Volume 9, Issue 04, 2019
43
Available at www.jpbms.info
Research article
Effect of Task Specific Mirror Therapy on
Chronic Stroke
Arun B*, Mohangandhi V, Mohanraj K, Punitha Kumar RK.
Author affiliations
KG College of Physiotherapy, Coimbatore (Affiliated to TN Dr MGR Medical University, Chennai), India
Address reprint requests to
Arun B
Professor, KG College of Physiotherapy, Coimbatore (Affiliated to TN Dr MGR Medical University, Chennai), India Email: [email protected]
Abstract:
Background Stroke is one of the most common devastating disorder, it is one of the leading causes of disability in adults. Stroke is a major cause of long term physical, cognitive, emotional, social and vocational disability. Long term rehabilitation is the most essential for stroke survivors. Recovery of the hand and its function is much difficult in stroke and needs a long term care. One of the best methods in recent times is mirror therapy. Mirror therapy is a visual guided motor imagery therapy which enhances recovery by enlisting direct visual stimulation showing the affected limb working. However it is lacking in promotion of motivation in stroke patients, so the task specific mirror therapy is established to make the individual to involve in the activities along with the mirror therapy.
Aim The aim of the study is to identify the effect of task specific mirror therapy on chronic stroke.
Materials & Methods: Experimental study design involving 30 stroke patients and they were divided into two groups. Based on the selection criteria the participants were divided randomly into group I with Task specific mirror therapy (TSMT) and group II with Mirror therapy (MT) group, treatment programme continued for 8 week duration. Following the management Action research arm test (ARA) and the Box and block test (BBT) were used to identify the improvements.
Results Statistical analysis was done using SPSS 19.0. The data analysis shows the t value for grasp is 8.82 ± 0.25, Grip is 8.29 ± 0.17, Gross movement is 9.2 ± 0.16 and Pinch is 0.85 ± 0.39, and for the BBT is 13.28 ± 1.52 with
p<0.05% .
Conclusion The study concluded that TSMT produce significant result in improving hand function in ARA components and the BBT, on analysis of the each component in the ARA, the pinch component was not showing significant effect between the groups.
Key words
Upper extremity function, Chronic Stroke, Task specific mirror therapy, Mirror therapy, Action research arm test, Box and Block test.INTRODUCTION
troke is one of the most devastating neurological diseases which often causing death or
gross physical impairments or disability[1]. Stroke is the second leading cause of disability.
15 million people around the world affected by stroke every year[2]. It is one of the leading
causes of death above 60 years and 5th leading cause of death in people aged 15—59 years.
Stroke is the global epidemic and it is the leading cause for the disability and impairments. It
is an important cause for morbidity and mortality[3]. 85% of the stroke survivors experiences
disability in the upper extremity. About 69% of the stroke survivors has upper extremity deficits.[4]
S
https://doi.org/10.20936/jpbms/19/04/02
Volume 9, Issue 04, 2019
44
Upper extremity functional deficits or Hemiplegia is the common and detrimental effect of stroke. Upper extremity deficits are longer than the lower extremity deficits. Upper extremity
impairment affects the normal activities of daily living of any individual[5]. Upper extremity
recovery is significantly poor than the lower extremity in hemiplegia. Numerous longitudinal studies has shown that at least 85% of the stroke patient experiences upper limb deficits in that
only 50% of hemiplegia patients shows significant recovery with useful arm functions[6]. Initial
severity of paresis remains as the best predictor of recovery of arm function[6].
Many interventions fall in line for the rehabilitation of stroke, most common measures includes
drugs, electro stimulation, local nerve block and physiotherapy exercises[7,8]. Conventional
rehabilitation therapy for spasticity administered by therapist included passive exercises,
stretching and ROM exercises[9]. Interventions focusing on the rehabilitation of the upper
extremities are limited.
Mirror therapy is a therapeutic technique focusing to improve the functional movements of the paretic limb. This was introduced by Ramachandran and Roger Ramachandran to treat phantom limb pain after amputation. It is relatively simple and cost effective approach for
improving upper extremity function[10]. It was theorized that brain makes changes which affect
the motor recovery. Much strong evidences supports the use of Mirror therapy for upper
extremity recovery in patients with CVA[11].
However there is a lack of improvement in stroke and some of the literatures are not providing successful results. Various researchers has observed the positive effects of mirror therapy decreases over the time, they identified that simple movement of the limbs makes the patients bored and their motivation reduces over the time. Based on these observations mirror therapy programmes are being incorporated with variety of functional tasks which are
proposed to be effective[12]. So this study identifies the effect of task specific mirror therapy on
the upper extremity stroke patients.
METHODOLOGY
Study was approved by the institutional ethical committee. Informed consent was obtained from all the participants prior to the beginning of the study. Experimental study design with 36 subjects with chronic stroke were included in the study after due consideration of inclusion and exclusion criteria. Through initial assessment was done to all the selected subjects and clear instruction about the study were given and consent signed. Assessment of the subject was done by a Blinded assessor who is not involved in the study. 36 subjects who are derived from 50 subjects of samples who were initially evaluated. All the 36 subjects were divided into two equal groups using the computer assisted random sampling method. Subjects included were age group of more than 50--63 years, both gender, patients who are referred from the department of neurology, first stroke subjects, stroke with more than six month duration, able to understand commands, subjects without perceptual disorders, unilateral neglect, Brunnstrom
score between stages I—IV upper extremity, able to do the shoulder movement as per
commands and able to produce minimal movement in the affected wrist and hand.
Volume 9, Issue 04, 2019
45
releasing. Both group underwent 45 minutes of exercises and 15 mins for regular physiotherapy. Total duration was 60 minutes for all the participants. Outcome of the study was Action research arm test (ARA) and the Box and Block test (BBT). ARA test is developed by Ronald Lyle in 1981 which is extremely valid and reliable test. This test is an evaluative tool to assess the specific changes in the limb function among individuals with cortical damage. The Box and Block Test (BBT) measures unilateral gross manual dexterity. It is a quick, simple and inexpensive test. It can be used with a wide range of populations, including clients with stroke.
RESULTS
A total of 36 patients were included in the study, demographic demonstrations are presented in table 1. Table 2 shows the outcome measures of the action reach arm test values and box and block test value, table 3 shows calculated t values. 6 patients were withdrawn from the study owing to personal reasons so the study was concluded with 30 patients. On the analysis of the each component in the action reach arm test.
Table 1 Demographic data.
Age group (Years) Numbers Mean
50—52 7 50.86 ± 0.9
53—55 6 54.00 ± 089
56—58 6 56.83 ± 0.98
59—61 5 60.20 ± 0.84
62—63 6 62.50 ± 0.55
Males 17 56.70 ± 4.03
Females 13 56.38 ± 5.03
Year of stroke 30 3.93 ± 0.980
Table 2.ARA Test Analysis.
TSMT Group n=15
MT Group n=15
ARA Before After Before After
Grasp 5.87±0.833 11.67±0.72 5.8±0.77 9.47±0.64
Grip 1.2±0.41 2.80±0.41 1.13±0.35 1.4±0.51
Pinch 5.27±0.59 6.4±1.3 5.33±0.72 6.07±0.8
Gross Movement 1.13±0.35 2.87±0.35 1.13±0.35 1.4±0.51
BBT 40.33±1.95 71.27±4.2 40.53±1.68 51.07±4.13
Significant differences were obtained between the groups and within the groups for all the components in the Action research arm test and the Box and Block test. The pinch in the ARA was showing significant differences within the group whereas there was no significant difference obtained between the groups. Significance was obtained at <0.05%.
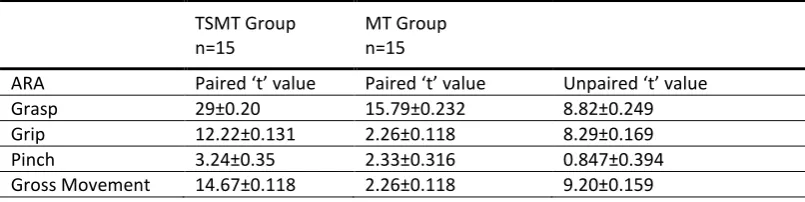
Table 3.Box and Block Test.
TSMT Group n=15
MT Group n=15
ARA Paired ‘t’ value Paired ‘t’ value Unpaired ‘t’ value
Grasp 29±0.20 15.79±0.232 8.82±0.249
Grip 12.22±0.131 2.26±0.118 8.29±0.169
Pinch 3.24±0.35 2.33±0.316 0.847±0.394
Volume 9, Issue 04, 2019
46
BBT 32.11±0.963 8.86± 1.191 13.28±1.521
All the calculated t values were showed significant differences when it compared with the table values. The values of Pinch between the group comparisons shows insignificant, states that there is no marked differences obtained between the experimental group and the control group. All the other values were showing significance differences at <0.05%. No adverse event occurred during the training period in the current study. There were no deleterious effects of the application of TSMT or MT group on measurement parameters.
DISCUSSION
The aim of the study is to find out the effect of Task-specific Mirror therapy on upper extremity function in chronic stroke patients. In this study all the parameters were found to be improved except the pinch component in the ARA. There was significant differences were obtained in the groups whereas there was no significant difference obtained between the groups.
Task specific mirror therapy involves common ADL activities that can effect on the patient motivation in doing the exercises. TSMT reduces the frequency of inappropriate movements by
repeatedly undertaking a wider movements which adapts to do other specialized tasks[13]. It
also promotes functions of the musculoskeletal and neuromuscular systems[14].
TSMT could produce recovery of the motor abilities of the upper extremity based on interactions with the normal upper limb. Inter limb transfer produces functional improvement of the hemiplegic upper extremity transfer of the effects of training the normal upper limb to
the hemiplegic upper extremity[15].
Mirror therapy theorized to work on the principle of visual stimuli conveyed to the brain through observation of the unaffected body part movements it can improve the function of the
affected limbs[15]. Dominant hand movements during the MT could make the non-dominant
hemisphere to experiences normalization of the asymmetrical activation. However the movement of non-dominant hand leads to the recruitment of the mirror neuron system which
enhances the contralateral brain to control movement in the reign limb[16].
Similar results were found by winstein et al.,[17] who reported that a significant difference in
upper limb motor function was found for those with less severe stroke in favor of task specific
mirror therapy versus standard care. Dean and shepherd[18], also reported that after training,
patients in the experimental group were able to reach faster and further. In comparison, improvements in reaching were not found with the control group.
Study limitation includes the small size limits the ability to make general conclusion regarding the efficacy of these methods. Long term efficacy is not assessed, future research could compare the other treatment methods. Follow up assessment should be added in the study to find the efficacy of the treatment.
CONCLUSION
The study concludes that task specific movement therapy produces significant improvement in the upper extremity function in ARA and BBT. The pinch component in the ARA is not significantly reduced between the groups.
ACKNOWLEDGEMENTS
Our sincere thanks to Padmashree Dr. G. Bakthavathsalam, Chairman, Mrs. Vasanthi Ragu, Vice Chairman, Mrs. Vaijeyanthi M Das, CEO, Mr. Prabhu Kumar, CEO, Prof. V. Mohan Gandhi, CEO, K.G. Hospital, Coimbatore, for their continuous support and guidance’s.
REFERENCES
1. Abegunde, D.O., Mathers, C.D., Adam, T.,
Volume 9, Issue 04, 2019
47
2. World Heart Federation, Stroke, Geneva, Switzerland, 2016. Available from:
http://www.world-heartfederation.org/cardiovascularhealth/stroke/ 3. Luke C, Dodd KJ, Brock K: Outcomes of the Bobath concept on upper limb recovery following stroke. Clin Rehabil. 2004, 18: 888–898. 4. Wolf SL, Catlin PA, Ellis M, et al.: Assessing Wolf motor function test as outcome measure for research in patients after stroke. Stroke. 2001; 32:1635–1639.
5. Pollock A, Farmer SE, Brady MC, Langhorne P, Mead GE, Mehrholz J, van Wijck F. Cochrane Overview: interventions for improving upper limb function after stroke. Stroke. 2015;46:e57-8. doi:10.1161/STROKEAHA.114.008295.
6. Sunderland A, Tinson D, Bradley L. Arm function after stroke: an evaluation of grip strength as a measure of recovery and a prognostic indicator. J Neurol Neurosurg Psychiatry. 1989;52:1267–1272.
7. Oki A, Oberg W, Siebert B, Plante D, Walker ML, Gooch JL. Selective dorsal rhizotomy in children with spastic hemiparesis. J Neurosurg Pediatr. 2010;6:353–358.
8. Gallichio JE. Pharmacologic management of spasticity following stroke. Phys Ther. 2004;84:973–981.
9. Selles RW, Li X, Lin F, Chung SG, Roth EJ, Zhang LQ. Feedback-controlled and programmed stretching of the ankle plantar flexors and dorsi flexors in stroke: effects of a 4-week intervention program. Arch Phys Med Rehabil. 2005;86:2330– 2336.
10. Stevens JA, Stoykov ME: Simulation of bilateral movement training through mirror reflection: a case report demonstrating an occupational therapy technique for hemiparesis.
Top Stroke Rehabil. 2004;11:59–66.
11. Wu CY, Huang PC, Chen YT, Lin KC, Yang HW. Effects of mirror therapy on motor and sensory recovery in chronic stroke: A randomized controlled trial. Arch Phys Med Rehabil. 2013;94:1023-30.
12. Khandare SS, Singaravelan RM, Khatri SM. Comparison of Task specific exercises and mirror therapy to improve upper limb function in subacute stroke patients. IOSR JDMS. 2013:7;5-14
13. Thielman GT, Dean CM, Gentile AM. Rehabilitation of reaching after stroke: task-related training versus progressive resistive exercise. Arch Phys Med Rehabil. 2004;85:1613– 1618.
14. Yang YR, Wang RY, Lin KH, Chu MY, Chan RC. Task-oriented progressive resistance strength training improves muscle strength and functional performance in individuals with stroke. Clin Rehabil. 2006;20:860–870.
15. Arya KN, Verma R, Garg RK, Sharma VP, Agarwal M, Aggarwal GG. Meaningful task-specific training (MTST) for stroke rehabilitation: a randomized controlled trial. Top Stroke Rehabil. 2012;19:193–211.
16. Bartur G, Pratt H, Dickstein R, Frenkel-Toledo S, Geva A, Soroker N. Electrophysiological manifestations of mirror visual feedback during manual movement. Brain Res. 2015;1606:113-24. 17. Winstein CJ, Rose DK, Tan SM, Lewthwaite R, Chui HC, Azen SP. A randomized controlled comparison of upper-extremity rehabilitation strategies in acute stroke: a pilot study of immediate and long-term outcomes. Archives of physical medicine and rehabilitation.2004; 85(4):620-628.
18. Dean CM, Shepherd RB. Task-Related Training Improves Performance of Seated Reaching Tasks After Stroke A Randomized Controlled Trial.
Stroke. 1997; 28(4):722-728.
Article citation: Arun B, Mohangandhi V, Mohanraj K, Punitha Kumar RK. Effect of Task Specific Mirror Therapy on Chronic Stroke. J Pharm Biomed Sci. 2019;09(04):43-47. Available at htp://www.jpbms.info
Conflicts of Interest: No conflict of interest.
Statement of originality of work: The manuscript has been read and approved by all the authors, the requirements for authorship have been met, and that each author believes that the manuscript represents honest and original work.
Source of support:None