EXPERIENCE AND REASON—Briefly Recorded
‘‘In Medicine one must pay attention not to plausible theorizing but to experience and reason together. . . . I agree that theorizing is to be approved, provided that it is based on facts, and systematically makes its deductions from what is observed. . . . But conclusions drawn from unaided reason can hardly be serviceable; only those drawn from observed fact.’’ Hippocrates: Precepts. (Short communications of factual material are published here. Comments and criticisms appear as letters to the Editor.)
Femur Fracture in Infants: A
Possible Accidental Etiology
ABSTRACT. Femoral fractures in nonambulating in-fants are generally felt to be attributable to abuse in the absence of significant trauma or underlying organic pa-thology. The investigation of such fractures includes a report to appropriate social service and law enforcement agencies, and legal involvement. This paper describes 2 nonambulatory infants who sustained identical oblique distal femoral metaphyseal fractures extending through the growth plate after playing in an infant stationary activity center called an Exersaucer. It is possible that the twisting motion provided by the Exersaucer (Evenflo, Picqua, OH) might be consistent with the generation of forces necessary to cause these fractures.Pediatrics2001; 108:1009 –1012;femoral fractures, infants, child abuse.
ABBREVIATION. CML, classic metaphyseal lesion.
F
emoral fractures are reported in 12% to 29% of physically abused children.1 Femoral fracturesin nonambulating infants, particularly spiral fractures, are believed to be highly specific for in-flicted injury. This association has been replicated over time. In 1983, a retrospective chart review of all children⬍4 years of age seen at a university hospital for a femur fracture found that 30% were attributable to abuse.2The most common reason for suspicion of
abuse was lack of any history of injury. In that study, the radiographs did not distinguish between abused and nonabused children, as the most common site of fracture for both was the mid-diaphysis. The authors noted that abused children had a higher incidence of fractures of the proximal diaphysis and the distal metaphysis. Another study published the same year retrospectively analyzed femur fractures in children ⬍5 years of age. Among children⬍1 year of age, 70% of fractures were found to be attributable to abuse.3
In one study from 1991, 60% of fractures of the femur occurring in infants 1 year or younger were the result of abuse, whereas only 20% of fractures in children between the ages of 2 to 3 years were determined to be the result of abuse.4
In infancy, a pattern injury like a spiral fracture is often inflicted. A spiral or oblique pattern implies
application of a torsional force resulting from man-ual torsion with abuse, or twisting against a planted foot with a fall. As is the case with accidental injuries, most inflicted fractures of the femoral shaft involve the middle and distal third.5 Leventhal et al6
per-formed retrospective chart reviews of children ⬍3 years of age who were examined for a fracture. For femoral fractures, the child’s age was the best distin-guishing feature of etiology: in children⬍12 months, 60% were classified as abuse compared with 0% in children older than 23 months. History characteris-tics were found to be vague in the abuse cases where the second most commonly occurring event was when the caretaker noted a change in the child’s behavior, such as a nonmoving extremity: the major-ity (79%) in this group were classified as abuse. This type of history along with an abnormality in the child, such as swelling without report of any acci-dent, occurred in 52% of the abuse cases. In contrast to nonambulatory children, oblique midshaft femur fractures have been reported to occur as a result of accidental injury in ambulatory children.6
The following 2 case reports document the possi-bility of distal femur fractures in infancy in a manner other than child abuse. Two infants, both⬍9 months old, with oblique femur fractures, were referred to the Broward County Child Protection Team for pos-sible physical abuse. During the course of the inves-tigation, it was learned that both infants had report-edly played in a product called an Exersaucer (Evenflo, Picqua, OH) before their parents suspect-ing an injury to their legs. The Exersaucer is a sta-tionary activity center and is a successor to the infant walker. The Exersaucer’s seat swivels as the child uses his feet to push off on the saucer-shaped base. The seat can swivel in both directions and the base rocks. The height of the seat can be adjusted to 3 different levels (Fig 1). The child can plant his feet on the base such that a twisting motion is generated with the seat and the base moving in opposite direc-tions.
CASE REPORTS Case 1
C. S., a 7-month-old female, presented to her pediatrician’s office on September 5, 1996, with an approximately 48-hour his-tory of irritability and decreased range of motion of the right lower extremity. She normally had been able to stand, move, and kick with both lower extremities. The pediatrician noted swelling and discomfort in the right lower extremity, and the child was referred for an orthopedic consult. The child seemed comfortable when the right lower extremity was not moved. No bruises were noted on physical examination. Femur films revealed an acute oblique distal femur fracture involving the physeal plate. This was
Received for publication May 12, 2000; accepted Feb 1, 2001.
Address correspondence to Penny Grant, MD, Department of Pediatrics, University of Oklahoma: Tulsa, Child Abuse Network, 2829 South Sheridan Rd, Tulsa, OK 74129. E-mail: [email protected]
a Salter-Harris type II fracture with a large posterior metaphyseal fragment with an anterior extension into the physis (Fig 2). A bone survey was negative for any other fractures. On initial interview, the parents denied any history of trauma. They clearly noted a lack of movement of the right leg on the night of September 3. When asked about other possibilities, they recalled that the child had been using an Exersaucer. They brought it to the hospital and stated that they had not adjusted the height of the seat to lengthen it in conjunction with the child’s growth. They demonstrated that the child could thus plant her feet on the base of the product and twist. The child underwent closed reduction and application of a
spica cast. Femur films done through a fiberglass cast on 9/9 revealed an oblique fracture of the distal metaphysis of the femur with apparent extension into the physeal plate on the lateral view. There was minimal posterior displacement of the distal fragment of approximately 2 mm. Some early periosteal reaction is sug-gested (Fig 3). The mechanism of this injury was felt to possibly be consistent with the use of the Exersaucer as reported by the parents. No family concerns were identified during the Child Protection Team Family Assessment, which is a detailed psycho-social interview of the family members. Child Protective Services closed the case without any indicators of abuse.
Case 2
E. M., a 4.5-month-old female, was reportedly playing in her Exersaucer the day before her presentation to the emergency department of a community hospital with the chief complaint of not moving her leg for 1 day. The mother noted the child was not moving her left leg when she put her to bed, and the child cried when her left leg was touched. There was no history of injury given. No bruises were noted on the nursing admission assess-ment. Femur films done in the emergency department revealed a minimally displaced oblique fracture extending from the physis into the posterior metaphysis (Fig 4). A bone survey did not reveal any other fractures. The child underwent traction and placement of a long leg cast. Healing films (Fig 5) revealed a left oblique distal femur fracture with posteromedial callus formation. The mechanism of this injury was felt to possibly be consistent with the described use of the Exersaucer. Child Protective Services closed the case without evidence of abuse.
The 2 above incidents were reported to the Consumer Product Safety Commission. These reports are currently under investiga-tion.
DISCUSSION
A pediatric radiologist and pediatric orthopedist independently reviewed both children’s films. They concluded that these fractures are similar in geome-try and reflect a similar causative mechanism. Both show an oblique fracture line beginning at the an-terolateral aspect of the growth plate ending in the posteromedial aspect of the femoral metaphysis. A mechanism of injury to these children might be as follows: The child’s feet are planted on the base of the Exersaucer. As the child rotates, the force gener-ated is transmitted to the weakest part of the child’s leg, the anterolateral aspect of the knee or growth plate, where the fracture begins. The twisting motion from the child’s rotation causes the oblique fracture. As the child rotates outward in a partially or fully Fig 1. Exersaucer (Evenflo, Picqua, OH).
weight-bearing position with the foot of the involved extremity fixed in place and the knee fully extended or even slightly flexed, a varus force is created: the fracture begins proximal to the growth plate, travels laterally and proximally into the metaphysis behind the knee where the fracture ends, leaving the perios-teum separated from the bone. The fracture ends medially because of the rotational component. As the bone heals, new bone forms under the periosteum forming a callus posterior and medial to the knee. Healing films of both children confirm that this cal-lus is located at the posteromedial aspect of the knee. This type of fracture might also be sustained by a child swiveling in the seat in 1 direction then stop-ping suddenly by planting a foot and hyperextend-ing the knee. The momentum of the body against the planted, hyperextended, and fixed knee would gen-erate torsional forces into the femur or tibia. Depend-ing on the point of maximal stress concentration, a fracture may result. A likely point of stress concen-tration would be above the knee: the middle of a long lever arm fixed at the base of the toy by the foot and by the hip locked in the seat. In full or even hyper-extension, and with external rotation of the body over the fixed lower extremity, the forces generated by this sudden stop would be anterolateral directed posteromedial. The physeal plate would be the weak
link resulting in the initial fracture line starting an-terolateral in the physis extending obliquely proxi-mal into the metaphyseal bone resulting from the torsional load. A Salter-Harris II fracture would be the result just as these 2 cases demonstrate.
A child’s bone is inherently weakest at the physis or growth plate. Injuries predictably involve this area, so this type of fracture is quite typical in grow-ing bones, particularly when angulatory and rota-tional forces are applied.7Furthermore, metaphyseal
and cortical bone is more porous and not nearly so organized into lamellar structures in infants making failure in compression, particularly when combined with rotation, more likely.8 Lastly, because these
fractures involve the growth plate, growth arrest is a possibility.
This oblique fracture is in contrast to the classic metaphyseal lesion (CML) described by Paul Klein-man.9This lesion was described in 11 infants ages 1
to 5 months old who had died as a result of inflicted injuries that were examined both histologically and with detailed radiographic studies. In the same pa-per, the authors describe another radiographic pat-tern of the healing CML, a relatively discrete medial metaphyseal fragment corresponding to the corner fracture pattern.10Dr Kleinman described the classic
CML as always involving the posteromedial aspect of the femur, with anterior and lateral extension occurring in more diffuse lesions. The projection of Fig 4. Left femur, March 1, 1997.
the fracture fragment radiographically will result in either a “corner fracture” pattern or a “bucket han-dle” fracture. Only a small part of the metaphysis is visible by radiograph.
In both of our case reports, the fracture originates in the physis and extends obliquely into the metaph-ysis. The CML lesion, on the other hand, originates in the metaphysis, parallels the growth plate, and is entirely through the most distal portion of the me-taphysis. It does not extend into the physis. The different mechanisms of injury explain the difference in the pattern of these 2 types of fractures. Classi-cally, the CML lesion is thought to result from pri-marily a traction injury. In contrast, our 2 children sustained weight-bearing, torsional injuries. Each of these mechanisms creates the respective fracture anatomy.
Both parents report the use of the Exersaucer be-fore the onset of their children’s symptoms. The par-ents of E. M. spontaneously mentioned the toy when they brought the child to the emergency department. The parents of C. S. mentioned the toy when told by one of the authors (P. G.) that a possible twisting motion to the leg caused the fracture. The direction and type of both of these fractures fits the forces generated when a child is using the Exersaucer. One would not have expected the parents to directly link the toy to the injury as neither parent reported a distinct episode of sudden onset of crying while the child was using the toy.
A literature search was performed via the National Center for Biotechnology Information PubMed. No matches were found for the search words Exersaucer and femur fracture. We believe this is the first pub-lished possible association between this type of prod-uct and the described fractures.
CONCLUSION
These 2 identical femur fractures sustained by nonambulating infants serve as a reminder that a good history must always be obtained in cases of pediatric trauma. These fractures were initially be-lieved to possibly be the result of physical abuse. Additional questioning revealed a possible acciden-tal mechanism that could be consistent with the in-juries sustained by these children. Thus, although the majority of femur fractures in this age group are the result of abuse, these 2 cases demonstrate that there are exceptions. As these are just 2 incidents, a con-clusion as to the safety of this product cannot be drawn without additional investigation.
ACKNOWLEDGMENTS
We thank Dr Robert W. Block for his critical review of the manuscript.
We greatly appreciate the thoughtful comments of Dr Betty Spivack and Dr Randall Alexander.
Penny Grant, MD Department of Pediatrics University of Oklahoma Tulsa, OK 74129
Maria B. Mata, MD Department of Radiology Broward General Medical Center Fort Lauderdale, FL 33316
Michael Tidwell, MD Department of Orthopedics Miami Children’s Hospital Miami, FL 33155
REFERENCES
1. Reece RM.Child Abuse: Medical Diagnosis and Management. Malvern, PA: Lea & Febiger; 1994:32
2. Beals RK, Tufts E. Fractured femur in infancy: the role of child abuse.
J Pediatr Orthop. 1983;5:583–586
3. Gross RH, Stranger M. Causative factors responsible for femoral frac-ture.J Pediatr Orthop. 1983;3:341–343
4. Reece RM.Child Abuse: Medical Diagnosis and Management. Malvern, PA: Lea & Febiger; 1994:36
5. Kleinman P.The Diagnostic Imaging of Child Abuse. 2nd ed. St Louis, MO: Mosby; 1998:34
6. Leventhal JM, Thomas SA, Rosenfield NS, Markowitz RI. Fractures in young children: distinguishing child abuse from unintentional injuries.
Am J Dis Child. 1993;147:87–92
7. Rang M.Children’s Fractures.2nd ed. Philadelphia, PA: JB Lippincott Company; 1983:7
8. Bright RW, Elmore SM. Physical properties of epiphyseal plate carti-lage.Surg Forum. 1968;19:463
9. Kleinman PK, Marks SC. A regional approach to the classic metaphy-seal lesion in abused infants: the distal femur.AJR Am J Roentgenol. 1998;170:44
Bladder Retention of Urine as a
Result of Continuous Intravenous
Infusion of Fentanyl: 2 Case
Reports
ABSTRACT. Sedation has been commonly used in the neonate to decrease the stress and pain from the noxious stimuli and invasive procedures in the neonatal intensive care unit, as well as to facilitate synchrony between ven-tilator and spontaneous breaths. Fentanyl, an opioid an-algesic, is frequently used in the neonatal intensive care unit setting for these very purposes. Various reported side effects of fentanyl administration include chest wall rigidity, hypotension, respiratory depression, and brady-cardia. Here, 2 cases of urinary bladder retention leading to renal pelvocalyceal dilatation mimicking hydrone-phrosis as a result of continuous infusion of fentanyl are reported.Pediatrics2001;108:1012–1015;fentanyl, preterm infant, side effects.
ABBREVIATION. NICU, neonatal intensive care unit.
S
edation has been commonly used in the neo-nates to decrease the stress and pain from the noxious stimuli and invasive procedures in the neonatal intensive care unit (NICU). Furthermore, sedation facilitates the synchrony between ventilatorReceived for publication Oct 12, 2000; accepted Jan 29, 2001.
Reprint requests to (U.G.D.) MS 213A, 9701 Watertown Plank Rd, Milwau-kee, WI 53226. E-mail: [email protected]
and spontaneous breaths and reduces physiologic instability.1 Stress responses have been shown to
increase catecholamines and changes in blood pres-sure in neonates. Because the most vulnerable period for intraventricular hemorrhage in preterm neonates is during the first 5 to 7 days of life, it has become a routine in the NICUs to keep infants under minimal handling with sedation in sick, ventilated, preterm neonates.2– 4
Fentanyl, an opioid analgesic, is used frequently for this purpose in NICUs in bolus, as well as con-tinuous infusion doses to achieve effective sedation. Various side effects of fentanyl administration have been reported, including chest wall rigidity,5,6
hypo-tension,7 respiratory depression,7bradycardia,7and
laryngospasm.6Here, we describe 2 cases of urinary
bladder retention as a result of continuous infusion of fentanyl.
CASE REPORTS Case 1
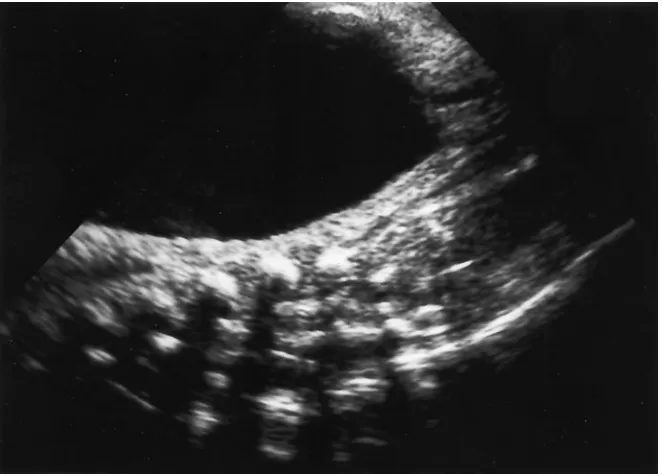
A 1.5-kg, 30 weeks’ gestational age, female infant was born to a 22-year-old gravida 2, para 1 to 2 via cesarean section secondary to placenta previa and late decelerations. At delivery, she was noted to have a weak cry, poor respiratory effort, and a sacral dimple, but the remainder of the physical examination was within normal limits. She was intubated and given surfactant via the endotra-cheal tube. She was also placed on a continuous fentanyl infusion, at a dose of 3g/kg/h. On the third day of her hospitalization, she became hypertensive, for which she received a few doses of Enalapril. Her blood urea nitrogen and creatinine peaked at 36 and 1.3, respectively. Renal ultrasounds at 4 days of age, done primarily to check for renovascular disease as a cause of the hypertension, revealed: diffuse parenchymal lining thinning bilat-erally; right kidney 4-cm long, left kidney 3.5-cm long; moderate increased bilateral echogenicity of renal parenchyma; no abnormal perinephric fluid collections; very large fluid-filled mass extend-ing from pelvis to upper abdomen, probably representextend-ing dis-tended bladder (Fig 1); normal arterial flow in renal arteries; severe bilateral hydronephrosis (Fig 2); and severe bilateral hy-droureter. The urine output was diminished and the differential diagnosis was: 1) urinary tract obstruction attributable to bladder outlet obstruction secondary to possible ureterocele or urogenital sinus malformation or posterior urethral valves, 2) megacystic
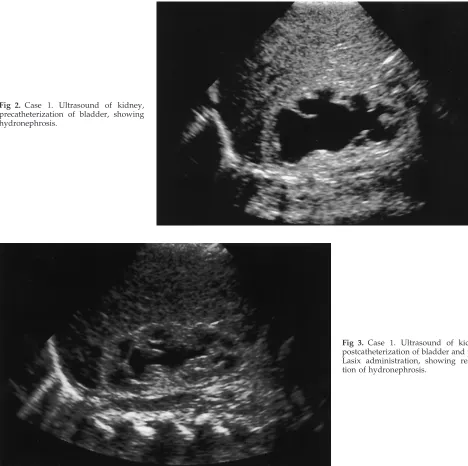
microcolon syndrome, or 3) neurogenic bladder (as patient had a sacral dimple). An indwelling catheter was inserted into the blad-der and a large amount of urine was drained. The follow-up renal ultrasound (Fig 3) revealed: resolution of hydronephrosis and hydroureter, right kidney 3.3-cm. long, and left kidney 3.0-cm long.
At 9 days of age, a voiding cystourethrogram was done and the results were normal.
Case 2
A 1.335-kg, 31 weeks’ gestational age, male infant was born to a 27-year-old gravida 1, para 0 to 1, via emergency cesarean section secondary to maternal pulmonary edema. The infant de-veloped respiratory distress requiring intubation and a total of 4 doses of surfactant. He was placed on a fentanyl drip of 3g/ kg/h shortly after birth and remained on it until 2 days of age. The infant also developed diminished urine output. A renal ultra-sound done at 2 days of age, showed hydronephrosis with a large distended bladder. The bladder was catheterized with an indwell-ing catheter and approximately 40 mL of urine was obtained. A renal ultrasound done at 7 days of age was normal, and a voiding cystourethrogram done at 28 days of age was normal.
DISCUSSION
Both infants described here presented with urinary bladder retention unrelated to anatomic causes. The reason for the urinary retention in both cases was administration of fentanyl, a narcotic. Fentanyl clear-ance during the first few days of life is correlated to the gestational age and birth weight.8Narcotics
de-crease intravesical pressure and inde-crease bladder compliance by partially inhibiting parasympathetic nerves that innervate the bladder.9Parasympathetic
nerves control tone and contraction of bladder. Ad-ditionally, narcotics have been shown to increase urethral sphincter pressures.9Therefore, in
evaluat-ing a sedated infant with bladder distention and/or hydronephrosis, one must look for anatomic abnor-malities, as well as iatrogenic causes.
An ultrasound examination showing a distended bladder with distension of the pelvocalyceal system can be misleading because the presence of a posterior urethral valve in a male newborn can also present
with similar findings. Most of such cases can be diagnosed by prenatal ultrasound examinations, while the bladder distension due to fentanyl infusion in the newborn is a postnatal event, and the effects are reversible by ensuring bladder drainage with an indwelling urinary catheter. Monitoring for urinary output also may not be able to diagnose this condi-tion, as in both of our patients there was some urine output, although quite low (⬍1 mL/kg/h). This was thought to be attributable to the decreased urine output observed frequently in these infants during the first 48 hours after birth. One of our patients was a female, and posterior urethral valve giving rise to bladder distension and subsequent hydronephrosis is unlikely in such a scenario. Both of our patients had mild swelling of the suprapubic area, probably because of the distended bladder; however, it was not very evident clinically.
This complication of bladder distension giving rise to renal pelvocalyceal distension masquerading as
hydronephrosis has not been reported previously in preterm infants with continuous fentanyl infusion alone. This complication is preventable if an indwell-ing catheter is inserted into the bladder. We recom-mend that preterm infants receiving continuous fen-tanyl infusion, even as low a dose as 3 g/kg/h, should have an indwelling urinary catheter, or be closely observed for development of bladder disten-sion.
Utpala G. Das, MD P. Sasidharan, MD Department of Pediatrics Division of Neonatology
Children’s Hospital of Wisconsin Medical College of Wisconsin Milwaukee, WI 53226
REFERENCES
1. Dyke MP, Kohan R, Evans S. Morphine increases synchronous ventila-tion in preterm infants. J Pediatr Child Health. 1995;31:176 –179
Fig 2. Case 1. Ultrasound of kidney, precatheterization of bladder, showing hydronephrosis.
2. Barker DP, Rutter N. Stress, severity of illness and outcome in venti-lated preterm infants.Arch Dis Child. 1996;75:187–190
3. Goldstein RF, Brazy JE. Narcotic sedation stabilizes arterial blood pres-sure fluctuations in sick premature infants.J Perinatol. 1991;11:365–371 4. Orsini AJ, Leef KH, Costarino A, et al. Routine use of fentanyl infusions for pain and stress reduction in infants with respiratory distress syn-drome.J Pediatr. 1996;129:140 –145
5. Wells S, Williamson M, Hooker D. Fentanyl induced chest wall rigidity in a neonate: a case report.Heart Lung. 1994;23:196 –198
6. Fahnenstich H, Steffan J, Kau N, Bartmann P. Fentanyl-induced chest
wall rigidity and laryngospasm in preterm and term infants.Crit Care Med. 2000;28:836 – 839
7. Bowdle TA. Adverse effects of opioid agonists and agonist-antagonists in anesthesia.Drug Safety. 1998;193:173–189
8. Saarenmaa E, Neuvonen PJ, Fellman V. Gestational age and birth weight effects on plasma clearance of fentanyl in newborn infants.
J Pediatr. 2000;136:767–770
9. Terris MK, Merguerian PA. Administration of a neuromuscular block-ing agent and a narcotic agent mimickblock-ing posterior urethral valves in a premature infant.West J Med. 1998;168:194 –196
DRUG STUDIES TO FACE SCRUTINY BY JOURNALS
“Major medical journals plan to tighten rules for drug-industry–sponsored stud-ies, reserving the option to not publish research where investigators are not guaranteed control of study data and publication rights, according to [the] Wash-ington Post. Major journals such as theNew England Journal of Medicine, theJournal of the American Medical Association, theLancet, and others will announce the policy in September 2001. Using publication rights and ownership of study data, firms have sometimes suppressed or spun ambiguous study results to their advantage. The 1997 publication of a University of California-San Francisco researcher’s find-ing that generic thyroid drugs equaled a brand name in performance, released over the objection of the sponsoring company, first brought the issue to national attention. “The issue is an important one, and it’s getting worse,” says Arnold Relman, a former editor of the New England Journal of Medicine.”
USA Today. August 6, 2001
DOI: 10.1542/peds.108.4.1012
2001;108;1012
Pediatrics
Utpala G. Das and P. Sasidharan
Fentanyl: 2 Case Reports
Bladder Retention of Urine as a Result of Continuous Intravenous Infusion of
Services
Updated Information &
http://pediatrics.aappublications.org/content/108/4/1012
including high resolution figures, can be found at:
References
http://pediatrics.aappublications.org/content/108/4/1012#BIBL
This article cites 9 articles, 0 of which you can access for free at:
Subspecialty Collections
skeletal_disorders_sub
http://www.aappublications.org/cgi/collection/rheumatology:musculo
Rheumatology/Musculoskeletal Disorders
following collection(s):
This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtml
in its entirety can be found online at:
Information about reproducing this article in parts (figures, tables) or
Reprints
http://www.aappublications.org/site/misc/reprints.xhtml
DOI: 10.1542/peds.108.4.1012
2001;108;1012
Pediatrics
Utpala G. Das and P. Sasidharan
Fentanyl: 2 Case Reports
Bladder Retention of Urine as a Result of Continuous Intravenous Infusion of
http://pediatrics.aappublications.org/content/108/4/1012
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397.