University of Toronto Medical Journal
Table of Contents
All articles are externally peer-reviewed with the exception of poetry and short stories and book reviews. All manuscripts are internally reviewed. Informed consent practices and any conflicts of interest are specified in the articles if applicable.
Cover Artist: Front cover illustration by Janice Yau, University of Toronto medical student (1T6). Please visit www.janiceyau.com for her portfolio. PREFACE
77 Preface from the Editors
LETTER TO THE EDITORS 78 CPSI Letter to the Editors Hugh MacLeod
INTERVIEW
79 Medical Error in Psychiatry: An Interview with Dr. Robert Buckingham
Vahagn A. Karapetyan
82 UTMJ Interview with Dr. Amir Ginzburg
Katie Bies
85 Medical Error – A Discussion with Dr. Wendy Levinson Catherine Brown
87 UTMJ Interview with Dr. Brian Wong Meg Casson
90 UTMJ Interview with Dr. Kaveh Shojania Ilya Mukovozov and Kirill Zaslavsky
95 UTMJ Interview with Dr. Doug Weir
Matthew MacDonald
All articles are externally peer-reviewed with the exception of poetry and short stories and book reviews. All manuscripts are internally reviewed. Informed consent practices and any conflicts of interest are specified in the articles if applicable.
RESEARCH
99 The Use of EKG to Exclude a Diagnosis of Acute Coronary Syndrome in a Population with Low-Risk Chest Pain
Alexander Leung, Gaurav Puri, Vincent Ho and Steven Rhee
HEALTH POLICY AND ECONOMICS
103 Introduction to Cost-Effectiveness Analysis for Clinicians
Jennifer D. Cape, Jaclyn M. Beca, Jeffrey S. Hoch
106 US Drug Policy: Lessons for Canada
Daniel Heffner and David Moore
INTERNATIONAL HEALTH
110 Hepatitis B in Vietnam – A Crisis Waiting to Happen
Michael Mina
REVIEW
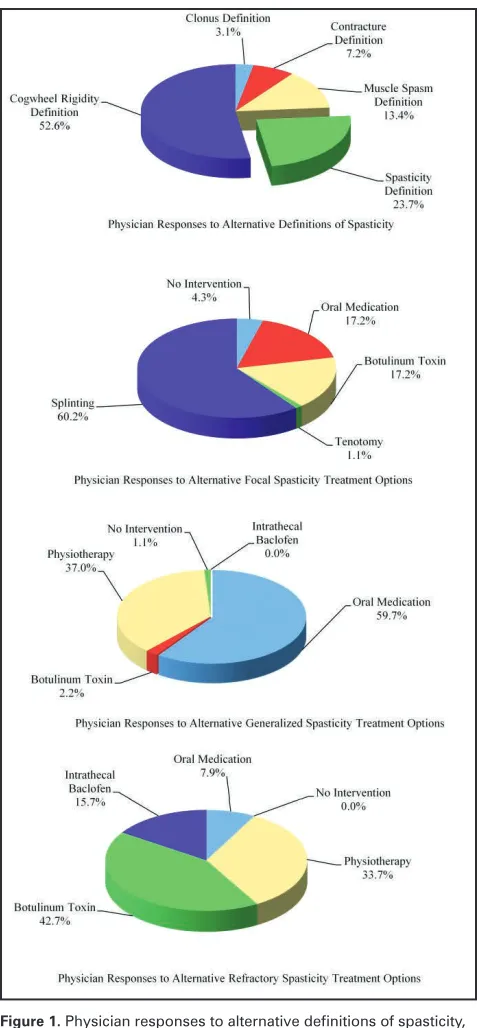
114 A Survey of Rural and Urban Family Physicians: Analysis of Spasticity Health Literacy and Availability of Appropriate Spasticity Care
A student-run scientific publication since 1923
University of Toronto Medical Journal
University of Toronto Medical Journal, 1 King’s College Circle, Room 2171A, Medical Sciences Building, Toronto, Canada M5S 1A8 E-mail: [email protected] • http://www.utmj.org • Phone: 416-946-3047 • Fax: 416-978-8730
Editors-in-Chief Ilya Mukovozov
Kirill Zaslavsky
Managing Editors Lucas Djelic Karim Virani Thomas Andrew Berk
Associate Editors Alex Cressman
Ahmed Faress Joel Davies Rosamond E Lougheed
Maria Jogova Alex Kumachev Vanda McNiven Jennie Giselle Pouget
Laura Stratton Arash Azin
Xin Wang Ethan Tumarkin Keith Gunaratne Michael D. Fridman
Caleb Zavitz Tenneille Loo
Copy Chief Tetyana Pekar
Copy Editors Andrew Arjun Namasivayam
Kevin Yau Meghna Rajaprakash
Pinder Sahota Catherine Brown
Natasha Correa Alexander Leung
Case Reports Editors William K. Chan James Thomas England
Reviews Editors Lawson Eng Sarah Levitt Jonathan H Hsu
Medical Education Editors Annie Liu Khaled Ramadan
International Health Editors Miliana Vojvodic Suparna Sharma Supreet Sunil
Research Editors Bailey Allison Dyck
Khaled Ramadan John Lee Mengzhu Jiang
News and Views Editors François Mathieu
Hiten Naik Marie Yan Jeremy Zung
Technology Review Editor Ayan K. Dey
Health Policy and Economics Alanna Wong David Chenhan Wang
Monali Ray Jesse Nathanael Kancir
History and Philosophy of Medicine Editors Elysia Adams
Jonathan Fuller
Interview Manager Meg Casson
Interview Editors Catherine Brown
Katie Bies Vahagn Karapetyan Matthew James MacDonald
Khaled Ramadan
UTMJ Lecture Coordinators Zamir Merali Igor Mihajlovic Mehwish Idrees
Webmaster Ritesh Gupta
The University of Toronto Medical Journal is funded in part by its subscribers and the Medical Society. Patronage to the Journal is sub-divided into five categories. UTMJ Friend – $75; UTMJ Patron – $75-99; UTMJ Advocate – $100-149; UTMJ Benefactor – $150-199; and UTMJ Grand Benefactor – >$200. To subscribe, please see the last page of the Journal.
The UTMJ wishes to thank the following patrons for their generous donations:
UTMJ Grand Benefactor
Dr. Barry Goldlist
UTMJ Benefactor
Graduate Life Sciences Michael Baker Hugh D. McGowan
UTMJ Advocate
Dr. Anne Agur
UTMJ Patron
Jay Rosenfield Kathy Siminovitch
Graham E. Trope
UTMJ Friend
Anne Agur Shabbir Alibhai
Edward Cole Helen Demshar David Goldbloom
Anna Jarvis Stephen Kraft Chetan Phadke Lannis Lee Tynes
Preface from the Editors
Dear reader,
W
e would like to cordially welcome you to our is-sue on Medical Error. Medical practice grows more complex every year and by its very nature, includes risk. The costs, both human and financial, are significant. According to the Canadian Adverse Events Study, at least 2.7% of the 2.5 million annual hospital visits result in ad-verse events attributable to preventable medical error. These events increase the likelihood of complications, prolong hos-pital stays and carry a staggering financial burden.Patient safety is a topic that is near and dear to the heart of every physician. Yet, in medical school this topic is seldom discussed. At the University of Toronto, we are privileged to have access to national leaders in the area of patient safety and quality improvement. To this end, we have interviewed several Canadian experts. Dr. Kaveh Shojania discusses the importance of system-wide design improvements to improve patient safety. In addition, he stresses the importance of team-work training in preventing medical errors. Dr. Brian Wong discusses the impact of evolving information technologies on medical education and patient care. He includes an over-view of the different domains of quality, with an emphasis on communication. Dr. Wendy Levinson, an expert in the field of physician-patient communication, discusses the relation-ship between communication and patient health outcomes. She includes a discussion of the cultural challenges faced by physicians in disclosing medical errors, or ‘near misses’. Dr.
Robert Buckingham talks about the kinds of medical errors
most prevalent in psychiatry and the mechanisms in place in hospitals to curb those errors. Dr. Amir Ginzburg describes the role of organization-wide cultural changes and medical education in bringing about improvements in patient safety.
We also bring forth an array of great articles. Leung et al. describe the use of an electrocardiogram to rule out acute coronary syndrome. Cape et al. offer an introduction for trainees to understanding economic evaluations. Further-more, they discuss the utilization of cost-effective interven-tions, allowing physicians to make well-informed decisions when choosing between different treatments for their pa-tients. Heffner and Moore describe the recent federal legisla-tion aimed at curbing drug related offences. Interestingly, they discuss how this legislation has the potential to nega-tively target marginalized individuals who suffer from drug addiction as a way to cope with trauma or mental illness. Michael Mina reviews the potential for hepatitis B infections to develop into a public health crisis in Vietnam and possible ways to prevent this from happening. Finally, Canning et al. report a distressingly low level of spasticity health literacy among primary care physicians, both rural and urban. They further report a paucity of health resources for spasticity care at the rural level and discuss the implications of these find-ings for patients with spasticity.
We hope you enjoy this issue as much as we enjoyed pro-ducing it. We would like to thank our entire UTMJ team, for without their hard work, dedication, and creativity this issue would not have been possible.
Sincerely,
Letter to the Editors
D
id you know that every year, thousands of people suf-fer preventable and unnecessary harm during their interactions with the Canadian healthcare system? Certainly, no one goes to work in the morning to make mistakes, but the fact remains that preventable errors do oc-cur. Not only do these mistakes have a profound impact on patients and their families, when you add them all up, the cost to a resource-strapped healthcare system in time and money is astronomical.This is where the Canadian Patient Safety Institute (CPSI) comes in. We were established ten years ago and are tasked with working with governments, health organizations, lead-ers, and healthcare providers to inspire extraordinary im-provement in patient safety and quality. We develop evi-dence-informed patient safety and quality products and services and customize them for the frontline, middle man-agers, senior leaders, and boards. We are backed by a faculty of hundreds of experts from all facets of the healthcare sys-tem and are supported and funded by Health Canada.
At CPSI, we have adopted ASK. LISTEN. TALK. as our mantra and have woven it into everything that we do. These three human concepts have also resonated with providers across the country.
Great healthcare starts with a question – ASK Great healthcare requires an open mind – LISTEN Great healthcare requires a responsive heart – TALK We also value the voice of the patient and bring them into the conversation via Patients for Patient Safety Canada, a patient-led program of CPSI. They work to ensure the voice of the patient is never drowned out in the din of the health
care system and are fuelled by the belief and the knowledge that there is no greater stakeholder in the effort to improve patient safety than patients and their families.
Over the course of the next five years, our strategic areas of focus include leading the establishment of a national in-tegrated patient safety strategy, knowledge mobilization and innovation to enable and sustain transformational change, building patient safety capability at organizational and sys-tem levels, and expanding reach by engaging all audiences throughout the system.
As medical students, the future of our healthcare system is in your hands and in your heads. The pursuit of knowledge and excellence is one that lasts a lifetime and you should never lose that sense of wonder and curiosity about the world around you or feel content that you’ve heard or seen it all. This is especially important in the medical profession where continuing education can be difference between a successful outcome for a patient and one that results in harm, and in some cases, death. After all, patient safety is about continu-ous quality improvement.
We have very bright people working in healthcare, some of the most intellectually gifted folks…. ”Knowing is not enough; we must apply. Willing is not enough; we must do”….Goethe
I encourage you to visit our website at www.patientsafety-institute.ca to learn more about who we are and what kinds of products and services we have to offer. For those who are active on social media, follow us on Facebook or on Twitter @patient_safety.
Preventing harm is worth the effort. We invite you to join us in making every patient experience safe.
CPSI Letter to the Editors
M
edical error is the ever-prevalent shadow that hangs over the vigilant practitioner. It is seldom discussed and often shunned because it is associat-ed with the concept of failure. The failure of a sole practitio-ner, however, may not be as alarming as a failure within the healthcare system. The great strides that have brought medi-cine into the modern age, turning many serious diseases into chronically managed conditions, have also inadvertently cre-ated an environment more prone to error. The compliccre-ated management strategies employing collaborative and inter-disciplinary approaches have generated additional avenues where things can go wrong. The accelerating progress rede-fines the medical literature and advances novel treatments has made it more difficult for physicians to stay up to date and compliant with the standards of care. Yet as technology integrates into the practice of medicine, an opportunity ex-ists to close many of these gaps. As cases of medical error are brought to the scrutiny of litigation, it becomes possible to better define the roles and responsibilities of physicians and improve the quality of care delivered to patients.Psychiatry offers a unique perspective on medical error, as it is a largely collaborative practice that involves the long-term management of difficult patients. In an interview with Dr. Robert Buckingham, the concept of medical error was discussed with a unique focus on the field of psychiatry. Dr. Buckingham attained his medical degree at the University of Western Ontario in 1968, and completed his residency in psychiatry at the University of Toronto in 1977. Currently, he serves as the Head of the General Psychiatry Program as well as the Clinical Director of the Department of Psychiatry at the University Health Network (UHN). He has a special interest in Mental Health Law.
UTMJ: What constitutes an error in your field?
RB: I think that there are two types of medical errors.
One is an error in judgement. Physicians are human and we sometimes make an error in our judgement. A misdiagnosis can be an error in judgement. The other type of error is negligence and the two types have a distinction legally. You must recognise that all physicians, including psychiatrists, can make an error in judgement, and you cannot be successfully sued for an error in judgement. But for an error that is negligent, you can be sued and pay damages. You
are expected to meet the standards of a reasonable physician, not the best physician but certainly better than the worst. So a lot of the medical legal cases revolve around what the standard for the reasonable psychiatrist would be when you’re looking at medical error. Those standards may be treatment guidelines, discussion of the risks and benefits associated with treatment, or appropriate follow-up care. There’s a whole set of standards that may go into the question of whether care met the standards of a reasonable specialist.
UTMJ: Would errors in judgement be distinct from
negli-gence in that they would still comply with the stan-dards of care?
RB: They’re basically one of degree. It’s accepted that
all physicians are human, and therefore they may make errors. As long as they have shown reasonable effort to avoid error, they are not liable for an er-ror. It’s when the evidence shows that they may not have been as careful as what the reasonable physi-cian would have been that it becomes negligence.
UTMJ: What kinds of errors that predominate in psychiatry?
RB: More than 50% of lawsuits against psychiatrists stem from the failure to prevent attempted or completed suicide. Others include incomplete disclosure of sig-nificant medication side effects, which is the same as in any area of medicine. But the prevention of sui-cide is the biggest one.
UTMJ: Is this unique to psychiatry?
RB: No, family doctors can get sued for it as well. It could be a failure to identify or manage a suicide risk. A psychiatrist, however, would be expected to be more proficient than the family doctor at assessing this risk, or the risk of a person with a mental disorder in harming others. A specialist training implies they have more expertise in their field, and therefore they are held at a higher level of standard than the family doctor.
Medical Error in Psychiatry: An Interview with
Dr. Robert Buckingham
Medical Error in Psychiatry: An Interview with Dr. Robert Buckingham
Interview
RB: The only difference may be that in the academic hos-pital, there are many more people involved in the care. Considering the medical aspect alone, there is the medical student, the psychiatric resident, and the staff person, so the risk of communication failing is higher. Each may be getting pieces of information, and if it’s not all put together, it can lead to error in decision-making.
UTMJ: What practices are currently in place to monitor
the prevalence of medical errors, minimize them or catch them before they cause an adverse event?
RB: The hospital has a number of mechanisms for
qual-ity review. Here, the important one is incident re-porting. If there is a medication error, or anything that generates concern, it can be qualified as either minor or something with more severe consequences. Severe incidences are reviewed at a number of dif-ferent levels, and the final review is by the Quality Committee of the Board of Trustees. So if there is a patient who is in active care and they commit sui-cide, there is an active review looking at the care the person received to try to identify systemic issues that need to be addressed, which perhaps contributed to the outcome. This is a constant process. Every hospi-tal by law is required to have Morbidity and Morhospi-tal- Mortal-ity rounds where there is a formal group that reviews serious outcomes of errors with the intent to avert future events. In the case of individual error, that is usually litigated, where one side will sue and try to prove that the standard of care fell below the expec-tation of the level of training.
UTMJ: How do you protect against underreporting minor
errors or lapses?
RB: It’s a matter of constant reminders to generate an
incident reports. In fact, there is a degree of under-reporting because it has to be initiated by someone, and many of the front line staff may decide that an event was not significant enough. However, there are certain errors that everyone is obliged to report in-cluding falls, medication errors, and any behaviour among patients that result in a degree of physical threat to staff, patients, or visitors.
UTMJ: Do you think this underreporting stems from a lack of recognition that an event occurred or from a fear of being identified as incompetent?
RB: I think it’s both. I think one way of improving the re-porting is to try to get across that it’s a non-blaming system. A lot of people may feel that they shouldn’t report because they feel it will make them look bad, which is human nature.
UTMJ: So then this is more a matter of degree than specificity?
RB: Yes, and that would be with any specialty. The gastro-enterologist would be held to a greater standard in diagnosing an illness of the GI system than the non-specialist. Each specialist brings their own level of expertise to the problem, and the level of their train-ing determines whether they have met the expected standards.
UTMJ: We have discussed errors in judgement from the
physician’s side. Are there medical errors that have their roots in the system or the patient?
RB: Yes, I mean certainly in any medical error, the pre-dominant omission may be with the physician or with the patient. But certainly with psychiatry, many patients don’t acknowledge they have a condition that needs treatment or they may not be necessar-ily compliant with treatment, and therefore they may get worse. Their psychiatric illness may make it more difficult for them to follow the treatment regimen. An inability to follow a treatment recommendation could be labeled it as an error in the individual. But there are also systems factors that go into errors. Particularly in psychiatry, I think that a lot of the treatment is multidisciplinary but communication between the system pieces may be faulty. Individuals with a serious psychiatric illness often have financial issues, housing issues, a number of nonmedical ports, and often the system doesn’t adequately sup-port them. I mean they talk about the whole area of mental health care being a non-system, in that you have these silos that don’t communicate well with each other. So transfer from hospitalized care to community care is a big problem with the system where error may occur. The team that’s responsible for picking up care in the community may not get adequate information from the hospital. Similarly, when individuals seek out emergency care, they usu-ally do not carry any information that is critical to their care.
UTMJ: Do you think Electronic Medical Records may help
alleviate these kinds of communication gaps?
RB: Definitely. In the emergency department, for
in-stance, being able to assess a patient at risk depends on your access to a lot of the past information, which is currently a challenge.
Medical Error in Psychiatry: An Interview with Dr. Robert Buckingham
UTMJ: How is medical education tailored to increasing
awareness of error in practice?
RB: Well certainly in psychiatry, at some point in residen-cy training there are seminars with a focus on avoid-ing medical liability, specifyavoid-ing the measures you need to take to minimize your risk of being sued and ensure that you meet the expected standard. By the time you finish and start to practice, it’s important to be aware of the standards so that you can monitor your own practice. If you don’t know the expecta-tions, it is difficult to self-reflect on the quality of the care that you provide.
UTMJ: What are some of the emerging solutions to manage
preventable errors?
RB: Mobile devices have allowed for rapid access to a lot of information on medication side effects and inter-actions, which may reduce the possibility of having a medical error, and students are becoming quite adept at knowing how to access that information. That’s probably the biggest development in the last several years.
UTMJ: Given your interest Mental Health Law, do you see
the legal system as a tool that can be used to mini-mize errors?
RB: Certainly knowing the cases where negligence was
proven and was not proven can help the individual psychiatrist better understand standards of account-ability. I do a lot of work as an expert witness in cases where I address what is expected of psychiatrists in the assessment of risk, and even though more than 50% of lawsuits that are initiated have to do with self-harm, the actual success is low. The importance of good documentation is a skill that really needs to be emphasized in the training of doctors. There have been many cases where I felt that the doctor’s care was adequate, but the documentation didn’t support it.
UTMJ: As these cases progress, do guidelines for physicians evolve over time?
Interview
D
r. Amir Ginzburg is a General Internal Medicine spe-cialist and the Medical Director of Patient Safety and Quality at Trillium Health Partners in Mississauga, ON. He is currently championing several organization-wide improvement efforts centered on avoidable hospitalization, patient safety education, and the spread of evidence-based order sets into the Long Term Care arena. Nationally, Dr. Ginzburg is a Master Facilitator for the Patient Safety Educa-tion Program Canada, a member of the Quality and Patient Safety Committee in the Canadian Society of Hospital Medi-cine, and a faculty member at the Canadian Patient Safety In-stitute. Along with other physicians, Dr. Ginzburg is working with the Royal College of Physicians and Surgeons of Canada to develop a curriculum to Advance the Safety of Patients in Residency Education (ASPIRE). He is very passionate about leading change, supporting a culture of safety, and align-ing physician governance of quality and patient safety with corporate strategic aims. Dr. Ginzburg is an Assistant Profes-sor at the University of Toronto’s Institute of Health Policy, Management and Evaluation, and he is helping to coordinate the implementation of health system funding reform in the Mississauga-Halton Local Health Integration Network.UTMJ: What sparked your interest in patient safety?
AG: For me, it was actually having a personal experience with medical error. My story goes back to when I was a resident. I was involved in a thoracentesis, which proved to be challenging. We positioned the patient appropriately at the side of the bed and we were all behind the patient facing the door. We did the tho-racentesis and we had a complication in that we hit an intercostal. As we were providing expert care to manage the complication, we noticed that there was a sign posted at the head of the bed that read “This pa-tient is on Enoxaparin” (a blood thinner). We quickly recognized that we had a more serious complication than initially expected. Going through this experi-ence was one thing, but seeing how the staff support around me responded was really what galvanized my interest in patient safety.
I was asked to present that case at patient safety rounds, which at the time was very forward think-ing. Traditionally these were morbidity and mortal-ity rounds – which was something very different from patient safety rounds. During those rounds, it became clear that I was not the first person to perform a pro-cedure on a patient that may have had a relative con-traindication because they were on blood thinners.
That’s why there was a big blue sign at the end of the bed – there had been similar instances and the hospi-tal had tried to make an intervention to mitigate fu-ture recurrences of that event. Recognizing that with human beings, being what we are – to err is to be hu-man, after all – the sign may have been a great idea. However, for certain procedures where you would not see the sign because of the patient’s positioning, that reminder might not work. The conversation then shifted from ‘blame and shame’ to supportive con-versation about how we support our patients and our team members to provide safer care and how can we add another layer of protection, to ensure that a so-lution improved the situation. For me, I found that conversation to be very forward thinking, and it was a very healing experience. That really pushed me into saying, that this was a really innovative way of think-ing about this. We often define ourselves as bethink-ing a physician – it is part of our core being, so when we do make a mistake, there is a lot of self-deprecation, assessment of self-worth, and a lot of guilt. This was a healing experience for me and led me to really con-sider this field.
UTMJ: After that experience, how did you become more in-volved in improving patient safety?
AG: Through residency and training, it’s often difficult
to explore these sorts of interests, and at the time (around 2001), there really wasn’t a formal curricu-lum to advance my own knowledge in this area, so it took a backseat to my clinical training for quite some time. When I became a staff member, I came out here to Trillium Health Partners (which at the time was Trillium Health Centre). As an internal medicine specialist and hospitalist, I started taking part in the fabric of hospital life as I had no outpatient practice. I wanted to really try and understand the inner work-ings of the hospital and how I could be a more valu-able team member. Opportunities started unfolding because of my involvement in multiple committees and trying to take active participation in trying to im-prove care. It started off with work on small projects and ultimately I became like a hub, bridging clini-cians and hospital administrators. Out of that came a formal role in advancing the quality of patient safety in the organization.
UTMJ Interview with Dr. Amir Ginzburg
UTMJ Interview with Dr. Amir Ginzburg
need to consider some of the simple things: dis-tractions, the working environment, the team functions, our organizational culture, and staffing ratios. All of these things require people coming together to determine what’s best for patients, what’s best for staff, and how we integrate across the continuum of care.
UTMJ: The concept of organizational culture is very inter-esting, especially given that medicine is a historically rooted profession, in which change can often occur slowly. Has Trillium Health Partners been receptive to improving patient safety?
AG: Trillium Health Partners has been on this journey
for over ten years. Even since 2005, when I arrived, there has been a palpable change to the front-line culture and to the organizational strategic priorities that incorporate patient safety and improve quality of care. If you ask other organizations in the health-care industry, you’ll hear that over the last 14 years, since the landmark report “To Err is Human” (from the U.S. Institute of Medicine), the whole industry has made immense strides in improving patient safety, but the culture piece evolves over time, it does not change overnight. Everyone is on a different phase of that journey. It requires perseverance and overcoming the historical aspects associated with this. Where medical and health profession education is going, I expect that there will be a new school of thought that will permeate through all of our profes-sions relatively quickly, and that will help transform the culture. Hopefully in a shorter timeframe than what has occurred over the past 14 years.
UTMJ: What do you think has been the greatest
advance-ment in terms of patient safety and reducing medical errors in the past 5-15 years?
AG: We have a more complete understanding of errors of
commission, where we misread a label or incorrectly program an intravenous pump. We have looked at the process of those errors, found the holes, and tried to put in new layers of protection to fill the gaps. We have many tools to help us, both in diagnosing and in implementing improvement and we have a national discourse around this. There are provincial organi-zations aimed at helping us and we have a lot of local improvement. I think the next phase of the discussion will focus on errors of omission. These are rooted in cognitive psychology and psychiatric literature. Why do we forget to order an antibiotic? Why do we focus on only one diagnosis rather than looking at other aspects of the differential and miss the opportunity to diagnose and treat someone early before compli-cations develop? Why do we allow these cognitive biases to affect our decision-making abilities? We will be looking at these errors of omission,
troubleshoot-UTMJ: Do you have a particular area of interest with respect to improving patient safety?
AG: Currently my interests are focused on patient safety education, which as a curriculum is best delivered in an interprofessional education environment. I am very lucky in that on the national level I am a master facilitator for the Patient Safety Education Program Canada through the Canadian Patient Safety Insti-tute. I get a chance to affect knowledge translation in this area to a wide audience, which I find rewarding and exciting. I am also very interested in avoidable hospitalization, particularly in readmissions. One of the key areas there that is relevant to clinical prac-tice is multiple hand-offs, especially as we transition people from the hospital to the community when discharging from the hospital to the home.
UTMJ: Are team members receptive to the team approach
to improving patient safety? Have there been any challenges in coordinating the involved parties?
AG: The mission of most care providers universally, is
to come to work every day to provide the highest quality and safest care possible. As each health care provider has this engrained in their profession, pa-tient safety on the whole requires engagement with a huge array of stakeholders. On any given issue, when we design interventions, we really focus on communication amongst the interprofessional team and ensure we have appropriate policies and proce-dures to support safety. There is no doubt that it is challenging. Every time we want to pat ourselves on our backs because we have completed a project and demonstrated success, we then have to sustain that success over time and keep chipping away at the tip of the iceberg in terms of enhancing our healthcare processes to improve the safety of patients, because ultimately our industry is almost completely rooted in human factors. Human beings make mistakes.
UTMJ: What have been some of the challenges you have en-countered?
UTMJ Interview with Dr. Amir Ginzburg
Interview
nities or requirements. Second, you have to have a passion. If you see an issue, it is very easy to be silent and just assume that someone else will take charge of it – either report it, discuss it with a mentor or staff person. It is very easy not to get involved as you’re busy and have competing interests, but participat-ing in these improvement activities can be one of the most fulfilling professional activities that people do. Look for these opportunities and it is as simple as expressing a desire to make things better. There are mechanisms in almost every hospital to have these interests cultivated and develop an improvement ac-tivity or participate in current programs. There are also formal and informal educational opportunities within U of T, including at The Centre for Patient Safety. In most U of T teaching sites, there is a dedi-cated physician leading safety/quality improvement within each department or in the hospital as a whole. There are lots of ways to get involved. We need to hear the voices of people delivering care on the front line at all levels of training and incorporate trainees, particularly in our training environments when we make improvement activity decisions.
There will also be a discussion at high levels as the Royal College revamps the CanMEDS roles about how to integrate patient safety competencies into these roles. In the near future, training programs will be incorporating these concepts and perhaps adding the requirement of a dedicated curriculum in patient safety and quality improvement. The culture is begin-ning to shift for the better.
UTMJ: Do you have any quick tips regarding preventing
medical errors?
AG: Communicate, communicate, communicate! Most
adverse events in health care are rooted in commu-nication failures amongst members of the interpro-fessional team. I would say to make communication among your top priorities in the common activities in which medical students and residents partake – particularly during hand-offs, either to each other or from hospital to home. Communicate safety concerns very clearly to members of the team and up the chain to residents or to staff, and do it in real time. People sometimes hesitate to voice safety concerns. It is of-ten the voice of the person who expresses a concern but feels low in the medical hierarchy that is able to stop everything as they were the only person who saw an error evolving. Sometime it can be hard with our training hierarchies to be that voice, but I would say that if you see something that is concerning, take the initiative and express it. No one would ever fault a medical student or a resident for expressing a patient safety concern. In fact, I think our culture has gotten to the point where this is a behaviour that should be modelled and celebrated. It’s easy not to speak – but I would suggest speaking up!
ing, and trying to support physicians in recognizing cognitive biases and providing better bedside tools to improve safety.
UTMJ: Do you think electronic tools such as Electronic Med-ical Records that warn you about possible contraindi-cations when you prescribe a drug will help or be a hindrance in the future?
AG: The jury is still out on that. There is absolutely a
role for clinician decision support tools at the point of care, but we have to be very careful in designing them. We have to be aware of “alert fatigue” and if we develop all of these alerts, we can just as easily start ignoring them. In a busy practice environment, a clinician has a certain amount of time in which to see a patient, diagnose, write orders, and input them into an electronic system. If they are being bombard-ed with copious different alerts during the process, there is a high likelihood that a significant portion of those alerts will be ignored and turned off. If a culture develops around “alert fatigue” where these alerts just get ignored, will clinicians pay attention to that one critical alert? We don’t know. We also don’t always think of the downstream consequences when we rush to a technological solution to improve pa-tient safety. There have been incidences in the litera-ture where technological solutions have led to worse outcomes because of consequences that were not pre-dicted when the technology was developed. Again, this comes back to the human interface with ogy – human factors”. Implementing this technol-ogy requires a lot of careful thought and tremendous education. It requires monitoring, tracking changes and issues, and resolving these issues. We will see the interface between technology and medical practice in the future; we will just have to design these interven-tions very carefully.
UTMJ: Do you have any recommendations for medical
stu-dents or recent graduates regarding how they can be-come more involved in patient safety initiatives?
AG: Within the University of Toronto, and many other
opportu-Medical Error – A Discussion with Dr. Wendy Levinson
Interview conducted by Catherine Brown, MD Candidate, Faculty of Medicine, University of Toronto
D
r. Levinson is the Sir John and Lady Eaton Profes-sor and Chair of the Department of Medicine at the University of Toronto (U of T). She is an expert in the field of physician-patient communication. Her research includes the relationship of communication to patient out-comes, how communication breakdowns can influence medi-cal malpractice, and the effectiveness of primary care phy-sicians and surgeons in helping patients to make informed decisions. Her current research focus is on disclosure of med-ical errors to patients. She earned her bachelor’s degree from U of T and her medical degree from McMaster University.She is a member of the American Board of Internal Med-icine (ABIM) Foundation’s Board of Trustees and is a past Chair of the ABIM’s Board of Directors. She is the Chair-elect of the Association of Professors of Medicine and a past Presi-dent of the Society of General Internal Medicine.
We had the pleasure of interviewing Dr. Levinson recently regarding her thoughts on medical error.
UTMJ: There seems to be a constant stream of stories in the lay press about medical errors. Do you believe that the number of medical errors is increasing or are we getting better at talking about them?
WL: I think there have always been medical errors. We just didn’t pay much attention to it until the American report To Err is Human: Building a Better Health System, which by the way is more than 10 years ago. That report published by the Institute of Medicine really started to study the epidemiology of medical errors, and I think it set the stage for changing the conver-sation. They made it lay, understandable. They talk about this being the equivalent to a jumbo jet crash-ing every day. One of my Canadian friends works in errors and patient safety, Dr. Kaveh Shojania, says in Canada that’s the equivalent of a Greyhound bus go-ing off the road. But I think it made it accessible to understand the magnitude of the problem, and so it really led to a major shift in hospital care to look for the common causes of error and look for systems to prevent them.
UTMJ: You write that disclosure of medical errors is a very difficult conversation for physicians – especially since they often fear litigation and have little training in disclosing errors. How can we encourage physicians to disclose medical errors? How can our institutions better support effective disclosure?
WL: First of all, before I talk about the institutional part, I want to address the individual physician. Physicians are sort of perfectionists. They have been groomed to excel through rigorous education, and I don’t think we’ve built into the culture talking about mistakes, in general. It’s not a culture that’s fostered that. I think up until the To Err is Human report, we had all these errors, but we just never talked about them. And typically if we made mistakes, I think people actu-ally kind of hid them. They saw them as individual errors; they didn’t see the team approach or the sys-tems problems that led to the errors. Not that there aren’t individual errors too; a physician can make mistakes. So we built a culture of silence, and not only silence, what people talk about in the early er-ror movement is shame and blame. When people did make mistakes, they were chastised for it, so people really didn’t talk about them.
Medical Error – A Discussion with Dr. Wendy Levinson
listen to those tapes, you would not think they were stellar. In one tape I remember I listened to, I said to the person working with me, “Which scenario did we give this guy?” because I could barely tell what he was talking about. It was so uncomfortable for him so he was using jargon, which made it very confusing. Ac-tually, to the standardized patient’s credit, they said, “I’m a little confused,” which they should have been. So I think it’s very difficult.
Now shifting to the system, hospitals throughout North America have started to develop systems to support error disclosure, support the providers, and coach the providers so that they can learn from the mistakes. In the States, the commission that accred-its hospitals requires that systems be in place to deal with errors and to disclose them to patients. So not only have physicians – and not just physicians, but nurses – developed more skills, hospitals too have de-veloped support systems for that.
UTMJ: What do patients want when physicians are disclosing an error?
WL: We did research on this quite a number of years ago. We ran focus groups and talked to patients, and it’s very clear what patients want. They want to know exactly what happened, in plain and clear language without jargon. They want to know the consequences of the problem for them. They want an apology. They absolutely want an apology. They do not want people to pretend it didn’t happen or to be indirect. We tell people that expressing regret, “I’m sorry this happened to you,” is okay initially until you real-ly acknowledge that it was an error, and then you re-ally need to apologize, which is different than regret. Apology takes responsibility, so it’s not enough to say, “I’m sorry this happened to you.” Patients want, “I’m really sorry that I caused you harm,” “I feel terrible about it,” or “It was my fault.” The other thing they want – that physicians don’t always recognize – is to know that we will learn from this mistake: “Because this happened to me, you and the other providers will do something so another person does not suffer from the same problem that I just had.” That’s very clear. That’s the one good thing that can happen out of this is that you will learn from the mistake and not let it happen again.
UTMJ: There seems to be less of a consensus as to whether physicians should disclose near misses. Do you think physicians should regularly disclose near misses as well as medical errors?
WL: It’s interesting because in other countries, disclosing near misses is part of the practice. I once gave a talk
and brought up near misses and asked if anyone had disclosed a near miss. Two people put up their hands. I said, “Where are you from?” and they said, “Austra-lia.” In some places, the concept is that if you disclose a near miss, that’s an opportunity for learning even though the harm didn’t occur to the patient. But on the other hand, I always joke that you don’t want to have someone run into your hospital room saying, “Oh, Mrs. Jones, I nearly did this or I near-ly did that.” It obviousnear-ly has to be selective. It’s not the standard of practice in the US or in Canada to disclose near misses. It’s interesting to think about whether it would be helpful in terms of quality im-provement. For instance, “Mrs. Jones, fortunately we did not give you the wrong medication, but be-cause your name was the same as someone else on the ward, we nearly did. We are trying to understand how we can make sure that doesn’t happen. We have a couple of ideas. Can we talk to you about that?” That might be very useful. “Mrs. Jones, would you be willing to stop the nurse before she gave the medica-tions and say ‘I’m Betty Jones; I understand there is a Maxine Jones on the floor.’ Would you be willing to do that?” So you can engage patients in thinking about error prevention if you use near misses, but it is not the standard of practice in North America.
UTMJ: Disclosure in health care has progressed a long way since the 1960s when physicians would often with-hold diagnoses for serious illnesses such as cancer. As we move forward, how can we continue to build a transparent culture for disclosing and learning from medical errors?
WL: I think it’s some of what we talked about already. It’s about building a culture. It’s about having institution-al support and education that support it. I would say it’s embedded in a broader societal change, which is a movement towards transparency.
UTMJ Interview with Dr. Brian Wong
Interview conducted by Meg Casson, MD Candidate, Faculty of Medicine, University of Toronto
D
r. Brian Wong’s is an Associate Scientist, of evalua-tive clinical sciences, in the Veterans & Community Research Program at Sunnybrook Research Institute, is an Assistant Professor in the Department of Medicine at the University of Toronto and is staff physician, general in-ternal medicine, Sunnybrook Health Sciences Centre. His research foci include improving in-hospital communication using information technology, reducing in-hospital paging errors, adverse event surveillance and transitions in care. Dr. Wong also conducts research in the field of medical education where he focuses on disclosure of medical error and the best approach for teaching quality improvement.He is also involved in medical education research. He was the principal author of a systematic review and a state-of-the-science review, which summarize the best evidence for how to teach quality improvement and patient safety to residents and medical students. Current research focuses on teaching error disclosure skills to residents, and evaluating the impact of a co-learning model on resident and faculty learning about quality improvement.
UTMJ: You work as General Internist at Sunnybrook Health
Science Centre and are an Associate Professor at the University of Toronto in the Department of Medi-cine, but also conduct research on patient safety and quality improvement. How did you come to focus your research in these areas?
BW: Like many students and residents, it started for me when I started looking after patients. When you are looking after patients, in the trenches, you see how things work and you start to realize that things could work more efficiently. You start to see that often you need to work around the system and within the sys-tem. I initially had this naive notion that I could fix things quickly, and I thought it would very straight-forward, but I realize very quickly how challenging it can be.
For me it went back to when most of us did not carry cell phones, we did not text each other or use smartphones at all. I had several experiences of missed pages and pages going to the wrong the wrong person. I remember being on-call one time and not getting any pages for almost six hours. This was back when pager numbers were just written on a white board, and my number had simple been mixed up by a couple numbers so I was not receiving any pages. I felt bad- there was a delay in care and it was mak-ing it more difficult for other people to be effective in their work. Pages back then were numeric so you could be in an important meeting with a patient and their family or doing a procedure and you wouldn’t
know whether you should call back right then. We had an idea that it would be great to receive a text message on your pager because it would give more information than just the number to call. It may seem archaic now, but back then there wasn’t Blackberry Messenger, or iChat, nor was there the ubiquitous use of the technology like there is now. This project came up very serendipitously. When I was chief resident at Sunnybrook Health Science Centre, a hospital health informatician, Sherman Kwan, hired by the Depart-ment of Medicine, approached me with twenty new text pagers given to the hospital to try out, and the project built from there.
Ultimately, the focus of my research came from the convergence of my own lived experience and frustra-tion of inefficiencies, in addifrustra-tion to having someone come by with an opportunity and running with the idea. I fumbled my way through but it was fun and something that was meaningful. And in contrast to other research I had done, you could see the progress unfold in front you. It was really nice to make changes that helped to make people’s work more efficient and more enjoyable.
It is very easy to assume that new technology is perfect but in reality the benefits of smartphones and similar technologies can be a bit of a “double edge sword”. They allow instant access to other people but there are also many unintended consequences, for which I think we need more oversight. For example, we are starting to see students using these devices during teaching sessions and during patient encoun-ters people are using these devices and we need to clarify what is the professional conduct that is neces-sary. Including in many hospitals can be connected to the EPR [Electronic Patient Records] and you could be looking up patients’ records or something similar, but the patient will not necessarily know why you are looking at your phone. We need to establish how to communicate what you are doing to patients and col-leagues. There is definitely the need for faculty devel-opment in this area. In addition, such technology can be very interruptive and we know that interruptions contribute to medical error. While they may make some task more efficient or some aspects of com-munication more effective you need to consider the influence of these types of interruptions on patient encounters and care.
UTMJ: What are the main challenges in identify sources
UTMJ Interview with Dr. Brian Wong
Interview
some of our procedures and diagnostic tests, treat-ments.
I think the tension you are referring to is one that I consider as a tension between different domains of quality. For example, in the emergency room there is a big push for patients to be seen in a timely matter, especially if you have a serious problem. Through the quality improvement lens you could say that this is about improving timely access to care, or even safety because you do not want someone with an undiag-nosed problem to go without an assessment for a prolong period of time. In this case you would re-ally work to decrease waiting times by improving flow and create new incentives in emergency rooms- as we have done [in Ontario]. But sometimes these solu-tions put other components of quality at risk. For example, one solution proposed for reducing wait times and overcrowding in emergency rooms is mov-ing patients out of waitmov-ing rooms into hallways. Many argue that it is not patient-centered to be in a hall-way, unwell and in a gown, and some even argue it is unsafe (though there is limited evidence for this claim). But some hospitals have implemented these or similar policies, like sending patients to a different hospital, to reach the goal of improve waiting times. This tension, and the unintended consequences of quality improvement initiatives, comes when trying to improve one part of our system but creating new problems in other areas. But there is no doubt in my mind that we will continue to talk about value and cost in the future.
UTMJ: What is the role for scientific or clinical research in identifying and un-packaging these issues?
BW: There is an idea basic science helps understand mechanisms and what works and what does not work, and then the applied research is about taking this knowledge to the bedside. Quality improvement is similar in that research is needed to do large studies to identify the problems, like adverse events in hos-pitals or extended wait times in the emergency room, but you also need these people to do the actual qual-ity improvement “in the weeds” and to work through how to address the problem once it is identified. But quality improvement whether it is called “research or “practices” “research”, or practices if you will, are based on a different paradigm compared to tradi-tional health services research or evaluative research. For example, this paradigm includes discussion of rapid cycle changes, and collecting small amounts of data continuously over time. It includes more trial and error, and making small, incremental changes rather than implementing large scale changes. A lot of this is taken from industry, from such as engineer-ing, airlines, and the nuclear industry, and we are learning how to make our processes more reliable.
BW: There are a number of different ways we know about error. There is a helpful commentary on this topic by Dr. Kaveh Shojania titled “The Elephant of Pa-tient Safety”. It is based on the fable of the five blind men who are all touching an elephant at different parts and depending what part of the elephant they are feeling (the tusks, the body, the tail etc.) they are convinced they are touching something different. In some ways detecting medical error is like this in that depending on how you try to find these problems in-fluences what is identified.
There are a lot of different ways that institutions try to find such problems. One way is through in-stant reporting systems, in which staff voluntary re-port problems. Another is through executive “walk-arounds” where executives actually walk around the hospital and interview people and make observa-tions. A final example is referred to as “trigger tools,” in which you randomly select charts from patients that have been discharged from your service and you look for triggers, like for example a blood transfusion or new antibiotics started partway through an admis-sion, then you review admission and discharge, and then examine whether there were any problems with the care provided. It is now clear that while there are many tools available, no one tool will identify all your problems, but ultimately a combination of tools will provide an overall description of the major problems. Interestingly, I think we have a pretty good sense actually of what the main sources of problems and errors are; most are related to medications, commu-nication failures and procedures. Coming up with so-lutions and interventions is not as straightforward as we had hoped, but rather it is about implementing complex interventions in complex environments- it is like taking a multifaceted intervention onto different wards with different layouts, different.
UTMJ: Quality improvement and reducing medical error
has gained considerable attention over the past de-cade. In today’s economic climate however, there is a tension between quality and safety on the one hand and efficiency and cost-effectiveness on the other. Have you observed this tension?
UTMJ Interview with Dr. Brian Wong
are other skill sets, those of advocate, manager and collaborator for example, that need to be addressed. There are some instances when these areas can be combined and taught at the same time, but there is a real capacity issue as to what can be put into a cur-riculum.
I have gone back and forth on these questions. We have taken the approach of integrating things as much as possible into practice through general rounds, or teaching while on the wards, because the teaching quality improvement and the principals of patient safety can be integrated into daily work. Stu-dents pick up on how staff behaves and if we as clini-cians are respectful, do not perpetuate professional hierarchies and are reflective of our work, students will learn through our examples. I do believe how-ever there are some basic concepts that can be best conveyed through lecture and we have been putting more formal training into the curriculum like qual-ity improvement projects for trainees and web-based modules.
UTMJ: What projects are you currently working on and what direction is your research on patient safety, quality improvement and medical error taking?
BW: I am continuing with my research on training in qual-ity improvement and patient safety. The first phase was figuring out what are the best models for to teach these concepts. The second phase is developing fac-ulty so that there is a group of people who are inter-ested in teaching on quality and patient safety, and building the curriculum and teaching resources fur-ther. It can be problematic to only have a few people teaching as it limits the perspectives given. So we are trying out different models of engaging faculty on these topics. A new model we have had success with is a shared teaching environment with faculty and senior residents learning at the same time. In this model, faculty and senior residents attend the same workshops and collaborate on projects. The initial participants’ impressions have been positive and we are continuing to build and make improvements. I have always wanted to be involved in teaching and have developed expertise in this area so that I am able to teach. I am very interested in the intersection between patient safety and medical training, such as resident workload, handing over care between and students and how students experience medical error (the idea of “second victim”- the idea that the first victim is the patient and the second victim is the pro-viders who are also affected by medical area) and dis-closing errors. We even hope to extend this to how we deliver continuing education so that we can bring in more quality improvement for practicing physicians. What I really like about my work to date is that at times it is more on the education side and at others it is more on the research side; but at the moment it is very much integrated.
UTMJ: You have identified communication as a key
compo-nent to quality and patient safety. What are the other components of a system or teams that are important in minimizes medical error?
BW: There is a lot of literature around optimizing team-work such as a “shared mental model” or “situational awareness”, but I my own lived experience, just like in any other work that you do having clear lines of com-munication and expectation setting are key. For ex-ample, I always set out clearly guidelines with all my students as to when to get in touch with me or when to call when they are uncertain or if a patient is sick, so that they do not have to wonder about whether to call or worry about the implications. I also get to know from them what they are comfortable with and when they are uncomfortable.
As a team, considered workload is an important is-sue. If residents have too many patients to look after for example, not only does is their quality of educa-tion degraded but their ability to funceduca-tion effectively is degraded, and their attention to detail and care they provide will decline. It is important to help to teach residents and students manage the workload and make changes if it is too much, as well as to pri-oritize tasks.
UTMJ: You have also written extensively on medical
edu-cation and teaching medical students and residents about quality improvement. What is the importance of addressing medical error in undergraduate medi-cal education and at the residency level, and should it be formally addressed in the medical school cur-riculum?
BW: You will think that I will say “Yes, we should abso-lutely it has got to be in the curriculum”. There is no doubt in my mind that we as health care practitioners need to be component in systems thinking, quality improvement, reflecting on your own practice We should be incorporating this into in our practice and we should all be engaging with it.
Interview
D
r. Shojania joined Institute for Clinical Evaluative Services (ICES) as an affiliate scientist in 2008. He is a general internist at Sunnybrook Health Sciences Centre and Director of the recently established University of Toronto Centre for Patient Safety, a joint collaboration be-tween the Faculty of Medicine, Sunnybrook, and Sick Kids Hospital.Dr. Shojania’s research focuses on identifying evidence-based patient safety interventions and effective strategies for translating evidence into practice. His work has appeared in leading journals, including New England Journal of Medicine, Journal of the American Medical Association, British Medical Jour-nal, and Canadian Medical Association Journal. Dr. Shojania has delivered invited presentations on patient safety to the US Institute of Medicine and holds a Tier 2 Canada Research Chair in Patient Safety and Quality Improvement.
UTMJ: Could you tell us a little about the history of the field?
KS: People have been talking about the need for quality improvement for a long time, especially in the last thirty years. There were some prominent academics working in the field and they got tired of nobody lis-tening to them. So in the late 90s, they published a report with the Institute of Medicine called “To Err is Human.” There were headlines in major newspa-pers claiming that “medical error kills 98000 patients per year in hospitals alone,” which would make it the 8th leading cause of death, beating out breast cancer and motor vehicle accidents. While it turns out those numbers may not have been entirely accurate, they did grab everyone’s attention more than something like “people are not getting vaccinated” or “people with diabetes aren’t getting proper chronic disease management.”. Shortly after publication, President Bill Clinton signed the “Healthcare Research and Quality Act of 1999,” which provided over 50 million dollars in appropriations for newly expanded Agency for Healthcare Research and Quality. This really ush-ered in the era of studying quality of care and patient safety.
UTMJ: What is your working definition of “medical error”? KS: I don’t know if I would use the term “medical
er-ror” anymore. Most of us have switched to terms like “preventable harm” or “preventable adverse events.” It’s usually the failure to do something you’re sup-posed to (error of omission) or doing something in
the wrong way (error of commission). Adverse event commonly refers to iatrogenesis. It’s a Greek term meaning “coming from the healer.”. Preventable ad-verse events are mostly due to errors. The advantage of not using the term “error” comes from not getting others to feel defensive. Sometimes, the “error” is a systems problem. It is a little difficult to refer to some things as errors when there is not a specific human individual who made the error, but, for example, a computer glitch. It would not be right to call that an error; it is more correct to use the term “preventable adverse event.”
UTMJ: Does that encompass patient non-compliance or is
that a separate issue?
KS: That’s an interesting example of a quality problem. The most commonly used definition of quality in-cludes six dimensions. Patient compliance can be regarded as another dimension. Historically, physi-cians would blame the patient. However, there are a lot of examples where non-compliance reflects the failure on our part to explain things to people prop-erly. For example, a lot of people with hypertension may think that if they don’t experience any symp-toms like headaches then they’re fine and don’t need to take anything. If you don’t explain to them that hy-pertension means high blood pressure that persists even in the absence of any symptoms, then this might then not be only a patient issue. Calling this a patient safety issue or medical error doesn’t seem quite right – it is in the grey zone and definitely a quality of care problem.
UTMJ: Why are you personally interested in studying medi-cal error? How did you begin in the field?
KS: I had a mentor while doing residency at Harvard Uni-versity. At the time, he was not famous, but eventually made a name for himself in the field by advancing computerized entry of medication orders. I also did some early work to prevent errors during autopsies. In addition, I had a personal incident: when I was an intern in my second month, there was a 29-year old guy with an atypical presentation of a heart attack that was missed by the ER department.
So I started to think: it’s fine to advance some new drug, but most new therapies don’t really work or only work a little bit. On the other hand, one can
UTMJ Interview with Dr. Kaveh Shojania
UTMJ Interview with Dr. Kaveh Shojania
blame would be on the last person to see the patient. We know now that that’s not really right. They may be competent but working in dysfunctional system. So we might need to also look to changing the cul-ture.
UTMJ: What do you think is the bigger source of errors: hu-man error or systems error?
KS: The short answer is systems problem. Some of the valuable lessons to draw in patient safety come from other high risk industries (Aviation, nuclear power). In those industries, the idea that human error is in-evitable has been around for longer. There are two basic types of errors that are useful to distinguish. One is the one we always think of, but is actually not as common, is a cognitive error – doing the wrong thing. For example, misinterpreting an X-ray or making a calculation mistake. What’s more common is a slip: you’re doing something you know how to do, but either because you’re distracted or tired, you accidentally do the wrong thing. A greater burden of errors in medicine comes from slips.
The solutions to these types of problems tend to be rooted in design. There is no point talking about getting rid of human error. As long as we have hu-mans, we will have human error. The problem is that the field of medicine generally has not recog-nized that. What we need to do is design a system that allows human error to happen but be trapped or stopped before it reaches the patient.
The solution to most human errors is not more knowledge. It comes from understanding what types of situations give rise to predictable human errors.
UTMJ: Building on your comments about medical culture: as medical students, we have little exposure to the topic of medical error early on. What role do you think undergraduate medical education should be playing in discussing this topic?
KS: Lots of schools still teach nothing about medical error. University of Toronto has something in the Transition-to-Clerkship Period that I used to teach. There is one day where you do some case-based and didactic learning. We do the case-based stuff because we know that medical students are nervous before they go on the wards and want to know the very ba-sic things – what pneumonia is, what a heart attack is. So, we have some nice bread and butter medicine cases that involve interesting errors and we discuss both the clinical parts of the case and the errors. I definitely think people should be exposed to medical error cases in medical school. On the other hand, some schools have tried to introduce it too early. Until you’ve actually been on the wards for a few months, have seen how chaotic it can be, and how prevent more harm and save more lives by improving
the problems in the delivery of care that we already know about. So, as someone who liked the clinic but was also interested in academic medicine, I thought this was best way to do something useful in improv-ing care.
UTMJ: What are the most common sources of medical error?
KS: That depends what you mean by “sources.” You can categorize medical errors into clinical categories (di-agnostic, medication, complications after surgery, nosocomial infections). Some of these are not really “errors,” but rather indicate that, for example, we might do better in preventing patients from getting C. difficile infections or ventilator-associated pneumo-nia. These are preventable harms from medical care. Now, for some of these, you can find concrete causes. Messy handwriting is a famous example but it actually doesn’t cause that much harm, as there are many other prescription errors. There are deeper causes like communication and teamwork problems, or poor design of equipment and processes – things that we haven’t thought much about historically. Research in medical error has gone along two different pathways. One is where you take a specific common complication like infections and try to come up with specific things to prevent it. The other is where you look at more cross-cutting causes, such as poor teamwork or communication between doctors and nurses on the wards or between doctors of differ-ent specialties. Both approaches have merit and have made advances.
Historically, one of the ways medicine has made progress was by having a certain professional ethos where the doctor did everything for their patient and if anything went wrong, it must be because the doc-tor didn’t try hard or know enough. We don’t want to erode the professional ethos, but on the other hand, it’s unrealistic to hold this view now. Almost nobody is taken care of by a single person and nobody can have all the knowledge in the world. Even when you have a person fitting these criteria, there are so many system problems that even a competent person could make errors. For example, poorly designed medical records where you can accidentally write things in the wrong chart or order something for the wrong pa-tients aren’t issues of knowledge or skill. There has been progress in thinking about these cross-cutting problems, including addressing the culture and the ethos of medicine where people feel comfortable in talking about their errors.