_____________________________________________________________________________________________________
*Corresponding author: E-mail: mariam.Omar@uob.edu.ly; Mariamelsaltani@gmail.com;
(Past name: British Journal of Medicine and Medical Research, Past ISSN: 2231-0614, NLM ID: 101570965)
Culture, Sun Exposure and Vitamin D Deficiency in
Benghazi Libya
Mariam Omar
1*, Faiza Nouh
1, Manal Younis
2, Moftah Younis
3, Nesma Nabil
1,
Marwa Saad
1and Munyah Ali
11Department of Nutrition, Faculty of Public Health, University of Benghazi, Benghazi, Libya. 2University College Cork, Ireland. 3University of Saskatchewan, Canada.
Authors’ contributions
This work was carried out in collaboration between all authors. Author MO designed and conducted the study, wrote the protocol, managed the literature search and drafted the manuscript. Author FN performed the study analyses, data reporting and tabulation and contributed to literature search. Authors MO, NN, MS and MA collected data and provided technical support in clinics. Authors FN, Manal Younis and Moftah Younisparticipated in the critical revision of the article. All authors read and approved the final manuscript.
Article Information
DOI: 10.9734/JAMMR/2018/39562
Editor(s):
(1)Syed Faisal Zaidi, Department of Basic Medical Sciences, College of Medicine, King Saud Bin Abdulaziz University-HS, National Guard Health Affairs, King Abdulaziz Medical City, Kingdom of Saudi Arabia.
Reviewers:
(1) Md. Nurshad Ali, Shahjalal University of Science and Technology, Bangladesh. (2)Mostafa Saif-Elnasr, Egypt. Complete Peer review History:http://www.sciencedomain.org/review-history/23253
Received 23rd November 2017 Accepted 11th February 2018 Published 20th February 2018
ABSTRACT
Background: Vitamin D is produced from sunlight exposure through ultraviolet B radiation of the skin. Several factors affect sunlight exposure include time of day, seasonal variation, lower absorption of vitamin D due to dark skin color, sunscreen use, clothing and coverage for cultural or religious reasons along with behavioral attitudes. There is a dearth of studies looking into socio-cultural and behavioral reasons for vitamin D deficiency in the Middle East particularly in Libya. The aim of this study was to identify sun exposure and cultural influences on vitamin D status among patients attending three out patient clinics in Benghazi.
Methods: A cross-sectional sample of 287 subjects who were attending three polyclinics in Benghazi. 258 females, and 29 males. Data on participants’ attitudes and behaviors in relation to sun exposure, cultural and skin tone preference were collected using interviews and questionnaires.
Results: Duration of sun exposure, use of sun block, wearing long sleeves, believing lighter skin is more attractive than darker and feeling unhappy if the sun made the skin darker were all significantly different between different serum vitamin D level groups and predicted lower vitamin D levels. Vitamin D deficiency was 76.1%, insufficiency was 15.2% and Vitamin D sufficiency was 8.7% in our study.
Conclusion: Culture, attitudes and sun exposure behavior could be major contributing factors to the observed high prevalence of VDD in this study. Circulating concentrations of 25(OH)D was significantly lower in subjects with less sun exposure and in those exhibiting negative attitudes toward sunlight. A more accurate measure for culture, behavior and knowledge and sun exposure in a controlled environment is needed to confirm these findings.
Keywords: Vitamin D; deficiency; sun exposure; culture; attitudes.
1. INTRODUCTION
Vitamin D is increasingly becoming a public health concern as sufficient sun exposure to prevent vitamin D deficiency (VDD) would avoid a larger burden of disease [1].
Vitamin D is important for musculoskeletal health, and deficiency causes rickets in children and osteomalacia in adults [2]. More research has linked the deficiency with other major diseases as coronary heart disease [3], different types of cancer [4,5], type 1 and 2 diabetes [6-8], hypertension, rheumatoid arthritis, Alzheimer’s [4,9], mental health deterioration [9] and multiple sclerosis [10].
Skin exposure to sunlight is the main determinant of vitamin D status [11]. The vitamin is endogenously produced from ultraviolet B radiation of the skin (UV-B, 280–315 nm) [12,13], with diet contributing only to a small amount of circulating vitamin D levels [11].
Restriction of sunlight resulting from decreased ambient light and living in northern latitudes is easily understood. Other phenomena affecting sunlight exposure include time of day when exposed to sunlight, seasonal variation, lower absorption of vitamin D due to dark skin color, sunscreen use, clothing and coverage due to
cultural or religious reasons when outdoors [14-16], and behavioral attitudes [18-20]. High
prevalence of vitamin D deficiency has been reported even in sunny climates [4,9,21-23].
The prevalence of vitamin D deficiency and rickets is estimated to be greater across the Middle East than Western countries [22]. A large meta-analysis showed that 20–80% of apparently healthy individuals in the Middle East are vitamin D deficient. Cultural traditions [4], and behavioral attitudes whereby Muslim communities avoid
body exposure have been recognized as factors for the scarcity of sun exposure [16,24].
Currently there is a dearth of studies looking into socio-cultural and behavioral reasons for vitamin D deficiency in the Middle East particularly in Libya. Libya; and Benghazi in particular, is located across the Mediterranean Sea (32.0948° N, 20.1879° E) and is sunny most of the year [25], thus sun exposure and levels of vitamin D are expected to be adequate. The aim of this study was to identify cultural and sun exposure behavior effects on vitamin D status among patients attending three out-patient clinics in Benghazi.
2. METHODOLOGY
2.1 Study Participants and Setting
In 2016, a cross sectional study was conducted to determine sun exposure, culture, and attitude and their influence on serum 25(OH)D levels (vitamin D) in a sample of 287 subjects recruited purposively from three polyclinics in Benghazi (Alkiesh polyclinic, Alfohyaht and Yakeen Health Center).
Subjects were eligible if they were (18-80) years old and live in Benghazi. Subjects taking any medications known to alter bone metabolism, and previously VDD diagnosed subjects and receiving VD treatment at the time of study or have received their last treatment less than one month before the study were all excluded. Data sets were also excluded if any parameter investigated was not recorded.
2.2 Procedure
The University Ethics Committee and the
fully informed of the study procedures and aims, and participants provided written informed consent.
Researchers conducted qualitative interviews and interview based questionnaires with individual participants between July the 1st to September 30th 2016. The interview and questionnaire aimed to probe for the participants’ attitudes and behaviors in relation to sun exposure and protection, along with cultural and skin tone preference. The interviews and questionnaires proceeded for about 20 to 30 minutes, usually occurred in the clinic waiting room or at doctor’s office, and were conducted by the researchers who underwent training sessions on interviewing skills, anthropometry taking and data coding and handling at Benghazi University. A small pilot study was conducted and tested, and sample selection and methodology were explained in more details previously [26].
Vitamin D test was collected as part of routine investigation for all subjects. For the current analysis, vitamin D deficiency (VDD) was defined as 25-OHD values of ≤20 ng/ml, insufficiency at 21-29 ng/l; and sufficient serum 25-OHD level at ≥30 ng/ml [27]. Subjects were accordingly divided into 3 diagnostic categories. To reduce bias of different vitamin D analysis techniques, ELISA, an enzyme-linked immunosorbent assay for 25(OH)D; which has been regarded as an accepted test [28], was used for being the most commonly available test in laboratories in Benghazi.
2.3 Statistical Analysis
SPSS version 21 was used for the description and analysis of data. Data was coded before entering into a computer. Chi-square t-test was performed to test the association of serum 25(OH)D with variables, based on predefined cut-points of serum 25(OH)D concentrations. Serum 25(OH)D was normally distributed, confidence intervals were set at 95% and level of significance was defined at p-value of ≤ 0.05. Bivariate correlation was carried out to test the relationships between serum 25(OH)D and other variables. Multiple logistic regression investigated predictors of vitamin D deficiency (serum 25(OH)D of ≤20 ng/ml). Multiple regression model and adjustments for confounding factors were also conducted. Covariates included sun exposure frequency and duration, dress codes, attitudes toward sun
exposure, skin preferences, and use of sun cream and transportations. The goodness-of-fit of a model was assessed using Chi square test and multiple regression model.
3. RESULTS
3.1 Sample Demographics and Serum Vitamin D Level
Out of 319 surveys distributed, 89.9% (total n=287) questionnaires were completed by subjects who chose to participate in this study. 258 females (90%), and 29 males (10%) with mean age range (20-41). Standard deviation (SD) of 36.2 years ± 0.9 (37.4± 3.8) years for females and 29.2 ± 2.9 for males.
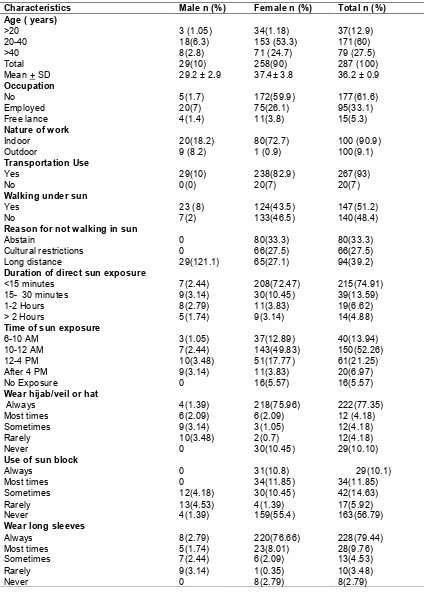
Overall, the estimated prevalence of vitamin D deficiency (≤20 ng/ml) was 76.1%, insufficiency (21-29 ng/ml) was 15.2% and the proportion of the sample population with sufficient vitamin D concentrations (≥30 ng/ml) was 8.7% as shown in Table 1.
3.2 Sun Exposure
With regard to sun exposure variation between subjects, as shown in (Table 1); majority of subjects use vehicles (cars) as a mean of transportation when leaving home (92%), all of those who reported no use of vehicles were females. Half of the whole sample reported not walking under the sun light, (51%) of all females, compared to only (24) % of males. Reasons for not walking were distributed as follows; (39%) of the whole sample mentioned long distance as the reason for not walking under sun light, with the remaining subjects either mentioning traditional and social restrictions as the reason or abstaining from answering the question. The majority of females abstained. While all males regarded long distance as the reason they do not walk under sunlight.
3.3 Culture and Attitudes
(44.6%) of the sample believe fair skin is more attractive than dark; (43.7%) of females agree and strongly agree compared to (51%) among males. (38%) are unhappy “strongly agree” if sun made their skin darker, with (42%) females strongly agreeing to the statement, while (43%) of males disagree.
(58%) of the subjects tend to be careful when going out so their complexion or skin wont look “bad”, 63% of females strongly agree, and 34% males disagree. 14.6% and 8% strongly agree on avoiding sun because fear of wrinkles and cancer.
3.4 Correlation and Predictors of Serum 25(OH) Level
Out of the 287 participants, serum 25(OH)D concentrations were provided by 190 subjects; six subjects were tested by immune essay and thus were excluded. 184 subjects provided test by ELISA with an effective participation rate of 64%.
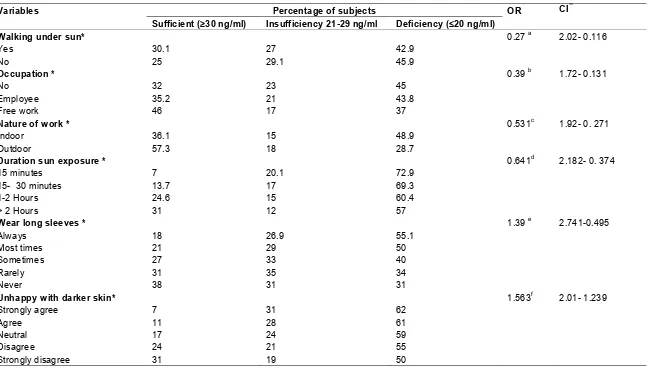
Duration of sun exposure was significantly different across different vitamin D status, those with vitamin d deficiency had the least sun expose duration. Time of sun exposure did not differ significantly, while means of transportation- though not statistically significant- were more in those with less than normal vitamin D level. Detailed in (Table 2).
Occupation and nature of work, walking under sun, using sun block, wearing long sleeves, believing fair skin is more attractive than dark and feeling unhappy if the sun made the skin darker, were all significantly different between different vitamin D groups, with more subjects using sun blocks and holding negative beliefs and attitudes in the vitamin deficiency or insufficiency groups. However, wearing hijab/ face veil or hat, and fear of skin cancer and wrinkles were not significantly different across groups.
Correlation and Significant predictors of vitamin D deficiency are summarized in (Table 2). In the full model, preference of light skin associated with higher odds of deficiency (OR 2.31, CI 4.01- 1.139), using sun block (OR 1.723, CI 3.982-0.9874), feeling unhappy if the sun made skin darker (OR 1.563 CI 2.01- 1.239), wearing long sleeves (OR 1.39 CI 2.741- 0.495) were associated with higher odds of deficiency, while
duration of sun exposure (OR 0.641 CI 2.182- 0.374) nature of work; out door work (OR 0.531CI 1.92- 0.271) occupation (OR 0.39 CI1.72- 0.131) and walking under sun (OR 0.27 CI 2.02- 0.116) were associated with lower odds of the deficiency. When gender was accounted for, similar level of statistical significance, correlation and OR was obtained, including skin preference, dress code, and sun exposure attitudes, however among male gender employment and work type did not differ across different Vitamin D levels. Furthermore, no difference was shown with regard to date of vitamin D test during the study (data not shown).
4. DISCUSSION
This study allowed the examination of sun exposure attitudes and cultural influences on serum 25(OH)D concentrations. Negative attitude toward sun exposure and cosmetic concerns appear to be major contributing factors to the high prevalence of low vitamin D status reported in this sample. It appears that preference of fair skin in both genders especially among females and the tendency to avoid sun light due to fear of darkening of skin were the main attributing factors in this study. Subjects preferring fair skin in both males and females had twice the odds of vitamin D deficiency (OR 2.31). Feeling unhappy if skin was made darker by sun exposure predicted vitamin D deficiency (OR 1.5) in both genders, more among females.
This finding is in accordance with other studies carried in Saudi Arabia, Pakistan, and among Korean and Chinese immigrants in Australia [17,29,30] these studies reported that subjects with VDD longed for fairer completion and tended to avoid sun in fear of darkening the skin.
The idealization of fair complexion, particularly for females, has a long history in many Arabic and East Asian countries. Historically, a fair skin was an indication of privilege, beauty, social status, and femininity. Those from poor, working class families, who had to work outdoors, had rough, sun-tanned skin; fair skin was regarded as “noble” and “aristocratic” and became a symbol of higher social class [31]. In modern times, this idealization has been more related to standards of beauty [32].
Table 1. Age, gender, sun exposure, and cultural attitudes among 287 subjects selected from 3 outpatient clinics in Benghazi
Characteristics Male n (%) Female n (%) Total n (%)
Age ( years)
>20 20-40 >40 Total Mean + SD
3 (1.05) 18(6.3) 8(2.8) 29(10) 29.2 ± 2.9
34(1.18) 153 (53.3) 71 (24.7) 258(90) 37.4± 3.8 37(12.9) 171(60) 79 (27.5) 287 (100) 36.2 ± 0.9
Occupation No Employed Free lance 5(1.7) 20(7) 4(1.4) 172(59.9) 75(26.1) 11(3.8) 177(61.6) 95(33.1) 15(5.3)
Nature of work
Indoor Outdoor 20(18.2) 9 (8.2) 80(72.7) 1 (0.9) 100 (90.9) 100(9.1) Transportation Use Yes No 29(10) 0(0) 238(82.9) 20(7) 267(93) 20(7)
Walking under sun
Yes No 23 (8) 7(2) 124(43.5) 133(46.5) 147(51.2) 140(48.4)
Reason for not walking in sun
Abstain Cultural restrictions Long distance 0 0 29(121.1) 80(33.3) 66(27.5) 65(27.1) 80(33.3) 66(27.5) 94(39.2)
Duration of direct sun exposure
<15 minutes 15- 30 minutes 1-2 Hours > 2 Hours
7(2.44) 9(3.14) 8(2.79) 5(1.74) 208(72.47) 30(10.45) 11(3.83) 9(3.14) 215(74.91) 39(13.59) 19(6.62) 14(4.88)
Time of sun exposure
6-10 AM 10-12 AM 12-4 PM After 4 PM No Exposure 3(1.05) 7(2.44) 10(3.48) 9(3.14) 0 37(12.89) 143(49.83) 51(17.77) 11(3.83) 16(5.57) 40(13.94) 150(52.26) 61(21.25) 20(6.97) 16(5.57)
Wear hijab/veil or hat
Always Most times Sometimes Rarely Never 4(1.39) 6(2.09) 9(3.14) 10(3.48) 0 218(75.96) 6(2.09) 3(1.05) 2(0.7) 30(10.45) 222(77.35) 12 (4.18) 12(4.18) 12(4.18) 29(10.10)
Use of sun block
Always Most times Sometimes Rarely Never 0 0 12(4.18) 13(4.53) 4(1.39) 31(10.8) 34(11.85) 30(10.45) 4(1.39) 159(55.4) 29(10.1) 34(11.85) 42(14.63) 17(5.92) 163(56.79)
Wear long sleeves
Characteristics Male n (%) Female n (%) Total n (%) Wear long legged
Always Most times Sometimes Rarely Never 11(3.83) 7(2.44) 3(1.05) 4(1.39) 4(1.39) 233(81.18) 12(4.18) 7(3.14) 2(0.7) 2(0.7) 244(85.02) 19(6.62) 10(3.48) 6(2.09) 8(2.79
Light skin is more attractive than darker
Strongly agree Agree Neutral Disagree Strongly disagree 9(3.1) 6(2.1) 8(2.8) 6(2.1) 0 42(14.6) 71(24.7) 120(41.8) 5(1.7) 20(7) 51(17.8) 77(26.8) 128(44.6) 11(3.8) 20(7)
Feeling unhappy with darkening of skin due to sun exposure
Strongly agree Agree Neutral Disagree Strongly disagree 2(0.7) 7(2.4) 7(2.4) 10(3.5) 3(1.1) 109(38) 77(26.8) 58(20.2) 2(0.7) 12(4.2) 111(38.7) 84(29.3) 65(22.7) 12(4.2) 15(5.3)
Being cautions to skin when going out
Strongly agree Agree Neutral Disagree Strongly disagree 2(0.7) 5(1.7) 10(3.5) 5(1.7) 7(2.4) 165(57.5) 78(27.2) 1(0.35) 4(1.4) 10(3.5) 167(58.2) 83(28.9) 11(3.8) 9(3.14) 17(5.9)
Avoidance of sun exposure for fear of wrinkles
Strongly agree Agree Neutral Disagree Strongly disagree 3(1.1) 2(0.7) 8(2.8) 9(3.1) 7(2.4) 39(13.6) 63(22) 117(40.8) 2(0.7) 37(12.9) 42(14.6) 65(22.6) 125((43.6) 11(3.8) 44(15.3)
Avoidance of sun due to cancer risk
Strongly agree Agree Neutral Disagree Strongly disagree 1(0.35) 6(2.09) 9(3.14) 7(2.44) 6(2.09) 22(7.67) 36(12.5) 114(39.7) 8(2.8) 78(27.2) 23(8) 42(14.6) 123(42.9) 15(5.2) 84(29.3)
Vitamin D status
<20ng/ml 21-29 ng/ml ≥30 ng/ml Total 2(1.1) 5(2.7) 10(3.3) 17(9.2) 138(75) 23(12.5) 6(3.3) 167(90.8) 140(76.1) 28(15.2) 16(8.7) 184(100)
Published studies suggest that regular use of sunscreen may increase vitamin D deficiency risk [37]. Sunscreens prevent absorption of UV-B radiation and thus sun burning, cancer of the skin and premature aging. Nonetheless; the blocked UV-B radiation is also responsible for the photosynthesis of vitamin D3. Studies indicate
that sunscreens interfere with the cutaneous production of vitamin D3 [38,39].
Using sun block in our study was associated with a reduction of serum vitamin D to deficiency levels, which corresponds to other studies. Our result is in agreement with other similar studies
performed in Saudi Arabia [34], Vietnam [35], Oman [36], and Kuwait [40] where (males and females) exhibited negative attitude towards sunlight exposure by regular use of sunscreens, and embracing other sun protective measures in their daily life leading towards inadequate amount of vitamin D level.
7
Table 2.Correlation and predictors of serum 25(OH) among 184 patients in relation to sun exposure, culture and attitudes
Variables Percentage of subjects OR CI**
Sufficient (≥30 ng/ml) Insufficiency 21-29 ng/ml Deficiency (≤20 ng/ml) Walking under sun*
Yes No
30.1 25
27 29.1
42.9 45.9
0.27 a 2.02- 0.116
Occupation *
No Employee Free work
32 35.2 46
23 21 17
45 43.8 37
0.39 b 1.72- 0.131
Nature of work *
Indoor Outdoor
36.1 57.3
15 18
48.9 28.7
0.531c 1.92- 0. 271
Duration sun exposure *
15 minutes 15- 30 minutes 1-2 Hours > 2 Hours
7 13.7 24.6 31
20.1 17 15 12
72.9 69.3 60.4 57
0.641d 2.182- 0. 374
Wear long sleeves *
Always Most times Sometimes Rarely Never
18 21 27 31 38
26.9 29 33 35 31
55.1 50 40 34 31
1.39 e 2.741-0.495
Unhappy with darker skin*
Strongly agree Agree
Neutral Disagree
Strongly disagree
7 11 17 24 31
31 28 24 21 19
62 61 59 55 50
8
Variables Percentage of subjects OR CI**
Sufficient (≥30 ng/ml) Insufficiency 21-29 ng/ml Deficiency (≤20 ng/ml) Using of sun block *
Always Most times Sometimes Rarely Never
9 14 23 29 34
39 36 32 30 27
52 50 45 41 39
1.723g 3.982-0.9874
Fair skin is more attractive*
Always Most times Sometimes Rarely Never
17.2 25 30 39 49
28.1 24 22 16 11
54.6 51 48 45 40
2.31h 4.01- 1.139
*
P ≤0.05,** CI= confidence interval.
OR reference groups a compared to subjects walking undersunlight, b compared to workers, c outdoor workers, d ≥1 hour of sun exposure, e most times wearing long sleeves, f
attributed to the large representation of females wearing hijab in the sample. On the other hand, wearing long-sleeved clothes predicted VDD in both genders. Area of skin exposed and duration of sunlight exposure strongly correlated with Vitamin D levels in this study as shown similarly by other studies [42,47,48]. Sun exposure of skin areas of face and hands may partially provide synthesis of vitamin D, but may not be adequate to prevent vitamin D deficiency [48], especially considering the short duration of sun exposure reported in this study.
Sun exposure amount required to produce the recommended amount of vitamin D among individuals varies both individually and according to time of day, time of year, and latitude. White people at 40 degrees’ latitude with Type II skin can achieve their annual requirements of vitamin D by spending about 15 minutes in the sun with exposed face, arms and legs 2 to 3 times per week between 11 a.m. and 3 p.m. during the months of May through October [49,50]. People with darker skins require more time in the sun to produce their requirements of the vitamin [3]. The majority of subjects in this study reported exposure to sun light during peak hours, however this was not shown to differ with nor predict serum 25(OH) D levels, and this was explained when duration of sun exposure was taken into consideration; the majority had sun exposure duration less than 15 minutes, longer durations predicted an improvement in serum vitamin level in the studied sample which comes in accordance with the findings of others who reported a corresponding increase in plasma vitamin D concentrations with increasing duration of sun exposure [18,51-53].
Some explanationfor the high prevalence of low vitamin D status is assumed to result from the fact that contemporary humans are adapted to lifestyle changes that have occurred over the past years. Urbanization and fast life style pattern lead to more use of cars rather than walking and direct exposure to sunlight [54,55]. In most of the Middle East countries, indoor lifestyle plays a major role in predisposing the adults and children towards vitamin D deficiency [4]. In this study majority of the subjects with VDD reported using cars when commuting under sun rather than walking. A possible reason for this attitude and behavior can be justified by the rapid socio-economic growth of Arab countries including Libya which affected their traditional lifestyle [56]. This is further verified by the majority of this sample who reported long
distance as the reason for not walking outdoors.
A problem we apparently share with other Arab countries in general. Avoidance and restriction of sunlight exposure has been reported as a major cause of vitamin D deficiency especially in females in Oman [36] Kuwait [40], and Saudi Arabia [57].
The problem maybe further aggravated by working patterns [58]. Working patterns influence our lifestyle and health and determine much of how we use our time [59]. As a substantial proportion of time in adult life is spent working indoors, this has a major influence on sunlight exposure of an individual [60]. Our results add strength to this argument as unemployed and indoor workers in our study had lower vitamin D level, but interestingly this was found in women but not in men. This corresponds to the 1958 British birth cohort which suggested that work may have and adverse influence on Vitamin D status in women but not in men. Women where shown to spend less time outdoors and had less leisure time than men [60,61]. Women are still responsible for most of the housework and family responsibilities and as a result have less leisure time than their male partners [61].
We have previously reported contributing factors for VDD in this same sample [23], which included female gender, older age, obesity, and low consumption of Vitamin D rich food sources. Cultural beliefs and negative attitudes toward sun exposure, working indoors, and low sun exposure shown in this paper also explain the high reported prevalence of VDD and call for nationwide intervention and prevention strategies.
in Libya and to allow advocacy for this public health problem.
5. CONCLUSION
In conclusion, our study demonstrated that circulating concentrations of 25(OH)D was significantly lower in subjects with less sun exposure and in those exhibiting negative attitudes toward sunlight. Identified factors included duration of sun exposure, occupation and type of work, preference of fair skin, feeling unhappy if the sun made the skin darker, use of sun block, and dress code. These factors resulted in excessive sun-avoidance among participants. Culture could be a major contributing factor to the observed high prevalence of VDD in this study. A more accurate measure for culture, behavior, knowledge and sun exposure in a controlled environment are needed to confirm these findings.
CONSENT
As per international standard or university standard, patient’s written consent has been collected and preserved by the authors.
ETHICAL APPROVAL
As per international standard or university standard, written approval of Ethics committee has been collected and preserved by the authors.
COMPETING INTERESTS
Authors have declared that no competing interests exist.
REFERENCES
1. Lucas RM, McMichael AJ, Armstrong BK, et al. Estimating the global disease burden due to ultraviolet radiation exposure. Int J Epidemiol. 2008;37:654-67.
2. Wolpowitz D, Gilchrest BA. The vitamin D questions: How much do you need and how should you get it? J Am Acad Dermatol. 2006;54:301–17.
3. Vieth R, Kimball S. Vitamin D in congestive heart failure. Am J Clin Nutr. 2006;83:731– 2.
4. Holick M. The vitamin D epidemic and its health consequences. J Nutr. 2005;35: 2739S–48S.
5. Grant W. An estimate of premature cancer mortality in the U.S due to inadequate doses of solar ultraviolet-B radiation. Cancer. 2005;94:1867–75.
6. Hyppo ̈nen E, La ̈a ̈ra ̈ E, Reunanen A, Jarvelin M, Virtanen S. Intake of vitamin D and risk of type 1 diabetes: A birth-cohort study. Lancet. 2001;358:1500–3.
7. Lee P, Chen R. Vitamin D as an analgesic for patients with type 2 diabetes and neuropathic pain. Arch Intern Med. 2008;168:771–2.
8. Pittas A, Lau J, Hu F, Dawson-Hughes B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007;92:2017–29.
9. Khalsa K. The vitamin D revolution, how the power of this amazing vitamin can change your life. Hay House Inc., New York; 2009.
10. Mahon B, Gordon S, Cruz J, Cosman F, Cantorna M. Cytokine profile in patients
with multiple sclerosis following vitamin D supplementation. J Neuroimmunol.
2003;134:128–32.
11. Brand C, Abi H, Couch D, Vindigni A, Wark J. Vitamin D deficiency: A study of community beliefs among dark skinned and veiled people. International Journal of Rheumatic Diseases. 2008;11:15–23. 12. Holick MF, MacLaughlin JA, Clark MB,
Holick SA, Potts Jr JT, Anderson RR, et al. Photosynthesis of previtamin D3 in human skin and the physiologic consequences. Science. 1980;210:203–205.
13. Holick MF. Environmental factors that influence the cutaneous production of vitamin D. Am. J. Clin. Nutr. 1995;61: 638S–645S.
14. Reed S, Laya M, Melville J, Ismail S, Mitchell C, Ackerman D. Prevalence of vitamin D insufficiency and clinical associations among veiled east African women in Washington State. Journal of Women’s Health. 2007;16:2.
15. Mahmood S, Rahman M, Biswas SK, Saqueeb SN, Zaman S, Manirujjaman M, Perveen R, Ali N. Vitamin D and parathyroid hormone status in female garment workers: A case-control study in Bangladesh. Biomed Res Int. 2017;2017: 4105375.
16. Siddiqui A, Kamfar H. Prevalence of vitamin D deficiency rickets in adolescent school girls in Western region, Saudi Arabia. Saudi Med J. 2007;28:441-444. 17. Al-Daghri NM, Al-Attas OS, Al-Okail MS,
Alkharfy KM, Al-Yousef MA, Nadhrah HM, et al. Severe hypovitaminosis D is widespread and more common in non-diabetics than non-diabetics in Saudi adults. Saudi Med. J. 2010;31:775–780.
18. Booth SL, Sallis JF, Ritenbaugh C, Hill JO, Birch LL, Frank LD, et al. Environmental and societal factors affect food choice and physical activity: Rationale, influences, and leverage points. Nutr. Rev. 2001;59:S21– _S39 discussion S57–S65.
19. Hjartaker A, Lund E. Relationship between dietary habits, age, lifestyle, and socio-economic status among adult Norwegian women. The Norwegian Women and Cancer Study, Eur. J. Clin. Nutr. 1998;52: 565-572.
20. Wardle J, Parmenter K, Waller J. Nutrition knowledge and food intake. Appetite. 2000;34:269–275.
21. Fuleihan G. Vitamin D deficiency in the Middle East and its health consequences for children and adults. Clinic Rev Bone Miner Metab. 2009;7:77–93.
22. Bahijri SM. Serum 25-hydroxy cholecalciferol in infants and preschool children in the Western region of Saudi Arabia Etiological factors. Saudi Med J. 2001;22:973–9.
23. Sadat-Ali M, AlElg A, Al-Turki H, Al-Mulhim F, Al-Ali A. Vitamin D levels in healthy men in eastern Saudi Arabia. Ann Saudi Med. 2009;29:378–82.
24. Brand C, Hodan Y, Abi D, Couch A, Vindigini A, Wark J. Vitamin D deficiency: A study of community. International Journal of Rheumatic Disease. 2008;11(1): 15-23.
25. Ali AA. Estimation of evapotranspiration in Libya under the impact of plausible global climate change. Polish National Committee International Geosphere-Biosphere Programme. 1997;25.
26. Omar M, Nouh F, Younis M, Younis M, Nabil N, Saad M, Ali M. Vitamin D status
and contributing factors in patients
attending three polyclinics in Benghazi Libya. Journal of Advances in Medicine and Medical Research. 2017;24(5):2231-0614.
27. Holick M, Binkley N, Bischoff-Ferrari H, Gordon C, Hanley D, Heaney R, Murad H, Weaver C. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology and Metabolism. 2011; 96(7):1911–1930.
28. Zerwekh J. Blood biomarkers of vitamin D status. The American Journal of Clinical Nutrition. 2008;87(4):1087S–1091S. 29. Jang H, Kuen Koo F, Ke L, Clemson L,
Cant R, Fraser D, Seibel M, Tseng M, Mpofu E, Mason R, Brock K. Culture and sun exposure in immigrant East Asian women living in Australia, Women & Health. 2013;53(5):504-518.
30. Mahmood K, Akhtar ST, Talib A, Haider I. Vitamin D status in a population of healthy adults in Pakistan. Pak J Med Sci. 2009;25(4):545-550.
31. Li EPH, Min HJ, Belk RW, Kimura J, Bahl S. Skin lightening and beauty in four Asian cultures. Adv Consum Res. 2008;35:444– 9.
32. Kung AW, Lee KK. Knowledge of vitamin D and perceptions and attitudes toward sunlight among Chinese middle-aged and elderly women: A population survey in Hong Kong. BMC Pub Health. 2006;6:226– 36.
33. Al-Kindi MK. Vitamin D status in healthy Omani women of childbearing age: Study of female staff at the Royal Hospital, Muscat, Oman. Sultan Qaboos University Medical Journal. 2011;11(1):56-61.
34. Al-Ghamdi KM, et al. Knowledge, attitudes and practices of the general public toward sun exposure and protection: A national survey in Saudi Arabia. Saudi Pharmaceutical Journal. 2016;24(6):652-657.
35. Ho-Pham LT, et al. Survey on knowledge and attitudes on vitamin D and sunlight exposure in an urban population in Vietnam. Journal of the ASEAN Federation of Endocrine Societies. 2012;27(2):55-59. 36. Nasiruddin Khan, et al. Attitudes and
behavior towards sunlight exposure and knowledge about vitamin D among Omani female university students. EC Nutrition. 2017;8(2):35-42.
sunburn among an Australian urban population. Prev Med. 1992;21:654-669. 38. Matsuoka LY, Ide L, Wortsman J,
Maclaughlin JA, Holick MF. Sunscreens suppress cutaneous vitamin D3 synthesis. The Journal of Clinical Endocrinology & Metabolism. 1987;64(6):1165-1168. 39. Matsuoka LY, Wortsman J, Hanifan N,
Holick MF. Chronic sunscreen use decreases circulating concentrations of 25-hydroxyvitamin D: A preliminary study. Archives of Dermatology. 1988;124(12): 1802-1804.
40. Al-Mutairi N, et al. Photoprotection and vitamin D status: A study on awareness, knowledge and attitude towards sun protection in general population from Kuwait, and its relation with vitamin D levels. Indian Journal of Dermatology Venereology and Leprology. 2012;78(3): 342-349.
41. El-Rassi R, Baliki G, Fulheihan GE. Vitamin D status in Middle East and Africa. Available:http://www.iofbonehealth.org/do wnload/osteofound/filemanager/health_pro
fessionals/pdf/Vitamin-D-re-ports/Vitamin_D-MEast_Africa.pdf (Last Visit December 14th, 2017)
42. Mishal AA. Effects of different dress styles on vitamin D levels in healthy young Jordanian women. Osteoporos Int. 2001;12:931-935.
43. Sedrani SH. Low 25-Hydroxy vitamin D and normal serum calcium concentrations in Saudi Arabia: Riyadh region. Ann Nutr Metab. 1984;28:181-185.
44. Hashemipour S, Larijani B, Adibi H, Javadi E, Sedaghat M, Pajouhi M. Vitamin D deficiency and causative factors in the population of Tehran BMC Public Health. 2004;4(1):38.
45. Meddeb N, Sahli H, Chahed M, et al. Vitamin D deficiency in Tunisia. Osteoporos Int. 2005;16:180-183.
46. El Sonbaty MR, Abdul Ghaffar NU. Vitamin D deficiency in veiled Kuwaiti women. Eur J Clin Nutr. 1996;50:315-318.
47. Alagol F, Shihadeh Y, Boztepe H. Sunlight exposure and vitamin D in Turkish women. J Endocrinol Invest. 2000;23:173-77. 48. Barger-Lux MJ, Heaney RP. Effects of
above average summer sun exposure on serum 25-hydroxyvitamin D and calcium absorption. The Journal of Clinical
Endocrinology & Metabolism. 2002;87(11): 4952-4956.
49. Kroll MH, Bi C, Garber CC, Kaufman HW, Liu D, Caston-Balderrama A, Zhang K, et al. Temporal relationship between vitamin D status and parathyroid hormone in the United States. PLoS One. 2015;10(3): e0118108.
50. Lambing CL. Osteoporosis, Proceeding of the American Academy of Family Physicians, Annual Scientific Assembly, New Orleans, Louisiana; 2003.
51. Brazerol WF, McPhee AJ, Mimouni F, Specker BL, Tsang RC. Serial ultraviolet B exposure and serum 25 hydroxyvitamin D response in young adult American blacks and whites: No racial differences. J. Am. Coll. Nutr. 1988;7:111–118.
52. Al-Othman A, Al-Musharaf S, Al-Daghri NM, Krishnaswamy S, Yusuf DS, Alkharfy KM, et al. Effect of physical activity and sun exposure on vitamin D status of Saudi children and adolescents. BMC Pediatr. 2012;12:92.
53. Ardawi MS, Qari MH, Rouzi AA, Maimani AA, Raddadi RM. Vitamin D status in relation to obesity, bone mineral density, bone turnover markers and vitamin D
receptor genotypes in healthy Saudi pre-and post menopausal women.
Osteoporosis International. 2011;22(2): 463-475.
54. Hollis BW. Circulating 25-hydroxyvitamin D levels indicative of vitamin D sufficiency: Implications for establishing a new effective dietary intake recommendation for vitamin D. The Journal of Nutrition. 2005;135(2):317-322.
55. Cordain L, Eaton SB, Sebastian A, Mann N, Lindeberg S, Watkins BA, et al. Origins and evolution of the Western diet: Health implications for the 21st century. The American Journal of Clinical Nutrition. 2005;81(2):341-354.
56. Nutrition Country Profile Libyan Arab Jamahiriya. Geneva: World Health Organization; [Last Updated on 2015 August]. (Accessed 15th Dec 2017)
57. Kensarah OA, et al. Vitamin D status of healthy school children from western Saudi Arabia. Pakistan Journal of Nutrition. 2012;11(3):288-292
approach in National policy. Br J Nutr. 2010;104:309-14.
59. Bambra C, Gibson M, Sowden AJ, et al. Working for health? Evidence from systematic reviews on the effects on health and health inequalities of organisational changes to the psychosocial work environment. Prev Med. 2009;48:454.
60. Ward W, Berry D, Power C, Hyppönen E. Working patterns and vitamin D status in mid-life: A cross-sectional study of the 1958 British birth cohort. BMJ. 2011;68(12):902-907.
61. Boivin DB, Tremblay GM, James FO. Working on atypical schedules. Sleep Med. 2007;8:578-89.
_________________________________________________________________________________ © 2018 Omar et al.; This is an Open Access article distributed under the terms of the Creative Commons Attribution License
(http://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium,
provided the original work is properly cited.
Peer-review history: