Preface
Preface from the Editors
I
t is our pleasure to bring you the second issue of the UTMJ for the 2011-2012 academic year. In this edition, we sought to discuss an exciting topic often encountered first-hand by health care providers and the general public alike whether living in large cities or small rural towns and villages – Trauma.The word trauma can conjure a diverse array of images to different individuals, ranging from local news broadcasts of violence, motor vehicle accidents, to environmental or man-made global disasters encompassing large scale weapons use and natural catastrophes such as tsunamis and earthquakes. Underlying all these images is the central notion of unantici-pated injury and damage to both the body and mind.
A thought that often does not immediately come to mind is the role of physicians and healthcare providers at the front lines of such traumatic events. Trauma from the healthcare perspective is managed by a diverse, multidisciplinary team under the organization of the Trauma Association of Canada (TAC) serving below the governance of the Royal College of Physicians and Surgeons of Canada.1 The goal of the TAC is to
promote injury control and excellence in trauma care.1 The
proper management and reaction to traumatic incidences is of utmost importance, given the fact that injury stands as the most common cause of death in the first four decades of life and costs the Canadian economy roughly $4 billion annually.1
In Canada, the distribution of trauma cases is allocated to regional trauma systems consisting of one or two trauma centers, each of which are based on a population of 1-2 mil-lion people and serve to consolidate major trauma caseloads.1
These regional trauma systems are largely independent but work together towards a coordinated, common provincial trauma plan.1 On the front line of trauma management
works the emergency medical services (EMS), whose function is to prevent further injury, initiate resuscitation, and pro-vide timely transport of injured individuals to the appropri-ate trauma center.1 Via the EMS, patients are transported to
the appropriate trauma center, which are numerically classi-fied (I-IV) as adult and pediatric centers.1 Collectively, these
trauma systems provide a comprehensive and coordinated process of injury control that reduce mortality and morbidity associated with injury.
To start off our Trauma issue, we present a guest editorial from Drs. Harris, Cadotte and Fehlings on the management and exquisite challenges of traumatic spinal cord injury, in-cluding an exploration of current and future therapeutic developments aimed to reduce the negative long-term conse-quences of such injuries.
In Letters to Editor, Brander speaks about her experience carrying out a rural medical elective in Botwood, Newfound-land. She frames her experience by the concept of “clinical courage”, which she defines as a question that requires physi-cians to ask themselves “How far do I trust my skills? How soon do I hand over responsibility of a patient?
We believe the concept of clinical courage underscores two key aspects of managing trauma. The first is the confi-dence that a physician must have in their ability to provide quality patient care in a setting where time and other resourc-es may be limited. The second is the importance of recogniz-ing one’s limitations and actrecogniz-ing to mitigate its impact on the care of the patient.
In the News & Views section Hamilton reports on a press-release about stopconcussion.com, an online concussion and neurotrauma educational and awareness hub for all sports, designed to address the growing trend of concussions in sports. One of the topics of focused on at the press-release was growing popularity of baseline testing. Baseline tests col-lect normalized characteristics of an athlete playing in the sport, which can then be used to aid in the assessment of a concussion by comparing their post-impact function to their pre-impact function.
Next, this issue features two excellent interviews. First, the UTMJ brings you a conversation with Sunnybrook trauma sur-geon and associate professor at the University of Toronto, Dr. Peter Chu. Alongside an exciting career in trauma, Dr. Chu travels each year to Niger, West Africa to volunteer his surgical services at Galmi Hospital. In this conversation, Dr. Chu sheds light on the field of trauma surgery in an epicenter such as Toronto and provides insightful advice for interested medical students and professionals alike.
Second, we feature a transcript of the first ever broadcast of Radiology, a new air show designed to bring interesting and clinically relevant issues to medical students. In the transcript, MacDonald interviews the infamous Dr. Philip Hébert, author of “Doing Right: A practice guide to ethics for medical train-ees and physicians.” Herein, MacDonald explores some inter-esting and stimulating questions with regard to Dr. Hébert’s text.
In the Quick Diagnosis section Levy and Barankin describe the diagnosis of a patient with dermatomyositis. They place emphasis on the clinical presentation of dermatomyositis, es-pecially on several associated dermatological features, as well as the prognosis and treatment of this condition.
Preface
undergraduate medical curriculum, as reviewed by Hartung, Henriques and Nyhof-Young. In this article, readers can find in-formation on the skills medical students can acquire with re-gard to patient spirituality, with recommendations for imple-mentation in the medical curriculum.
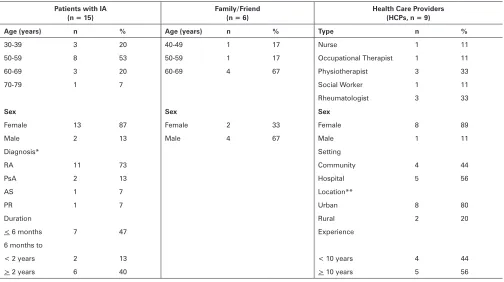
Next, Olsen and Schemitsch explore the interesting roles of gender and socioeconomic status in patients living in To-ronto undergoing hip resurfacing arthroplasty as opposed to total hip replacement. Continuing on in our Research sec-tion, Tran, Nyhof-Young, Embuldeniya, Veinot, Diamandis, Das, Cho and Bell examine informational and emotional support needs of elderly individuals living with inflammatory arthritis, including insightful advice from health care providers regard-ing peer-to-peer mentorregard-ing and peer support programs.
In Health Policy and Economics, Chadi argues that break-ing the taboo surroundbreak-ing physicians’ rigid scope of practice is an innovative way of increasing the cost-effectiveness of the healthcare system. The author proposes that this would pro-mote a stronger and more integrated multidisciplinary ap-proach to medicine. Furthermore, this article discusses the potential role of nurse practitioners and physician assistants under this integrated scheme.
Microfinance loans have been shown to be effective at ducing poverty in low-income countries by empowering re-cipients to start small business ventures in their communities. In the Global Health section using an example of pediatric burns from rural Nepal, Chan and Izadi, discuss the potential
for microfinance loans to reduce injury rates. The authors also discuss the challenges of implementing effective injury prevention programs in this setting.
In the following section Yang uses poetry to present a unique insight on the experience of a man who is having a heart attack. While the poem “Old Movies” juxtaposes the dis-crepant images of the human body.
We hope that this issue has piqued your interest on the topic of trauma. We would like to thank our editorial staff for their effort on this issue. We would also like to extend a very special thank you to all the faculty members who take the time out to help us review submissions to the UTMJ. Your assistance is pivotal to our success! In addition, we would like to thank our faculty advisors, subscribers and advertisers for their support. Last but not least, thank you to all our readers; we hope you enjoy the March issue of the UTMJ!
Sincerely,
Bailey Dyck and Sheron Perera Editors-in-Chief
REFERENCES
Guest Editorial
Emerging Trends in the Management of Spine Trauma and
Spinal Cord Injury
Michael G.Fehlings, MD, PhD, FRCSC, FACS, Division of Neurosurgery, University of Toronto Division of Genetics and Development, Toronto Western Research Institute
Krembil Chair, Neural Repair and Regeneration, Head, Spinal Program, University Health Network Simon A. Harris MA, MB, BChir, MRCS(Eng), Division of Orthopaedic Surgery, University of Toronto David W. Cadotte MSc, MD, Division of Neurosurgery, University of Toronto
Introduction
T
raumatic spinal cord injury (SCI) is a common cause of morbidity in children and young adults with devas-tating lifelong physical and psychosocial effects.1 Theprevalence of SCI in Canada and the US is estimated at 1.4 million cases (www.christopherreeve.org), with approximate-ly 13,000 individuals sustaining a SCI annualapproximate-ly.1 The resultant
financial and social impact of SCI is significant, with costs of care estimated at greater than $4 billion (USD) annually in North America.1,2 Despite improved, evidence-based,
system-atic, multi-disciplinary management of SCI patients, current clinical therapeutic modalities beyond surgery are limited. In addition to the initial traumatic insult, the prospect for re-covery from SCI is worsened by the resulting inflammatory cascade, neuronal loss and glial scar formation in the weeks to months following. However, the potential therapeutic ben-efits are significant, given that a small improvement in neuro-anatomical integrity in the central nervous system (CNS) can greatly improve clinical neuromotor function.
Pathophysiology
Acute traumatic injury to the spinal cord can come in the form of a blunt mechanism, such as an acrobat falling onto a hard surface or a person thrown from a car during an au-tomobile collision, or a penetrating injury such as a stab or gunshot wound. The forces involved in each of these events are transmitted to the spinal column, and if great enough, result in disruption of the bony and ligamentous structures and result in damage to the neural elements. Damage to the spinal cord or the exiting nerve roots can result in motor, sensory or autonomic dysfunction.
In an attempt to delineate the precise cause of neurological dysfunction, researchers have divided the temporal sequence
of destructive events into primary and secondary injury. Pri-mary injury refers to the destructive forces that directly dam-age the neural structures, such as the shear force tearing an axon or a direct compressive force occluding a blood vessel resulting in ischemia. These destructive primary mechanisms not only result in instantaneous damage to neurons and blood vessels but also initiate a cascade of cellular mechanisms that result in ongoing damage to the neural structures, termed secondary injury. In fact, in cases of ongoing primary injury, for example in the setting of a fracture dislocation where the bony spinal column is displaced and physically pushed against the spinal cord, these cellular mechanisms are thought to be locked into the ‘on’ position until such physical forces are removed either by closed reduction or surgical intervention.
Secondary injury may persist for hours to weeks to years following primary injury. A great deal of work has gone into the detailed understanding of these cellular cascades and along with this work has come an appreciation for the de-structive effects of the mechanisms and the role of potential therapeutics to halt these cascades. In the section titled From Bench to Bedside, we will highlight some of the recent therapeu-tics that are being developed along these lines.
From Impact to Intact: Optimizing the Acute Care of the Spinal Cord Injured Patient
Epidemiology
Spinal cord injury (SCI) has a global annual incidence of 15-40 cases per million population.1 The true incidence is
likely under-reported due to the occurrence of death prior to hospitalization. Motor vehicle collisions (MVCs) account for approximately half of all SCIs, with sporting injuries, falls and assaults accounting for the majority of the remaining occur-rences.3 55% of SCIs occur in the cervical spine.3 The risk of
cervical SCI from MVCs increases significantly with complete or partial ejection, lack of seatbelt use, increased number of rollovers, higher BMI, greater roof crush, and older age oc-cupants.4
A 10 year retrospective cohort analysis of SCI performed at the University of British Columbia, which covers a population of 4 million people, found an incidence of 35.7 per million, with a median age of 34.5-45.5 years and a male to female ratio of 4.4:1. Interestingly, despite an increasing rate of sur-gical intervention (61.8% to 86.4%), there was no
improve-Corresponding Author:
Michael G.Fehlings, MD, PhD, FRCSC, FACS Toronto Western Hospital
McLaughlin Pavilion
399 Bathurst St., 12th floor Rm.407 Toronto, Ontario, Canada M5T 2S8 Tel: 416 603-5627
Guest Editorial
Emerging Trends in the Management of Spine Trauma and Spinal Cord InjuryAn Ounce of Prevention to Make It Work
ment in mortality rate or length of stay. SCI patients over 75 years old had a 20% mortality rate.5
SCI is commonly associated with other traumatic injuries, including contemporaneous SCI at non-adjacent levels, head and facial injury, appendicular skeletal trauma, pelvis frac-tures, hollow organ and vascular injuries.6 Simply put, the
greater the amount of energy transferred during the injuri-ous insult, the more likely the presence of associated injuries.
Patterns of SCI
The level of injury determines the patient’s functional out-come. For example, in cervical SCI, preservation of C6 allows the patients to feed themselves, whilst C7 function allows pa-tients to propel themselves in a wheelchair due to the pres-ence of triceps motor power. This highlights the importance of C7 for patient independence. For all SCI, 34.3% suffer incomplete tetraplegia, 25.1% complete paraplegia, 22.1% complete tetraplegia and 17.5% incomplete paraplegia.3
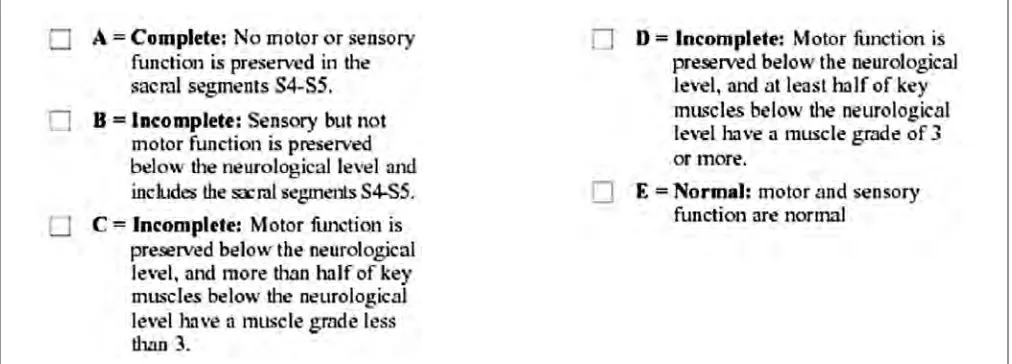
The ASIA impairment scale is the most commonly used system for grading SCI (Figure 1), grading injury from A (complete injury) to E (no motor or sensory deficit). This simple system allows for clear communication and recording as to the deficit at the time of injury and any post-operative improvement. In addition, there are 5 commonly recognized clinical syndromes of spinal cord injury:
1. Central Cord Syndrome – Upper limb impairment great-er than lowgreat-er limb.
2. Brown-Sequard Syndrome/Hemisection of the cord – Loss of ipsilateral motor function, fine touch and vibra-tion sense and loss of contralateral pain and temperature sensation.
3. Anterior Cord Syndrome – Compromise of the anterior spinal vascular supply, resulting in loss of motor power with preservation of fine touch and proprioception. 4. Conus Medullaris Syndrome – Compression at level of the
conus resulting in a mixed upper and lower motor neuron pattern distal to the lesion.
5. Cauda Equina – Bilateral leg weakness, faecal inconti-nence, urinary retention, and perineal saddle anaesthesia.
Advanced Trauma and Life Support (ATLS) and Initial Management
The optimal management of the SCI patient begins with the Advanced Trauma and Life Support (ATLS) protocol. In summary:
s !IRWAYPROTECTIONWITHCERVICALSPINECONTROL)NLINETRAC -tion or hard collar.
s "REATHING ASSESSMENT AND OPTIMIZATION /XYGEN SATURA -tion measurement, bilateral air entry ausculta-tion, ventila-tory assistance if required.
s #IRCULATORYASSESSMENTANDOPTIMIZATION6ITALSIGNSINTRA -venous access, blood tests, warm volume resuscitation. s $ISABILITYASSESSMENT0UPILLARYRESPONSES'LASGOW#OMA
Scale.
s %XPOSURE!SSESSLIMBSANDPELVISFORINJURIES
s 3ECONDARY SURVEY &!34 ULTRASOUND SCAN LOGROLL AND spine assessment including anal sphincter tone and bulbo-cavernosus reflex.
s 4RAUMAROENTOGRAMS-USTINCLUDEALATERALCERVICALSPINE x-ray and AP images of the chest, abdomen and pelvis.
Imaging in SCI
When the SCI patient is haemodynamically stable and well ventilated with a patent airway, they should undergo full-length spine CT. In Canada, the 24-hour ease of access to CT scanning facilities at Level 1 trauma centers allows for quick and thorough assessment of the bony anatomy – essential for diagnosis and operative planning. As an example, Figure 2 shows the CT scan of a 30-year-old male who dived head first into a shallow swimming pool, resulting in a burst fracture of the vertebral body of C6. Unfortunately, this gentleman’s neurological impairment was ASIA grade A.
Magnetic resonance imaging (MRI) is recommended in SCI to delineate the soft tissues (discoligamentous complex), rule out epidural haematoma and identify the level of injury (increased signal with the spinal cord). Figure 3 shows the 6-month post-operative MRI of the same patient illustrated in Figure 2. The degeneration within the cord at the level of injury is highlighted (arrow). Further research into the
Guest Editorial
Emerging Trends in the Management of Spine Trauma and Spinal Cord Injury
nostic use of MRI diffusion weighted imaging may be useful in quantifying axonal loss whilst functional MRI may be useful in measuring the metabolic correlates of sensory and motor activities in persons with SCI.7
Figure 2. Sagittal cervical spine CT$CVSTUGSBDUVSF BSSPX
Figure 3. Sagittal cervical spine MRI$PSETJHOBMDIBOHFBU$ (arrow)
Minimizing Secondary Injury
Secondary prevention of SCI must include avoidance of hypotension (mean arterial pressure greater than 85 mmHg) for 7 days to maximize spinal cord perfusion.8 Controversy
surrounds the use of intravenous methylprednisone. The National Acute Spinal Cord Injury Study II (NASCIS) was a blinded randomized controlled study comparing meth-ylprednisone against naloxone or placebo in 427 acute SCI patients.9 There was no significant difference in
neurologi-cal recovery at one year, except in those patients receiving methylprednisone within 8 hours of SCI.9 A subsequent trial
(NASCIS III) compared the use of methylprednisone for 24 hours or 48 hours post-injury against tirilazad mesylate (a lip-id peroxlip-idation inhibitor) after SCI, in which patients had all received an initial bolus of methylprednisone. There was no difference in outcome if patients received methylprednisone bolus within 3 hours of SCI. If patients received the bolus within 3 to 8 hours of injury, patients who received 48 hours of methylprednisone had a better motor recovery (but not functional improvement) at the cost of increased episodes of sepsis and pneumonia.10
Timing of Surgical Intervention
The evidence justifying early surgical decompression in cervical SCI patients is increasing in volume and quality. In 1999, Mirza et al. showed that patients suffering from acute cervical SCI had improved neurological recovery and shorter hospitalization if operated on within 72 hours when compared to a cohort that underwent closed reduction followed by ob-servation and subsequent surgery within 10 to 14 days.11 This
year, Fehlings et al., as part of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS), published the strongest evidence to date in favor of early surgical intervention.12 As
part of a multicenter, international, prospective study of cer-vical SCI, the group showed that 19.8% of patients undergo-ing early surgery (mean 14.2 hours from time of injury) com-pared to 8.8% in the late decompression group (mean 48.3 hours) improved their ASIA impairment scale by >2 grades at 6 months.12 It is therefore recommended to perform surgical
decompression for acute cervical SCI within 24 hours.
From Bench to Bedside: Translational Research in Traumatic Spinal Cord Injury
An in-depth understanding of secondary mechanisms of spinal cord injury have led to numerous possible targets for prevention of this secondary damage and possible regenera-tion of partially damaged neural circuits. Here we will review a number of agents that are currently under investigation. Broad categories include neuroprotective agents (Minocy-cline and Riluzole), myelin-associated inhibitors of neural regeneration (ATI-355 and Cethrin), and cellular transplan-tation strategies (activated autologous macrophages, bone marrow stromal cells and human embryonic stem cells). This list is by no means exhaustive. Numerous other strategies have been attempted in the past and many lessons have been learned – both positive and negative. Readers interested in a recent history of translational research in the field of spinal cord injury are referred to a recently published open source review.13
Neuroprotective Agents
Guest Editorial
Emerging Trends in the Management of Spine Trauma and Spinal Cord Injury
these conditions, its potential application was carried over to the realm of SCI. Initially studied in animal models, its ben-efit became apparent in improved neurological outcomes15
and its mechanism of action was thought to be a result of de-creased microglia activation and anti-apoptotic pathways me-diated by the inhibition of cytochrome c release. Because of its extensive use in other neurological conditions and prom-ise in animal models of SCI, at least two clinical trials are un-derway to test the efficacy of minocycline in human SCI.
Table 1. Selected neuroprotective approaches, in early phase clinical trials, with a potential role for improving outcomes in SCI
Age (years) Riluzole Minocycline
1PMZFUIZMFOFHMZDPMNBHOFTJVN Hypothermia
Riluzole is a benzothiozole anticonvulsant that has been in clinical use for greater than a decade. Used primarily in patients with amyotrophic lateral sclerosis (ALS), it has been shown to prolong the lives of patients by 2-3 months.16
Rilu-zole is thought to act by blocking voltage-sensitive sodium channels, whose over-activity after trauma has been associ-ated with neural tissue destruction. In addition, riluzole has been shown to block presynaptic calcium-dependent gluta-mate release, whose deleterious effects were discussed above. Multicenter clinical trials are underway in order to study this agent. Its dosing will be similar to that for ALS patients and the duration will be 10 days. This duration was decided as a direct effect of studies into secondary injury cascades, where results indicate that sodium- and glutamate-mediated damage persists for that time period – an excellent example of how translational research is the direct result of thorough and comprehensive basic science research.
A non-pharmacologic means of neuroprotection currently under study in the spinal cord injury population is hypother-mia. Cooling the human body to slow metabolism and en-zymatic processes is certainly not new in clinical medicine. However, its application for SCI has received recent attention likely due to new methods that allow for easy and faster cool-ing via a femoral sheath catheter. A recent retrospectively designed study demonstrated the safety of this method and gathered preliminary data with regard to cooling tempera-ture, time to target temperatempera-ture, duration of cooling and any adverse events.17 The long-term follow up of these patients
compared to controls will be necessary to demonstrate any functional benefit.
Myelin-Associated Inhibitors of Neural Regeneration Many regenerative strategies for the treatment of SCI are under investigation. These can be broadly classified as molecu-lar and pharmaceutical strategies and cellular and bioengineered strategies. Select agents in these categories are summarized in Table 2. Here, we further discuss the evolution of this field along with two therapeutic agents. The notion that the cen-tral nervous system cannot regenerate axons after injury was
convincingly disproved in the 1980’s18 and with numerous
other studies after this. Axons, however, do not typically re-grow after injury for the many reasons discussed in the sec-ondary injury cascade above. Of the innate mechanisms that stunt this growth are the myelin-associated proteins whose ac-tivity has been directly linked to a lack of regenerative capac-ity. Many inhibitors of myelin-associated proteins have been researched in cell culture and animal models, and two in par-ticular have been the focus of investigation in clinical trials: ATI-335 and Cethrin.
Table 2. 4FMFDUFENPMFDVMBSQIBSNBDFVUJDBMTUSBUFHJFT UPQBOEDFM-lular and bioengineered strategies (bottom) with a potential role for improving outcomes in SCI by influencing regeneration or plasticity
Molecular and Pharmaceutical strategies /PHP"NPOPDMPOBMBOUJCPEZ "5*
Cethrin Rolipram Lithium Carbonate Chondroitinase ABC
Cellular strategies either in Phase I clinical trials or destined for Phase I clinical trials
Neural stem cells
Oligodendroglial precursor cells Schwann cells
Olfactory ensheathing cells
Bioengineered strategies in late stage pre-clinical trials or early Phase I studies
Cethrin
5SBOTDSJQUJPOBMGBDUPSTUPVQSFHVMBUF7&(' ;'17&('
ATI-335 has a rich history ranging form basic laboratory science through animal models and into the realm of trans-lational research. CNS myelin, at this time known to be an inhibitor of axonal growth, was biochemically separated into component proteins.19 Antibodies to these proteins were then
developed and applied to in vitro models that demonstrated their ability to diminish the inhibitory effects of myelin. Sub-sequent animal models demonstrated improved neurological outcomes with administration of these antibodies.20 After a
flurry of excitement in the animal world, Nogo was character-ized as the target antigen and human antibodies were subse-quently developed. These antibodies were demonstrated to promote axonal growth and functional recoveries in primate models of SCI. Clinical trials began shortly thereafter and are currently underway in both Europe and Canada.
Guest Editorial
Emerging Trends in the Management of Spine Trauma and Spinal Cord Injury
mixture is applied directly to the dura at the time of surgical decompression of spinal cord injury. A 48 patient multicenter phase I/IIa trial showed no adverse effects attributable to the drug. Moreover, 31% of cervical SCI patients improved their ASIA scores from A to C or D by 12 months, compared to 66% of cervical SCI that received 3 mg of Cethrin.22 Phase III trials
are currently planned.
Cellular Transplantation Strategies
Cellular transplantation is a concept that transcends the notion of optimizing the spinal cord for natural recovery and introduces cell types with the goal of integrating these cells within spinal circuits and allowing for neurological recovery. Furthermore, evidence continues to show that these implant-ed cells are able to induce neuronal plasticity and modify their microenvironment by promoting axonal elongation and collateral sprouting, remyelination, and synapse formation.23
Whilst basic science research aims to deepen our under-standing of the barriers to successful stem cell transplantation in SCI, patients continue to suffer. It is therefore the belief within our research group that the time is right for safe, rigor-ous and ethical clinical trials of stem cell transplantation in SCI.24
Many different cell types have been studied. Here we will focus on three: activated autologous macrophages, bone mar-row stromal cells, and human embryonic stem cells.
Activated Autologous Macrophages
It has been realized for about two decades that macro-phages play a vital role in the regeneration of peripheral ner-vous function and that this role does not exist in the central nervous system. Following injury to a nerve in the peripheral nervous system, macrophages are recruited to the site of injury and are responsible for clearing myelin debris and optimizing the local environment for regeneration. In order to capital-ize on this finding in the central nervous system, researchers attempted to take autologous macrophages from spinal cord injury patients, activate them with peripheral myelin and in-ject them into the damaged area of the spinal cord shortly after injury. The initial results were promising, although only a small number of individuals received treatment. Due to fi-nancial circumstances, the trial was never expanded beyond the initial study. This strategy once again highlights a bridge between understanding the secondary mechanisms of dam-age, in this case how central myelin acts to inhibit neural regeneration and repair, and the development of potential therapy. Hopefully this promising strategy will be revitalized and studied in a larger population.
Bone Marrow Stromal Cells
The use of bone marrow stromal cells aims to take advan-tage of a relatively accessible multipotent stem cell that has potential to differentiate and integrate into existing spinal circuits and result in neural recovery. A number of groups around the world are reporting the use of these cells, includ-ing scientists from Korea, China, Russia, the Czech Republic, and Brazil. To date, trials have been small and are often not blinded, prompting cautious interpretation of the results.
Nonetheless, researchers report significant neurological re-covery after direct injection of this cell type in the damaged area of the spinal cord. Researchers in Prague, Czech Re-public, did have blind assessors evaluate patients at follow-up in terms of both the ASIA scale and electrophysiologically. Significant improvement was noted in patients that received therapy within 3-4 weeks of injury, but not those that were in the chronic stages of injury.25
Human Embryonic Stem Cells
While human embryonic stem cells are theorized as one of the more promising strategies in cell replacement in the spinal cord, there are a number of hurdles that must be over-come. This cell type is first cultured in vitro and the purity of these cultures is paramount and somewhat challenging. In addition, viral contamination via delivery vectors and the acquisition of membrane polysaccharides that may react with the host immune system are all concerns that are being ad-dressed. Significant advances have been made in this field, mainly out of the University of California at Irvine,26,27 and
are currently being evaluated by the FDA in the United States. The goal of this therapy is to achieve differentiation of these stem cells into oligodendrocytes that would aid in remyelin-ation of spared but demyelinated axons. This represents a promising avenue of research in the decades to come.
Conclusion
Spinal cord injury is a life-changing event with a predilic-tion for young patients who face a long life of physical and emotional struggles. The treatment of acute SCI is an ever-evolving landscape and one which is likely to see tremendous changes over the next 20 years. SCI continues to be at the forefront of scientific research into stem cell and biotechnol-ogy innovation. The combination of basic science and clinical advances brings hope to current and future sufferers of SCI.
References
1. Sekhon LH, Fehlings MG. Epidemiology, demographics, and pathophysiol-ogy of acute spinal cord injury. Spine (Phila Pa 1976) 2001;26:S2-12. 2. Tator CH, Fehlings MG, Thorpe K, Taylor W. Current use and timing of
spinal surgery for management of acute spinal surgery for management of acute spinal cord injury in North America: results of a retrospective multi-center study. J Neurosurg 1999;91:12-8.
3. Lieberman J. AAOS Comprehensive Orthopaedic Review: American Acad-emy of Orthopaedic Surgery; 2009.
4. Funk JR, Cormier JM, Manoogian SJ. Comparison of risk factors for cervi-cal spine, head, serious, and fatal injury in rollover crashes. Accid Anal Prev;45:67-74.
5. Lenehan B, Street J, Kwon BK, et al. The epidemiology of traumatic spinal cord injury in british columbia, Canada. Spine (Phila Pa 1976);37:321-9. 6. Patzkowski JC, Blair JA, Schoenfeld AJ, Lehman RA, Hsu JR. Multiple
as-sociated injuries are common with spine fractures during war. Spine J. 7. Lammertse D, Dungan D, Dreisbach J, et al. Neuroimaging in traumatic
spinal cord injury: an evidence-based review for clinical practice and re-search. J Spinal Cord Med 2007;30:205-14.
8. Markandaya M, Stein DM, Menaker J. Acute Treatment Options for Spinal Cord Injury. Curr Treat Options Neurol.
9. Bracken MB, Shepard MJ, Collins WF, Jr., et al. Methylprednisolone or naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study. J Neurosurg 1992;76:23-31.
Guest Editorial
Emerging Trends in the Management of Spine Trauma and Spinal Cord Injury
low up. Results of the third National Acute Spinal Cord Injury randomized controlled trial. J Neurosurg 1998;89:699-706.
11. Mirza SK, Krengel WF, 3rd, Chapman JR, et al. Early versus delayed surgery for acute cervical spinal cord injury. Clin Orthop Relat Res 1999:104-14. 12. Fehlings MG, Vaccaro A, Wilson JR, et al. Early versus Delayed
Decompres-sion for Traumatic Cervical Spinal Cord Injury: Results of the Surgical Tim-ing in Acute Spinal Cord Injury Study (STASCIS). PLoS ONE;7:e32037. 13. Hawryluk GW, Rowland J, Kwon BK, Fehlings MG. Protection and repair
of the injured spinal cord: a review of completed, ongoing, and planned clinical trials for acute spinal cord injury. Neurosurg Focus 2008;25:E14. 14. Yong VW, Wells J, Giuliani F, Casha S, Power C, Metz LM. The promise of
minocycline in neurology. Lancet Neurol 2004;3:744-51.
15. Wells JE, Hurlbert RJ, Fehlings MG, Yong VW. Neuroprotection by minocy-cline facilitates significant recovery from spinal cord injury in mice. Brain 2003;126:1628-37.
16. Miller RG, Mitchell JD, Lyon M, Moore DH. Riluzole for amyotrophic later-al sclerosis (ALS)/motor neuron disease (MND). Cochrane Database Syst Rev 2007:CD001447.
17. Levi AD, Green BA, Wang MY, et al. Clinical application of modest hypo-thermia after spinal cord injury. J Neurotrauma 2009;26:407-15. 18. David S, Aguayo AJ. Axonal elongation into peripheral nervous
sys-tem “bridges” after central nervous syssys-tem injury in adult rats. Science 1981;214:931-3.
19. Caroni P, Schwab ME. Two membrane protein fractions from rat central myelin with inhibitory properties for neurite growth and fibroblast spread-ing. J Cell Biol 1988;106:1281-8.
20. Fouad K, Dietz V, Schwab ME. Improving axonal growth and functional recovery after experimental spinal cord injury by neutralizing myelin as-sociated inhibitors. Brain Res Brain Res Rev 2001;36:204-12.
21. Dergham P, Ellezam B, Essagian C, Avedissian H, Lubell WD, McKerracher L. Rho signaling pathway targeted to promote spinal cord repair. J Neurosci 2002;22:6570-7.
22. Fehlings MG, Theodore N, Harrop J, et al. A phase I/IIa clinical trial of a recombinant Rho protein antagonist in acute spinal cord injury. J Neu-rotrauma 2011;28:787-96.
23. Ruff CA, Wilcox JT, Fehlings MG. Cell-based transplantation strategies to promote plasticity following spinal cord injury. Exp Neurol 2011. 24. Fehlings MG, Vawda R. Cellular treatments for spinal cord injury: the time
is right for clinical trials. Neurotherapeutics 2011;8:704-20.
25. Sykova E, Homola A, Mazanec R, et al. Autologous bone marrow trans-plantation in patients with subacute and chronic spinal cord injury. Cell Transplant 2006;15:675-87.
26. Keirstead HS, Nistor G, Bernal G, et al. Human embryonic stem cell-de-rived oligodendrocyte progenitor cell transplants remyelinate and restore locomotion after spinal cord injury. J Neurosci 2005;25:4694-705. 27. Lebkowski JS, Gold J, Xu C, Funk W, Chiu CP, Carpenter MK. Human
Letter to the Editors
thought was extremely funny. The biggest challenge I faced was dealing with the hopelessness I felt when a complex-care diabetic patient revealed that she had been sexually abused by her brother. I knew that there was no way she could leave her home, because she was the sole caregiver of her mother who lived there. There were absolutely no psychiatrists in the area to whom I could refer the patient, and the economics situation of the village meant there were no jobs she could find to help support herself – she was financial reliant on her mother’s savings and her brother’s income. How could I even attempt to be clinically courageous in the face of this scenario? The hospital staff were overwhelmingly welcoming, and the family doctor I was shadowing explained that his wife, a behavioural psychologist, had begun coaching him on how to help patients such as this woman. That’s how they made the resources work: one doctor expanded his clinical skills as far as he could to fill the gaps in the system. Here, I hoped to observe first-line care of vulnerable populations and better understand the range of practice options for rural physicians.
Early in my second week, a patient arrived: 27-weeks preg-nant, with a possible cord prolapse! She was assessed in our small ER by the two attending family physicians. She was in acute distress but the foetal heart rate was only slightly ele-vated. I had told the doctors previously about my interest in obstetrics so they were quick to include me in the team but we quickly realized that her care was out of our scope of practice. The stakes were high as we were fighting for two lives and the nearest level-two care centre was 35 kilometers away by ambulance. It takes just as much courage to assess and treat a patient; as it does to assess and refer them. The rural nurses and physicians, while coping with stress, fear and indecision, displayed clinical courage when they told the mother that she could no longer be treated in Botwood.
After stabilizing the patient we had a hectic ambulance ride to the nearest health centre. An obstetrician assessed and decided it wasn’t the umbilical cord, but redundant mu-cosa that had prolapsed. The baby and mom were out of the woods.
The hand-over to the obstetrician brought such relief to everyone, especially to the mother. I realized that his deci-sion to work as an obstetrician in such a remote place must have been a difficult one to make. His clinical courage must be in overdrive all of the time, but this incident showed how he coped with that challenge. In order to clear the fog of
“Clinical Courage” and Rural Obstetrics in Newfoundland
&NJMZ1"#SBOEFS#4D.%DBOEJEBUF'BDVMUZPG.FEJDJOF6OJWFSTJUZPG5PSPOUP
I
n the President’s Message in the spring 2011 issue of the Canadian Journal of Rural Medicine (CJRM),1 PresidentJohn Wootton referred to the term “clinical courage”. He wanted to share the concept, knowing it would resonate with all physicians. As a second year pre-clerk, the message behind “clinical courage” certainly hit home with me. Clinical cour-age is a quality that doctors show when they are working in the best interests of their critically ill patient, but are forced to be working at the limits of their competence. It is truly terrify-ing, as a new medical student, to realize the necessity of such a quality. When a doctor feels out of their depth, surely both patient and doctor would feel more comfortable if the patient were transferred to a better equipped coentre. Clinical cour-age involves asking oneself: “How far do I trust my skills? How soon do I hand over responsibility of a patient?”
As a follow-up to his editorial in the CJRM, Dr. Wootton recently wrote a Letter to the Editor in the Globe and Mail.2 He
outlined the Canadian Medical Association’s (CMA)commit-ment to distributing physicians to rural areas: “The CMA will examine practice location patterns of recent entry cohorts of Canadian medical school graduates to assess implications for the urban-rural distribution of physicians”. Even though the provincial governments have increased medical class sizes, the resultant doctors may not be filling the void in rural com-munities where they are so desperately needed.
These concepts of human resource allocation and clini-cal courage piqued my growing interest in rural medicine, so this summer I set up an independent medical elective in Botwood, Newfoundland. This small town has a clinic with four general practitioners and serves a catchment of 7,300, including many small fishing outposts.
Rural doctors face a myriad of challenges: lack of re-sources, distance from tertiary centres, and isolated pock-ets of at-risk patients; but I wasn’t just in rural medicine, I was in rural Newfoundland medicine. All of the challenges became amplified. The accent was so thick that I often had to get a nurse to help translate for me, which the patients
Corresponding Author: Emily PA Brander, B.Sc.
University of Toronto, Faculty of Medicine, 1 King’s College Circle, Toronto ON, M5S 1A8, Canada
Letter to the Editors
“Clinical Courage” and Rural Obstetrics in Newfoundland
uncertainty when making a clinical decision, he relied on a networked team. The obstetrician was respectful to the Bot-wood team, and we managed the patient with courage before entrusting her to his care. The successful outcome belonged to everyone because we all depended on one another. Wit-nessing how this successful medical team functioned made me feel that rural practice is now an attractive career path.
Would all medical students feel the same way after expo-sure to a rural practice setting? It is vital to discover whether the CMA-backed, larger cohort has helped the situation. It would be foolish to assume that the solution is to simply admit more medical candidates from rural backgrounds. It was be-cause of my time spent in a rural clinic, not my background, that made rural medicine attractive to me.
A more organic and effective approach to the rural doctor deficit is to expose students to the realities of rural practice early in their training. The sooner that happens, the sooner there will be an influx of prepared, young doctors to the
iso-lated areas of Canada. If the students become immersed in remote medical care early, they will become devoted to the cause of improving healthcare delivery and be more likely to settle, long-term, in those areas. I don’t feel it is only those graduates from rural backgrounds who will return to practice there. Case and point – even I, a hardened Montreal and To-ronto resident, can be convinced. After my experiences out East, I can’t imagine any other situation where I would rather demonstrate my clinical courage.
Acknowledgements
I thank Dr. Jody Woolfrey and the staff at the Dr. Hugh Twomey Healthcare Clinic in Botwood, Newfoundland.
References
1. Wootton, J. President’s Message: Clinical Courage. Can J Rural Med. 2011 Spring;16(2):45-6.
News and Views
(BWJO.)BNJMUPO.4D.%$BOEJEBUF*OTUJUVUFPG.FEJDBM4DJFODF'BDVMUZPG.FEJDJOF6OJWFSTJUZPG5PSPOUP
Concussion: The Sport Injury of the Year
Corresponding Author: Gavin M. Hamilton, MSc University of Toronto
Faculty of Medicine, 1 King’s College Circle Medical Sciences Building, Room 2109 Toronto, ON M5S 1A8
Tel: 647-216-4339
Email: [email protected]
I had the pleasure of being invited to attend a press-release about a prevention initiative called Stopconcussion.com, cre-ated by former elite hockey players (Keith Primeau, among others). Although I have had minimal exposure to preventative medicine, this was a prime example. What inspired me about the event was not necessarily the content of the public initiative that was being brought forward; it was the energy and effort that was involved in getting a message out to the public.
Stopconcussion.com is an online concussion and neu-rotrauma educational and awareness hub for all sports, de-signed to address the growing trend of concussions in sports. The mandate of this concussion resource is based upon a four step program; 1) Education, 2) Prevention, 3) Management, and 4) Research. The media release focused on a number of topics, which included an announcement about new alliances with other organizations, a new scholarship fund, and other concussion awareness products Stopconcussion.com supports. The topic that was especially pertinent was the baseline test-ing initiatives that are now gaintest-ing momentum in some nearby communities.
The importance of baseline testing is widely accepted in the sport medicine world, and has been included as an important step in the diagnosis of concussions in a recent international consensus statement.1 Because the diagnosis of concussion is
not as objective as other injuries (e.g., fracture), a normalized screen of the five clinical domains (presented above) con-ducted prior to the injury can be very useful when assessing for a concussion. The baseline test obtains normalized charac-teristics of an athlete playing in the sport, and can be used to compare their post-impact function to their pre-impact func-tion to aid in the assessment of a concussion. The comprehen-sive assessment includes an athlete’s baseline symptoms, the Glasgow Coma Scale (GCS), orientation, balance, coordina-tion, memory, concentracoordina-tion, and delayed recall. There are a number of baseline tests available including the Sport Concus-sion Assessment Tool 2 (SCAT2),1 the Computerized Cognitive
Assessment Tool (CCAT),7 and the King-Devick Test.8 These
assessment tools have yet to be validated but the clinical use-fulness of this testing has been endorsed by researchers and concussion experts alike.
Peterborough, a community in southern Ontario, has tak-en the steps to try to implemtak-ent a baseline test on all youth aged 10 to 17 who play hockey in the area.9 The five
Peterbor-ough Networked Family Health Teams encompass most of the primary care available in the region, and this unique health care structure enables the city to implement large scale public
A
concussion is a complex pathophysiological processaf-fecting the brain, induced by traumatic biomechanical forces.1 Disturbance of brain function is related to
neu-rometabolic dysfunction,2 and the injury is typically associated
with normal structural imaging findings.1 The presentation of
a concussion can be variable, and a suspected diagnosis of a concussion can be made if any of the 5 clinical domains are affected; 1) symptom manifestation (e.g., headache), 2) physi-cal signs (e.g., loss of consciousness), 3) abnormal behavior, 4) cognitive impairment, or 5) sleep disturbance.1 It is one of
the most common and potentially dangerous types of injuries sustained in collision sports and the long-term morbidity as-sociated with concussions is relatively unknown. In addition, concussions have rendered many athletes, elite or otherwise, unable to participate in their chosen sport.
Concussion was the sport injury of the year in 2011 and the reason for the sudden increase in publicity is debatable. Was it because the face of the National Hockey League and Cana-dian hockey, Sidney Crosby, missed a significant portion of the last two consecutive seasons as a result of his concussion or his concussion-like symptoms? Did Don Cherry, a renowned Cana-dian NHL television commentator, single-handedly create the media uproar when he called retired fighters “pukes” and hyp-ocrites for blaming their life problems on head impacts and the combatant lifestyle? Was it the three tragic hockey enforcer deaths that occurred recently, which was followed by the NY Times exposé published about the tragic rise and fall of one of them (Derek Boogaard)?3 Another possibility is the publicity
surrounding the long lasting danger of repeated high-impact collisions in the National Football League; epitomized by a 2011 New Yorker article?4 Or lastly, is it the increase in the
pub-lication of concussion research in youth sport and the long-term morbidity that has been associated with concussions?5,6
News and Views
Concussion: The Sport Injury of the Year
health initiatives. It is the first program of its kind in Canada and this pilot project is designed to be an adoptable model of collaboration between specialists and primary care providers to establish standardized guidelines for concussion assessment, treatment, and management. In addition, any athlete with a suspected concussion will be seen within 48hrs by a concus-sion specialist to assess their injury. The health care teams are working with coaches and parents to increase the awareness of concussions, and to ensure that children will be provided with access to a health care provider within a short time period post-injury. The benefits of the program have yet to be seen, but this initial step in implementing this public health campaign is promising.
I was very encouraged with the interest generated about this very serious public health concern for youth and adults alike. Although much of the press release appears exciting and valu-able, it is easy to fall into the trap of neglecting to consider the bias that can be associated with products endorsed and infor-mation provided. It is necessary to continue to always be critical of information disseminated in settings such as this.
Knowledge translation, or closing the gaps between research and practice, is an integral part of health research.10 An
organi-zation such as Stopconcussion.com can be invaluable to health researchers in making their results accessible to the public, and providing a means for sharing information. In addition, it provides a medium to empower the public to educate them-selves about the importance of these health issues. Researchers must also capitalize on the media hype surrounding the areas of public interest; the researchers examining concussion have
certainly been provided with an opening to take advantage of. Although it pains me to say, as I too am a fan of the game of hockey, thank you Mr. Crosby, for lighting this fire.
References
1. McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, et al. Consensus Statement on Concussion in Sport: the 3rd International Con-ference on Concussion in Sport held in Zurich, November 2008. Br J Sports Med 2009;43 Suppl 1:i76-90.
2. Henry LC, Tremblay S, Boulanger Y, Ellemberg D, Lassonde M. Neuromet-abolic changes in the acute phase after sports concussions correlate with symptom severity. J Neurotrauma 2010;27(1):65-76.
3. Branch J. Punched Out: The Life and Death of a Hockey Enforcer. The New York Times. Dec 3, 2011. Available from: http://www.nytimes. com/2011/12/04/sports/hockey/derek-boogaard-a-boy-learns-to-brawl. html?_r=1
4. Mcgrath B. Does Football have a future? The NFL and the concussion cri-sis. The New Yorker. New York, January 31, 2011. Available from: http:// www.newyorker.com/reporting/2011/01/31/110131fa_fact_mcgrath 5. Emery CA, Kang J, Shrier I, Goulet C, Hagel BE, Benson BW, et al. Risk
of injury associated with body checking among youth ice hockey players. JAMA 2010;303(22):2265-72.
6. Castile L, Collins CL, McIlvain NM, Comstock RD. The epidemiology of new versus recurrent sports concussions among high school athletes, 2005-2010. Br J Sports Med 2011. doi:10.1136
7. Cogstate. Axon Sports CCAT. Wausau, WI, [cited 2011 Dec 22]. Available from: http://www.axonsports.com/index.cfm
8. King Devick Test. King-Devick Test. Oakbrook, IL, 2011. [cited 2011 Dec 23]. Available from: www.kingdevicktest.com
9. Primary Health Care Services of Peterborough. Youth Sports Concussion Program. Peterborough, ON, 2011. [cited 2011 Dec 22]. Available from: http://youthsportsconcussionprogram.com
Interview
D
r. Peter Chu is an attending staff trauma surgeon at the Tory Regional Trauma Unit, Sunnybrook Health Sciences Center. He is an Associate Professor at the University of Toronto. In addition, since 1998, he and his fam-ily have annually volunteered at Galmi Hospital, a missionary hospital in the country of Niger in West Africa. Dr. Chu com-pleted medical school and residency in general surgery at the University of Toronto.He is a graduate of the Surgical Scientist Program, having completed a Masters of Science studying the immune re-sponse to sepsis.
UTMJ: Can you tell us about your background and training?
Dr. Chu: I grew up in Ottawa and did my undergraduate studies in Toronto. This was the old system where you could get in [to medical school] after two years, so I did two years in Sciences and then got into medical school in 1986. I completed medical school here [in Toronto], as well as residency in general surgery. I broke up my residency with two years of research, and after I finished my residency, the plan was to work in a missionary hospital in Africa. Probably one of the best and most critical elements of my surgical training was the year I spent as a fellow at Toronto East General Hospital right after my residency. That hospital was where I learned how to do surgical procedures outside of general surgery such as orthopedics, plastics, head and neck, urology and obstetrics/gynecology. That was probably the best year of my life in terms of surgical training. At that time, the other services didn’t have many residents so I had the chance to learn how to do old-fashioned GENERAL surgery. It’s still one of my favourite hospitals. It’s a great hospital in terms of teaching and patient volume. When I finished my fellowship, I took a year off from medicine to study at Bible College/seminary and then I came back to Toronto. My wife was finish-ing her family medicine residency and I was lookfinish-ing for a job to kill some time. I happened upon a no-tice for a plastic surgery fellowship at Sunnybrook Hospital. I thought plastic surgery would be really helpful in Africa, so I called them up and got the position. While I was there, the trauma surgeons at Sunnybrook told me they needed a trauma fellow for a year. My wife still had another year of residency left, so I decided to be a trauma fellow for a year.
Interview with Dr. Peter Chu
#BJMFZ%ZDL1I%.%$BOEJEBUF'BDVMUZPG.FEJDJOF6OJWFSTJUZPG5PSPOUP
I finished the fellowship, and my wife and I went to Africa for a year. While we were there, the trauma surgeons at Sunnybrook contacted me and told me they needed another trauma surgeon. They asked if I would consider coming back to join them. I en-joyed my trauma fellowship and loved trauma but never thought it would be possible to marry an aca-demic career with working in Africa. At the same time, my wife got a job offer [in Toronto] as well. So, we thought about it and were able to negoti-ate the terms of our work to include having up to two months a year to work in Africa. That’s how we ended up being where we are. It definitely wasn’t something I had planned or foresaw.
As a student, many staff would tell us, “Don’t worry about the job. The job will be there. Just do what you love. Then you will find the job.” I think it’s true. I think if you stay true to yourself and do what you love, the job will be there.
UTMJ: What exactly is trauma surgery, and what do you do in your job as a trauma surgeon?
Dr. Chu: There are two trauma centers in Toronto, Sunny-brook and St. Michael’s. We are equipped to pro-vide comprehensive care for the trauma patient with multi-system injuries. As soon as the ambu-lance drops them off, the trauma team takes over. The team will resuscitate the patient and simulta-neously conduct a thorough assessment to identify their injuries. This need to parallel process within a time constraint is what makes trauma exciting or stressful depending on your perspective. The resus-citation and assessment usually takes about 2 hours to complete. At the end of the process, the patient will either be admitted (ward or ICU), taken to the operating room, or discharged (home or police custody).
facilitat-Interview with Dr. Peter Chu
Interview
Interview with Dr. Peter Chu
modynamically stable and there usually isn’t a time pressure component to deal with. In trauma, the operative field is a mess, the patient is often unsta-ble, and there is a time pressure to get things done quickly but safely. There is destroyed and devital-ized tissue, staining from all types of body fluids, and all the tissue planes are disrupted. I think the challenge of operating in that type of environment and still doing a technically correct operation is what I find very interesting and rewarding.
The second aspect is that you never know what you’re going to find. With CT scanning, you have a better idea but it is similar to Forrest Gump’s box of chocolates – you never know what you’re going to find when you unwrap the chocolate. However, at the end of the day, similar to elective general surgery, you know what the injuries are and usually have an answer to the mystery.
UTMJ: What is an average day or week like for you?
Dr. Chu: I have to begin with several caveats. First, I do not have any research commitments or obligations. Second, I closed my elective practice four years ago when my wife and I had our first child. My wife and I essentially work part-time in order to maintain bal-ance and margin in our family life. Our work weeks are scheduled to be the complement or mirror im-ages of each other. Her busiest days are my light-est days and vice versa. A typical “light” day for me would include tidying up the house after the daily tornado left by our girls, some grocery shopping, a weekly visit to my favourite store Canadian Tire, running errands, drop off and pick up from daycare and primary school, and working out at the gym. I’ll squeeze in some paperwork and rounding. My “busy” days are more typical of a surgeon’s schedule with rounding, clinic, paperwork, teaching, etc. My wife and I have basically traded income for time. I no longer have an elective operating list. I’m on call for trauma six nights a month and 1:5 week-ends. The rest of the time is spent teaching, doing administrative tasks, or looking after the patients who came in on those six nights of call. I have a clinic roughly once a month with no more than 5 patients. This schedule allows me to have time off during the day to get the “things of life” accom-plished (errands) and maximize family time.
UTMJ: That’s really useful. As students, I think it’s very helpful to get a little more exposure to appreciating that there is a balance to be sought and that you can do it.
Dr. Chu: Right. No one puts a gun to your head and forces you to operate five days a week, see 80 patients in your clinic between 4-10 pm at night, perform en-doscopy on Saturday, and write opinions for the WSIB and CMPA on Sundays. There is a choice because there are other surgeons to help provide ing communication. It’s all geared towards moving
the patients forward in their recovery and returning them as much as possible to their former lives and activities.
UTMJ: Are there big differences in trauma management between Toronto and say, another city in Ontario, or across Canada?
Dr. Chu: No, the Canadian systems are pretty similar, wheth-er it’s Toronto or Calgary or Vancouvwheth-er or London. All the major centres are staffed with trauma sur-geons with regular site visits and accreditation by the Trauma Association of Canada.
UTMJ: Are there trauma centres only in the bigger cities?
Dr. Chu: Yes. For Ontario, there’s Ottawa, Kingston, two in Toronto, London and Hamilton. The smaller cen-ters (1A and 1B) would include Sudbury and Thun-der Bay. One big difference is that those two centres don’t have neurosurgical coverage.
UTMJ: Do the smaller centres just triage and then send pa-tients to the trauma centers?
Dr. Chu: Yes, whatever they can handle, they handle, and whatever they can’t, they send down to southern Ontario.
UTMJ: You mentioned that you went into general surgery before pursuing trauma surgery. Maybe you could tell us about what drew you to general surgery, and from there, into trauma surgery?
Dr. Chu: I came to general surgery late. It was probably the end of third year/beginning of fourth year during clerkship, when I discovered that surgery was really fun. I think what drew me to it was that it is very mechanical and you get to work with your hands. Surgical problems tend to be mechanical in na-ture - there is a hole, a blockage, or a lump. It is very concrete, and I realized those were the type of problems that I enjoyed tackling. The results in surgery are often immediate, so you receive instant feedback and hopefully, gratification. I also liked the pace of surgery - it was like the old US Army commercial, “We do more by 9 than the rest of the world does by 5.” The last aspect I liked about gen-eral surgery was that you had to be a good internist in order to look after your patients pre and post op. Orthopedics was a very, very close second, but I ended up applying to general surgery.
UTMJ: What would you say is the biggest difference be-tween general surgery and trauma surgery?
he-Interview
Interview with Dr. Peter Chu
surgical care to the Canadian population. It’s not like Africa, where you very well could be the only surgeon for 100,000 people and 200 people wait to see you every day in clinic with problems span-ning the entire spectrum of surgery. In Canada, we have the luxury of choice. We can choose to trade income and professional or academic advancement for personal and family time. This decision is not unique to physicians. Every member of the work force makes this choice. Do you take on a part-time job, extra shifts, or start a small business in addition to your primary job? Or, do you forego the addi-tional income for time? You may choose differently depending on your life stage. What’s important is being aware of this decision and the consequences. You can try but you probably won’t be able to have everything in life and have it on your terms.
UTMJ: Going back to those six nights a month that you are on call: what is one of those nights like?
Dr. Chu: Well, the busiest trauma season time for us is be-tween the Victoria Day and the Thanksgiving long weekends. The rest of the time it can be quiet. As a trauma surgeon, most of us will do two types of trau-ma on call. The first is trautrau-ma team leading (TTL) and the second is taking call as the trauma surgeon. We can be on call for both or only as the trauma surgeon. It is the TTL call that can be very busy. As the TTL, you would direct the resuscitation and as-sessment of each trauma patient who is referred to your centre. As the trauma surgeon, you would only be called to operate or for advice regarding man-agement issues. The incidence of trauma patients requiring a general surgical procedure is declining while orthopedic procedures are far more com-mon. The current trend in trauma management is increasingly towards non-operative management. One big factor in this development is improved diagnostic and therapeutic imaging with CT, MRI, and angiography. However, at the same time, we’re seeing more and more penetrating trauma in To-ronto. At Sunnybrook, incidence of penetrating trauma referrals is approximately 20%.
UTMJ: Is there a specialized residency for trauma surgery, or is it something that you pursue through a gen-eral surgery residency?
Dr. Chu: The current model in North America consists of a fellowship following general surgery residency. The fellowship is usually trauma in combination with something else, i.e.. trauma and ICU/critical care, or trauma and what is termed acute care surgery (ACS). Acute Care Surgery is basically the compre-hensive management of the patient that comes to the ER with a surgical problem. ACS has now be-come a specialty in itself. The natural combination is ACS with trauma so a surgeon with this type of training can manage anyone with a surgical
prob-lem (trauma or non-trauma) that presents to the ER.
UTMJ: I imagine there must be some myths and miscon-ceptions that circulate about trauma surgery. Is that an accurate statement? Are there any myths out there that particularly need de-bunking?
Dr. Chu: Only one … trauma surgeons are not God. They are not infallible, not omniscient, not omnipotent, and not omnipresent. God is the OR nurse.
UTMJ: I’m curious to ask, are you still working two months each year in Africa?
Dr. Chu: No. Before we had kids, my wife and I would spend January and February at Galmi hospital. Niger was our version of wintering in Florida. We were able to spend two months in Africa for about 7 or 8 years. Once we had kids, it became a lot more challeng-ing. I continue to go each year and my wife stays with our girls and holds down the fort at home. I go for a much shorter length of time and now look for periods during which my presence will allow the long-term surgeons to take vacation or attend a con-ference. When I am there, I also try to take a lot of call to give the long-term surgeons a break.
UTMJ: What do you do while you’re there?
Dr. Chu: We have returned to the same missionary hospi-tal each year so we are now very familiar with the staff, the procedures and routines, the pathology, and what it takes to live there. While we’re there, my wife would cover adult medicine, pediatrics, and some obstetrics. I would do general surgery in the traditional sense: GI surgery, thoracic surgery, head and neck, orthopedics, plastics, urology, lots of ob-stetrics and gynecology. The first few years were very stressful as I had no idea what I was seeing in the clinic let alone what the correct management was. You basically do an entire residency in tropi-cal surgery. Fortunately, I had great teachers in the form of older missionary surgeons and the Nigerien nurses who had seen everything and every form of management that had ever been attempted. What I have discovered is that working in Africa makes me a better trauma surgeon and being a trauma surgeon makes me a better surgeon in Africa. In both settings, I drift into other surgical disciplines. At home, I pay attention to the decision-making un-dertaken by my colleagues in orthopedics, plastics, and neurosurgery. I have also emailed cases back to these colleagues for advice.
UTMJ: What drew you to this particular mission hospital in Africa?
Mis-Interview
Interview with Dr. Peter Chu
sion what doctors they need at which times of the year. Doctors tell World Medical Mission what they can do and when they’re available. World Medical Mission then tries to match the two lists. When I was finishing my residency, I did the “medical mission match,” and they told me about this one hospital in West Africa in Niger that could really use a surgeon but they had great difficulty finding volunteers. I didn’t know any better so I said I would go. When I got there I realized why it was so hard to get sur-geons to go to Niger: it is a physically tough place to live in and is very under-developed. It consistently places within the bottom five in the annual UN ranking of economic development.
UTMJ: Do you have any fellow colleagues that go to Africa as well?
Dr. Chu: Yes. There are many doctors at U of T who volun-teer in Africa. Dr. Liesly Lee is a neurologist based at Sunnybrook. He has volunteered in Niger with me, in Kenya, and in Angola. Dr. Georges Azzie, a pediatric surgeon at Sick Kids, is probably the gen-eral surgeon at U of T who has the greatest experi-ence in international surgery. He has worked in the Middle East, Sierra Leone, Ghana, and is currently leading a very innovative surgical training program in Botswana.
UTMJ: That sounds similar to the University of Toronto psychiatry residency program, that takes psychiatry residents to Ethiopia.
Dr. Chu: Yes. The relationship between the University of Toronto and the Black Lion Hospital in Ethiopia is a major success story. The index specialty which started it all off was psychiatry. They have successful-ly graduated several classes of psychiatry residents. The program has expanded to now include twinned training programs in emergency medicine, internal medicine and most recently, a family medicine resi-dency. The person to talk to is Dr. Clare Pain, a psy-chiatrist at the Mount Sinai Hospital. The program she coordinates is called the Toronto Addis Ababa Academic Collaboration (www.taaac.ca).
UTMJ: When you go to Africa, are you just treating patients or are you also doing any training?
Dr. Chu: Both. There are usually elective medical students and the occasional resident there from North America, Europe or Australia, as well as Nigerien students rotating to Galmi from the medical school in Niamey. In the past, both my wife and I have brought Canadian residents with us to Galmi.
UTMJ: What advice would you give to medical students who have an interest in trauma surgery?
Dr. Chu: I think the first thing would be to concentrate on being well trained during your surgical residency. You don’t have to be a technical superstar, but you have to be technically capable, understand your anatomy, and know your way around the body, be-cause tissue planes in operative trauma are often bloodstained or destroyed. Second, you need to plan ahead and always have a plan B, and maybe even a plan C. Third, you need to be able to handle stressful situations without decompensating. There can be a lot of Brownian motion during a trauma resuscitation. The trauma team leader needs to re-main outwardly calm, organize the team, formulate a plan, and clearly communicate that plan to the entire team. Fourth, learn your internal medicine and critical care medicine well. It will help you man-age the critically ill patient with multisystem inju-ries. Fifth, you should develop an interest outside of medicine to keep you sane. You need some form of release and self-therapy such as sports, art, carpen-try, etc. Unfortunately, much of trauma is dealing with people who have made foolish or unsafe deci-sions resulting in the loss of life and/or a life of loss in the form of disability or grieving families. You will face this apparent waste of the precious gift of life and deal with crying families all because of the deci-sions that were made.
UTMJ: Is there anything else you think is really important for student readers to know?
Dr. Chu: Probably what I shared with your class at the end of my lecture [in first year], the whole Alice in Wonderland thing: When facing a fork in the road, Alice didn’t know where she wanted to go, so the Cheshire Cat pointed out that it didn’t matter which path she took. I would encourage the read-ers to think of what are the most important things in their lives, where do they want to go and who do they want to be. If you know what your priorities are, where your destination is, who you want to be, then you have a framework with which to consider all the decisions that will come your way in life. It’s important to fit medicine around your life rather than your life around medicine.