Effect of Position on Sleep, Heart Rate Variability, and QT Interval in
Preterm Infants at 1 and 3 Months’ Corrected Age
Ronald L. Ariagno, MD*; Majid Mirmiran, MD*§; Marian M. Adams, MD*; Anna G. Saporito, MS*; Anne M. Dubin, MD‡; and Roger B. Baldwin, MA*
ABSTRACT. Objective. Prone sleeping position has a strong link to sudden infant death syndrome (SIDS), and the “Back to Sleep” campaign has played an important role in reducing SIDS. We tested the hypothesis that the mechanism of the sleep position effect is based on changes in sleep, arousal, heart rate variability (HRV), and the QT interval of the electrocardiogram.
Study Design. We studied 16 premature infants lon-gitudinally, at 1 and 3 months’ corrected age. Video-somnography recordings were made during the infants’ normal daytime naps. Each infant was recorded in both supine and prone positions. The recordings were ana-lyzed in 30-second epochs, which were classified as awake, active sleep (AS), quiet sleep (QS), or indetermi-nate sleep. Electrocardiogram data were sampled with an accuracy of 1 millisecond. Time domain analysis of HRV was measured by standard deviation of all R-R intervals and by the square root of the mean of the sum of the squares of the differences between adjacent R-R inter-vals. Frequency domain analysis was done for low fre-quency (0.04 – 0.14 Hz) and high frefre-quency (0.15– 0.5 Hz) HRV. We measured QT, JT, and R-R intervals during AS and QS for each position.
Results. We found no significant differences be-tween supine and prone position, either in total sleep time or in percentage of QS. Percentage of AS was sig-nificantly lower in the supine position, but only at 1 month corrected age. The incidence of short, spontane-ous, sleep transitions was significantly higher in supine, also only at 1 month corrected age. Time domain analysis of HRV showed a significantly lower variability in prone, but only during QS. Frequency domain analysis of HRV showed no differences between the 2 sleeping positions. Both QT and JT intervals were significantly longer in prone during QS, but only at 1 month corrected age.
Conclusions. Despite the commonly held belief, prone position did not substantially increase total sleep at these ages. On the other hand, prone sleeping de-creased the number of sleep transitions at 1 month cor-rected age, increased QT and JT intervals, and reduced HRV, thereby potentially increasing the vulnerability for SIDS. This study supports “Back to Sleep” as the posi-tion of choice not only for term but also for preterm infants after discharge home.Pediatrics 2003;111:622– 625;
sleep, QT interval, prone, supine, heart rate variability.
ABBREVIATIONS. SIDS, sudden infant death syndrome; QTc,
corrected QT interval; HRV, heart rate variability; PCA, postcon-ceptual age; W, awake; AS, active sleep; QS, quiet sleep; IS, inde-terminate sleep; ECG, electrocardiogram; SDNN, standard devia-tion of all R-R intervals; RMSSD, mean of the sum of the squares of differences between adjacent R-R; LF, low frequency; HF, high frequency, SD, standard deviation.
S
udden infant death syndrome (SIDS) has been independently associated with both prone sleeping position and prolonged QT interval.1,2 Since the “Back to Sleep” campaign, the frequency of prone sleeping position in the United States has de-creased from ⬎70% to only 24%.3The rate of SIDS has concomitantly decreased by 38%. Despite this, a substantial number of infants continue to be placed in the prone sleeping position. The majority of care-givers, at home or in day care centers, who placed the infants in the prone sleeping position believe that the “infants sleep better that way.”4There is substantial scientific evidence that the prone sleeping position increases the risk of SIDS, but the mechanism by which positioning and/or sleep states increase this risk has not been elucidated. A prolonged, corrected QT interval (QTc) has been hypothesized as a marker of cardiac electrical insta-bility, therefore increasing the likelihood of a lethal ventricular arrhythmia.2Schwartz et al2have shown significantly longer QTcin SIDS victims. They spec-ulated that prolongation of the QTcinterval may be attributable to developmental alterations in cardiac sympathetic innervation. An alternative possibility is that a prolonged QTcis a marker of a genetic abnor-mality, which predisposes the patient to lethal ar-rhythmias particularly when placed prone.5
Alterna-tively, we hypothesize a lower number of
spontaneous arousals, lower heart rate variability (HRV), and a prolonged QTcduring prone sleep may increase the likelihood for cardiorespiratory failure. In support of this hypothesis, a number of studies showed depressed arousal responses and HRV to external stimuli in prone versus supine in term in-fants.6 – 8
Preterm infants are at much higher risk of SIDS than term infants.9 –11The association between prone sleeping and SIDS seems to be even stronger among low birth weight infants.12 Earlier, we had studied preterm infants at discharge, around 36 weeks’ postconceptual age (PCA). We found fewer arousals and reduced HRV in prone position.13In the current study, we extended the time period of the study to
From the Departments of *Pediatrics and ‡Pediatric Cardiology, Stanford University School of Medicine, Stanford, California; and §Netherlands In-stitute for Brain Research, Amsterdam, the Netherlands.
Received for publication Feb 12, 2002; accepted Jul 1, 2002.
Address correspondence to Ronald L. Ariagno, MD, Department of Pedi-atrics, Stanford University School of Medicine, 750 Welch Rd, Ste 315, Palo Alto, CA 94304. E-mail: [email protected]
examine the effects of prone sleeping position at a later developmental period, ie, at 1 and 3 months’ corrected age. To better understand the mecha-nism(s) of SIDS, we have tested the hypothesis that sleep position may influence sleep transitions, HRV, and QTc in formerly premature infants at 1 and 3 months’ corrected age.
MATERIALS AND METHODS
Sixteen asymptomatic preterm infants (6 girls and 10 boys) with a mean gestational age of 34.4⫾2.2 weeks (range: 28 –36 weeks) and mean birth weight of 2326⫾493 g (range: 1172–3000 g) were studied longitudinally at 1 and 3 months’ corrected age at home. These infants did not have any medical problems and were not on medications at the time of the study. Each infant was recorded at their usual nap time, between 11 am and 4 pm. Sensors were placed on the infant before feeding and the recording was then started right after the completion of feeding. The initial sleeping position was randomized. After 1 to 1.5 hours of recording, the infant was gently, without awakening, placed in the complemen-tary position.
The protocol was approved by the Human Subjects Institu-tional Review Board at Stanford University. Informed parental consent was obtained before the study.
Polysomnographic recordings were performed with an ambu-latory digital recorder (Embla; Flaga hf. Medical Devices, Reykja-vik, Iceland, 4.5⫻8.3⫻13.3 cm). The following variables were recorded simultaneously: 2 channels electroencephalogram (C4/A1 and C3/A2), an electrocardiogram (lead II); air flow (BreathSensor; Model 976; Nellcor Puritan Bennett Inc, Minneap-olis, MN); thoracic respiratory effort (Crystal Trace Piezo Respi-ratory Effort Belt; Pro-Tech Services Inc, Woodinville, WA); and transcutaneous oxygen saturation and pulse rate (Pulse Oximeter Sensor, Models 8001J & 8008J; Nonin Medical Inc, Minneapolis, MN). All data were stored on hard disk and later analyzed using Somnologica software (Flaga hf. Medical Devices, Reykjavik, Ice-land). Synchronized time-lapse video recordings (Panasonic, model AG6730, Osaka, Japan) were made simultaneously with the digital recordings. The camera framed the infant’s face and upper body for interpretation of sleep behavior (see Goto et al13 for
further details).
Sleep State Analysis
Each 30-second epoch of the recording was analyzed and clas-sified as Awake (W), Active Sleep (AS), Quiet Sleep (QS), or Indeterminate Sleep (IS) according to criteria in the literature.14
Percentages of each sleep state were calculated relative to the total sleep time in each position for each age. The number of transitions from one state to another was determined for each position. The number of transitions method was chosen rather than spontane-ous arspontane-ousals since, at this time, there is no consensus or univer-sally accepted criteria for defining spontaneous arousal.
Electrocardiogram (ECG) Analysis
ECG data were sampled at an effective accuracy of 1 millisec-ond. Artifacts on ECG traces were identified by visual inspection and periods with artifact were excluded from additional analysis. Somnologica software for HRV analysis was used to examine the data.15Time domain analyses included standard deviation of all
R-R intervals (SDNN) and the square root of the mean of the sum of the squares of differences between adjacent R-R (RMSSD). Frequency domain analyses were done for low frequency (LF; 0.04 – 0.14 Hz) and high frequency (HF; 0.15– 0.5 Hz) HRV. These measurements were based on standard criteria.16All artifact-free
episodes lasting at least 2 minutes during each sleep state, AS and QS, in each position were used for analysis.
An experienced pediatric cardiologist (A.M.D.) randomly se-lected 10 R-R intervals for each position and sleep state and manually measured QT, R-R, and JT intervals during AS and QS for each position.17 The JT interval, from the end of the QRS
complex to the end of the T wave, was measured to account for any interventricular conduction delay.17These measures, QT and
JT, were corrected for heart rate using Bazett’s formula, yielding QTcand JTc. Average QTcs and JTcs for each position and each
sleep state were then obtained. Any periods of apnea ⱖ10 s,
oxygen desaturation⬍90%, or bradycardia⬍80 beats per minute were also recorded.
Statistical Analysis
All values are expressed as mean⫾1 standard deviation (SD). Statistical analyses were done with pairedttests. Significance was accepted atPⱕ.05.
RESULTS
The sleep characteristics of both positions are sum-marized with means and SDs in Table 1. We found no significant differences in total sleeping time and %QS between the supine and prone positions (Table 1). The %AS was significantly lower in supine, but only at 1 month corrected age. The incidence of sleep transitions and %IS were significantly higher in su-pine, but only at 1 month corrected age.
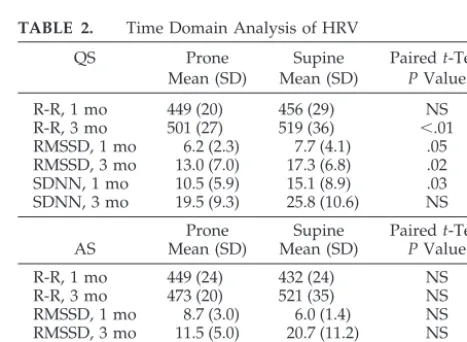
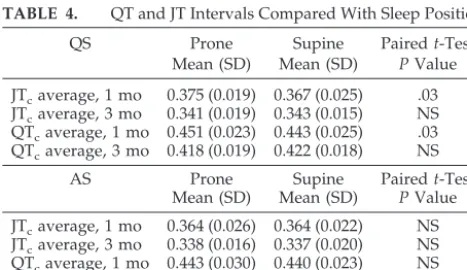
Time domain analysis of the HRV showed signif-icant differences in the sleeping position during QS, but not in AS (Table 2). The RMSSD was significantly greater in the supine position at both 1 and 3 months’ corrected age, whereas the SDNN was significantly higher in the supine position, but only at 1 month corrected age. Frequency domain analysis of HRV, on the other hand, showed no differences between the 2 sleeping positions either in LF or HF except for higher HF during QS in supine at 1 month corrected age (Table 3). QTc and JTc were significantly longer in prone but only at 1 month corrected age (Table 4). No apnea, desaturation, or bradycardia episodes were found in any infant in either sleeping position. TABLE 1. Comparison of Sleep Characteristics Between Prone and Supine Sleep Positions
Variable Prone Supine Pairedt-Test Mean (SD) Mean (SD) PValue
%AS, 1 mo 52.8 (10.9) 27.1 (24.6) ⬍.01 %AS, 3 mo 39.9 (21.7) 35.9 (14.0) NS %QS, 1 mo 42.09 (9.3) 53.4 (23.9) NS %QS, 3 mo 47.8 (26.6) 56.2 (13.6) NS %IS, 1 mo 3.1 (2.6) 6.3 (4.6) ⬍.01
%IS, 3 mo 9 (18.6) 3.6 (3.4) NS
No. transitions, 1 mo 5.9 (4.0) 12.2 (10.1) .05 No. transitions, 3 mo 6.2 (3.8) 5.2 (1.8) NS Total sleep time, 1 mo 89 (24) 70 (42) NS Total sleep time, 3 mo 70 (24) 61 (20) NS
NS indicates not significant.
TABLE 2. Time Domain Analysis of HRV
QS Prone Supine Pairedt-Test
Mean (SD) Mean (SD) PValue
R-R, 1 mo 449 (20) 456 (29) NS
R-R, 3 mo 501 (27) 519 (36) ⬍.01
RMSSD, 1 mo 6.2 (2.3) 7.7 (4.1) .05 RMSSD, 3 mo 13.0 (7.0) 17.3 (6.8) .02 SDNN, 1 mo 10.5 (5.9) 15.1 (8.9) .03 SDNN, 3 mo 19.5 (9.3) 25.8 (10.6) NS
Prone Supine Pairedt-Test
AS Mean (SD) Mean (SD) PValue
R-R, 1 mo 449 (24) 432 (24) NS
R-R, 3 mo 473 (20) 521 (35) NS
RMSSD, 1 mo 8.7 (3.0) 6.0 (1.4) NS RMSSD, 3 mo 11.5 (5.0) 20.7 (11.2) NS SDNN, 1 mo 21 (7.1) 16.7 (4.6) NS SDNN, 3 mo 24.7 (10.3) 32.8 (13.1) NS
NS indicates not significant.
ARTICLES 623
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news
DISCUSSION
At 1 month corrected age, we found a small but significant reduction in %AS in the supine sleeping position; however, this was accompanied by an in-creased %IS and no change in %QS or total sleep time. At 3 months’ corrected age, on the other hand, no significant differences were found between prone and supine sleeping positions. Although prone posi-tion may indeed increase duraposi-tion of QS right after feeding in preterm infants before discharge, there is no significant difference in overall sleep pattern at later age.18,19 These results contradict the common belief that a preterm or term infant may sleep better/ longer when in the prone sleeping position.4,20Our earlier study of preterm infants before discharge also failed to show any significant effect of position on amount of sleep.18The strength of our study is that each infant served as its own control. Differences between prone and supine in this study could not be attributed to the typical large individual sleep differ-ences in infants. On the other hand, to record the infant in both positions on a single afternoon, we were not able to record each infant for longer than 1 to 1.5 hours in each position. A longer overnight home study was impractical, less acceptable to par-ents, and we wanted to avoid laboratory influences
on sleep pattern of the infant.20 Although daytime naps may not be representative of nighttime sleep, we could not find evidence for substantial changes in amount of sleep based on position. We believe that although SIDS is associated with sleep, the amount of AS or QS per se may not be the determining factor in the occurrence of SIDS.
Prone position, by virtue of centrally increasing arousal threshold and upper airway resistance, may well serve as a potential independent risk factor in SIDS.21The decreased number of sleep transitions at 1 month corrected age in our study supports this hypothesis. Because the tendency of infants to sleep during the day decreases by 3 months’ corrected age (because of the development of circadian rhythms22), this may have influenced the number of sleep tran-sitions at this age. Investigators recording spontane-ous and evoked arspontane-ousals have shown the influence of sleep state and sleep position in term and preterm infants6,7,23–28). Galland et al25 showed lower HRV in prone versus supine in term infants at 1 and 3 months of age. Franco et al27 showed significantly more intense stimuli were required to induce arousal during REM sleep in prone versus supine. Arousal threshold in response to air-jet stimulation was sig-nificantly higher in prone versus supine both in ac-tive and in quiet sleep.23 Skadberg and Markestad26 found significantly less short arousals in prone ver-sus supine during REM sleep but not during QS.
Time domain analysis of HRV, particularly RMSSD, which is a measure of variability in succes-sive intervals, showed significant reduction of HRV in prone sleeping position both at 1 and 3 months’ corrected age. Both RMSSD and SDNN values dur-ing QS in prone were consistently lower than supine (Table 3). No significant differences in frequency do-main analysis of HRV were found. The reduction in HRV, particularly RMSSD, which is a measure of the degree of parasympathetic influences on heart rate over time, is interesting and is consistent with our earlier studies in preterm infants before discharge.13 Similar results have been reported by other investi-gators in term infants at 1 to 3 months’ corrected age and in preterm infants in the nursery.19,25Reduction in HRV after cardiac arrest has been considered a potential risk factor for cardiac arrhythmia in adult patients. For the preterm infant, we speculate that a decrease in sleep transitions in combination with reduced autonomic function variability at a critical age could increase the risk for SIDS.29,30
Although the JTcand QTcintervals were within a normal clinical range, statistically significant in-creases were found during QS at 1 month corrected age. JTc and QTc were both shorter at 3 months’ corrected age compared with 1 month. Prolongation of the QTcinterval has been associated with imbal-ances of sympathetic and parasympathetic tone; these imbalances may permit lethal ventricular ar-rhythmias to develop in those patients who are at risk of long QT syndrome.2On the other hand, the QT may not adequately reflect the autonomic state in this patient population. QT prolongation may be ev-ident only if the cellular substrate for prolonged QT syndrome is present. In the light of the provocative TABLE 3. Frequency Domain Analysis of HRV
QS Prone Supine Pairedt-Test
Mean (SD) Mean (SD) PValue
HF, 1 mo 5.6 (6.0) 9.5 (14.9) .02
HF, 3 mo 35 (37) 49 (44) NS
LF, 1 mo 51 (70) 131 (194) NS
LF, 3 mo 147 (183) 269 (295) NS
LF/HF, 1 mo 9.8 (9.6) 21.4 (28.3) NS LF/HF, 3 mo 6.3 (5.6) 7.8 (9.2) NS HF/LF, 1 mo 0.23 (0.22) 0.14 (0.15) NS HF/LF, 3 mo 0.34 (0.34) 0.34 (0.40) NS
AS Prone Supine Pairedt-Test
Mean (SD) Mean (SD) PValue
HF, 1 mo 16.9 (14.8) 6.2 (4.4) NS
HF, 3 mo 30 (31) 72 (87) NS
LF, 1 mo 221 (168) 116 (70) NS
LF, 3 mo 274 (237) 388 (401) NS
LF/HF, 1 mo 17.1 (12.9) 25.4 (18.2) NS LF/HF, 3 mo 12.67 (13.1) 8.3 (7.2) NS HF/LF, 1 mo 0.10 (0.07) 0.06 (0.04) NS HF/LF, 3 mo 0.13 (0.09) 0.23 (0.22) NS
NS indicates not significant.
TABLE 4. QT and JT Intervals Compared With Sleep Position
QS Prone Supine Pairedt-Test
Mean (SD) Mean (SD) PValue
JTcaverage, 1 mo 0.375 (0.019) 0.367 (0.025) .03
JTcaverage, 3 mo 0.341 (0.019) 0.343 (0.015) NS
QTcaverage, 1 mo 0.451 (0.023) 0.443 (0.025) .03
QTcaverage, 3 mo 0.418 (0.019) 0.422 (0.018) NS
AS Prone Supine Pairedt-Test
Mean (SD) Mean (SD) PValue
JTcaverage, 1 mo 0.364 (0.026) 0.364 (0.022) NS
JTcaverage, 3 mo 0.338 (0.016) 0.337 (0.020) NS
QTcaverage, 1 mo 0.443 (0.030) 0.440 (0.023) NS
QTcaverage, 3 mo 0.417 (0.021) 0.416 (0.021) NS
results reported by Schwartz,2we may expect even further increase of QT interval during QS in prone sleeping position in patients with long QT syndrome. Although both sleeping position and QT intervals are risk factors for sudden infant death syndrome, they do not appear to be related. Additional study of the relationship between sleeping position and the autonomic nervous system is warranted.
Beneficial influences of prone sleeping position have been found in critically ill preterm infants in the neonatal intensive care unit.31 We have found no clinically significant apnea, oxygen desaturation, or bradycardia in asymptomatic preterm infants before discharge from the hospital13 or at 1 and 3 months’ corrected age at home. A recent study of 22 symp-tomatic preterm infants with gestational age ranging from 24 to 30 weeks, recorded at 28 to 36 weeks’ PCA in the neonatal intensive care unit failed to show any beneficial influence of prone position on apnea, bra-dycardia, or desaturation.32Keene et al’s data as well as ours are in support of the statement of the Task Force of the American Academy of Pediatrics on SIDS1 for preterm infants. The American Society of Gastroenterology recently indicated that prone posi-tioning as a therapy for reflux in infants is no longer generally recommended because of the concern for an increase risk for SIDS.33There is simply no good reason to place a healthy infant in the prone sleeping position despite the myths of improved sleep, re-duced choking, and increased cardiorespiratory sta-bility.34
ACKNOWLEDGMENT
This study was supported by a Lucile Packard Children’s Hos-pital, Children’s Health Initiative grant.
REFERENCES
1. American Academy of Pediatrics, Task Force on Infant Sleep Position and Sudden Infant Death Syndrome. Changing concepts of sudden infant death syndrome: implications for infant sleeping environment and sleep position.Pediatrics. 2000;105:650 – 656
2. Schwartz PJ, Stramba-Badiale M, Segantini A, et al. Prolongation of the QT interval and the sudden infant death syndrome.N Engl J Med. 1998;338:1709 –1714
3. Willinger M, Hoffman HJ, Wu KT, et al. Factors associated with the transition to non-prone sleep position of infants in the United States.
JAMA. 1998;280:329 –335
4. Willinger M, Ko CW, Hoffman HJ, Kessler RC, Corwin MJ. Factors associated with caregivers’ choice of infant sleep position, 1994 –1998: the National Infant Sleep Position Study.JAMA.2000;283:2135–1242 5. Schwartz PJ, Priori SG, Dumaine R, et al. A molecular link between the
sudden infant death syndrome and the long-QT syndrome. N Engl J Med.2000;343:262–267
6. Galland BC, Hayman RM, Taylor BJ, Bolton DP, Sayers RM, Williams SM. Factors affecting heart rate variability and heart rate responses to tilting in infants aged 1 and 3 months.Pediatr Res.2000;48:60 – 68 7. Franco P, Groswasser J, Sottiaux M, Broadfield E, Kahn A. Decreased
cardiac responses to auditory stimulation during prone sleep.Pediatrics.
1996;97:174 –178
8. Franco P, Pardou A, Hassid S, Lurquin P, Grosswasser J, Kahn A. Auditory arousal thresholds are higher when infants sleep in the prone position.J Pediatr.1998;132:240 –243
9. Grether JK, Schulman J. Sudden infant death syndrome and birth weight.J Pediatr.1989;114:561–567
10. Malloy MH, Hoffman HJ. Prematurity, sudden infant death syndrome, and age of death.Pediatrics.1995;96:464 – 471
11. Malloy MH, Freeman DH Jr. Birth weight- and gestational age-specific sudden infant death syndrome mortality: United States, 1991 versus 1995.Pediatrics.2000;105;1227–1231
12. Oyen N, Markestad T, Skaerven R, et al. Combined effects of sleeping position and prenatal risk factors in sudden infant death syndrome: the Nordic Epidemiological SIDS Study.Pediatrics.1997;100:613– 621 13. Goto K, Mirmiran M, Adams MM, et al. More awakenings and heart
rate variability during supine sleep in preterm infants.Pediatrics.1999; 103:603– 609
14. Anders T, Emde R, Parmelee A.A Manual of Standardized Terminology, Technique and Criteria for Scoring States of Sleep and Wakefullness in New-born Infants. Los Angles, CA: UCLA Brain Information Service BRI Publications Office, NINDS Neurological Information Network; 1971 15. Bronzino J.The Biomedical Engineering Handbook. ISBN 0 – 8493-8346 –3.
Boca Raton, FL: CRC Press in cooperation with IEEE Press; 1995 16. Task Force Of The European Society of Cardiology and the North
American Society of Pacing and Electrophysiology. Heart rate variability: standards of measurement, physiological interpretation and clinical use.Circulation.1996;93:1043–1065
17. Dubin A, Kikkert M, Mirmiran M, Ariagno R. Cisapride associated with QTc prolongation in very low birth weight preterm infants.Pediatrics.
2001;107;1313–1316
18. Goto K, Mirmiran M, Adams MM, Longford RV, et al. More awaken-ings and heart rate variability during supine sleep in preterm infants.
Pediatrics.1999;103:603– 609
19. Sahni R, Schulze KF, Kashyap S, OhiraKist K, Myers MM, Fifer WP. Body position; sleep states; and cardiorespiratory activity in developing low birth weight infants.Early Hum Dev.1999;54:197–206
20. Kahn A, Groswasser J, Sottiaux M, Rebuffat E, Franco P, Dramaix M. Prone or supine body position and sleep characteristics in infants.
Pediatrics.1993;91:1112–1115
21. Davidson Ward S, Keens T. Maturation of the arousal response. In: Loughlin GM, Carroll J, Marcu C, eds.Sleep and Breathing in Children: A Developmental Approach. New York, NY: Marcel Dekker, Inc; 2000:79 –97 22. Mirmiran M, Ariagno RL. Influence of light in the NICU on the devel-opment of circadian rhythms in preterm infants.Semin Perinatol.2000; 24:247–257
23. Horne RS, Ferens D, Watts AM, et al. The prone sleeping position impairs arousability in term infants.J Pediatr.2001;138:811– 816 24. Horne RS, Sly DJ, Cranage SM, Chau B, Adamson TM. Effects of
prematurity on arousal from sleep in the newborn infant.Pediatr Res.
2000;47:468 – 474
25. Galland BC, Reeves G, Taylor BJ, Bolton DP. Sleep position, autonomic function, and arousal. Arch Dis Child Fetal Neonatal Ed. 1998;78: F189 –F194
26. Skadberg BT, Markestad T. Behaviour and physiological responses during prone and supine sleep in early infancy.Arch Dis Child.1997; 76:320 –324
27. Franco P, Pardou A, Hassid S, Lurquin P, Groswasser J, Kahn A. Auditory arousal thresholds are higher when infants sleep in the prone position.J Pediatr.1998;132:240 –243
28. Read PA, Horne RS, Cranage SM, Walker AM, Walker DW, Adamson TM. Dynamic changes in arousal threshold during sleep in the human infant.Pediatr Res.1998;43:697–703
29. Filiano JJ, Kinney HC. A perspective on neuropathologic findings in victims of the sudden infant death syndrome: the triple-risk model.Biol Neonate. 1994;65:194 –197
30. Ariagno R, Mirmiran M. Arousal and brain homeostatic control. In: Byard R, Krous H, eds.Sudden Infant Death Syndrome: Problems, Progress, & Possibilities. London, United Kingdom: Arnold; 2001:96 –117 31. Martin RJ, Okken A. Arterial oxygen tension during active and quiet
sleep in the normal neonate.Pediatrics.1979;94:271–274
32. Keene DJ, Wimmer JE Jr, Mathew OP. Does supine positioning increase apnea, bradycardia, and desaturation in preterm infants?J Perinatol.
2000;20:17–20
33. Rudolph CD, Mazur LJ, Liptak GS, et al. Evaluation and treatment of gastroesophageal reflux in infants and children: an evidence-based review for a clinical guideline—pediatric GE reflux clinical practice guidelines.J Pediatr Gastroenterol Nutr.2001;32(suppl 2):S1–S31 34. Jeffery HE, Megevand A, Page H. Why the prone position is a risk factor
for sudden infant death syndrome.Pediatrics.1999;104:263–269
ARTICLES 625
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news
DOI: 10.1542/peds.111.3.622
2003;111;622
Pediatrics
Dubin and Roger B. Baldwin
Ronald L. Ariagno, Majid Mirmiran, Marian M. Adams, Anna G. Saporito, Anne M.
Infants at 1 and 3 Months' Corrected Age
Effect of Position on Sleep, Heart Rate Variability, and QT Interval in Preterm
Services
Updated Information &
http://pediatrics.aappublications.org/content/111/3/622
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/111/3/622#BIBL
This article cites 30 articles, 13 of which you can access for free at:
Subspecialty Collections
sub
http://www.aappublications.org/cgi/collection/fetus:newborn_infant_ Fetus/Newborn Infant
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.111.3.622
2003;111;622
Pediatrics
Dubin and Roger B. Baldwin
Ronald L. Ariagno, Majid Mirmiran, Marian M. Adams, Anna G. Saporito, Anne M.
Infants at 1 and 3 Months' Corrected Age
Effect of Position on Sleep, Heart Rate Variability, and QT Interval in Preterm
http://pediatrics.aappublications.org/content/111/3/622
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.
the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2003 has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
at Viet Nam:AAP Sponsored on August 30, 2020
www.aappublications.org/news