Functioning at School Age of Moderately Preterm
Children Born at 32 to 36 Weeks’ Gestational Age
WHAT’S KNOWN ON THIS SUBJECT: Information on long-term development and functioning of moderately preterm children is scarce, despite the numbers of children involved (6% to 9% of all births) and their vulnerability resulting from their immature brain development at the time of birth.
WHAT THIS STUDY ADDS: This study adds empirical data on school situation, cognitive performance, and socioemotional functioning assessed by mothers, fathers, and teachers, of moderately preterm children in comparison to term-born children at school age. The preterm group specifically shows attention difficulties.
abstract
OBJECTIVE:To study outcome of low-risk moderately preterm birth between 32 and 36/7 weeks’ gestation.
METHODS:377 Moderately preterm children (M: 34.7, SD: 1.2 complete weeks), without need for neonatal intensive care and without dysma-turity or congenital malformations, were compared with 182 term chil-dren and assessed at eight years (M: 8.9, SD: 0.54). School situation, IQ, sustained attention, behavior problems, and attention-deficit/ hyperactivity characteristics were studied.
RESULTS:Special education was attended by 7.7% of the moderately preterm children, more than twice the rate of 2.8% in the general Dutch population of this age. Additional exploration for two preterm sub-groups of 32 to 33 versus 34 to 36 weeks’ gestation showed a need for special education in 9.7% versus 7.3% and a significant difference in grade retention for 30% versus 17%, respectively. Of the children at-tending mainstream primary schools, grade retention was found in 19% of the preterm versus 8% of the comparison children. Adjusting for maternal education, a group difference of 3 points was found in IQ. The preterm children needed more time for the sustained attention task. The preterm children had more behavior problems (specifically internalizing problems with 27% scoring above the borderline cut-off ), as well as more attention-deficit/hyperactivity disorder characteris-tics (specifically attention deficits).
CONCLUSIONS:Cognitive and emotional regulation difficulties affect functioning of moderately preterm children, as school problems, a slightly lower IQ, attention and behavioral problems are found when they are compared with term-born children. Identification and moni-toring of precursors of these problems at younger age is needed in view of prevention purposes.Pediatrics2009;124:251–257
CONTRIBUTORS:Anneloes L. van Baar, PhD,aJohn Vermaas,
Msc,a,bEdwin Knots, MD, Msc,cMartin J. K. de Kleine, MD, PhD,d
and Paul Soons, PhDa,e
aDepartment of Pediatric Psychology, Tilburg University, Tilburg,
Netherlands;bDepartment of Medical Psychology, Twee Steden
Hospital, Tilburg, Netherlands;cDepartment of Pediatrics,
Catharina Hospital, Eindhoven, Netherlands;dDepartment of
Neonatology, Ma´xima Medical Center, Veldhoven, Netherlands;
eDepartment of Medical Psychology, St Anna Hospital, Geldrop,
Netherlands
KEY WORDS
preterm children, attention, behavior problems, IQ, school age
ABBREVIATIONS
ADHD—attention-deficit/hyperactivity disorder CBCL—Child Behavior Checklist
TRF—Teacher Report Form
www.pediatrics.org/cgi/doi/10.1542/peds.2008-2315
doi:10.1542/peds.2008-2315
Accepted for publication Nov 6, 2008
Address correspondence to Anneloes L. van Baar, PhD, Utrecht University, Faculty of Social Sciences, PO Box 80140, 3508 TC, Utrecht, Netherlands. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE:The authors have indicated they have no financial relationships relevant to this article to disclose.
occurs in 9% of all births in the United States and 6.3% of all births in the Dutch population, around 11 000 chil-dren per year.1,2An increase in these
rates was found between 1992 and 2003.2 Most of these moderately
pre-term infants survive with declining mortality rates.3Information on
devel-opment of moderately preterm chil-dren is scarce, despite the large prev-alence and the potential risk for immature brain development. At 34 weeks of gestational age, the overall brain weight is only 65% of brain weight at 40 weeks.4 Potential brain
damage as a result of premature birth can occur during the last weeks of gestation to term age in the structural maturational processes of the brain, which include increasing neuronal connectivity, dendritic arborization, in-crease in synaptic junctions, and mat-uration of neurochemical and enzy-matic processes.
Previous reports on outcomes have used various definitions for over-lapping gestational ages, with some studies describing infants of 35 to 36.6 weeks’ gestation as near term and other studies describing infants of 34 to 36 weeks’ gestation as late-preterm.5 In respect to neonatal
out-comes, it has been found that infants born at 35 to 366⁄7 weeks’ gestation
have more medical problems com-pared with term infants.6 Preschool
readiness testing in Florida showed that 13.6% of late-preterm children versus 11.8% of term children re-quired special education at 5 years of age.7 In the United Kingdom, 7% of
7-year-old children born between 32 and 35 weeks’ gestation needed spe-cial education and 19% had an abnor-mal hyperactivity score.8Danish
regis-ters showed that 37 (6.4%) of 581 children between 2 and 18 years of age who were born between 34 and 36
In this study, the cognitive perfor-mance and socioemotional functioning of moderately preterm and term-born children at school age was compared.
METHODS
Participants
Selection criteria for the preterm chil-dren consisted of: a gestational age at birth of 32 through 36 weeks⫹6 days, no dysmaturity (⬍P10), no NICU admit-tance needed (uniform criteria for ad-mission to a NICU were used by all hos-pitals based on official guidelines from the Dutch Society for Obstetrics and Gynecology and the Dutch Pediatric Association), no severe congenital malformations, and an age of 7 to 9 years. For the term children, the selec-tion criteria were: gestaselec-tion of ⱖ37 weeks, no dysmaturity (⬍P10), no NICU admittance needed, no severe congenital malformations, attending a primary school, and an age of 7 to 9 years.
Instruments
All parents completed a background information questionnaire concerning school situation of the index child, family circumstances and lifestyle during pregnancy, and delivery char-acteristics. Neonatal data of the pre-term children were collected from the hospital files. The parents of the term children answered a question-naire regarding their children’s neo-natal characteristics. Cognitive abili-ties of the children were assessed with the Revised Amsterdam Chil-dren’s Intelligence Test (short version) for children 4 to 11 years of age.10The
norm score (IQ score) is 100 (SD: 15) and the mean for the subtests is 15 (SD: 5). A correlation of .81 was found with a Dutch version of the Wechsler Intelligence Test–Revised.10
used.11 The children are required to
mark configurations consisting of 4 dots as quickly as possible, in 33 rows of 24 figures of 3, 4, or 5 dots. Psychometric properties of the test were found acceptable by the Dutch organization that provides informa-tion on Dutch psychological tests and questionnaires.12
Both parents and teachers were asked to complete a questionnaire on compe-tences and behavior problems of the child; the Child Behavior Check List (CBCL) was filled in by the parents and the Teacher Report Form (TRF) by the teachers.13The CBCL and TRF are
par-allel forms of the same questionnaire with good psychometric qualities.13
CBCL scoring provides an assessment of the total number of behavior prob-lems, as well as separate scores for internalizing and externalizing be-havior problems. A total score of 60 indicates a cutoff score for children with many behavior problems, as was found for 15% of the norm population. The CBCL also provides specific sub-scale scores for anxious/depressed behavior, physical complaints, social problems, thought problems, attention problems, and aggressive behavior.
In addition, parents and teachers an-swered a questionnaire on symptoms of attention-deficit/hyperactivity disor-der (ADHD) of children aged 4 to 18 years.14 This questionnaire provides
both a total score, as well as subscale scores for attention deficit, impulsiv-ity, and hyperactivity. The validimpulsiv-ity, sen-sitivity, and reliability of the test are acceptable.12
Procedure
The participating preterm children were born between January 1996 and January 1998 in 1 of the 7 participating general hospitals in the south of the Netherlands. The preterm children were selected on the basis of the hos-pitals’ archives and their parents were invited to participate.
The term children were pupils of main-stream primary schools in the same geographical region and born between January 1996 and January 1999. Pri-mary schools were approached in the cities where the hospitals are located, as well as in surrounding villages. First, a request to the directors of these schools was made for their school’s participation. Next, the chil-dren were given a letter for their par-ents, which explained the study and requested their participation. If the parents gave their written informed consent, their child was tested in the hospitals or schools by examiners who each tested only preterm or only term children. The study was approved by the Committee of Medical Ethics of the St Elisabeth Hospital in Tilburg and by the committees of the other participat-ing hospitals.
RESULTS
In total, 270 preterm children who were eligible for the study were not included, because they could not be located (42%), could not be studied within the time frame of the examiners (34%), their parents refused participa-tion (5%), or the exact reason for non-participation was unknown (19%). The 377 participating preterm children did not differ in gestational age (34.7 weeks [SD: 1.2] vs 34.8 weeks [SD: 1.2]) or birth weight (2425 g [SD: 455] vs 2422 g [SD: 426]) from the nonpartici-pants. The participants also did not differ from the nonparticipants in way of delivery (82% vs 79% for vaginal de-livery, respectively) and (18% vs 21%
for cesarean delivery, respectively), occurrence of hypoglycemia (13% and 17%, respectively), nor in their need of any oxygen after birth (23% vs 18%, re-spectively). However, the participants had had phototherapy more often (43% vs 31%,2) ⫽8.79; P⬍ .001),
they were discharged from the hospi-tal 2 days sooner (13.6 [SD⫽9.0] vs 15.7 [SD⫽10.0],t1,586⫽2.61;P⬍.01), and they were less frequently part of multiples (22% vs 36%,2⫽14.4;
P⬍.001).
The distribution of 32, 33, 34, 35, and 36 completed weeks of gestation in the participating preterm group consisted of 6%, 11%, 20%, 28%, and 36%, respec-tively. Birth weight was ⬍2500 g in 56% with 2 cases⬍1500 g.
In Table 1, the basic neonatal and de-mographic characteristics are pre-sented of the term and preterm par-ticipants. The characteristics for the subgroup of preterm children, with those attending special education ex-cluded, are presented separately. The preterm participants (both the total and the subgroup) differed as ex-pected from the term children in birth weight, gestational age, duration of stay in the hospital, and number of multiples. The preterm infants were not more frequently born by cesarean delivery (18% vs 13%). No group differ-ences were found in the retrospective reports of any maternal smoking (18% vs 13%), but report of any alcohol use during pregnancy (8% vs 16%,2 ⫽
7.10;P⬍.01) was higher in the term group. The number of mothers and fa-thers who had completed higher edu-cation was lower in the preterm group (see Table 1). Hence, the analyses com-paring functioning of the preterm group to the term group were adjusted for maternal education.
School Outcome
In respect to school outcome, it was found that 29 (7.7%) of the
partici-pating preterm children attended a school for special education com-pared with 2.8% of the Dutch popu-lation of this age group.15 Grade
re-tention of the children attending mainstream primary schools was found in 19% of the preterm group, a significant difference from the 8.8% in the term group (2⫽9.45;P⬍.01).
IQ
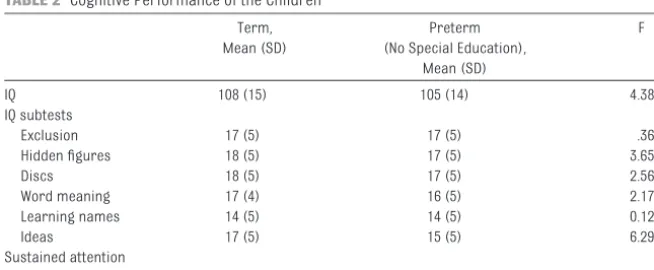
In Table 2, data are presented of the IQ test, excluding the preterm children attending a special school. The multi-ples did not differ from the singletons and had the same mean IQ scores in the preterm group, hence no adjust-ments were made in this regard. The comparisons between the preterm children and the term children are presented, adjusted for maternal edu-cation. With IQ, a small group mean dif-ference of 2.86 (SE: 1.37) was found (F1,495⫽4.38; P⫽.037). The groups
also differed over all subtests (F6,490⫽
2.59; P ⫽ .018), specifically in “idea production” (F6,488⫽6.18;P⫽.013),
that requires the child to name as many products of a certain category as possible within 1 minute and assesses verbal associations and ideational flu-ency (eg, “What can you put into your pocket?”) and marginally in “hidden figures” (F6,490⫽3.65;P⫽.057), which
assesses perceptual reasoning (pat-tern recognition, matching, visual dis-tractibility, and visual analyses) of the children.
Attention
The Bourdon-Vos test showed a group difference in sustained attention to the disadvantage of the moderately pre-term children, adjusted for maternal education: (F1,494 ⫽ 15.5; P ⫽ .000)
(see Table 2). The preterm children (M: 19.7 seconds, SD: 4.8) needed 2 sec-onds more to complete a line than the term children (M: 17.6 seconds, SD: 3.22), which was a significant differ-ence (F1,494⫽21.4;P⫽.000).
ADHD
According to the mothers (F3,484⫽4.09;
P⫽.007), fathers (F3,423⫽ 2.64;P⫽
.049), and teachers (F3,447⫽2.81;P⫽
.039), the preterm children had more ADHD characteristics, as analyzed with a multivariate analyses of variance
ad-justed for maternal education over all 3 subscales. Mothers of preterm children reported more attention deficit and hy-peractivity, whereas their teachers noted only more attention deficit prob-lems (see Table 3). Fathers’ reports showed no group differences for the
mothers and fathers (r⫽0.69) and for mothers and teachers (r⫽0.60).
Behavior Problems
The groups also differed in behavior problems on the CBCL and TRF accord-ing to their mothers and their teach-ers; the fathers did not note group dif-ferences (see Table 3). The difdif-ferences most clearly appeared in internalizing behavior problems. According to the mothers, 27% of the preterm children scored ⬎60, the borderline cutoff score, versus 17% in the term group for internalizing behavior (2⫽6.34;
P⬍ .05); respectively, 16% and 12% scored above borderline for external-izing behavior, a nonsignificant differ-ence. In respect to the specific CBCL subscales, mothers assessed the pre-term children higher in the anxious/ depressed, physical complaints, social problems, thought problems, attention problems, and aggressive behavior di-mensions, but not in the withdrawn/ depressed and rule-breaking dimen-sions (data not shown). Fathers’ ratings did not differ for any of the dimen-sions. The teachers assessed signifi-cantly more behavior problems in the preterm children in the anxious/ depressed, physical complaints, and social capacity dimensions.
Assessments of mothers and fathers for the total problem score correlated strongly (r⫽0.55) and moderately for the mothers and teachers (r⫽0.43).
Neonatal Characteristics and Subgroups in Relation to Outcome Measurements of All Preterm Children
Logistic regression analyses employ-ing “need for special education” as a dependent variable and gestational age, birth weight, duration of hospital stay, hypoglycemia, need for oxygen, and phototherapy as predictors dem-(Total Group) (No Special Education)
Gender, %
Boys 47 52 51
Girls 53 48 49
Gestation
Mean (SD), wk 39.5 (1.4) 34.7 (1.2)a 34.6 (1.2)a
Range, wk 37–43 32–36 32–36
Birth weight
Mean (SD), g 3431 (441) 2425 (455)a 2425 (439)a
Range, g 2385–4750 1340–4130 1340–3564
Time in hospital 1.3 (2.3) 15.7 (10.0)b 15.3 (9.7)a
Mean (SD), d
Range, d 0–11 2–51 2–51
Multiples, % 3 22a 24a
Ethnic origin: Dutch, % 91 96 96
Mothers’ education, %
Primary level 4 4 4
Secondary level 66 78 78
Tertiary level 30 17a 18a
Fathers’ education, %
Primary level 1 3 3
Secondary level 58 67 67
Tertiary level 41 29b 30b
Father employed, % 98 98 98
Mother employed, % 81 73 75
ttest and2analyses comparing the term and total preterm group as well as the term and preterm subgroup with children
needing special education excluded.
aP⬍.01. bP⬍.05.
TABLE 2 Cognitive Performance of the Children
Term, Mean (SD)
Preterm (No Special Education),
Mean (SD)
F
IQ 108 (15) 105 (14) 4.38a
IQ subtests
Exclusion 17 (5) 17 (5) .36
Hidden figures 18 (5) 17 (5) 3.65
Discs 18 (5) 17 (5) 2.56
Word meaning 17 (4) 16 (5) 2.17
Learning names 14 (5) 14 (5) 0.12
Ideas 17 (5) 15 (5) 6.29a
Sustained attention
Bourdon-Vos test 5.79 (3.2) 6.99 (2.9) 15.05b
Univariate analysis of variance for IQ and Bourdon-Vos test; multivariate analysis of variance for IQ subtests, adjusted for maternal education.
onstrated a significant effect for dura-tion of hospital stay (Exp[B] ⫽ 1.044 [95% confidence interval: 1.007–1.082]); P⫽.019), with a mean of 19.2 days (SD: 13.1) in the special education group versus 15.3 (SD: 9.7). Using grade re-tention as the dependent variable, no relationships were found with these predictors.
For IQ scores in relation to completed weeks of gestation, we found that the 21 children with a gestational age of 32 weeks differed with a mean IQ of 96 (SD: 14.5) from the later-born preterm children (mean IQ scores varying from 102–104). Comparisons of gestational age subgroups (32 to 336⁄7weeks [n⫽
62] vs 34 to 366⁄7 weeks [n ⫽ 315])
showed no differences in outcome re-garding special education (9.7% vs 7.3%,2⫽.412;P⫽.521). These
sub-groups did differ in grade retention, which was 30% in the youngest group and 17% for the late-preterm sub-group (2⫽5.46;P⬍.01).
Multivari-ate analysis of variance corrected for maternal education on all outcome measurements showed only 1 differ-ence: the CBCL assessment of the mothers indicated more behavior problems in the late-preterm sub-group (F1,274 ⫽ 5.59; P⫽ .019).
Out-come of the preterm children on all measurements did not differ in rela-tion to need for oxygen (23%, F8,228⫽
1.23;P⫽.28), or phototherapy (43%,
F8,262⫽1.36;P⫽.22) or hypoglycemia
(13%, F8,217⫽.678;P⫽.71).
DISCUSSION
More than twice as many moderately preterm born children attend special education schools compared with the registration for the general Dutch pop-ulation.15 This finding, in itself,
indi-cates a relatively large amount of cog-nitive or behavioral problems for the preterm group.
Although the moderately preterm chil-dren who attended mainstream pri-mary schools at 7 to 9 years of age are functioning relatively well, they still dif-fer from their term-born peers. Overall the results show a pattern of subtle but clear differences to the disadvan-tage of the moderately preterm chil-dren. These children have repeated a grade more often, indicating learning or adaptation problems. A slightly lower mean IQ of 3 points is found for the preterm children, which is not considered a clinically relevant differ-ence. However, they also show more difficulties in the sustained attention task. Their mothers assess more be-havior problems, except for the impul-sivity dimension of the ADHD rating and the withdrawn/depressed and rule-breaking dimension of the CBCL. In addition, the teachers of the pre-term children also report more atten-tion deficits and internalizing prob-lems, specifically regarding anxious/ depressed behavior, physical com-plaints, and social capacities. The fa-thers of the preterm children rate their children somewhat higher on the ADHD characteristics, but their ratings of both groups do not differ in more specific dimensions of behavior problems.
When exploring the importance of neo-natal characteristics, it was found that the children born at 32 weeks’ gesta-tion had a 6 to 8 points lower IQ com-pared with the later-born preterm
chil-TABLE 3 Ratings of Mothers, Fathers, and Teachers on ADHD and Behavior Problems
Term, Mean (SD)
Preterm (No Special Education),
Mean (SD)
F
Mothers
ADHD questionnaire
Attention deficit 2.80 (2.02) 3.47 (2.44) 8.18a
Hyperactivity 3.08 (2.10) 3.78 (2.34) 9.82a
Impulsivity 3.05 (2.19) 3.50 (2.33) 3.71
ADHD total 2.57 (1.90) 3.17 (2.26) 7.97a
CBCL
Total problems 47.91 (10.16) 51.92 (9.46) 16.70a
Internalizing problems 49.78 (10.25) 53.03 (9.38) 11.18a
Externalizing problems 47.60 (9.58) 49.41 (9.65) 3.07
Fathers
ADHD questionnaire
Attention deficit 2.88 (1.82) 3.31 (2.37) 3.24
Hyperactivity 3.18 (2.13) 3.55 (2.31) 2.22
Impulsivity 3.39 (2.15) 3.42 (2.34) 0.04
ADHD total 2.64 (1.84) 3.07 (2.28) 3.55
CBCL
Total problems 46.67 (10.87) 47.92 (9.70) 1.07
Internalizing problems 47.72 (10.25) 49.00 (9.51) 1.31
Externalizing problems 46.62 (9.82) 47.27 (9.44) 0.43
Teachers
ADHD questionnaire
Attention deficit 2.61 (2.22) 3.27 (2.78) 5.00b
Hyperactivity 3.14 (2.28) 3.38 (2.59) 0.62
Impulsivity 2.58 (2.15) 3.08 (2.63) 3.13
ADHD total 2.46 (1.98) 2.91 (2.55) 2.62
CBCL
Total problems 48.28 (8.29) 50.60 (8.46) 6.10b
Internalizing problems 47.89 (8.82) 51.43 (9.46) 13.00a
Externalizing problems 48.55 (7.60) 49.20 (7.88) 1.29
The F scores are based on univariate analysis of variance adjusted for maternal educational levels.
aP⬍.01. bP⬍.05.
was found in the children requiring special education. Dividing our pre-term sample into 2 subgroups of 32 to 33 versus 34 to 36 weeks’ gestation showed a clear difference in grade re-tention to the disadvantage of the youngest group. These preterm sub-groups did not differ in the other out-come measures, except for more be-havior problems assessed by mothers in the late-preterm subgroup. Conse-quently, the late-preterm children are also at risk, although the risk for prob-lems in developmental outcome is somewhat higher in the shortest ges-tational age subgroups.
The findings of our study of 8-year-olds show almost the same percent-age of children needing special edu-cation as found in a similar study on 5-year-olds from the United Kingdom.8
School outcome of the preterm chil-dren (32–36 weeks’ gestation) in the Early Childhood Longitudinal Study-Kindergarten Cohort from the United States indicated a higher need for special education services, varying from 10.1% to 11.3% in the 32 to 33 weeks’ gestation subgroup and 9.3% to 9.7% in the 34 to 36 weeks’ gesta-tion subgroup, in comparison with 9.4% to 9.7% in the term group.16
Although hyperactivity was found in 2 studies,8,9 our study indicates more
internalizing problems of the pre-term children, specifically attention difficulties.
The attention difficulties of the mod-erately preterm children indicate reg-ulation difficulties that may underlie their cognitive and behavioral prob-lems. The disturbance in early brain development because of premature birth and its associated treatment may have contributed to this outcome, as well as the underlying causes of premature birth or (epi-)genetic pro-cesses. More specific neonatal
prob-tional age and duration of hospital stay showed direct relations with outcome measures.
Information on the neonatal treatment and diagnoses of these moderately preterm children could not be col-lected in greater detail. The hospitals varied in their data collection and only 1 had computerized records. However, it is important to note that none of the children had been seriously ill and no intensive care treatment was needed. Recovery from preterm birth, as well as feeding difficulties, may have af-fected brain development. In addition, the bonding and interaction processes between parents and infants may have affected their development. The lower level of parental education may also have influenced the stimulation of the children.
The analyses reported are adjusted for the difference in maternal education, which may be a form of overcorrec-tion. Moderate prematurity may in it-self be associated with maternal edu-cation, in that higher educated women may better adjust their lifestyle to their pregnancy, or may seek help more efficiently in case of signals of premature labor.17
Clearly, the developmental outcome of our moderately preterm born chil-dren without need for neonatal in-tensive care treatment is much bet-ter than the results found for very preterm children with a gestational age of ⬍32 weeks.18 However, the
kind of difficulties found in function-ing of the moderately preterm chil-dren do conceptually match those of the very preterm children. This em-phasizes the importance of the period of brain development between 32 and 37 weeks’ gestational age. Although many (moderate) preterm children can survive, they cannot benefit from the neurobiological processes (eg,
re-womb that may be specifically impor-tant for brain development and un-derlie the development of attention. Also, the formation of a mirror neu-rons system, possibly already present at birth,20may be disturbed because
of the different experiences in motor actions accompanying the changes in the immediate environment (womb or isolette). Hence, additional study of the development of all infants in the phase between 32 weeks’ gestation until term age is necessary. Moder-ately preterm children should also be studied during infancy and at pre-school age, because early signs of regulation and attention difficulties could be used to design focused inter-vention programs. In addition, studies are needed on parent-child interaction and the quality of the stimulation pro-vided. Although it seems to have less serious consequences than very pre-term birth, moderately prepre-term birth certainly needs additional attention.
ACKNOWLEDGMENTS
REFERENCES
1. Stichting Perinatale Registratie Nederland. Perinatale Zorg in Nederland 2006. Utrecht, Netherlands: Stichting Perinatale Registratie Nederland; 2008
2. Raju TNK. Epidemiology of late preterm (near-term) births.Clin Perinatol.2006;33(4):751–763
3. Tomashek KM, Shapiro-Mendoza CK, Davidoff MJ, Petrini JR. Differences in mortality between late-preterm and term singleton infants in the United States, 1995–2002.J Pediatr.2007;151(5): 450 – 456
4. Kinney HC. The near-term (late preterm) human brain and risk for periventricular leukomalacia: a review.Semin Perinatol.2006;30(2):81– 88
5. Engle WA. A recommendation for the definition of “late preterm” (near-term) and the birth weight-gestational age classification system.Semin Perinatol.2006;30(1):2–7
6. Wang ML, Dorer DJ, Fleming MP, Catlin EA. Clinical outcomes of near-term infantsPediatrics. 2004;114(2):372–376
7. Adams-Chapman I. Neurodevelopmental outcome of the late preterm infant.Clin Perinatol.2006; 33(4):947–964
8. Huddy CLJ, Johnson A, Hope PL. Educational and behavioral problems in babies of 32–35 weeks gestation.Arch Dis Child Fetal Neonatal Ed.2001;85(1):F23–F28
9. Linnet KM, Wisborg K, Agerbo E, Secher NJ, Thomsen PH, Henriksen TB. Gestational age, birth weight, and the risk of hyperkinetic disorder.Arch Dis Child.2006;91(8):655– 660
10. Bleichrodt N, Drenth PJD, Zaal JN, Resing WCM.RAKIT Handleiding bij de Revisie Amsterdamse Kinder Intelligentie Test. Lisse, Netherlands: Swets & Zeitlinger; 1987
11. Vos P. Handleiding Bourdon-Vos Test, 3e Herziene Uitgave. Lisse, Netherlands: Swets Test Publishers; 1998
12. Evers A, van Vliet-Mulder JC, Groot CJ.Documentatie van Tests en Testresearch in Nederland Deel I Testbeschrijvingen. Assen, Netherlands: Van Gorcum; 2000
13. Achenbach TM, Rescorla LA.Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, and Families; 2001
14. Scholte EM, van der Ploeg JD.ADHD-Vragenlijst (AVL) Handleiding. Lisse, Netherlands: Swets & Zeitlinger; 2004
15. Central Institution of Statistics/Centraal Bureau voor de Statistiek. Basisonderwijs; leerlingen 2005/2006. Available at: http://statline.cbs.nl/StatWeb. Accessed May 14, 2008
16. Chyi LJ, Lee HC, Hintz SR, Gould JB, Sutcliffe TL. School outcomes of late preterm infants: special needs and challenges for infants born at 32 to 36 weeks gestation.J Pediatr.2008;153(1):25–31
17. Reedy NJ. Born too soon: the continuing challenge of preterm labour and birth in the United States.J Midwifery Womens Health.2007;52(3):281–290
18. Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood.Lancet.2008;371(9608):261–269
19. Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinemia during early pregnancy and subsequent child development: a 3-year follow-up study.Clin Endo-crinol (Oxf).2003;59(3):282–288
20. Lepage J-F, The´oret H. The mirror neuron system: grasping others’ actions from birth?Dev Sci. 2007;10(5):513–523
DOI: 10.1542/peds.2008-2315
2009;124;251
Pediatrics
Soons
Anneloes L. van Baar, John Vermaas, Edwin Knots, Martin J. K. de Kleine and Paul
Services
Updated Information &
http://pediatrics.aappublications.org/content/124/1/251
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/124/1/251#BIBL
This article cites 13 articles, 3 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_
Fetus/Newborn Infant
rning_disorders_sub
http://www.aappublications.org/cgi/collection/cognition:language:lea
Cognition/Language/Learning Disorders
al_issues_sub
http://www.aappublications.org/cgi/collection/development:behavior
Developmental/Behavioral Pediatrics following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2008-2315
2009;124;251
Pediatrics
Soons
Anneloes L. van Baar, John Vermaas, Edwin Knots, Martin J. K. de Kleine and Paul
Weeks' Gestational Age
Functioning at School Age of Moderately Preterm Children Born at 32 to 36
http://pediatrics.aappublications.org/content/124/1/251
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.