probably more suited for transportation from the community to the primary health facility—and not from the latter to the hospital for referrals. Again, traveling to a maternity waiting home is a possible solution.
6
Motorized transportation may be used to transport women from the maternity waiting home to the health facility or from the latter to the hospital for referrals.
No or little access to motorized transport
For communities with limited access to motorized transport and no access to roads, canoes and padded seats on animals are likely to be the only options. Once again, these means of transportation are probably more suited for transportation from the community to the primary health facility—and not from the latter to the hospital for referrals. Women may have the option of traveling to a maternity waiting home and then being taken by motorized transportation to the health facility.
Since emergency transportation systems constitute a part of the continuum of emergency referral and care, emergency transportation systems are closely linked with emergency communication systems. Communication systems are essential for alerting community-based health workers in the event of an obstetric emergency; calling a taxi, ambulance, etc. to transport a woman from her home to the health facility; contacting the health facility to give them advance notice of an obstetric emergency; and referring a woman from a primary health care facility to a hospital. There are numerous examples which demonstrate the strong synergies between emergency communication systems and emergency
transportation systems. These include the use of telephones to facilitate communication between primary health centers and hospitals in Bangladesh, Laos, and Peru; two-way radios in facilities and emergency vehicles in Malawi, Mali, Sierra Leone, Tanzania, and Uganda; the toll-free emergency phone number (108) for calling ambulances in India; and the “yellow flag initiative” of West Africa, where yellow flags are set up by the side of the road to notify passing drivers of a woman in need of emergency
transportation.
Community-based agents/volunteers play a vital role in maintaining the continuum of emergency referral and care. In addition to accompanying women to the facility or for referrals, community volunteers coordinate logistics related to emergency transportation—mobilizing transportation, obtaining funds, contacting the facility, etc. They also advise women and their families about ways to reach a facility, including transfer to maternity waiting homes in advance of delivery.
Gap Analysis
The end goal of an emergency transportation system is to ensure that a woman arrives at the appropriate health care facility in the most timely and comfortable manner possible. Any emergency transportation strategy will need to address barriers such as distance to the appropriate facility, geography, loss of road access during certain seasons, availability of transportation at different times, transportation costs, community ability and willingness to pay for emergency transportation, government buy-in, cultural norms, and availability of emergency communication systems.1 The mode of emergency transportation should also protect the woman’s privacy and possibly allow family members or a health worker to travel with the women.
7
The landscape analysis shows that there is no one transportationsolution that is applicable to all scenarios. For instance, in urban and peri-urban India, where communities have access to all-weather motorable roads and where there is significant buy-in from the government and the private sector, ambulances are used to transport women for receiving obstetric care. However, ambulances would not work in settings where communities do not have access to all-weather motorable roads, or where there is less buy-in from the government and the private sector. Because there is no one “silver bullet” solution to the emergency transportation problem, what is needed is a tool that will assist communities in developing an acceptable, sustainable strategy that will ensure that all women experiencing an obstetric emergency can be transported to a health facility.
The tool will assist communities to conduct a situational analysis related to emergency transportation and develop a strategy for emergency transportation that maximizes enabling factors and addresses specific barriers. The design of such a tool has been conceptualized by Holmes and Kennedy.8 The situational analysis would take into account inputs such as the following:
List of relevant facilities (health centers, hospitals, maternity waiting homes, etc.) and distance to and between each facility.
Availability and quality of obstetric care at each facility.
Means of transportation available from the community to the relevant facilities and between each facility.
Cost of the available means of transportation.
Seasonality of the available means of transportation, if any. Means of communication available in the community.
Cultural and financial barriers preventing women from being transported for emergency obstetric care.
Community-based facilitators, such as mother support groups and micro-financing schemes, which could potentially assist women to obtain emergency transportation.
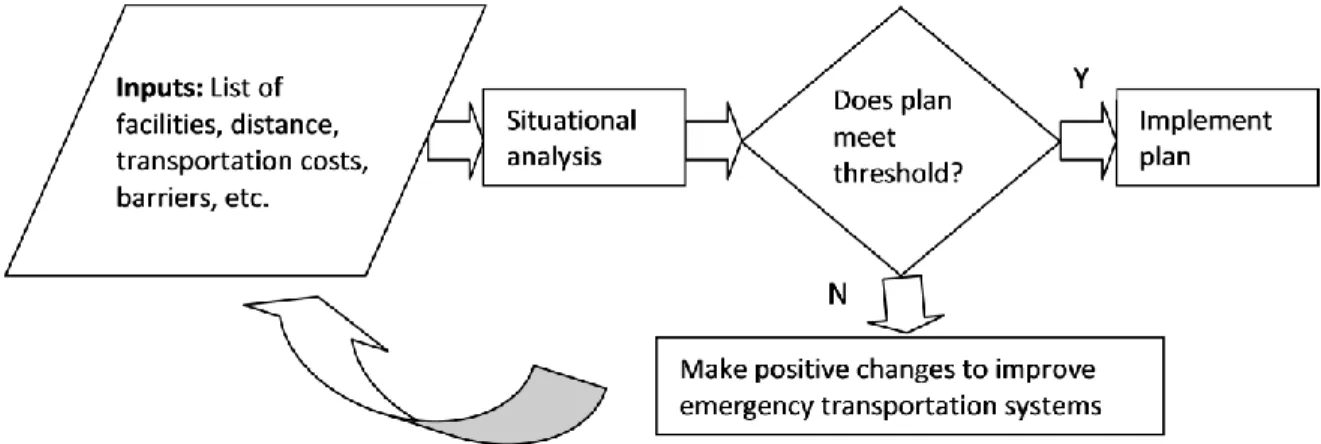
The strategy that would be developed from the above analysis would obviously need to be weighed against certain predetermined thresholds. In other words, the tool would also have an assessment function that would enable communities to make positive changes to reinforce their emergency transportation systems based on the results of the situational analysis. For instance, if the emergency transportation plan that is generated through the planning process is the use of an animal cart to reach a facility that is 30 kilometers away, this plan would not be considered ideal since the current recommendations suggest motorized transportation for any distance beyond 20 kilometers. In such a case, the tool and emergency transportation plan could be used as the basis of further work to address more systemic barriers to emergency transportation—e.g., cultural barriers against using certain means of transportation, lack of financial incentives for transportation operators to provide emergency transportation to women, or lack of all-season motorable roads. The process flow for using the planning tool is summarized in Figure 1.
8
Figure 1. Emergency tranportation planning process.†
Simple tools have been developed to help individual pregnant women prepare for birth including the “Preparing for my Birth” card from the CHANGE Project10
and the “Birth Preparedness and Complication Readiness” matrix from Jhpiego.11
The complication readiness plan helps individual pregnant women prepare for obstetric complications by addressing such areas as saving money, finding a means of transportation to the nearest facility, and recognizing signs and symptoms of obstetric
complications. However, a literature review did not identify any comprehensive tools currently in use that guide communities through the development of a customized emergency transportation plan using existing resources. This includes identifying systemic gaps and undertaking efforts to address such gaps. For funding the development and field testing of the emergency transportation planning tool, one should ideally look to couch this project in a larger project related to maternal and child health, health systems strengthening, etc. If that is not possible, there are several stand-alone funding opportunities that could kick-start an initiative, including the Bill & Melinda Gates Foundation’s Grand Challenges in Global Health, Saving Lives at Birth, Ashoka Changemakers, and internal funding opportunities within individual organizations.
Investment Opportunity
Based on the technology solutions landscape and gap analysis, which suggested that there is no single “silver bullet” emergency transportation solution, we have identified the emergency transportation planning tool as the intervention that would potentially have the greatest impact in reducing delays in obtaining transportation for women requiring EmOC. While community-level emergency transportation plans have been conceptualized in the literature, there are no tools that actually allow communities to determine the best use of existing resources to create emergency transportation plans. Therefore, we would propose investment in leading the developing, field testing, and scaling up a simple emergency
†
9
transportation planning tool that would allow communities to design comprehensive, customized emergency transportation plans to transport women in need of EmOC. The following are the specific investment opportunities:
Developing the emergency transportation planning tool
Over the years, governments and nongovernmental organizations have developed and implemented a wealth of emergency transportation and referral strategies in a variety of settings. Moreover, the general conceptual framework for emergency transportation has been elucidated in the literature. Therefore, we propose that as a first step, one should use existing emergency transportation frameworks and solicit feedback from stakeholders (international health bodies, donors, national governments, nongovernmental organizations, etc.) to design a beta version of the emergency transportation planning tool.
Pilot testing the emergency transportation planning tool
In order to build a solid case for the use of the emergency transportation planning tool as a standard community-based intervention, the tool must first be pilot tested in a variety of settings as described previously: communities with access to motorized vehicles and all-season roads, communities with no access to motorized vehicles and access to seasonal roads, communities with no access to motorized vehicles and no access to any roads, etc. There is a robust body of evidence that highlights the efficacy of individual emergency transportation strategies in specific settings (e.g., motorcycle ambulances in Malawi, private-public partnerships in India, AWD vehicles in Niger). However, there is little or no evidence that underscores the efficacy of using a community-based emergency transportation planning tool as evaluated through such outcome indicators as reduction in transportation times, increase in facility-based management of obstetric emergencies, or improvement in comfort levels experienced by women being transported to facilities. In addition to evaluating the efficacy of the emergency
transportation planning tool, the pilot testing phase would be an opportunity to identify deficiencies and weaknesses in the design of the tool. The latter will need to be addressed and incorporated into the final design of the tool.
Scaling up the emergency transportation planning tool
It is important to identify high-impact countries with demonstrated commitment toward realizing MDG 5 where community-based resources such as mother support groups and village development committees are established entities. Once these countries have been identified, sustained advocacy will need to be carried out to ensure inclusion of the emergency transportation planning tool as part of routine community-based programming. Advocacy efforts will need to focus on a variety of stakeholders including governments, nongovernmental organizations, and national medical associations. Care should be taken to create and strengthen linkages with existing emergency transportation, communication, and referral systems wherever possible—instead of replacing such systems. One will need to draw upon experience in community-based programming to facilitate the adoption of emergency transportation plans at the community level. Additionally, when communities consistently and regularly identify particular systemic gaps in referral systems while creating their emergency transportation planning tools, one will need to leverage its relationships with governmental stakeholders to address these gaps. The
10
implementing organization will also need to provide technical assistance to national governments to train master trainers and district health officials so that they are able to facilitate communities to prepare their emergency transportation plans.
Developing paperless versions of the emergency transportation planning tool
One can assume that the initial version of the emergency transportation planning tool will be a paper-based tool. However, given the widespread use of mobile phones in the developing world, an
implementing organization can look at opportunities to create mobile phone/personal digital assistant (PDA)–based versions of the tool. In addition to eliminating the use of paper, phone-based tools have the added advantage of allowing communities to seamlessly link emergency transportation plans with emergency communication systems, health management information systems, and geographic information systems.
11
References
1. World Health Organization (WHO). Managing Complications in Pregnancy and Childbirth: A Guide for Midwives and Doctors. Geneva: WHO; 2003.
2. WHO. Maternal mortality [fact sheet]. Geneva: WHO; 2010. Available at: http://www.who.int/mediacentre/factsheets/fs348/en/index.html
3. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Social Science & Medicine. 1994;38(8):1091–1100.
4. Bicego G, Curtis S, Raggers H, Kapiga S, Ngallaba S. Sumve Survey on Adult and Childhood
Mortality, Tanzania, 1995: In-depth study on estimating adult and childhood mortality in settings of high adult mortality. Calverton, Maryland: Macro International; 1997.
5. Fawcus S, Mbizvo M, Lindmark G, Nyström L. A community-based investigation of avoidable factors for maternal mortality in Zimbabwe. Studies in Family Planning. 1996;27(6):319–327.
6. Action Research to Advocacy Initiative (ARAI). Indigenous Women Working Towards Improved Maternal Health. London, United Kingdom: ARAI; 2006.
7. Babinard J, Roberts P. Maternal and Child Mortality Development Goals: What Can the Transport Sector Do? Washington, DC: World Bank; 2006.
8. Holmes W, Kennedy E. Reaching emergency obstetric care: overcoming the “second delay” [briefing paper]. Melbourne, Australia: COMPASS; 2010.
9. National Health Systems Resource Centre (NHSRC), Ministry of Health and Family Welfare,
Government of India. Study of Emergency Response Service—EMRI Model. New Delhi, India: NHSRC; 2009.
10. CHANGE Project. Preparing for my Birth. Available at: http://www.manoffgroup.com/ms_toolkit/docs/BP-01.pdf.
11. Jhpiego Maternal and Neonatal Health (MNH) Program. Birth Preparedness and Complication Readiness: A Matrix of Shared Responsibility. Baltimore, MD: Jhpiego; 2001. Available at: http://www.jhpiego.org/files/bpcrmatrix.pdf.