International Journal of Applied Exercise Physiology
2322-3537 www.ijaep.com Vol.7 No.1
Received: October 2017 , Accepted: February 2018 , Available online: March 2018
The effect of 12-weeks resistance and endurance training on the serum levels
NGF, BDNF, and VDBP in women with multiple sclerosis
Mitra Khademosharie1, Vahid Tadibi*2, Naser Behpoor2, Mohammad Reza Hamedinia3
1. PhD student of exercise physiology, Razi University, Iran 2. Associate Professor of exercise physiology, Razi University,Iran, 3. professor of exercise physiology, Hakim Sabzevari University, Iran
Corresponding author: Vahid Tadibi, Associate Professor of exercise physiology, Razi University, Iran. Tel:
09181321796 Email: [email protected]
DOI 10.22631/ijaep.v7i1.228
Abstract:
Recent studies suggest that patients with multiple sclerosis (MS) have low levels of neurotrophic factors such as nerve growth factor (NGF), brain-derived neurothrophic factor(BDNF) and the vitamin D-binding protein(VDBP). Moreover, the results of recent studies show that exercise training may have potential effects on these factors in people with MS. The purpose of the present study was to investigate the effect of 12-week resistance and endurance training program on the serum levels of neurotrophic factors in women with MS. A randomized controlled clinical trial was conducted in 24 volunteer MS patients (Expanded Disability Status Scale range of 1–5). The resting serum levels of BDNF, NGF, VDBP, body composition variables, and disability scale values were determined before and after the intervention. The intervention consisted of three sessions of combined training a week for 12 weeks (two sessions of aerobic and one session of resistance training, progressively). The results showed a significant decrease in the percentage of body fat (p=0.003), and disability scale value (p=0.007) in the experimental group. However no significant changes were observed in other variables. The results obtained in the present study indicated that although the resistance and endurance training for three non-consecutive days per week for 12 weeks has no significant effect on neurotrophics and VDBP, it triggered positive effects on the percentage of fat in the body, and the disability scale of women with MS. So, such a training seems a useful physical practice for people with MS.
1. Introduction
Multiple sclerosis is often described as a chronic, immune-mediated disease of the CNS, although neurodegenerative processes are increasingly being recognised in its pathogenesis[1]. MS is often associated with some symptoms (eg, fatigue and depression) and dysfunction (eg, mobility and cognitive impairment), which often affects the quality of life and participation in everyday life activities negatively [2]. Despite much attempt made by researchers, there is no definitive medical treatment for MS, with the currently available medications and treatments being only effective in relieving its side effects, and in preventing its recurrent attacks [3,4].
Neurotrophic factors, that is, the growth factors (such as neurotrophics) necessary for the survival of nerve cells, promote the survival rate of the nerve cells through inhibiting the nerve cells involved in the initiation of the programmed death of cells. They are also important in the differentiation of stem cells from neural cells[5]. Moreover, Nerve growth factor (NGF), the first recognized member of neurotrophics, is of great importance for the growth and phenotypic maintenance of neurons in the peripheral nervous system, and also for the functional accuracy of the cholinergic neurons in the central nervous system[6].
Another member of the neorotrophin family, Brain-derived neorotrophic factor (BDNF), serves to encourage the creation, growth, and survival of neurons and synapses [5]. Moreover, the results of the studies done so far indicate that vitamin D level is one of the important factors to be considered in patients with MS [7]. More specifically, the results of previous studies revealed a significant positive association between higher levels of 25-hydroxy vitamin D and a reduced risk of MS. Moreover, MS Patients had a lower level of
serum 25-hydroxy vitamin D, especially before the recurrent stage [8-10]. The main plasma protein carrying vitamin D and its metabolites is Vitamin D-binding protein(VDBP). It is responsible for transferring vitamin D3 to the liver and
25-hydroxy vitamin D to the kidneys. It also serves the function of transferring 25 and 1-hydroxy vitamin D to the targeted organs[11]. The results of recent studies have revealed that, during the acute phase of demyelination, VDBP level is low in the cerebrospinal fluid in patients with MS[12,13].
The results of numerous studies on animals have confirmed that exercise can have neuro-protective and -regenerative potential in that it induces neurogenesis in the hippocampus, an important brain structure for learning and memory[14,15]. These findings are in line with clinical observations in neurodegenerative diseases such as Parkinson's disease[16] or Alzheimer's disease[17], in which aerobic exercise has been found to be effective in reducing symptoms and delaying the disease progression. However, there is still controversy over the possible effect of physical activities in controlling MS.
Partly due to the fact that there has not been conclusive information on the most appropriate physical activities effective in controlling MS, it is widely believed that patients with MS should avoid intense physical activities in that such activities increase the body temperature, thus worsening the existing symptoms. However, over the last few years, our understanding of health and the type of physical activities (training) suitable for patients with MS has greatly improved[3,4].
78 International Journal of Applied Exercise Physiology www.ijaep.com
that an appropriate exercise therapy can be effective in suppressing (reducing) the symptoms of the disease[21-26]. In these studies, some MS patients were given either a resistance or aerobic physical activities while other MS patients[22,24,25] received a combined exercise training[23,26]. Generally speaking, MS patients suffer several functional problems including a decreased muscle strength and endurance[2], as well as a comparatively low cardiorespiratory endurance and flexibility[3].Therefore, patients with MS should be given a combination of aerobic and resistance training. To our knowledge, in the literature, there are only 6 projects on the effects of these important factors on the brain functioning of MS patients. However, the results obtained in these projects were contradictory[27-32]. Moreover, the majority of these studies focused on the effects of aerobic training, with none of them studying the effects of a combined exercise training program on these three factors in MS patients. Hence, the present study is aimed at examining the effect of the provision of one course of combined exercise training(aerobic and resistance) on the biochemical factors in patients with MS.
2. Method
The participants for the present randomized controlled trial (RCT) were patients with primary or secondary progressive MS (PPMS/SPMS)[33] and moderate disability (EDSS 1–5) (approved by specialists through tests of MS diagnosis, including MRI or CT scan and functional tests on balance, power, ability, walking, and visual and tactile tests) selected from among the members of the MS society at Sabzevar (IRAN).
After the approval by specialists, 24 interested female MS patients, between 20 to 50 years of age, were selected using an available sampling procedure, and were then assigned to the experimental (12 subjects) and control(12 subjects) groups.
However, those with medical
contraindications for exercise therapy (such as cardiovascular or major orthopedic disease), severe developmental, psychiatric, or neurological disorders other than MS, or any regular exercise training were excluded from the study.
After the initial enrollment of the subjects, the participants took part in an introductory meeting to get informed of the overall plan of the study, and the nutritional and medical programs to be followed. Having passed some cardiorespiratory tests necessary for the inclusion in the study, the final participants delivered their formal written consent to participate in the study. Then, for each subject, the necessary demographic and anthropometric information including age, weight, height, and subcutaneous fat percentage were recorded. This study being in accordance with the Helsinki declaration as revised in 2013, the ethics committee of the university approved the study morally (IR.MEDSAB.REC.1394.137)(
IRCT2017032633146N1).The training programs were tailored to the individual level of fitness of the participants, as determined by Rockport walk test at baseline.
Blood samples were taken from all subjects in the control and experimental group in the morning before breakfast. Then, the subjects in the experimental received exercise training while the subjects in the control group received no exercises and were asked to do their normal activities. After an interval of 12 weeks, the second blood samples were taken. However, two subjects from the experimental and 2 from the control group did not show up for the second blood sampling (post test). But the variables of weight, body fat, and disability scale were measured for these subjects.
2.1.Demographic information and disability scale:
79 International Journal of Applied Exercise Physiology www.ijaep.com
Resistance and endurance training, multiple sclerosis VOL. 7 (1)
height and the weight of the subjects, respectively. In addition, caliper was used to measure the fat percentage in the body (by an expert(. Finally, the physical disability of the subjects in both groups was measured using the expanded disability status scale.
2.2.Training program
Under the supervision of a specialist in exercise physiology, the participant received training three sessions in a week for a total period of 12 weeks(2 sessions of resistance training and 1 session of endurance training). The sessions were conducted in the afternoon in the gym with tolerable and appropriate levels of temperature and humidity for the patients.
In each session, balance and flexibility exercises were performed along with a 15 minute warm- up and a 10-minute cool-down. Resistance training included leg press, bench press, biceps curl, knee
extension and flexion, shoulders, leg dorsiflexion and plantar flexion performed with body-building devices whereas endurance training included jogging and age-appropriate rhythmic aerobic training, which were done in intervals. At the end of each session, cooling down was conducted in the form of slow running and stretching activities.
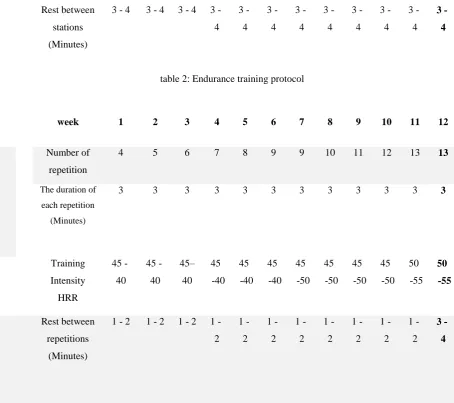
The intensity of resistance training was gradually increased in the course of training period following ACSM guidelines, with 60 to 80% of one repetition maximum, one session per week, 2 to 4 sets, 8-14 repetitions, and 3 to 4 minutes intervals between the sets. The aerobic training were done, similarly; with intervals and intensity of 40 to 55% HRR, 4-13 repetitions, and 1-2 minutes intervals between the sets[2].Table 1 and 2 summarize these protocols.
Table1: Resistance training protocol
12 11 10 9 8 7 6 5 4 3 2 1 week 8 8 8 8 8 8 8 8 8 8 8 8 Number of stations 8-10 8-10 8-10 8-10 10-12 10-12 10-12 10-12 12-14 12-14 12-14 12-14 repetition 4 4 4 4 3 3 3 3 2 2 2 2 set
3 -4 3
-4 3
-4 3
-4 3
-4 3
-4 3
-4 3
-4 3
-4 3 4 -3 4 -3 4
-Rest between
sets
(Minutes)
80 International Journal of Applied Exercise Physiology www.ijaep.com
3 -4 3
-4 3
-4 3
-4 3
-4 3
-4 3
-4 3
-4 3
-4 3 4 -3 4 -3 4
-Rest between
stations
(Minutes)
table 2: Endurance training protocol
12 11 10 9 8 7 6 5 4 3 2 1 week 13 13 12 11 10 9 9 8 7 6 5 4 Number of repetition 3 3 3 3 3 3 3 3 3 3 3 3
The duration of
each repetition (Minutes) 50 55 50 55 45 50 45 50 45 50 45 50 45 40 45 40 45 40 45– 40 45
-40 45
-40 Training
Intensity
HRR
3 -4 1
-2 1
-2 1
-2 1
-2 1
-2 1
-2 1
-2 1
-2 1 2 -1 2 -1 2
-Rest between
repetitions
(Minutes)
2.3.Blood sampling and biochemical analyses
from all participants, a blood sample of 5 cc was taken from the brachial vein, 48 hours after the last training session in the fasting state and half an hour after break in the sitting state. 2 cc of the blood were sent to laboratory to test for CBC. The remaining 3 cc were centrifuged and kept in three alicots, in the refrigerator at -80 0c for biochemical tests (measuring VDBP, BDNF, and NGF).
The NGF, VDBP, and BDNF levels in the blood were measured with an Eliza kit following the instruction offered by the manufacturing country, Human Nerve Growth Factor (NGF) ELISA Kit, Eastibiopharm, Torrance, USA; Human Vitamin D-Binding Protein(VDBP) ELISA Kit, Eastibiopharm, Torrance, USAand Human Brain-Derived Neurotrophic Factor(BDNF) ELISA Kit, Boster Biollogical Technology, Pleasanton, CA, USA and at sensitivity degree of NGF(2.48 pg/ml), VDBP(5.41 µg/ml) and BDNF(<2
pg/ml).
2.4.Statistical Methods
The descriptive statistics including mean and standard deviation were run on the
81 International Journal of Applied Exercise Physiology www.ijaep.com
Resistance and endurance training, multiple sclerosis VOL. 7 (1)
distribution. Moreover, an analysis of covariance(ANCOVA) was performed on the data to compare the obtained means for the variables. All the descriptive and
inferential statistical test were performed on the collected data using SPSS22, at a significance level of p<0.05.
3. Results
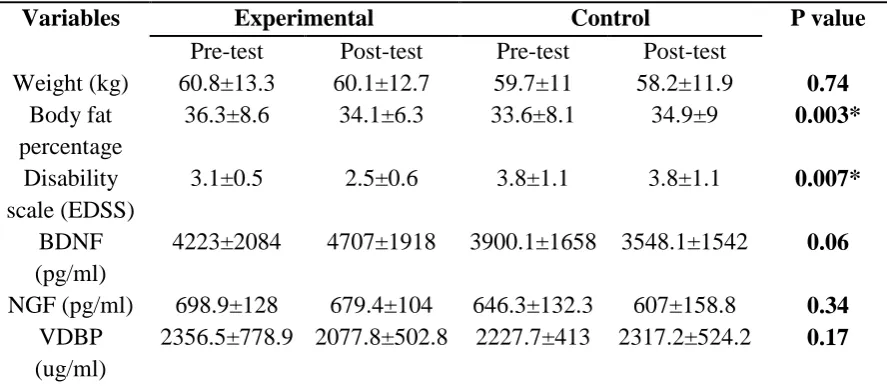
The changes in serum level at resting state, and changes in responsivity after the training period in the intervention group (n =10) were compared to those of the control group (n=10), 4 subject was excluded as described previously. There was no significant change in body weight.
However, exercise training led to a significant decrease in the percentage of the body fat, and the disability of the patients.
In addition, exercise training did not induce any significant change in the biochemical variables (BDNF, NGF, VDBP) .Table 3 summarizes the results.
Table 3. Changes in anthropometric variables, subjects' disabilities, and biochemical variables before and after training (mean± standard deviation)
P value Control
Experimental Variables
Post-test Pre-test
Post-test Pre-test
0.74 58.2±11.9
59.7±11 60.1±12.7
60.8±13.3 Weight (kg)
0.003* 34.9±9
33.6±8.1 34.1±6.3
36.3±8.6 Body fat
percentage
0.007* 3.8±1.1
3.8±1.1 2.5±0.6
3.1±0.5 Disability
scale (EDSS)
0.06 3548.1±1542
3900.1±1658 4707±1918
4223±2084 BDNF
(pg/ml)
0.34 607±158.8
646.3±132.3 679.4±104
698.9±128 NGF (pg/ml)
0.17 2317.2±524.2
2227.7±413 2077.8±502.8
2356.5±778.9 VDBP
(ug/ml)
*significant difference with the control group at significance level 0.05
4. Discussion
There is a lack of therapeutic strategies for progressive multiple sclerosis patients with a higher and average grade of disability and substantial neurodegeneration and axonal dysfunction, which are of utmost clinical need. The clinical data obtained in recent studies indicate that exercise might have positive effects on neurocognitive functions in patients with progressive multiple sclerosis; however, the underlying molecular pathways and quantifiable markers are currently missing [34].
In the present study, the potential effects of combined exercise training on previously proposed serum biomarkers as possible underlying mediators were examined in a
cohort of progressive MS patients. The results obtained in the present study suggested that 12 weeks of combined exercise training (two sessions of aerobic training and one session of resistance training in a week) could lead to a significate improvement of the body fat percentage and disability scale in women with MS. However, the exercise training had no significant effects on the body weight and the biochemical variables (BDNF, NGF, VDBP).
82 International Journal of Applied Exercise Physiology www.ijaep.com
of changes triggered by physical activities. However, some researchers have studied the effect of aerobic and resistance training separately, with few of them investigating the effect of the combined exercise training. Moreover, few researchers have examined the biochemical factors while studying MS, and the changes resulting from training. Thus, more research studies on the effects of physical activities, especially the combined exercise training, on the biochemical variables are needed for a deeper understanding of MS and how it can be controlled. Schulz et al(2004) showed that 8 weeks of bicycling brought about no significant changes in BDNF and NGF levels in patients with MS[28]. However, Gold et al (2003) showed that bicycling for 30 minutes, an activity which consumed 60% of maximum oxygen, resulted in an increased NGF but no change in BDNF[ 29]. Similarly, the results of the study by Bansi et al (2013) revealed that BDNF level in patients with MS increased significantly after 3 weeks of aerobic training in that such training consumed 60% of maximum oxygen. The results of their study suggested that NGF levels tend to increase [30]. However, Castellano and White (2008) claimed that, after 4 weeks of exercise training with 65% of aerobic capacity, MS patients showed an increase in BDNF level, however, after 8 weeks, it returned to the initial level[31]. Wens et al (2016) observed an increased concentration of BDNF after 24 weeks of aerobic-resistance training [27]. Briken et al (2016) showed that bicycling for 30 minutes resulted in a significant increase of BDNF level in patients with progressive MS, but after 22 sessions, there were observed no changes in BDNF levels [32]. The results of the present study showed that a course of combined exercise training triggered no significant changes in neurotrophic factors and VDBP, a finding which is in line with the results obtained by Schulz et al(2004), Briken et al (2016), and to some extent, with those reported by Gold et al(2003). However, the results of the present study
are congruent with those obtained by Castellano and White(2008), Bansi et al (2012), and Wens et al(2016). This lack of congruence can be partly accounted for by the difference in the subjects' disability scales in pre-test, the difference in initial levels of BDNF and NGF, and the difference in the type and the duration (durance) of training. In fact, training in and by itself cannot trigger changes in the serum levels in neurotrophics; it is the intensity of training that plays an important role[35]. Oliff et al(1998) reported that exercise training had no effect on gene expressions of BDNF and NGF as long as they did not have enough threshold intensity[36].Therefore, it seems that the exercise training in this study did not have enough load. Although, in the present study, the BDNF level induced, to some extent, a significant increase, the load of training was not high enough to produce significant effects on the variables.
83 International Journal of Applied Exercise Physiology www.ijaep.com
Resistance and endurance training, multiple sclerosis VOL. 7 (1)
study, no changes were observed in VDBP level, a finding which is not in line with the results obtained by Waschbisch et al (2012) who reported a positive relationship between fitness level and serum level of vitamin D [40].However, there is no training program in this study and the level of vitamin D is estimated rather than VDBP level, but apparently this is the only study focusing on this variable. Generally, brain is a complex system that may be affected by various environmental factors or drug treatment [31]. Alternatively, the fact that no significant changes in these variables were observed in this study can be partly the result of the medications taken by the patients.
5. Conclusion
In summary, the provision of exercise training including aerobic and resistance training for three non-consecutive days in a week can improve the disability and the percentage of body fat in women with MS. Therefore, it seems advisable for doctors and specialists to encourage their patients with MS to receive such training sessions in order to improve their recovery chance.
However, it was shown that such exercise training for 12 weeks had no significant changes in the levels of biochemical factors BDNF, NGF and VDBP).
Limitations of this research are composed of the lack of control of genetic status, sleep, the nutrition of participants, and their motivation to participate in exercises. In general, differences in the results from the scientific background and the present study may be due to such differences including the type of MS, the initial level of EDSS, the number of paricipants, the length of the training duration, the different kind of training program, the volume and intensity of exercise. It seems that according to the types of MS and the use of training groups based on the type of disease can be obtained for these patients in more accurate and practical results.
Acknowledgements
We thank the laboratory of doctor SEZAVAR and RAZI University for supporting this research.
Reference
1. Dendrou CA, Fugger L, Friese MA. Immunopathology of multiple sclerosis. Nat Rev Immunol,
2015. 15(9): 545–58.
2. American College of Sports Medicine. ACSM’s resource manual for guidelines for exercise
testing and prescription. 7th edn. Philadelphia, PA: Lippincott Williams & Wilkins, 2013.
3. Dalgas U, Stenager E, Ingemann– Hansen T. Multiple sclerosis and physical exercise:
Recommendations for the application of ressistance- endurance and combined training. Mult
sclera J, 2008. 14(1): 35-53.
4. Motl RW, Learmonth YC, Pilutti LA, Gappmaier E, Coote S. Top 10 research questions related
to physical activity and multiple sclerosis. Res Q Exerc Sport, 2015. 86(2): 117–29.
5. Bekinschtien P, Cammarota M, Katche C, Slipczuk L, Rossato J, Goldin A, Izquierdo I. BDNF
is essential to promote persistence of long – tern memory storage. Proc. Natil. Acad. Sci. USA,
2008. 105(7): 2711-6.
6. Aloe L, Rocco M, Bianchi P, Manni L. Nerve growth factor: from the early discoveries to the
84 International Journal of Applied Exercise Physiology www.ijaep.com
7. Hayes CE, Cantorna MT, DeLuca HF. Vitamin D and multiple sclerosis. Proc Soc Exp Biol
Med, 1997. 216(1): 21–27.
8. Ascherio A, Munger KL, Simon KC. Vitamin D and multiple sclerosis. Lancet Neurol, 2010.
9(6): 599–612.
9. Munger KL, Levin LI, Hollis BW. Serum 25-hydroxyvitamin D levels and risk of multiple
sclerosis. JAMA, 2006. 296(23): 2832–2838.
10. Smolders J, Menheere P, Kessels A. Association of vitamin D metabolite levels with relapse
rate and disability in multiple sclerosis. Mult Scler, 2008. 14(9): 1220–1224.
11. Disanto G, Ramagopalan V, Para A, Handunnetthi L. The emerging role of vitamin D binding
protein in multiple. Sclerosis Neurol J, 2011. 258(3): 353–358.
12. Lehmensiek V, Sussmuth SD, Tauscher G. Cerebrospinal fluid proteome profile in multiple
sclerosis. Mult Scler, 2007. 13(7): 840–849.
13. Qin Z, Qin Y, Liu S. Alteration of DBP levels in CSF of patients with MS by proteomics analysis.
Cell Mol Neurobiol, 2009. 29(2): 203–210.
14. Van Praag H, Shubert T, Zhao C, Gage F.H. Exercise enhances learning and hippocampal
neurogenesis in aged mice. J. Neurosci, 2005. 25(38): 8680–8685.
15. Cotman CW, Berchtold NC, Christie LA. Exercise builds brain health: key roles of growth
factor cascades and inflammation. Trends Neurosci, 2007. 30(9): 464–472.
16. Petzinger GM, Fisher BE, McEwen S, Beeler JA, Walsh JP, Jakowec MW. Exercise- enhanced
neuroplasticity targeting motor and cognitive circuitry in Parkinson's disease. Lancet Neurol,
2013. 12(7): 716–726.
17. de Andrade LP, Gobbi LT, Coelho FG, Christofoletti G, Costa J.L.R, Stella F. Benefits of
multimodal exercise intervention for postural control and frontal cognitive functions in
individuals with Alzheimer's disease: a controlled trial. J. Am. Geriatr. Soc, 2013. 61(11):
1919–1926.
18. Kj ّlhede T, Vissing K, Dalgas U. Multiple sclerosis and progressive resistance training: a
systematic review. Mult Scler, 2012. 18(9): 1215–28.
19. Langeskov-Christensen M, Heine M, Kwakkel G, Dalgas U. Aerobic capacity in persons with
multiple sclerosis: a systematic review and meta-analysis. Sports Med, 2015. 45(6): 905–23.
20. Platta M, Pilutti LA, Ensari E, Motl RW. The effect of exercise training on fitness in multiple
sclerosis: a meta-analysis. Arch Phys Med Rehabil, 2016. 97(9): 1564–72.
21. Bayer Shrink Farma. Introduction to multiple sclerosis. Translated to Persian by: Company
Bayer Farma Shrink Office. Tehran: Jalal pub, 2010.
22. Dalgas E, Stenager J, Jakobsen T. Fatigue, mood and quality of life improve in MS patients after
progressive resistance training. Mult Scler, 2010. 16(4): 480-490.
23. Cakt BD, Nacir B, Genc H. Cycling progressive resistance training for people with multiple
sclerosis: a randomized controlled study. Am J Phys Med Rehabil, 2010. 89(6): 446-57.
24. Van den berg M, Dawas H, Wade DT, Newman M, Burridge J, Izadi H. Treadmill training for
individuals with multiple sclerosis:a pilot randomized trial. J Neursung Psychiatry, 2006.
85 International Journal of Applied Exercise Physiology www.ijaep.com
Resistance and endurance training, multiple sclerosis VOL. 7 (1)
25. Pilutti LA, Lelli DA, Paulseth JE. Effects of 12 weeks of supported treadmill training on
functional ability and quality of life in progressive multiple sclerosis: a pilot study. Arch Phys
Med Rehabil, 2011. 92(1): 31-6.
26. Romberg A, Virtanen A, Ruutiainen J, Aunola S, Karppi S. Effect of a 6- month exercise
program on patients with Multiple Sclerosis. Neurology, 2004. 63(11): 2034- 2038.
27. Wens C, Keytsman N, Deckx N, Cools N, Dalgas U, Eijnde B.O. Brain derived neurotrophic
factor in multiple sclerosis: effect of 24 weeks endurance and resistance training. European
Journal of Neurology, 2016. 23(6): 1028–1035.
28. Schulz KH, Gold SM, Witte J. Impact of aerobic training on immune-endocrine rametrers,
neurotophic factors, quality of life and coordinative function in multiple sclerosis. J Neurol Sci,
2004. 225(1-2): 8-11.
29. Gold SM, Schulz KH, Hartmann S, Mladek M, Hellweg R. Basal serum levels and reactivity of
nerve growth factor and brain-derived. Journal of Neuroimmunology, 2003. 138(1-2): 99– 105.
30. Bansi J, Bloch W, Gamper U. Training in MS: influence of two different endurance training
protocols(aquatic versus overland) on cytokine and neurotrophin concentrations during three
week. randomized controlled trial. Multiple Sclerosis Journal, 2012. 1–9.
31. Castellano V, White LJ. Serum brain-derived neurotrophic factor response to aerobic exercise
in multiple sclerosis. J Neurol Sci, 2008. 269(1-2): 85-91.
32. Briken S, Rosenkranz S, Keminer O, Patra S, Ketels G, Heesen C, Hellweg R. Effects of exercise
on Irisin, BDNF and IL-6 serum levels in patients with progressive multiple sclerosis. Journal
of Neuroimmunology, 2016. 299: 53–58.
33. Polman CH, Reingold SC, Banwell B, Clanet M, Cohen JA, Filippi K… , Wolinsky JS.
Diagnostic criteria for multiplesclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol,
2011. 69(2): 292–302.
34. Fischer A, Heesen C, Gold S.M. Biological outcome measurements for behavioral interventions
in multiple sclerosis. Ther. Adv. Neurol. Disord, 2011. 4(4): 217–229.
35. Oken B, Kishiyama M, Zajdel D, Bourdette D, Carlsen J. Randomized controlled trial of yoga
and exercise in multiple sclerosis. Neurol, 2004. 62(11): 2058-2064.
36. Oliff HS, Berchtold NC, Isackson P. Exercise-induced regulation of brain-derived neurotrophic
factor(BDNF) transcripts in the rat hippocampus. Brain Res Mol Brain Res, 1998. 61(1-2):
147-153.
37. Sarichielli P, Greco L, Stipa A, Floridi A, Gallai V. Brain-derived neurotrophic factor in
patients with multiple sclerosis. J Neuroimmunol, 2002. 132(1-2): 180– 188.
38. Heyman E, Gamelin FX, Goekint M, Piscitelli F, Roelands B. Intense exercise increases
circulating endocannabinoid and BDNF levels in humans–possible implications for reward and
depression. Psychoneuroendocrinology, 2012. 37(6): 844–851.
39. Panab W, Banksc WA, Fasolda MB, Blutha J. Transport of brain-derived neurotrophic factor
86 International Journal of Applied Exercise Physiology www.ijaep.com
40. Waschbisch A, Wenny I, Tallner A, Schwab S, Pfeifer K, Mäurer M. Physical activity in
multiple sclerosis: a comparative study of vitamin d, brain-derived neurotrophic factor and