Effects of Anorexia Nervosa on Clinical, Hematologic, Biochemical, and
Bone Density Parameters in Community-Dwelling Adolescent Girls
Madhusmita Misra, MD*‡; Avichal Aggarwal, MD*; Karen K. Miller, MD*; Cecilia Almazan, BS*; Megan Worley, BA*; Leslie A. Soyka, MD§; David B. Herzog, MD㛳; and Anne Klibanski, MD*
ABSTRACT. Objective. Anorexia nervosa (AN) is an eating disorder that leads to a number of medical se-quelae in adult women and has a mortality rate of 5.6% per decade; known complications include effects on he-matologic, biochemical, bone density, and body compo-sition parameters. Few data regarding medical and devel-opmental consequences of AN are available for adolescents, in particular for an outpatient community-dwelling population of girls who have this disorder. The prevalence of AN is increasing in adolescents, and it is the third most common chronic disease in adolescent girls. Therefore, it is important to determine the medical effects of this disorder in this young population.
Methods. We examined clinical characteristics and performed hematologic, biochemical, hormonal, and bone density evaluations in 60 adolescent girls with AN (mean age: 15.8 ⴞ 1.6 years) and 58 healthy adolescent girls (mean age: 15.2ⴞ1.8 years) of comparable maturity. Nutritional and pubertal status; vital signs; a complete blood count; potassium levels; hormonal profiles; bone density at the lumbar and lateral spine; total body, hip, and femoral neck (by dual-energy x-ray absorptiometry) and body composition (by dual-energy x-ray absorptiom-etry) were determined.
Results. All measures of nutritional status such as weight, percentage of ideal body weight, body mass in-dex, lean body mass, fat mass, and percentage of fat mass were significantly lower in girls with AN than in control subjects. Girls with AN had significantly lower heart rates, lower systolic blood pressure, and lower body tem-perature compared with control subjects. Total red cell and white cell counts were lower in AN than in control subjects. Among girls with AN, 22% were anemic and 22% were leukopenic. None were hypokalemic. Mean age at menarche did not differ between the groups. How-ever, the proportion of girls who had AN and were pre-menarchal was significantly higher compared with healthy control subjects who were premenarchal, despite comparable maturity as determined by bone age. Ninety-four percent of premenarchal girls with AN versus 28% of premenarchal control subjects were above the mean age at menarche for white girls, and 35% of premenarchal
AN girls versus 0% of healthy adolescents were delayed >2 SD above the mean. The ratio of bone age to chrono-logical age, a measure of delayed maturity, was signifi-cantly lower in girls with AN versus control subjects and correlated positively with duration of illness and mark-ers of nutritional status. Serum estradiol values were lower in girls with AN than in control subjects, and luteinizing hormone values trended lower in AN. Levels of insulin-like growth factor-I were also significantly lower in girls with AN. Estradiol values correlated posi-tively with insulin-like growth factor-I, a measure of nutritional status essential for growth (r ⴝ 0.28). All measures of bone mineral density (zscores) were lower in girls with AN than in control subjects, with lean body mass, body mass index, and age at menarche emerging as the most important predictors of bone density. Bone den-sityzscores of<ⴚ1 at any one site were noted in 41% of girls with AN, and an additional 11% had bone densityz
scores of<ⴚ2.
Conclusions. A high prevalence of hemodynamic, he-matologic, endocrine, and bone density abnormalities are reported in this large group of community-dwelling ad-olescent girls with AN. Although a number of these consequences of AN are known to occur in hospitalized adolescents, the occurrence of these findings, including significant bradycardia, low blood pressure, and puber-tal delay, in girls who are treated for AN on an outpatient basis is of concern and suggests the need for vigilant clinical monitoring, including that of endocrine and bone density parameters. Pediatrics 2004;114:1574–1583; ado-lescent health, anorexia nervosa, blood, bone mineral den-sity, cardiovascular.
ABBREVIATIONS. AN, anorexia nervosa; GH, growth hormone; LH, luteinizing hormone; BMI, body mass index; UFC, urinary free cortisol; CBC, complete blood count; IGF-I, insulin-like growth factor-I; DXA, dual-energy x-ray absorptiometry; BMAD, bone mineral apparent density; BA/CA, ratio of bone age to chronological age; MCV, mean corpuscular volume; RBC, red blood cell; WBC, white blood cell; SA, surface area; LBMD, lumbar spine bone mineral density; LBMAD, lumbar spine bone mineral apparent density.
A
norexia nervosa (AN) is a potentially life-threatening eating disorder characterized by an intense fear of gaining weight, a distorted body image, and amenorrhea. It affects⬃0.2% to 4% of all adolescent girls in the United States,1,2and its incidence has increased at an alarming rate over the past few decades.3 AN represents the third most common chronic illness among adolescent girls,1and the true prevalence may be even higher because it goes undiagnosed in up to 50% of cases. The onset is most frequent during the adolescent years (bimodalFrom the *Neuroendocrine Unit, ‡Pediatric Endocrine Unit, and㛳Eating Disorders Unit, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts; and §Department of Pediatrics, University of Massachusetts Medical School, Worcester, Massachusetts.
Accepted for publication May 28, 2004.
Drs Misra and Aggarwal contributed equally to this work. doi:10.1542/peds.2004-0540
No conflict of interest declared.
Reprint requests to (A.K.) Bulfinch 457, Neuroendocrine Unit, Massachu-setts General Hospital, 55 Fruit St, Boston, MA 02114. E-mail: aklibanski@ partners.org
distribution with peaks at 14.5 and 18 years),4 a period during which the majority of physical and psychosocial growth occurs. Critical hormonal and growth-related changes (both statural and organ re-lated) occur during this period, and deprivation of substrates that are essential for growth and develop-ment can hinder these physiologic processes.
AN is associated with a mortality rate of 5.6% per decade in adults,5the highest among all psychiatric illnesses.6Suicide and cardiovascular events are im-portant causes of death in this disorder. Some deaths are of unclear cause and may be attributable to other medical complications.5,7In addition to these serious complications of AN contributing to the mortality associated with this disorder, other significant changes have been reported in hemodynamic, hema-tologic, and bone metabolism parameters in adults with AN.8–14 Although not life-threatening, these complications can be disabling and contribute to the morbidity of this disorder. Many of these complica-tions result from physiologic adaptation to self-im-posed starvation and malnourishment, and a large number are reversible with refeeding, at least in adults.15,16
Several groups have examined and reviewed med-ical complications of AN in adults.8–14 However, data derived from adults cannot be extrapolated to adolescents with this disorder, adolescence being a time when critical changes are occurring in the hor-monal milieu and in growth, very different from adult life, when pubertal development and growth are complete. The data that are currently available regarding the prevalence of medical complications in adolescent girls who have AN are primarily from hospitalized patients with this disorder17,18and from retrospective chart reviews.19–21 Warren and Vande Wiele22 examined 42 hospitalized girls and young women with AN and reported a 26% prevalence of bradycardia, 86% prevalence of hypotension, 64% prevalence of hypothermia, 38% prevalence of leu-kopenia, and 7% prevalence of anemia in a 1973 study without matched healthy control subjects. Shamim et al20 recently reported normalization of orthostatic pulse changes after nutritional rehabilita-tion in hospitalized adolescents with AN. All medi-cal consequences of AN may not be completely re-versible in adolescents, especially changes that pertain to growth, pubertal development, and attain-ment of peak bone mass.23–25
Because AN is increasing in prevalence in adoles-cents and because many of these patients are now being followed as outpatients, it is important to in-vestigate the prevalence of medical complications in community-dwelling adolescents with AN and to determine the predictors of these medical complica-tions. This will allow effective and timely interven-tion and help to reduce the morbidity associated with this eating disorder. The most comprehensive data on medical complications in ambulatory AN adolescents are from a 1988 chart review by Palla and Litt,19 which did not include a healthy control pop-ulation. The authors reported a high prevalence of bradycardia (94%), hypotension (70%), hypothermia (100%), anemia (32%), and neutropenia (38%) in girls
with AN. In a small study of 10 girls, Lambert et al26 reported lower leukocyte and platelet counts in girls with AN than in control subjects. There has been a growing awareness of the prevalence of AN in ado-lescence over the past decade, and monitoring of this condition is usually intensive. It is important to de-termine whether increased monitoring of adolescents who have this eating disorder has resulted in a de-crease in the prevalence of these complications. In this cross-sectional study, we investigated the prev-alence of medical complications in a large communi-ty-dwelling group of adolescent girls who had AN and were receiving multidisciplinary outpatient care at the time of the study as compared with healthy adolescents of comparable maturity, and we also determined demographic and body composition pre-dictors of these complications in the subjects studied.
METHODS Subject Selection and Enrollment
We studied 118 adolescent girls, 60 with AN diagnosed by Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria and 58 healthy control subjects, at Massachusetts General Hospital. A subset of data regarding bone metabolism and hor-monal parameters were reported earlier for 18 AN and 15 healthy subjects in the study by Soyka et al27and for another 19 AN and
20 healthy subjects in the study by Misra et al.28 Primary
end-points for the 2 studies were, respectively, bone density and growth hormone (GH) secretory dynamics in AN compared with healthy adolescents and hemodynamic, hematologic, and bio-chemical parameters were secondary endpoints. Clinical data col-lected at the baseline visit of subjects from both studies were examined to determine the prevalence of medical complications in this population. We also reviewed unpublished data from 23 girls with AN and 23 healthy control subjects. Girls with AN were recruited consecutively at Massachusetts General Hospital through referrals from primary care providers, nutritionists, psy-chiatrists, and therapists and also from day-treatment eating dis-order programs in and around Boston. A diverse referral group better represents community-dwelling girls with AN and pre-cludes selection bias that may occur if all subjects are enrolled from a single center.
All subjects were white and were in the age range of 12.0 to 18.8 years. The duration of amenorrhea in girls with AN ranged from 3 to 36 months, and the time since diagnosis ranged from 1 to 48 months. None of the girls were on any hormonal medications. There was no past or present history of eating disorders in the healthy control subjects. All girls with AN were receiving inte-grated multidisciplinary outpatient therapy at the time of the study. No subject had been hospitalized within 3 months of study initiation. Given the labile nature of this disorder with frequent hospitalizations in sicker patients, a period of 3 months or more without hospitalization was considered a sufficient period to de-fine a community-dwelling population. Our Institutional Review Board approved all studies, and written informed assent and consent were obtained from all subjects and their parents.
Study Procedures
Eligibility for participation in the study was determined during an initial screening visit at Massachusetts General Hospital, which included a history, physical examination, and screening labora-tory tests. Blood was drawn for thyroid-stimulating hormone in all subjects. Follicle-stimulating hormone, luteinizing hormone (LH), hematocrit, potassium, and glucose were recorded in sub-jects who participated in the study by Misra et al,28but these data
in the study because they were tall with heights greater than the 95th percentile for age and weights at approximately the 50th percentile (with percentage of ideal body weight for height ⬍85%). They fit other criteria for AN, including having the body image issues and amenorrhea for 3 months or greater. Hormonal, nutritional, and bone metabolism parameters were assessed.
Eligible subjects were evaluated at the General Clinical Re-search Center of Massachusetts General Hospital. Height and weight were measured. BMI was calculated, and BMI percentiles were determined from published charts.29Hemodynamic
param-eters, including heart rate, blood pressure, and temperature, were measured. A 24-hour urine sample was collected for urinary free cortisol (UFC), calcium, and creatinine. A complete blood count (CBC) and a fasting blood sample for insulin-like growth factor-I (IGF-I) and estradiol were obtained. Not all subjects had every endpoint measured. Bone density, bone age, and body composi-tion were assessed in 44 girls with AN and 48 healthy adolescents.
Anthropometric Measurements
Weight was measured on an electronic scale with the patient wearing a hospital gown, and a single stadiometer was used to measure height. Height was measured in triplicate, and an aver-age of three readings was used. Tanner breast and pubic hair staging was conducted in all subjects. However, breast staging may be unreliable to assess pubertal stage in girls with AN as excessive weight loss and low estrogen levels can result in breast atrophy. Therefore, bone age was obtained from an radiograph of the left hand and wrist using the methods of Greulich and Pyle.30
Subjects were classified as immature when bone age (BA) was⬍15 years and mature when BA wasⱖ15 years. BMI [weight in kg/ (height in m)2] percentiles were calculated using published
charts.29
Hematologic Parameters and Biochemical Assessment CBC was determined by the hospital laboratory. Measurements of serum ionized calcium, phosphorus, thyroid-stimulating hor-mone, LH, follicle-stimulating horhor-mone, potassium, prolactin and glucose, and urine creatinine were performed through the hospital laboratory using published methods.31
UFC was measured by the Gammacoat I125radioimmunoassay
(Diasorin Inc, Stillwater, MN; detection limit: 1g/dl; coefficient of variation: 7.0%) using the extraction method. The concentration of free cortisol in the 24-hour urine sample was multiplied by the total volume over 24 hours to obtain the value for UFC ing/day. Radioimmunoassay was used to measure estradiol (Diagnostic Systems Laboratories, Inc, Webster, TX; limit of detection: 2.2 pg/ml; coefficient of variation: 6.5%– 8.9%). An IRMA (Nichols Institute Diagnostics, San Juan Capistrano, CA) with a detection limit of 30g/L and a coefficient of variation of 3.1% to 4.6% was used to measure serum IGF-1.
Bone Density and Body Composition
Total body and anteroposterior lumbar spine (L1–L4) bone densities were measured by dual-energy x-ray absorptiometry (DXA; QDR-4500; Hologic Inc, Waltham, MA). The SD for bone density measurement is 0.01 g/cm2and does not vary with bone
density. Bone density at the hip was also measured for 24 healthy control subjects and 25 girls with AN using a QDR-4500. An estimate of volumetric bone density, ie, bone mineral apparent density (BMAD), was calculated using formulas described by Katzman et al,32as BMAD is a better measure of bone density in
a group that is not matched for height. A whole-body DXA scan was performed to determine the body composition comprising validated measures of fat mass and lean body mass.33–36
Percent-age of body fat was also determined using bioimpedance analy-sis.37
Statistical Analysis
The JMP program (JMP Statistical Data Software; SAS Institute, Inc, Cary, NC) was used for statistical analysis. Anthropometric, bone density, body composition, and biochemical data were ana-lyzed using thettest. The significance was set atP⬍.05 for all comparisons. Univariate regression analysis was used to deter-mine the correlations between variables being tested. Stepwise regression analysis was used to determine significant predictors of bone density. All results are expressed as mean⫾SD.
RESULTS
Clinical and Anthropometric Characteristics
Clinical and anthropometric data are shown in Table 1. Mean duration since diagnosis of AN was 10.5⫾10.4 months, and the duration of amenorrhea was 10.8⫾9.8 months. Chronological age, bone age, and Tanner stage did not differ between the groups. However, the ratio of bone age and chronological age was significantly lower in girls with AN than in healthy adolescents, suggestive of a delay in pubertal maturation. Girls with AN were taller than healthy control subjects in this particular group. Midparental height did not differ between the 2 groups.
BMI and weight were lower in girls with AN than in control subjects, as expected. In the AN group, total fat mass measured by DXA was significantly lower (⬍50%) than in healthy control subjects, and lean mass was also lower. Percentage of body fat (measured by DXA) was substantially reduced in girls with AN. Percentage of trunk fat was signifi-cantly lower in girls with AN (32.4⫾5.1% vs 37.9⫾ 5.1%;P⬍.0001), whereas percentage of extremity fat was comparable in the 2 groups. Ratio of trunk to extremity fat was lower in AN than in healthy ado-lescents (0.57⫾ 0.13 vs 0.67⫾0.14; P⫽ .0008). The duration of illness was found to correlate inversely with BMI (r⫽ ⫺0.40,P⬍.0001), lean body mass (r⫽ ⫺0.30,P⫽.004), total fat mass (r⫽ ⫺0.40,P⫽.0001), and 8% body fat (r⫽ ⫺0.38,P⫽ .0002).
Sixty-four percent of girls with AN had been hos-pitalized for treatment of eating disorders 3 months or more before study entry. Thirty-two percent of girls with AN and 26% of control subjects had sus-tained fractures during childhood or adolescence. No specific type of fracture was prevalent in either group.
Medication use is shown in Table 2. Sixty-two percent of patients with AN reported use of at least 1 psychiatric medication, and 14% reported use of 2 or more psychiatric medications at the time of the visit. Fifty-two percent reported taking antidepres-sants, 4% were on anxiolytics, and 6% of patients reported use of antipsychotics. Forty percent of the girls with AN were regularly taking multivitamins as compared with 4% of control subjects, and 20% of girls with AN reported taking regular calcium sup-plements compared with ⬍2% of healthy control subjects. In addition, 12% of girls with AN were taking antireflux, gastrointestinal motility, or stool-softening medications.
Menstrual Function
35% were delayed ⬎2 SD (ie, ⬎15.3 years). Con-versely, only 28% of premenarchal healthy subjects were older than 12.8 years, and none was older than 15.3 years. Of girls who had AN and had attained menarche, 32% had menarche at an age greater than the mean age of menarche. Primary amenorrhea was noted in 3 girls with AN. The ratio of bone age to chronological age (BA/CA) correlated inversely with duration of illness and positively with markers of nutritional status (BMI, lean and fat mass, percent body fat; Table 3).
Hemodynamic Status
Vital signs are detailed in Table 4. Mean heart rate in girls with AN was significantly lower than in control subjects. There was a wide range of heart rate (40 – 88 bpm) in girls with AN, with 27% having a heart rate ⬍56 bpm (ie, mean ⫺ 2 SD for control subjects). Patients with bradycardia (n⫽12) did not differ from patients whose heart rate was at least 56 bpm (n⫽33) when BMI and duration of illness were compared but did have significantly lower percent-age of body fat (13.3⫾3.8% vs 20.0⫾4.5%;P⫽.002) and total fat mass (5.8⫾2.2 vs 9.6⫾3.1 kg;P⫽.009). Overall, heart rate correlated positively with BMI, fat mass, and percentage of body fat and inversely with duration of illness (Table 3). Nine percent of girls with AN had a heart rate of⬍46 bpm (ie, mean⫺3 SD for control subjects).
Mean systolic pressure was lower and diastolic blood pressure trended lower in girls with AN. Di-astolic blood pressure was as low as 46 mm Hg in this group, and mean pulse pressure trended lower. Systolic pressure correlated inversely with duration of illness, and both systolic and diastolic pressures
TABLE 1. Clinical and Anthropometric Data in Girls With AN and Control Subjects
Controls (n⫽58)
AN (n⫽60)
PValue
Chronological age, y 15.2⫾1.8 15.8⫾1.6 NS
Bone age, y 15.7⫾1.7 15.7⫾1.5 NS
Weight, kg 56.5⫾11.1 46.4⫾5.9 ⬍.0001
Height, cm 161.1⫾7.6 163.9⫾6.2 .03
BMI, kg/m2 21.8⫾3.6 16.6⫾1.4 ⬍.0001
Fat mass, kg 18.5⫾5.9 8.8⫾3.0 ⬍.0001
% body fat 31.2⫾6.0 18.5⫾5.1 ⬍.0001
Lean body mass, kg 38.0⫾5.9 35.8⫾4.4 .05
Maturity, bone ageⱖ15 y 70.8% 71.7% NS
BA/CA 1.03⫾0.05 0.98⫾0.06 .0001
Tanner stage, pubic hair 4.1⫾0.8 4.1⫾0.7 NS
Tanner stage, breasts 4.3⫾0.9 4.1⫾0.9 NS
Age at menarche, y 12.2⫾1.0 12.4⫾1.4 NS
Premenarchal 10.6% 28.3% .02
Duration of illness, mo N/A 10.5⫾10.4
Duration of amenorrhea, mo* N/A 10.8⫾9.8
History of fractures 25.5% 31.5% NS
Body composition data were available for 46 healthy control subjects and 45 girls with AN. NS indicates not significant.
* Of the 60 girls with AN, 43 were postmenarchal and had secondary amenorrhea at the time of the study.
TABLE 2. Medication Use in 48 Subjects With AN
Medication % of Patients
Psychiatric medications 62.0
Antidepressants 52.0
Anxiolytics 4.0
Antipsychotics 6.0
Two or more psychiatric medications 14.0
Multivitamins 40.0
Calcium supplements 20.0
Antireflux/gastrointestinal motility/stool softeners
12.0
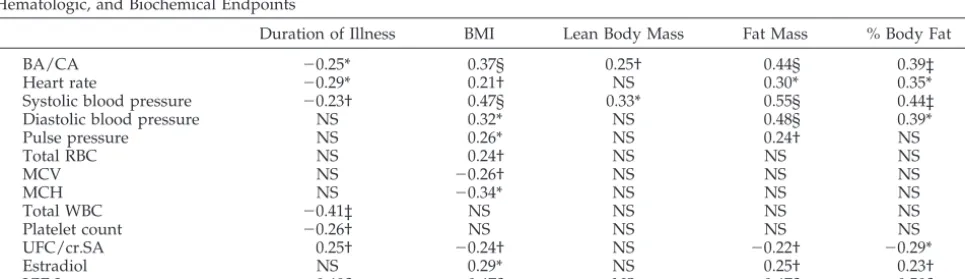
TABLE 3. Correlation Coefficient (r) Between Duration of Illness and Markers of Nutritional Status Versus Maturity, Hemodynamic, Hematologic, and Biochemical Endpoints
Duration of Illness BMI Lean Body Mass Fat Mass % Body Fat
BA/CA ⫺0.25* 0.37§ 0.25† 0.44§ 0.39‡
Heart rate ⫺0.29* 0.21† NS 0.30* 0.35*
Systolic blood pressure ⫺0.23† 0.47§ 0.33* 0.55§ 0.44‡
Diastolic blood pressure NS 0.32* NS 0.48§ 0.39*
Pulse pressure NS 0.26* NS 0.24† NS
Total RBC NS 0.24† NS NS NS
MCV NS ⫺0.26† NS NS NS
MCH NS ⫺0.34* NS NS NS
Total WBC ⫺0.41‡ NS NS NS NS
Platelet count ⫺0.26† NS NS NS NS
UFC/cr.SA 0.25† ⫺0.24† NS ⫺0.22† ⫺0.29*
Estradiol NS 0.29* NS 0.25† 0.23†
IGF-I ⫺0.48§ 0.47§ NS 0.47§ 0.50§
correlated positively with markers of nutritional sta-tus (Table 3). Pulse pressure was predicted by BMI and fat mass. On stepwise regression analysis when BMI, duration of illness, fat mass, and lean mass were entered into the model, fat mass emerged as the single significant predictor of heart rate, systolic and diastolic blood pressures, and pulse pressure, con-tributing to 15%, 33%, 22%, and 10% of the variabil-ity, respectively. Girls with AN had a lower mean oral temperature than healthy control subjects. An inverse correlation was noted between temperature and mean corpuscular volume (MCV;r⫽ ⫺0.38,P⫽ .006).
Hematologic Status
Table 5 shows the mean values of different hema-tologic parameters in girls with AN and control sub-jects. Twenty-two percent of girls with AN had ane-mia (hematocrit⬍37%). When subjects who had AN and anemia (n⫽8) were compared with those with-out anemia (n ⫽ 28), BMI (17.2 ⫾ 1.8 vs 17.0⫾ 1.1 kg/m2; not significant) did not differ between the groups. Duration of illness, fat mass, and lean mass also did not differ. No correlations were observed between hematocrit and measures of nutritional sta-tus or duration of illness. Total red blood cell (RBC) count, however, was significantly lower in girls with AN than in control subjects and was predicted by BMI (Table 3). Thirty-one percent of girls with AN had total RBC counts below normal. MCV was nor-mal in all subjects but was significantly higher in girls with AN when compared with control subjects. An inverse correlation was observed between MCV and BMI. Mean corpuscular hemoglobin was also higher in girls with AN than in control subjects and correlated inversely with BMI. Forty percent of the girls were on multivitamins with variable amounts of iron in the preparations being taken. However, none of the girls were on iron-only pills.
White blood cell (WBC) count in girls with AN was lower than in control subjects. Twenty-two per-cent of girls with AN had leukocyte counts below normal (normal range: 4.5–13 th/mm3). BMI did not differ in girls who had AN and leukopenia (n ⫽ 8) versus those with WBC count in the normal range (n ⫽28; 16.6⫾ 1.4 vs 17.2⫾ 1.3 kg/m2; not signifi-cant). However, there was an inverse correlation be-tween WBC count and duration of illness. Platelet counts did not differ but were predicted by the du-ration of illness.
Biochemical Data
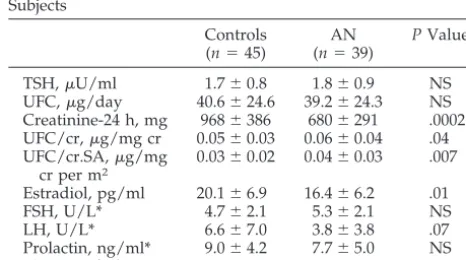
Biochemical data are shown in Table 6. Mean se-rum potassium was slightly higher in the group with AN, possibly because of dehydration (3.8⫾0.3 vs 3.6 ⫾0.2 mmol/L). No subject was hypokalemic (potas-sium⬍3.0 mmol/L), which may be attributed to the fact that only 2 girls with AN reported a history of regular purging. Levels of ionized calcium and phos-phorus were not different in the 2 groups. Calcium excretion in the 24-hour urine sample was found to be normal in all but 2 subjects. Of these 2 subjects, 1 was on a calcium supplement.
UFC standardized for creatinine and for surface area (SA) and creatinine39was significantly higher in girls with AN than in control subjects. Of girls with AN, 12.5% (5 of 40) had mildly elevated UFC (range: 72–115 g/day). Five girls with AN had values of UFC/cr.SA that were elevated above 0.07 g/mg creatinine per m2(mean⫹2 SD for control subjects). UFC/cr.SA correlated positively with duration of illness and duration of amenorrhea and inversely with BMI, fat mass, and lean body mass (Table 3). A strong positive correlation was observed between 24-hour creatinine levels and total lean mass (r ⫽ 0.53,P⬍ .0001).
Serum estradiol concentrations were significantly lower in girls with AN compared with control sub-jects, whereas LH values trended lower in this group All subjects were sampled in the early follicular phase of menstrual cycle to avoid variation in estra-diol levels across a menstrual cycle. Serum estraestra-diol correlated positively with BMI, fat mass, and
per-TABLE 4. Vital Signs in Girls With AN and Healthy Adoles-cents
Controls (n⫽47)
AN (n⫽44)
PValue
Heart rate, bpm 76⫾10 66⫾14 .0004 Blood pressure, mm Hg
Systolic 105⫾11 99⫾9 .005
Diastolic 66⫾8 63⫾9 .07
Pulse pressure, mm Hg 38⫾8 35⫾8 .09 Temperature, °F 98.1⫾0.7 97.7⫾0.5 .01
TABLE 5. Hematologic Parameters in Girls With AN and Control Subjects
Controls (n⫽33)
AN (n⫽36)
PValue
Hematocrit, % 38.2⫾2.5 37.4⫾2.4 NS RBC,⫻106/mm3 4.5⫾0.3 4.3⫾0.3 .001
MCV, fl 84.7⫾4.6 88.2⫾3.5 .0007 MCH, pg/rbc 29.1⫾1.7 30.6⫾1.4 .0003 MCHC, g/dl 34.4⫾1.0 34.7⫾1.0 NS WBC,⫻103/mm3 7.4⫾1.9 5.4⫾1.1 ⬍.0001
Platelet count,⫻103/ mm3 262⫾66 244⫾47 NS
MCHC indicates mean corpuscular hemoglobin concentration.
TABLE 6. Biochemical Data in Girls With AN and Control Subjects
Controls (n⫽45)
AN (n⫽39)
PValue
TSH,U/ml 1.7⫾0.8 1.8⫾0.9 NS UFC,g/day 40.6⫾24.6 39.2⫾24.3 NS Creatinine-24 h, mg 968⫾386 680⫾291 .0002 UFC/cr,g/mg cr 0.05⫾0.03 0.06⫾0.04 .04 UFC/cr.SA,g/mg
cr per m2
0.03⫾0.02 0.04⫾0.03 .007
Estradiol, pg/ml 20.1⫾6.9 16.4⫾6.2 .01
FSH, U/L* 4.7⫾2.1 5.3⫾2.1 NS
LH, U/L* 6.6⫾7.0 3.8⫾3.8 .07
Prolactin, ng/ml* 9.0⫾4.2 7.7⫾5.0 NS IGF-1, ng/ml 505⫾128 315⫾127 ⬍.0001
cr indicates creatinine; TSH, thyroid-stimulating hormone; FSH, follicle-stimulating hormone.
centage of body fat (Table 3) and predicted BA/CA (r ⫽ 0.25,P⫽.03).
Mean serum IGF-1 levels were significantly lower in girls with AN than in control subjects and were reduced by 38% in girls with AN. An inverse corre-lation was observed between IGF-I and duration of illness, and a positive correlation was observed with BMI, fat mass, and percentage of body fat (Table 3). A positive correlation also existed between IGF-I and estradiol (r ⫽0.28, P⫽ .02) and between IGF-I and the ratio of BA/CA (r⫽0.38,P⫽.001). On stepwise regression including BMI, fat mass, and duration of illness, the most significant predictors of IGF-I levels were fat mass and duration of illness, contributing to 32% and 8% of the variability, respectively.
Bone Density
Figure 1 exhibits bone densityzscores in girls with AN versus control subjects. Table 7 shows the pro-portion of girls with AN and control subjects who had zscores⬍⫺1 or⫺2 at the different sites exam-ined. Our results clearly demonstrate significant bone loss in a large number of girls with AN, pri-marily at the lumbar spine. Lumbar spine bone min-eral density (LBMD) z scores and lumbar spine BMAD (LBMAD)zscores were significantly lower in girls with AN than in control subjects. Forty-one percent of girls with AN hadzscores of⬍⫺1, and 9% had z scores of ⬍⫺2 at the lumbar spine. When LBMAD zscores were examined, 39% of girls with AN had zscores of less than ⬍⫺1, and 54% had z scores of⬍⫺2. Bone density at the lateral spine was significantly lower in girls with AN than in control subjects (0.71⫾0.10 vs 0.78 ⫾0.09;P⫽ .0009). Hip and femoral neck BMD z scores were also signifi-cantly lower in girls with AN.Zscores of⬍⫺1 at the hip and at the femoral neck were noted in 30% and 20% of girls with AN.Zscores of between⫺1 and⫺2 at any site were noted in 41% of girls with AN and in 23% of control subjects, whereas z scores of ⬍⫺2 were noted in 11% of girls with AN and in 2% of control subjects (P ⫽.03).
Weight, lean body mass, and fat mass correlated positively with BMD at all skeletal sites in our
sub-jects, whereas an inverse correlation was noted be-tween age at menarche and BMD (Table 8). In addi-tion, BMI correlated positively with LBMD (r⫽0.49, P⬍.0001), LBMAD (r⫽0.48,P⬍.0001), lateral BMD (r⫽ 0.52,P⬍ .0001), hip BMD (r⫽0.45,P ⫽.002), femoral neck BMD (r ⫽ 0.50, P ⫽ .0007), and total body BMD (r⫽0.39,P⫽.0001). On multiple regres-sion analysis when BMI, total fat mass, lean body mass, duration of illness, and age at menarche were entered into the model, lean body mass was the single most significant predictor of BMD at most sites, contributing to 28%, 34%, 43%, and 23% of the variability at the lumbar spine, hip, femoral neck, and total body BMD, respectively. BMI was the most significant predictor of BMD at lateral spine, contrib-uting to 24% of the variability. Age at menarche contributed to an additional 7%, 10%, and 5% of the variability of BMD at the lateral spine, hip, and total body, respectively. Similarly, lean body mass con-tributed to 22%, 29%, 31%, and 19% of the variability of thezscores at the lumbar spine, hip, femoral neck, and total body, respectively, whereas age at men-arche contributed another 8% and 10% to the vari-ability of LBMD and total body BMDz scores. An-other 7% of the variability of LBMD z scores was attributable to the duration of illness.
DISCUSSION
AN is a potentially fatal disorder that commonly affects adolescent girls, and its incidence is increas-ing. We previously reported abnormalities in bone metabolism25,27 and GH alterations in adolescent girls with AN.28 Here we evaluate the overall prev-alence of hematologic, hemodynamic, endocrine, and skeletal abnormalities in a large group of com-munity-dwelling subjects.
Twenty-seven percent of our patients had brady-cardia, with heart rate as low as 40 bpm, and the severity of bradycardia was predicted by the dura-tion of illness and nutridura-tional status. In addidura-tion, both systolic and diastolic blood pressures were found to be significantly lower in girls with AN than in healthy control subjects and were also predicted by length of illness and nutritional status. Fat mass was the most significant predictor of all hemodynamic parameters. In a previous study, we reported that fat
Fig 1. Zscores for lumbar spine, hip, and femoral neck BMD in girls with AN (■) and healthy control subjects (䊐). Girls with AN had significantly lowerzscores at each site than healthy adoles-cents. *P⬍.01; **Pⱕ.001.
TABLE 7. Prevalence of Low Bone Density at Different Sites in Girls With AN and Healthy Control Subjects
Controls (%;n⫽51)
AN (%;n⫽45)
PValue
LBMD .01
Normal 79.2 50.0
Zscore⬍⫺1 18.8 40.9
Zscore⬍⫺2 2.0 9.1
Hip BMD* NS
Normal 91.3 70.0
Zscore⬍⫺1 8.7 20.0
Zscore⬍⫺2 0 10.0
Femoral neck BMD* NS
Normal 86.0 79.6
Zscore⬍⫺1 14.0 13.6
Zscore⬍⫺2 0 6.8
intake in diet is a strong predictor of body fat mass.40 Changes in heart rate and blood pressure thus may be attributable to an adaptive response to weight loss and reduced energy intake. Although bradycardia, postural hypotension, and abnormalities in cardiac function are known to occur in inpatients and in girls with more severe AN,18,20,41the occurrence of signif-icant bradycardia and low blood pressure in ambu-latory girls with AN is of concern. However, the prevalence of bradycardia in this study was much lower than that reported almost 16 years ago by Palla and Litt19(27% vs 94%), which suggests that inten-sive monitoring of this condition in adolescent girls is resulting in an overall improvement in hemody-namic status.
Increased cardiac vagal hyperactivity is thought to cause the bradycardia of adolescent girls with AN.42 Nudel et al43 found abnormal cardiovascular and sympathetic responses to experimental physical ex-ercise in adolescent girls with AN, and QT prolon-gation has also been reported in adults with AN.9,10,19Decreased myocardial contractility and im-paired left ventricular function have been reported in adult women with AN,11,15but no differences were found in myocardial contractility in adolescent girls with AN compared with control subjects.44 How-ever, because cardiovascular events, especially ar-rhythmias, are a common cause of death in AN,45the high prevalence of bradycardia that we found in outpatient adolescent girls who have this eating dis-order, although lower than in the 1988 study by Palla and Litt,19 is disturbing. Monitoring hemodynamic status is necessary not only in adolescents who have AN and are hospitalized but also in community-dwelling adolescents with this eating disorder, and girls with a longer duration of illness seem to be particularly at risk. Because nutritional status, espe-cially fat mass, predicts heart rate and blood pres-sure, it is extremely important to emphasize weight recovery in girls who have AN and are noted to have bradycardia or low systolic or diastolic blood pres-sure. This is supported by a recent report by Shamim et al20 demonstrating normalization of orthostatic pulse changes in girls with AN after nutritional re-habilitation.
Data regarding hematologic complications in am-bulatory adolescents with AN are few. It has been reported that hematologic changes in young women with AN are selectively related to total body fat mass and amount of weight loss in AN.26 Bone marrow hypoplasia has been reported in adults with AN,46
resulting in low RBC, WBC, and platelet counts. Previous studies have reported a prevalence of ane-mia in⬃30% of hospitalized adults with AN.12,13We report a 22% prevalence of anemia in our adolescent subjects with AN. However, this is likely an under-estimate because mild degrees of dehydration are common in AN and may result in spuriously ele-vated hematocrit values. Palla and Litt19 reported 32% of anemia in their retrospective study of an adolescent AN population. Bone marrow suppres-sion and hypoplasia are a likely explanation for ane-mia,26 but dietary deficiencies of serum folate, vita-min B12, and iron may be contributory. Changes in red cell morphology (acanthocytosis, anisocytosis, and poikilocytosis) have been reported in some pre-vious studies.47We found significantly higher MCV and mean corpuscular hemoglobin values in girls with AN than in healthy control subjects predicted by the degree of undernutrition, suggestive of pos-sible relative deficiencies in vitamin B12 or folate intake, although both hematologic parameters were still within the accepted laboratory range. This has not been previously reported.
Twenty-two percent of our girls with AN had low WBC counts. Conversely, adult studies have re-ported leukopenia in as many as 36% of hospitalized AN patients,12 and Palla and Litt reported a 38% prevalence of neutropenia in their adolescent girls with AN.19A positive correlation between BMI and total WBC count in girls with AN suggests that lower BMI in these girls predisposes to lower WBC count in AN. Similarly, Lambert et al26reported that fat mass predicted WBC counts. Although Bowers and Eck-ert48found no increase in infection rates despite the low WBC counts, Devuyst et al12did report a higher incidence of infectious complications in patients who had AN and neutropenia. No serious infection was noted in any subject in our cross-sectional study. Previous reports suggest that the prevalence of ane-mia was either lower than or the same as leukope-nia.13,19,49We report a similar prevalence of anemia and leukopenia in this group of community-dwelling subjects. Although our subjects had a lower inci-dence of leukopenia than those reported in adult, sicker patients with AN and in older adolescent stud-ies,19,22 the report of increased infections in women with lower WBC counts12is of concern and suggests that regular monitoring of CBC may be necessary even on an outpatient basis in adolescent girls who have this eating disorder, especially in girls with a longer duration of illness. In addition, it may be
TABLE 8. Relationship Between Bone Density and Clinical Parameters
Chronological Age
Age at Menarche
Duration of Illness
Duration of
Amenorrhea Weight Height Total Fat
Lean Body Mass
r P r P r P r P r P r P r P r P
LBMD 0.29 .005 ⫺0.27 .02 ⫺0.30 .005 ⫺0.49 .008 0.58 ⬍.0001 0.31 .003 0.43 ⬍.0001 0.58 ⬍.0001 LBMAD 0.19 .07 ⫺0.20 .09 ⫺0.28 .007 ⫺0.28 NS 0.43 ⬍.0001 ⫺0.05 NS 0.41 ⬍.0001 0.27 .01 Lat BMD 0.00 NS ⫺0.38 .001 ⫺0.37 .0004 ⫺0.30 NS 0.54 ⬍.0001 0.15 .09 0.43 ⬍.0001 0.46 ⬍.0001 Hip BMD 0.33 .03 ⫺0.51 .002 ⫺0.21 NS ⫺0.10 NS 0.61 ⬍.0001 0.40 .002 0.43 .005 0.64 ⬍.0001 FN BMD 0.33 .03 ⫺0.41 .02 ⫺0.24 NS ⫺0.22 NS 0.68 ⬍.0001 0.45 .002 0.49 .001 0.69 ⬍.0001 TBMD 0.37 .0003 ⫺0.26 .03 ⫺0.17 NS ⫺0.28 NS 0.49 ⬍.0001 0.29 .005 0.33 .002 0.52 ⬍.0001
necessary to monitor intake and serum levels of mi-cronutrients, including iron, vitamin B12, and folate, and to advise dietary supplements as necessary to treat anemia.
Contrary to the earlier reports showing hypokale-mia19,50in patients with AN, all girls with AN in our study had normal serum potassium levels. This may be attributed to the fact that only 2 of our 48 girls with AN reported regular purging behavior. These findings are in accordance with the work of Green-feld et al,51 who reported that adult patients with purely restricting AN are not at risk for hypokalemia even when their weight is very low. Similar data were reported by Palla and Litt.19However, Powers et al52reported that even with normal serum potas-sium levels, these patients may be at risk for cardiac arrhythmias and other physiologic abnormalities be-cause total body potassium may be low. Hence, mon-itoring for cardiac abnormalities is advisable even when serum potassium is in the normal range.
This study confirmed our previous findings of nor-mal levels of calcium and phosphorus in ambulatory adolescents with AN,25,27,28in contrast to reports of hypocalcemia and hypophosphatemia in an older adolescent AN study.19 It is likely that AN is now being diagnosed earlier than in the past and that earlier intervention is resulting in fewer and less severe disturbances in calcium metabolism.
This study also confirms findings from our previ-ous, smaller studies demonstrating that osteopenia and osteoporosis are highly prevalent in adolescent girls with AN at the lumbar spine.25,27In this study, we demonstrate that BMD z scores at all sites are significantly lower in a large number of girls with AN compared with control subjects. Comparison of the prevalence of osteopenia and osteoporosis at dif-ferent sites, however, suggests that the lumbar spine is the site most affected in girls with AN. BMI, lean body mass, and age at menarche were the most significant predictors of BMD, confirming our find-ings in a smaller number of subjects25,27and concor-dant with findings in other studies.14,53,54Bone den-sity was also lower in girls with a longer duration of illness. Adolescence is a critical time for accrual of bone mass, and 90% of peak bone mass is accrued by the end of the second decade of life.55 Low bone density at this time of life thus is of concern because enough time may not be available for catch-up even if weight recovery does occur,25 especially because many girls who do recover weight will relapse. In-adequate bone mass accrual in adolescence results in increased fracture risk, which may persist despite weight recovery.
A large proportion of girls with AN were pre-menarchal compared with control subjects, and one third of the girls who had AN and were premenar-chal had delayed menarche (menarche not achieved by 15 years). This is also reflected in the lower estra-diol levels in adolescents with AN than in healthy control subjects. Moreover, this study underesti-mates the degree of difference in these levels be-tween healthy control subjects and girls with AN because the healthy girls were studied in the early follicular phase of their cycles, whereas estradiol
lev-els are highest around midcycle. Hypothalamic hy-pogonadism is a well-recognized feature of AN with low LH levels and attenuation of episodic release of the hormone.22,56 As amenorrhea precedes signifi-cant weight loss in a number of patients,57,58weight loss by itself does not completely explain the rela-tionship between nutritional deprivation and men-strual dysfunction, and studies suggest that energy deprivation and emotional stress may also contribute to the hypogonadism seen in AN.
Delayed menarche was a predictor of low bone density in this study, suggesting that hypogonadism may contribute to impaired bone metabolism in AN. Estrogen has important effects in adolescence. In early adolescence, the gradually rising estrogen lev-els are followed closely by increases in levlev-els of GH and IGF-I, both of which are anabolic to bone. In addition, adult levels of estrogen in late adolescence result in a decrease in bone resorption. Estradiol levels in this study were predicted by nutritional status. An improvement in nutritional status there-fore should result in increasing levels of estradiol and thus an increase in bone density. However, ad-ministration of oral estrogen did not improve bone density in adult women or in adolescents with AN.59,60 This study demonstrates very low levels of IGF-I in girls with AN, another possible cause of the low bone density seen in girls with this disorder.
Hypercortisolemia in AN may be a consequence of persistent stress related to this illness and can also contribute to decreased bone density. UFC levels were not different between the 2 groups in this study. This is in contrast to the higher UFC values reported in adult women with AN as compared with healthy control subjects.61 However, Legro et al39 demonstrated that UFC levels increase with increas-ing age through the pubertal years, and standardiz-ing urinary cortisol for creatinine and SA provides a fairly constant value for children in the age range of 12 to 17 years, suggesting that this standardization may be necessary when comparing values in groups that differ in creatinine excretion and SA. When we standardized UFC values for creatinine and SA, val-ues were significantly higher in girls with AN than in control subjects, suggesting that there is hyperactiv-ity of the hypothalamic-pituitary-adrenal axis in AN in adolescence as has been demonstrated previously in adults.62,63 Licinio et al63 reported that hypercor-ticalism in adults with AN was associated with in-creased corticotrophin-releasing hormone levels and normal circulating levels of adrenocorticotropic hor-mone. Failure of cortisol to respond to the dexameth-asone suppression test has also been reported.64 Refeeding causes reversal of these findings, suggest-ing that malnutrition may be responsible for this hypercortisolemia.
most of their adult height potential before develop-ing this disorder and as a result were not stunted for height. Our findings may also be related to a small sample size, and a larger sample may be necessary to sort out differences in adult stature in AN versus control subjects.
We report an increased prevalence of hematologic, metabolic, hemodynamic, and skeletal abnormalities in community-dwelling outpatient girls with AN when compared with healthy subjects, suggesting a need for continued medical monitoring of these pa-rameters in this population. Most of these medical complications relate to the duration of illness and nutritional status of the individual, and in particular fat mass. Girls who have had AN for a prolonged duration are specifically at risk for these complica-tions, as expected, and should be monitored more intensively. In addition, BMI predicts leukopenia; fat mass is an important predictor of hemodynamic complications, and lean body mass predicts bone density; thus, monitoring BMI and body composition is important in girls with AN as a means of predict-ing the risk for these complications. It is reassurpredict-ing to note, however, that the prevalence of medical com-plications in an ambulatory adolescent AN popula-tion, although still high, has decreased compared with older published studies. Intervention in this younger population is often earlier than in adults with AN and thus may be more successful.
ACKNOWLEDGMENTS
This work was supported in part by National Institutes of Health grants M01-RR-01066, DK 062249, and K23 RR018851.
We thank the skilled nursing staff of the General Clinical Re-search Center (GCRC), Ellen Anderson and her Bionutrition staff for the care provided to our subjects at the GCRC, and Gregory Neubauer of the Core Laboratory of the GCRC for analyzing our samples. We also thank our study volunteers, without whose participation this study would not have been possible.
REFERENCES
1. Lucas AR, Beard CM, O’Fallon WM, Kurland LT. 50-year trends in the incidence of anorexia nervosa in Rochester, MN: a population-based study.Am J Psychiatry.1991;148:917–922
2. Von Ranson K, Iacono W, McGue M. Disordered eating and substance abuse in an epidemiological sample: 1. Associations within individuals.
Int J Eat Disord.2002;31:389 – 403
3. Eagles J, Johnston M, Hunter D, Lobban M, Millar H. Increasing inci-dence of anorexia nervosa in the female population of northeast Scot-land.Am J Psychiatry.1995;152:1266 –1271
4. Halmi K, Casper R, Eckert E, Goldberg S, Davis J. Unique features associated with age of onset of anorexia nervosa.Psychiatry Res.1979; 1:209 –215
5. Sullivan P. Mortality in anorexia nervosa.Am J Psychiatry.1995;152: 1073–1074
6. Keel P, Dorer D, Eddy K, Franko D, Charatan D, Herzog D. Predictors of mortality in eating disorders.Arch Gen Psychiatry.2003;60:179 –183 7. Becker A, Grinspoon S, Klibanski A, Herzog D. Eating disorders.N Engl
J Med.1999;340:1092–1098
8. Mehler P. Diagnosis and care of patients with anorexia nervosa in primary care settings.Ann Intern Med.2001;134:1048 –1059
9. Cooke R, Chambers J, Singh R, et al. QT interval in anorexia nervosa.Br Heart J.1994;72:69 –73
10. Galetta F, Franzoni F, Cupisti A, Belliti D, Prattichizzo F, Rolla M. QT interval dispersion in young women with anorexia nervosa.J Pediatr.
2002;140:456 – 460
11. Kalager T, Brubakk O, Bassoe H. Cardiac performance in patients with anorexia nervosa.Cardiology.1978;63:1– 4
12. Devuyst O, Lambert M, Rodhain J, Lefebvre C, Coche E. Haematologi-cal changes and infectious complications in anorexia nervosa: a case-control study.Q J Med.1993;86:791–799
13. Rieger W, Brady J, Weisberg E. Hematologic changes in anorexia ner-vosa.Am J Psychiatry.1978;135:984 –985
14. Grinspoon S, Miller K, Coyle C, et al. Severity of osteopenia in estrogen-deficient women with anorexia nervosa and hypothalamic amenorrhea.
J Clin Endocrinol Metab.1999;84:2049 –2055
15. Gottdiener J, Gross H, Henry W, Borer J, Ebert M. Effects of self-induced starvation on cardiac size and function in anorexia nervosa.Circulation.
1978;58:425– 433
16. Waller E, Wade A, Treasure J, Ward A, Leonard T, Powell-Tuck J. Physical measures of recovery from anorexia nervosa during hospital-ized re-feeding.Eur J Clin Nutr.1996;50:165–170
17. Kreipe R, Goldstein B, DeKing D, Tipton R, Kempski M. Heart rate power spectrum analysis of autonomic dysfunction in adolescents with anorexia nervosa.Int J Eat Disord.1994;16:159 –165
18. Mont L, Castro J, Herreros B, et al. Reversibility of cardiac abnormalities in adolescents with anorexia nervosa after weight recovery.J Am Acad Child Adolesc Psychiatry.2003;42:808 – 813
19. Palla B, Litt I. Medical complications of eating disorders in adolescents.
Pediatrics.1988;81:613– 623
20. Shamim T, Golden N, Arden M, Filiberto L, Shenker I. Resolution of vital sign instability: an objective measure of medical stability in an-orexia nervosa.J Adolesc Health.2003;32:73–77
21. Siegel J, Hardoff D, Golden N, Shenker I. Medical complications in male adolescents with anorexia nervosa.J Adolesc Health.1995;16:448 – 453 22. Warren M, Vande Wiele R. Clinical and metabolic features of anorexia
nervosa.Am J Obstet Gynecol.1973;117:435– 449
23. Nussbaum M, Baird D, Sonnenblick M, Cowan K, Shenker I. Short stature in anorexia nervosa patients.J Adolesc Health Care. 1985;6: 453– 455
24. Lantzouni E, Frank G, Golden N, Shenker R. Reversibility of growth stunting in early onset anorexia nervosa: a prospective study.J Adolesc Health.2002;31:162–165
25. Soyka L, Misra M, Frenchman A, et al. Abnormal bone mineral accrual in adolescent girls with anorexia nervosa.J Clin Endocrinol Metab.2002; 87:4177– 4185
26. Lambert M, Hubert C, Depresseux G, et al. Hematological changes in anorexia nervosa are correlated with total body fat mass depletion.Int J Eat Disord.1997;21:329 –334
27. Soyka L, Grinspoon S, Levitsky L, Herzog D, Klibanski A. The effects of anorexia nervosa on bone metabolism in female adolescents.J Clin Endocrinol Metab.1999;84:4489 – 4496
28. Misra M, Miller K, Bjorson J, et al. Alterations in growth hormone secretory dynamics in adolescent girls with anorexia nervosa and effects on bone metabolism.J Clin Endocrinol Metab.2003;88:5615–5623 29. Ogden C, Kuczmarski R, Flegal K, et al. Centers for Diseases Control
and Prevention 2000 growth charts for the United States: improvements to the 1997 National Center for health Statistics version.Pediatrics.
2002;109:45– 60
30. Greulich W, Pyle S.Radiographic Atlas of Skeletal Development of the Hand and Wrist. 2nd ed. Stanford, CA: Stanford University Press; 1959 31. 1992 Case Records of the Massachusetts General Hospital. Weekly
clinicopathological exercises. Normal reference laboratory values.
N Engl J Med.1992;327:718 –724
32. Katzman D, Bachrach L, Carter D, Marcus R. Clinical and anthropo-metric correlates of bone mineral acquisition in healthy adolescent girls.
J Clin Endocrinol Metab.1991;73:1332–1339
33. Ellis K, Shypailo R, Pratt J, Pond W. Accuracy of dual-energy x-ray absorptiometry for body-composition measurements in children.Am J Clin Nutr.1994;60:660 – 665
34. Kelly T, Berger N, Richardson T. DXA body composition: theory and practice.Appl Radiat Isot.1998;49:511–513
35. Kohrt W. Body composition by DXA: tried and true?Med Sci Sports Exerc.1995;27:1349 –1353
36. Visser M, Fuerst T, Lang T, Salamone L, Harris T. Validity of fan-beam dual-energy X-ray absorptiometry for measuring fat-free mass and leg muscle mass. Health, Aging, and Body Composition Study—Dual-Energy X-ray Absorptiometry and Body Composition Working Group.
J Appl Physiol.1999;87:1513–1520
37. Schoeller D. Bioelectrical impedance analysis.What does it measure? Ann N Y Acad Sci.2000;904:159 –162
38. Herman-Giddens M, Slora E, Wasserman R, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network.Pediatrics.1997; 99:505–512
40. Misra M, Soyka LA, Miller KK, Grinspoon S, Levitsky LL, Klibanski A. Regional body composition in adolescents with anorexia nervosa and changes with weight recovery.Am J Clin Nutr.2003;77:1361–1367 41. de Simone G, Scalfi L, Galderisi M, et al. Cardiac abnormalities in young
women with anorexia nervosa.Br Heart J.1994;71:287–292
42. Kollai M, Bonyhay I, Jokkel G, Szonyi L. Cardiac vagal hyperactivity in adolescent anorexia nervosa.Eur Heart J.1994;15:1113–1118
43. Nudel D, Gootman N, Nussbaum M, Shenker I. Altered exercise per-formance and abnormal sympathetic responses to exercise in patients with anorexia nervosa.J Pediatr.1984;105:34 –37
44. Rowland T, Koenigs L, Miller N. Myocardial performance during max-imal exercise in adolescents with anorexia nervosa.J Sports Med Phys Fitness.2003;43:202–208
45. Isner J, Roberts W, Heymsfield S, Yager J. Anorexia nervosa and sudden death.Ann Intern Med.1985;102:49 –52
46. Amrein P, Friedman R, Kosinski K, Ellman L. Hematologic changes in anorexia nervosa.JAMA.1979;241:2190 –2191
47. Mant M, Faragher B. The haematology of anorexia nervosa.Br J Haema-tol.1972;23:737–749
48. Bowers T, Eckert E. Leukopenia in anorexia nervosa. Lack of increased risk of infection.Arch Intern Med.1978;138:1520 –1523
49. Alvin P, Zogheib J, Rey C, Losay J. Severe complications and mortality in mental eating disorders in adolescence. On 99 hospitalized patients.
Arch Fr Pediatr.1993;50:755–762
50. Biebl W, Kinzl J. Hypokalemia in eating disorders.Am J Psychiatry.
1996;153:295–296
51. Greenfeld D, Mickley D, Quinlan D, Roloff P. Hypokalemia in outpa-tients with eating disorders.Am J Psychiatry.1995;152:60 – 63 52. Powers P, Tyson I, Stevens B, Heal A. Total body potassium and serum
potassium among eating disorder patients.Int J Eat Disord.1995;18: 269 –276
53. Jagielska G, Wolanczyk T, Komender J, Tomaszewicz-Libudzic C, Przedlacki J, Ostrowski K. Bone mineral density in adolescent girls with
anorexia nervosa—a cross-sectional study.Eur Child Adolesc Psychiatry.
2002;11:57– 62
54. Turner J, Bulsara M, McDermott B, Byrne G, Prince R, Forbes D. Predictors of low bone density in young adolescent females with an-orexia nervosa and other dieting disorders.Int J Eat Disord.2001;30: 245–251
55. Bachrach L. Acquisition of optimal bone mass in childhood and ado-lescence.Trends Endocrinol Metab.2001;12:22–28
56. Schwabe A, Lippe B, Chang R, Pops M, Yager J. Anorexia nervosa.Ann Intern Med1981;94:371–381
57. Hurd Hn, Palumbo P, Gharib H. Hypothalamic-endocrine dysfunction in anorexia nervosa.Mayo Clin Proc.1977;52:711–716
58. Golden N, Jacobson M, Schebendach J, Solanto M, Hertz S, Shenker I. Resumption of menses in anorexia nervosa.Arch Pediatr Adolesc Med.
1997;151:16 –21
59. Klibanski A, Biller B, Schoenfeld D, Herzog D, Saxe V. The effects of estrogen administration on trabecular bone loss in young women with anorexia nervosa.J Clin Endocrinol Metab.1995;80:898 –904
60. Golden N, Lanzkowsky L, Schebendach J, Palestro C, Jacobson M, Shenker I. The effect of estrogen-progestin treatment on bone mineral density in anorexia nervosa.J Pediatr Adolesc Gynecol.2002;15:135–143 61. Gwirtsman H, Kaye W, George D, Jimerson D, Ebert M, Gold P. Central
and peripheral ACTH and cortisol levels in anorexia nervosa and bu-limia.Arch Gen Psychiatry.1989;46:61– 69
62. Gold P, Gwirtsman H, Avgerinos P, et al. Abnormal hypothalamic-pituitary-adrenal function in anorexia nervosa. Pathophysiologic mech-anisms in underweight and weight-corrected patients.N Engl J Med.
1986;314:1335–1342
63. Licinio J, Wong M, Gold P. The hypothalamic-pituitary-adrenal axis in anorexia nervosa.Psychiatry Res.1996;62:75– 83
64. Estour B, Pugeat M, Lang F, et al. Rapid escape of cortisol from sup-pression in response to i.v.dexamethasone in anorexia nervosa. Clin Endo-crinol (Oxf).1990;33:45–52
BEAT GOES ON: CARP HEART KEEPS PACE WHEN FISH LACKS OXYGEN
“Without oxygen, a mere human dies in minutes, but a Scandinavian fish not only can survive but also maintains a normal heartbeat for days, say researchers. The Crucian carp (Carassius carassius) has long been recognized as a champion survivor, thriving even in shallow ponds that freeze over during long northern winters. These waters can turn into dead zones as creatures exhaust the oxygen in the water. What researchers haven’t known, though, is what strategy the carp follows for such a feat, says Jonathan A. W. Stecyk of Simon Fraser University in Burnaby, British Columbia. Turtles, the other vertebrates famed for toughing out times with no oxygen, reduce their heart functions to only about 10% of normal. The new study of the Crucian carp, however, shows that its heart rate dips when oxygen drops but rises again to essentially normal rates, Stecyk and his colleagues report in the October 1Science. ‘This is the 1st time we’ve seen in vertebrates that the heart will perform like this,’ he says. ‘I hope it will spur medical research into protecting human hearts during transplant or malfunction.’”
Milius S.Science News. October 2, 2004
DOI: 10.1542/peds.2004-0540
2004;114;1574
Pediatrics
Worley, Leslie A. Soyka, David B. Herzog and Anne Klibanski
Madhusmita Misra, Avichal Aggarwal, Karen K. Miller, Cecilia Almazan, Megan
Density Parameters in Community-Dwelling Adolescent Girls
Effects of Anorexia Nervosa on Clinical, Hematologic, Biochemical, and Bone
Services
Updated Information &
http://pediatrics.aappublications.org/content/114/6/1574
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/114/6/1574#BIBL
This article cites 63 articles, 8 of which you can access for free at:
Subspecialty Collections
skeletal_disorders_sub
http://www.aappublications.org/cgi/collection/rheumatology:musculo Rheumatology/Musculoskeletal Disorders
http://www.aappublications.org/cgi/collection/eating_disorders_sub Eating Disorders
icine_sub
http://www.aappublications.org/cgi/collection/adolescent_health:med Adolescent Health/Medicine
sub
http://www.aappublications.org/cgi/collection/hematology:oncology_ Hematology/Oncology
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.2004-0540
2004;114;1574
Pediatrics
Worley, Leslie A. Soyka, David B. Herzog and Anne Klibanski
Madhusmita Misra, Avichal Aggarwal, Karen K. Miller, Cecilia Almazan, Megan
Density Parameters in Community-Dwelling Adolescent Girls
Effects of Anorexia Nervosa on Clinical, Hematologic, Biochemical, and Bone
http://pediatrics.aappublications.org/content/114/6/1574
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.