Comparing the Usability of Paediatric Weight Estimation Methods:
a Simulation Study
Dr Robin D Marlow1,2, Dr Dora L B Wood3, Dr Mark D Lyttle4,5
1) Academic clinical lecturer in Paediatric Emergency Medicine,
Faculty of Health Sciences, University of Bristol.
2) Registrar in Paediatric Emergency Medicine,
Bristol Royal Children’s Hospital, Upper Maudlin Street, Bristol, BS2 8AE
3) Consultant in Paediatric Intensive Care,
Bristol Royal Children’s Hospital, Upper Maudlin Street, Bristol, BS2 8AE
4) Consultant in Paediatric Emergency Medicine,
Bristol Royal Children’s Hospital, Upper Maudlin Street, Bristol, BS2 8AE
5) Senior Research Fellow, Faculty of Health and Applied Sciences, University of the West of
England, Bristol
Corresponding Author
:Dr Robin Marlow, Bristol Royal Children’s Hospital, Upper Maudlin Street, Bristol, BS2 8AE
[email protected] 07989348023
Manuscript word count
: 1398Abstract
Objective: Estimating weight is essential in order to prepare appropriate sized equipment and doses
of resuscitation drugs in cases where children are critically ill or injured. Many methods exist with
varying degrees of complexity and accuracy. The most recent version of the Advanced Paediatric
Life Support (APLS) course has changed their teaching from an age based calculation method to the
use of a reference table. We aimed to evaluate the potential implications of this change.
Method: Using a bespoke online simulation platform we assessed the ability of acute paediatric staff
to apply different methods of weight estimation. Comparing the time taken, rate and magnitude of
errors made using the APLS single and triple age based formulae, Best Guess, and reference table
methods. To add urgency and an element of cognitive stress, a time based competitive component
was included.
Results: 57 participants performed a total of 2240 estimates of weight. The reference table was the
fastest (25(22-28) vs 35(31-38) to 48(43-51) seconds) and most preferred, but errors were made
using all methods. There was no significant difference in the percentage accuracy between methods
(93-97%) but the magnitude of errors made were significantly smaller using the three APLS formulae
10%(6.5-21) compared to reference table (69%(34-133)) mainly from month/year table confusion.
Conclusion: In this exploratory study under psychological stress none of the methods of weight
estimation were free from error. Reference tables were the fastest method but also had the largest
INTRODUCTION
In acutely ill or injured children, estimates of weight are often used to calculate drug and fluid
dosage, and select appropriately sized equipment. Many methods exist, attempting to optimise the
balance between ease of use and accuracy. The most accurate are based on physical measurements
such as length or mid-arm circumference,[1] but those commonly used in the UK are age-based;
these are particularly applicable in Emergency Departments as with an ambulance pre-alert they
allow preparations to be made prior to the arrival of a child. In 2011, the Advanced Paediatric Life
Support (APLS) recommendations changed from using a single formula to three. However the UK
Resuscitation Council maintained that complexity increases risks of error and advocated the use of a
single formula.[2] The most recent revision of the APLS handbook moves away from traditional
calculation methods, now advocating the use of a reference table.[3] However to date no studies
have assessed the crucial human factors affecting ease of use or rates of error of these different
approaches. This project aimed to pilot a technique for testing accuracy, speed and user preference
(usability) of different methods.
METHODS
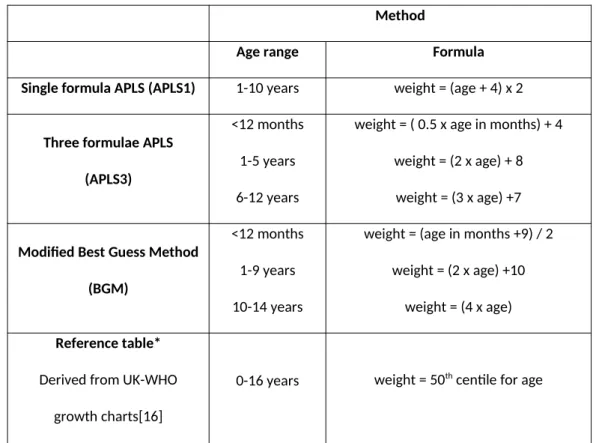
We developed an interactive game website (www.pemresearch.org) where participants estimated weights using APLS single and three formula, Best guess[4], and reference table methods (table 1) to a set range of ages. Questions were grouped by method with starting block and order of ages
randomised for each attempt. All subjects answered the same sets of questions estimating the
weight of 6 months, 1, 5, 7, 10, 13 and 15 year olds; with the relevant formulae/table of the method
being tested visible for reference at the time.
To replicate some of the human factors which may influence a resuscitation situation, psychological
stress was generated by a large visible running timer – participants were made aware of a
medical students and doctors were recruited through word of mouth and social media. Pre-test
participants were asked their usual method of weight estimation and after the test which of the four
methods they preferred. As the study was a maths quiz open to anyone to enter, following the
Health Research Authority guidance ethical approval was not required and so was not sought. As a
pilot study no power calculation was performed.
Inter-method variability of speed and accuracy were analysed for normally distributed data using
one way repeated measures ANOVA with post hoc pairwise t-tests, and for non-parametric data we
used Kruskal and Dunn tests. P-values were adjusted for multiple testing using the Holm method.
Analysis was done using R.[5] Comparing the responses to the expected answers we categorised
errors into simple arithmetical, data entry or month/year confusion. Answers were considered an
error if not equal to the result generated by the formulae/table for the current age being assessed
and were analysed as rates, absolute and percentage difference from correct answer. Errors more
than ten times larger or smaller than the correct answer were deemed input errors and excluded
RESULTS
57 acute paediatric staff (table 2) completed the test with a median of 1.4 attempts each (range 1-6).
In practice 71% reported routinely using the single formula APLS method. Post-test 69% reported a
preference for the reference table method, finding it easiest to use.
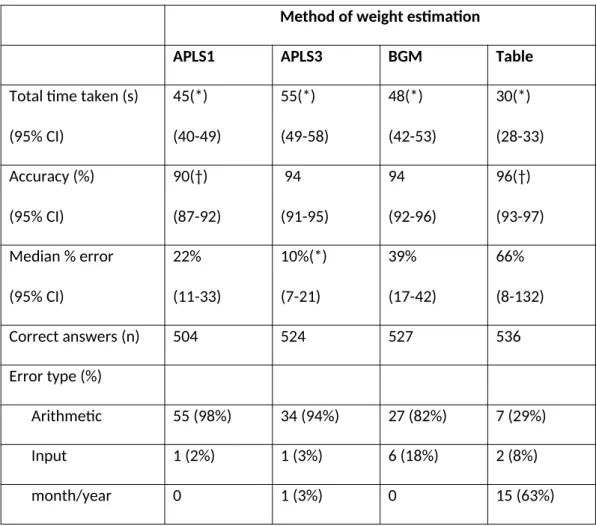
Comparing the total time taken to complete the tests, the reference table method was significantly
quicker to use than other methods (p<0.001). (Table 3) Comparing the accuracy of the methods,
there were significantly more errors made using the single formula APLS compared to using the
reference table (p=0.002). However most errors using the single formula APLS occurred when it was
applied to 6 month olds; as the formula is only recommended between the ages of 1-10 years we
repeated the analysis excluding the 6 month task. This demonstrated no significant difference in
accuracy between these methods (Table 4). Across the 2240 answers provided there were only 10 errors classified as input type.
The magnitude of errors made using the triple formulae APLS method was significantly less than the
other methods (p=0.02, 0.02 0.05), with a median percentage error of 10% of bodyweight compared
to 22-65% using other methods. Whilst overall the table method had the lowest frequency of errors,
a proportion of these were disproportionately large; mainly due to month/year confusion.
DISCUSSION
Our novel method of assessing usability found significant differences in the speed of use of different
age based methods of weight estimation. Using this as a proxy for task difficulty suggests that the
use of single formula or a reference table are easier tasks to carry out than the other methods.
However speed did not automatically correlate with accuracy of application. Whilst reference tables
were faster and there was a non-significant trend to more frequent correct usage, the magnitude of
Many studies have examined the predicted accuracy of estimation methods against a population’s
true weight with no consensus of the ideal method[6], but few studies have examined their practical
application in real world settings. Age based calculations tend to underestimate true weight but
instead predict an ideal bodyweight which, due to the pharmacological properties of most
resuscitation drugs, may be more suitable.[7] The only other study comparable to ours applied both
age and length based methods to a cohort of 80 children in the USA, and found a 5% error of
application rate, with device based methods (e.g. tapes) having the highest rate of application errors
(25%).[8]
The additional choices and calculation inherent in paediatric resuscitation increase cognitive loading.
[9] An alternative method to avoid weight estimation altogether by having pre-assigned equipment
and drawn up medications in broad age based categories.[10] Although conceptually simpler this
requires dedicated colour coded equipment and leads to improvement but not abolition of error.
[11] With an increasing move in medicine to checklists for cognitive unloading, the use of a
pre-populated table of weights, drug doses and equipment sizes for age is highly appealing and would
seem to facilitate the optimum balance of usability and accuracy. We seem to have come full circle
as these were first described in the 1980s,[12] but with concerns over their accuracy [13] they fell
out of favour in preference for the APLS calculation methods. Whilst technological innovations
including device applications promise the potential for more complex calculations, the practicalities
of touch-screens, blood and latex gloves represent significant barriers in high pressure clinical
scenarios. With critically unwell or injured children we feel the paradigm must be avoidance of
errors through simplification. Poor design in aviation[14] and anaesthesia[15] cognitive aids has
been linked to harmful effects. Our data suggest that reference tables should also be designed in a
way to minimise potential picking errors.
As with all clinical medicine we have to be pragmatic; estimated weight will rarely be as accurate as
should be guided by response. More accurate methods bring with them more complexity, even
before considerations of body composition are taken into account. But we should remember that
the evidence base for paediatric dosing in general is limited and there are practical limitations
around the accuracy of small volume doses of many drugs (for example. adrenaline) that can be
administered. We would hope that in a team situation other members would identify and challenge
implausible weights, although this identification would become less likely with increasingly
uncommon interventions - there may be less recognition of a reasonable value for e.g. defibrillation.
With the initial identification of weight such a crucial component of the resuscitation perhaps there
should be a formalised second person check as is commonplace during the preparation of drug
doses.
CONCLUSION
In summary, our study which stress tested individuals applying methods of weight estimation under
time pressure revealed significant differences in task difficulty and identified unexpected sources of
error. With significant mistakes still made in 5-10% of cases we feel usability must be an important
consideration in the development of future methods of emergency decision making. Simply
providing a list of weight values is not enough to avoid errors, with design and layout important
factors that require assessment before clinical use. We feel our simple tool provides a method of
rapid evaluation to identify and prevent uncommon but potentially significant errors.
FUNDING SOURCES
– none.
What is known about this topic:
There are many methods of weight estimation of children balancing complexity and
accuracy.
The use of checklists helps cognitive unloading during stressful tasks.
The Advance Paediatric Life Support course is moving away from calculations in favour of
reference tables.
What this study adds:
Weight look-up tables are faster to use and preferred by clinicians over calculations
REFERENCES
[1] Wells M, Goldstein LN, Bentley A. The accuracy of emergency weight estimation systems in children-a systematic review and meta-analysis. Int J Emerg Med 2017;10:29. doi:10/gc93qp. [2] FAQs Paediatric Life Support n.d. https://www.resus.org.uk/faqs/faqs-paediatric-life-support/
(accessed October 11, 2017).
[3] Samuels M, Wieteska S, editors. Advanced paediatric life support: a practical approach. Sixth edition. Chichester, West Sussex, UK; Hoboken, NJ, USA: John Wiley & Sons, Ltd; 2016.
[4] Thompson MT, Reading MJ, Acworth JP. Best Guess method for age-based weight estimation in paediatric emergencies: Validation and comparison with current methods. Emerg Med Australas 2007;19:535–42. doi:10.1111/j.1742-6723.2007.01031.x.
[5] R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2014.
[6] Young KD, Korotzer NC. Weight Estimation Methods in Children: A Systematic Review. Ann Emerg Med 2016;68:441-451.e10. doi:10.1016/j.annemergmed.2016.02.043.
[7] Carasco CF, Fletcher P, Maconochie I. Review of commonly used age-based weight estimates for paediatric drug dosing in relation to the pharmacokinetic properties of resuscitation drugs. Br J Clin Pharmacol 2016;81:849–56. doi:10.1111/bcp.12876.
[8] Abdel-Rahman SM, Jacobsen R, Watts JL, Doyle SL, OʼMalley DM, Hefner TD, et al. Comparative Performance of Pediatric Weight Estimation Techniques: A Human Factor Errors Analysis. Pediatr Emerg Care 2015:1. doi:10.1097/PEC.0000000000000543.
[9] Luten R, Wears RL, Broselow J, Croskerry P, Joseph MM, Frush K. Managing the unique size-related issues of pediatric resuscitation: reducing cognitive load with resuscitation aids. Acad Emerg Med Off J Soc Acad Emerg Med 2002;9:840–7.
[10] Luten R. Error and time delay in pediatric trauma resuscitation: addressing the problem with color-coded resuscitation aids. Surg Clin North Am 2002;82:303–14, vi.
[11] Moreira ME, Hernandez C, Stevens AD, Jones S, Sande M, Blumen JR, et al. Color-Coded Prefilled Medication Syringes Decrease Time to Delivery and Dosing Error in Simulated Emergency Department Pediatric Resuscitations. Ann Emerg Med 2015;66:97-106.e3.
doi:10.1016/j.annemergmed.2014.12.035.
[12] Oakley PA. Inaccuracy and delay in decision making in paediatric resuscitation, and a proposed reference chart to reduce error. BMJ 1988;297:817–9.
[13] Alexander R, El-Moalem HE. Comparison of two paediatric resuscitation charts for ease of use. Resuscitation 1998;38:151–5.
[14] Kathleen L. Mosier, Everett A. Palmer, Asaf Degani. Electronic Checklists: Implications for Decision Making. Proc Hum Factors Ergon Soc Annu Meet 1992;36:7–11.
doi:10.1177/154193129203600104.
[15] Marshall S. The use of cognitive aids during emergencies in anesthesia: a review of the literature. Anesth Analg 2013;117:1162–71. doi:10.1213/ANE.0b013e31829c397b.
Table 1: Methods of weight estimation compared in the study.
Method
Age range Formula
Single formula APLS (APLS1) 1-10 years weight = (age + 4) x 2
Three formulae APLS
(APLS3)
<12 months 1-5 years 6-12 years
weight = ( 0.5 x age in months) + 4 weight = (2 x age) + 8 weight = (3 x age) +7
Modified Best Guess Method
(BGM)
<12 months 1-9 years 10-14 years
weight = (age in months +9) / 2 weight = (2 x age) +10
weight = (4 x age)
Reference table*
Derived from UK-WHO growth charts[16]
0-16 years weight = 50th centile for age
(*reference table as provided to participants available as online supplement)
Table 2: Grade and speciality of respondents
Table 3 – Results of estimation estimates for each method.
Method of weight estimation
APLS1 APLS3 BGM Table
Total time taken (s)
(95% CI)
45(*)
(40-49)
55(*)
(49-58)
48(*)
(42-53)
30(*)
(28-33)
Accuracy (%)
(95% CI)
90(†)
(87-92)
94
(91-95)
94
(92-96)
96(†)
(93-97)
Median % error
(95% CI)
22%
(11-33)
10%(*)
(7-21)
39%
(17-42)
66%
(8-132)
Correct answers (n) 504 524 527 536
Error type (%)
Arithmetic 55 (98%) 34 (94%) 27 (82%) 7 (29%)
Input 1 (2%) 1 (3%) 6 (18%) 2 (8%)
month/year 0 1 (3%) 0 15 (63%)
Comparing each method by pairwise analysis, (*) denotes that a result is significantly different from
the three others methods (p<0.05). Pairs of results marked with (†) are significantly different from
Table 4 - Results of estimation estimates for each method - excluding the 6m old task.
Method of weight estimation
APLS1 APLS3 BGM Table
Total time taken (s)
(95% CI)
35(*)
(31-38)
48(*)
(43-51)
38(*)
(34-42
25(*)
(22-28)
Accuracy (%)
(95% CI)
95
(92-97)
93
(90-95)
94
(92-96)
96
(94-98)
Median % error
(95% CI)
24%
(10-60)
10%(†)
(7.0-21)
32%
(17-67)
70%(†)
(34-133)
Correct answers (n) 455 444 453 461
Error type
Arithmetic 25 (100%) 34 (94%) 21 (78%) 3 (16%)
Input 0 1 (3%) 6 (22%) 1 (5%)
month/year 0 1 (3%) 0 15 (79%)