Descriptive Analysis of Patient Sexual Identity and Trust in the Doctor-Patient Relationship
By Claire Couch
Senior Honors Thesis Department of Sociology
University of North Carolina at Chapel Hill April 3, 2017
Approved:
Liana Richardson, Thesis Advisor
TABLE OF CONTENTS
Abstract 2
Introduction 3
Literature Review 4
Methods 9
Results 11
Discussion 13
ABSTRACT
Previous research has identified a strong link between patients’ social characteristics and health care disparities, and attributed it largely to distrust within the doctor-patient relationship. However, this research has focused almost exclusively on patients’ race and gender, while ignoring other aspects of their identity that may also influence the clinical encounter, such as sexual identity. Even less research has focused on whether sexual identity could affect trust in the doctor-patient relationship and, specifically, whether sexual minorities feel less trust in their physicians than individuals who identify as heterosexual. To fill this gap, I assessed the
INTRODUCTION
There is a substantial body of literature on doctor-patient interactions, and much of this literature focuses on the experiences of patients, such as whether they trust their physicians. This focus has also characterized research on health care disparities, due to growing concerns about the significant inequalities in quality of care by race/ethnicity and gender. This research has led to the well-accepted finding that these social characteristics influence the clinical encounter and its outcomes, including patients’ trust in their physician (Banerjee and Sanyal 2012; Boulware et al. 2003; Doescher et al. 2000; Halbert et al. 2006; Wiltshire, Person, and Allison 2011).
It is reasonable to suspect that patient trust may also be associated with other social characteristics, such as the sexual identity, of the patient. However, there is a definite lack of research on this relationship. This gap is potentially consequential for sexual minority
populations because they have higher rates of risky health-related behaviors, such as cigarette smoking and low health care utilization, and an increased risk of a variety of health issues, such as certain cancers and STIs (IOM LGBT Health Report 2011; Lesbian, Gay Bisexual, and Transgender Health 2010; Mayer et al. 2008; National Health Statistics Report 2014). Regular health care and presumably trustworthy doctors are critical for this population. If sexual identity and trust are associated with each other, such that sexual minorities are less likely to trust their physicians than others, then this group may be less likely to adhere to their physicians’
recommendations, which may hasten the degradation of their health.
three reasons: negative implicit biases towards sexual minority patients by physicians; lack of education, experience, and cultural competence regarding sexual minority patients among
physicians; and/or sexual minority patients’ expectations of experiencing discrimination, whether physicians actually discriminate against them or not. Despite the plausibility of these
mechanisms, I found no significant association between patients’ sexual identity and trust in bivariate descriptive analyses of data from the HIV Cost and Services Utilization Study (HCSUS).
LITERATURE REVIEW
In light of persistent racial and gender disparities in health care utilization and outcomes, differences in patient trust based on race and gender have been studied extensively (Banerjee and Sanyal 2012; Boulware et al. 2003; Doescher et al. 2000; Halbert et al. 2006; Wiltshire, Person, and Allison 2011), and the connections between these social characteristics and patient trust have been well-established. Differences in patient trust by other indicators of identity, such as sexual identity, have been less well researched. As a result, we know little about the extent of trust that individuals in the LGBT community have in their physicians. This gap is potentially
National Health Statistics Report 2014). However, sexual minorities have low rates of
healthcare utilization (Mayer et al. 2008; National Health Statistics Report 2014). For those that do utilize health care, trusting their physicians will increase the likelihood that they adhere to physicians’ treatment recommendations, which can lead to improved health outcomes.
Scholars have found that certain social characteristics of the patient and the physician may have an impact on the quality of the doctor-patient relationship, including the development or perpetuation of distrust among patients (van Ryn 2002). Research on racial and gender differences in the doctor-patient relationship suggests three possible explanations for why we might also expect to find high levels of distrust among sexual minorities as well. First, physicians may have implicit biases or conscious discriminatory attitudes towards sexual minorities that negatively influence their communication and behavior during the clinical encounter and, in turn, undermine the development of trust among their patients. Second, physicians may feel uncomfortable with sexual minority patients because of a lack of education and clinical experience with this population, and this discomfort may be visible enough to undermine the development of trust among their patients. Third, patients may also bring an expectation of stigma based on their self-identification as sexual minorities into the clinical encounter; this expectation whether met or unmet by their physicians could make it more difficult for patients to develop trust in the first place.
Stereotype Application in the Doctor-Patient Relationship
application (van Ryn 2002). Scholars have argued that physicians can unintentionally allow stereotypes or beliefs about patients’ social characteristics to influence their behavior and decision-making throughout different aspects of the clinical encounter, including the interview and diagnosis. This affects how symptoms are interpreted, how a diagnosis is arrived at, and how a treatment plan is constructed and implemented (van Ryn 2002). The stereotypes or beliefs are often guided by how physicians identify, or categorize, themselves because people can hold preferences toward others who they perceive to identify concordantly (LaVeist and Nuru-Jeter 2002; Schmittdiel et al. 2000; Street et al. 2008). Indeed, healthcare providers have been shown to demonstrate implicit preference for patients whose sexual identity is concordant with their own through “in-group” favoritism (Sabin, Riskind, and Nosek 2015). This may explain why Elliot et al. (2015) found that sexual minorities in England were one and a half times more likely to report negative healthcare experiences at their local general practice compared with
heterosexual patients. Although I do not test for the mediation of the relationship between sexual identity and trust by discrimination in the present study, it may offer an explanation as to why patients who identify as sexual minorities report feeling a lack of trust in their providers. Culturally (In)competent Care
racial/ethnic minorities (Betancourt et al. 2003; Johnson et al. 2004). Poteat et al. (2013), for example, found that a lack of education on caring for transgender patients created uncertainty for the physician in the clinical encounter, which undermined their authority, and that discrimination served as a power play for physicians to reassert their authority in the traditional doctor-patient hierarchical relationship. The curriculum in medical and nursing schools on how to care for sexual minorities is quite limited, which undermines students’ ability to comprehensively care for these patients (Lim, Brown, and Justin Kim 2014). Without clinical experience, physicians also are unable to apply evidence-based practices. Sexual minority populations have reported having to teach their physicians about how to provide them with medical care (Butler et al. 2016; Lim, Brown, and Justin Kim 2014; Poteat, German, and Kerrigan 2013). The absent curriculum on sexual minorities during medical training facilitates the discrimination that could explain why sexual minorities experience distrust in their physician.
Expectations of Discrimination among LGBT Patients
Beyond the direct actions of the physician, patients might also allow their own fears and beliefs based on their experience of stigmatization in other social situations to shape the doctor-patient relationship in the clinical encounter. Personal identification as a member of a
privacy concerns, and fear of discrimination may deter sexual minority patients from disclosing information about their sexual identity to their physician, which could have significant relevance to their health care needs (Cahill and Makadon 2013; Gonser 2000), or from even maintaining routine health care visits at all. In fact, one of the most significant risk factors for the health of sexual minorities is their general avoidance of routine care (Gonser 2000). These expectations and fears are similar to those described in research on racism-related vigilance among Blacks. Blacks have demonstrated that they constantly prepare themselves through anticipation and avoidance (Hicken et al. 2013). As a marginalized group that is discriminated against, sexual minorities can reasonably be expected to harbor similar anticipatory behaviors, even in health care interactions. Thus, expectations of discrimination among sexual minority patients may undermine patients’ ability to trust their physician, regardless of physicians’ actual behavior and attitudes towards them.
The Present Study
These explanations for why a sexual minority may feel a lack of trust in the doctor-patient relationship compared with non-minorities are not mutually exclusive. The extent of stereotype application by physicians, cultural competency regarding sexual minorities among physicians, and patients’ expectations of discrimination all contribute to the doctor-patient interaction and to the formation of a trusting or distrusting relationship between patient and physician. These potential contributions provide strong rationale for hypothesizing that reports of distrust will be higher among sexual minorities compared with those who identify as
METHODS Data
Data for the study come from the HIV Cost and Services Utilization Study (HCSUS). HCSUS was a nationally representative, longitudinal survey of adults receiving care for HIV-infection at a non-military, non-prison, non-emergency medical provider between January 5 and February 29, 1996. The study consisted of a baseline survey with two follow-up surveys. A total of 4402 patients were sampled from 28 metropolitan areas and 24 rural areas. The 2864 successful baseline interviews were conducted using computer-assisted personal interviewing instruments (Shapiro et al. 1999; Frankel et al. 1999).
Respondents who were missing data or responded “don’t know,” “other,” or “refused” for any item were excluded from the analysis, with the exception of the sexual identity variable in which case respondents who selected “don’t know” or “other” in response to the sexual identity item were retained. The vast majority of excluded respondents (n = 2161) were excluded because they were skipped out of the item used for the dependent variable of this study. (The logic for this skip is not available in the documentation for the HCSUS survey.) As a result, the analytic sample for this study is comprised of the 676 participants who had complete data for all study variables.
Dependent Variables
There is no consistent definition of patient trust, but this study used one of the core tenets of most definitions (Barefoot et al.1998; Hillman 1998; Mechanic and Schlesinger 1996;
baseline survey to evaluate respondents’ level of trust in their health care provider. Respondents reported how much they trusted their provider to put their health above all other concerns on a 5-point scale (1 = completely to 5 = not at all). On a 4-5-point scale (1 = strongly agree to 4 = strongly disagree), respondents also indicated how much they believed it better to trust a health care provider than to question them and if they would rather have their provider make decisions for them instead of giving them a lot of options.
Independent Variable
Sexual identity was measured as a dichotomous variable based on responses to the sexual orientation item of the questionnaire (coded as 1 for sexual minority (gay/lesbian, bisexual, celibate/asexual, transsexual, in transit, other, and don’t know) and 2 for heterosexual). Covariates
To determine whether the relationship between sexual identity and trust varies by other markers of identity, measures of race and gender were also included in the analysis for this study. The race measure was a trichotomous variable that classified respondents as white, black/African American, or Hispanic. The gender measure was respondents’ self-identification as male or female.
Analysis
RESULTS Sample Description
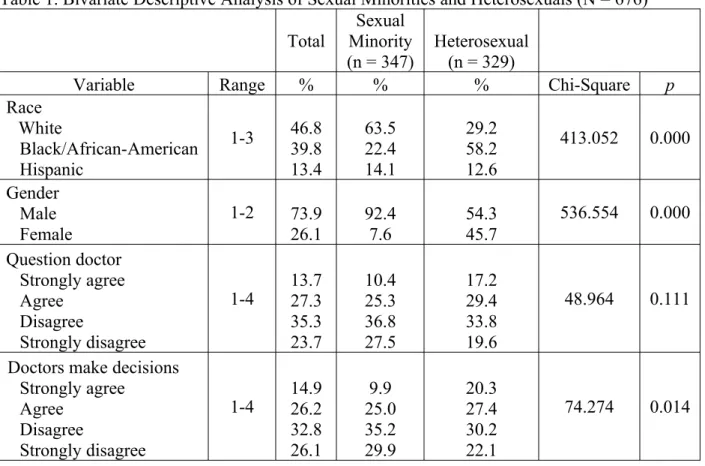
Of the 676 respondents in the sample, about 51% identified as a sexual minority and 49% identified as heterosexual. The sample was about 47% white, 40% black/African-American, and 13% Hispanic. The majority of sexual minorities (63.5%) were white, while most heterosexuals (58.2%) were black/African-American. With the total sample about 74% male, men constituted the majority of both sexual minorities (92.4%) and heterosexuals (54.3%).
When asked whether it is better to trust a doctor than to question their actions and whether they would rather have doctors make decisions for them rather than have a lot of
choices, the majority of respondents (59% and 58.9%, respectively) indicated that they disagreed to some degree with these statements. The majority of respondents (80%) also indicated a lack of trust when asked if they trust their doctor to make their health a top concern, with responses of “somewhat,” “a little,” or “not at all.”
Bivariate Relationships
Results of bivariate analyses comparing the distributions of study variables across the two sexual identity categories are also provided in Table 1. The chi-square tests revealed a
statistically significant association between race and sexual identity, and between gender and sexual identity. Sexual minority status was more correlated with being white and being male than heterosexual status was; heterosexuals were more likely to be a racial minority.
The distribution across response options for whether the patient trusted their doctor to make their health a top concern was proportionally similar for sexual minorities and
that there is no statistically significant relationship (χ2 = 41.607, p > .05). Similarly, no
statistically significant difference between the sexual identity groups was found regarding their opinion about trusting rather than questioning their doctor’s actions (χ2 = 48.964, p > .05). On
the other hand, a statistically significant difference between sexual identity groups was found regarding their preference for having health care professionals make decisions for them (χ2 =
74.274, p < .05). Specifically, about 48% of heterosexuals agreed with the statement, “I’d rather have doctors and nurses make decisions about what’s best rather than for them to me give a lot of choices,” while only 35% of sexual minorities agreed with it.
Table 1. Bivariate Descriptive Analysis of Sexual Minorities and Heterosexuals (N = 676) Total
Sexual Minority
(n = 347) Heterosexual(n = 329)
Variable Range % % % Chi-Square p
Race White Black/African-American Hispanic 1-3 46.8 39.8 13.4 63.5 22.4 14.1 29.2 58.2 12.6 413.052 0.000 Gender Male Female 1-2 73.9 26.1 92.4 7.6 54.3 45.7 536.554 0.000 Question doctor Strongly agree Agree Disagree Strongly disagree
1-4 13.727.3 35.3 23.7 10.4 25.3 36.8 27.5 17.2 29.4 33.8 19.6 48.964 0.111
Doctors make decisions Strongly agree
Agree Disagree
Strongly disagree
Make health top concern Completely
Mostly Somewhat A little Not at all
1-5 6.7 13.3 21.5 28.6 29.9 5.8 10.8 19.2 31.6 32.6 7.6 15.8 24.1 25.4 27.1 41.607 0.132 DISCUSSION
The goal of this study was to determine whether patient sexual identity is associated with patient trust—defined as feeling that the physician will put their health above all other concerns —in the doctor-patient relationship. I hypothesized a disparity between sexual minorities and heterosexuals in their levels of trust based on three theoretical premises—physician bias against sexual minorities, physician inexperience and consequent discomfort with sexual minorities, and patient expectations of discrimination—generated from related literature on racial/ethnic
differences in the doctor-patient relationship. While my analysis did not reveal significant differences between sexual minorities and heterosexuals, the majority of people in the sample indicated a low level of trust in their physician, regardless of their sexual identity. These findings may not be surprising when considering the study population and historical context of the data, i.e., an HIV positive population in the 1990s. At the time the HCSUS data were being collected, HIV was highly stigmatized due to concerns regarding the transmission of the disease and efficacy of treatment (Crawford 1996; Lee, Kochman, and Sikkenma 2002; Valdiserri 2002). These factors could have resulted in high levels of distrust amongst anyone infected with HIV, with very little variability across sexual identity groups.
Limitations
trust their doctor to make decisions for them rather than have a lot of choices) could be indicators of other factors, such as an inclination to challenge authority. If patients were likely to challenge authority, they might disagree with these statements in a similar way to if they distrusted their physician. Younger patients are more inclined to have a negative response to the authority of their physician (Pescosolido, Tuch, and Martin 2001). The ages of the patients participating in the HCSUS survey were removed to protect their identities, so while there is no way to know for sure, this could be a contributing factor. An increasingly more consumerist view of medicine that results in patients becoming more likely to question their physician and challenge the traditional power dynamic within the doctor-patient relationship could also explain these results (Pescosolido, Tuch, and Martin 2001). Second, the sexual identity variable conflated sexual orientation and gender. Specifically, two of the response categories for this item (i.e.,
transsexual and in transit) are actually indicative of gender identity. While less than one percent of the sample identified with each of these categories, it may have created confusion for those and other respondents whose gender and sexual identities are not aligned. This circumstance may also have impacted responses to the gender item.
The age of the HCSUS data, collected about twenty years ago, also presents a
considerable limitation because it runs the risk of making the results inapplicable to the current population of HIV-positive people. Additionally, utilizing data that is confined solely to an HIV patient population reduces the applicability to a larger population of sexual minorities without HIV due to the layers of stigma associated with both identities.
Future Research and Practice Implications
Despite these limitations, the study results have implications for the clinical encounter. Health disparities that affect the sexual minority population have been recognized by the Institute of Medicine and the Healthy People 2020 initiative, and both advocate for training healthcare providers on LGBT health to understand and improve the disparities that exist for this population (IOM LGBT Health Report 2011; Lesbian, Gay Bisexual, and Transgender Health 2010). Expansion of the medical education of student doctors to incorporate a greater focus on how to care for marginalized populations, including HIV patients, would be a logical approach for addressing the significant feelings of distrust found in this sample.
The limitations presented by the HCSUS dataset and other similar datasets offer
and outside the medical community has decreased since the 1990s (Valdiserri 2002). Surveying the current population of those living with HIV may reveal differences or confirm similar feelings of distrust in their physician as compared with the 1990s. Also, including data from the viewpoint of both the patient and the physician would offer a more complete understanding of the clinical encounter. This would provide insight to the motivations behind the behaviors of the physician that may have contributed to the feelings of distrust evidenced in these patients.
Although these descriptive results suggest that sexual identity may not be related to trust in the doctor-patient relationship, more advanced regression approaches, such as a multivariate ordinal regression, would offer a more comprehensive analysis of the two variables. A
multivariate analysis would allow adjustment for other covariates, such as race, gender, or socioeconomic status that may influence the link between sexual identity and trust. It may also reveal factor(s) that are suppressing the relationship between patient sexual identity and trust. The descriptive analysis indicated that sexual minorities were significantly associated with being white and male, so race and gender would be relevant control variables for a multivariate
regression analysis. With the trust variables used in this study being on Likert-type scales, an ordinal regression would retain information about the ordering of the response categories. Conclusion
My study revealed that trust, while not significantly associated with sexual identity, was considerably low for this sample. This is especially relevant for the maintenance of health and treatment regimens of HIV patients where trust is key factor. Specifically, HIV patients have a poorer health status due to their chronic disease, and treatment adherence and regular healthcare utilization is vital for maintaining better health and preventing the development of AIDS.
Mostashari, and Friedland 2001; Blackstock et al. 2012; Roberts 2002; Vanable et al. 2006). Therefore, it is essential to replicate these results on the current HIV population and improve the lack of trust within the doctor-patient relationship demonstrated here.
REFERENCES
Altice, Frederick L., Farzad Mostashari, and Gerald H. Friedland. 2001. “Trust and the Acceptance of and Adherence to Antiretroviral Therapy.” JAIDS Journal of Acquired Immune Deficiency Syndromes 28(1):47–58.
Anon. n.d. “IOM LGBT Health Report | The Fenway Institute.” Retrieved November 6, 2016a (http://thefenwayinstitute.org/research/iom-report/).
Anon. n.d. “Lesbian, Gay, Bisexual, and Transgender Health | Healthy People 2020.” Retrieved November 6, 2016b
(https://www.healthypeople.gov/2020/topics-objectives/topic/lesbian-gay-bisexual-and-transgender-health).
Anon. n.d. “National Health Statistics Report (Number 77 - July 15, 2014)—Sexual Orientation and Health Among U.S. Adults: National Health Interview Survey - nhsr077.pdf.” Retrieved November 5, 2016c (https://www.cdc.gov/nchs/data/nhsr/nhsr077.pdf).
Banerjee, Amitav and Debmitra Sanyal. 2012. “Dynamics of Doctor-Patient Relationship: A Cross-Sectional Study on Concordance, Trust, and Patient Enablement.” Journal of Family and Community Medicine 19(1):12.
Betancourt, Joseph R., Alexander R. Green, J.Emilio Carrillo, and Owusu Ananeh-Firempong. 2003. “Defining Cultural Competence: A Practical Framework for Addressing
Racial/Ethnic Disparities in Health and Health Care.” Public Health Reports 118(4):293– 302.
Blackstock, Oni J., Dianne N. Addison, Jennifer S. Brennan, and Oladipo A. Alao. 2012. “Trust in Primary Care Providers and Antiretroviral Adherence in an Urban HIV Clinic.” Journal of Health Care for the Poor and Underserved 23(1):88–98.
Boulware, L.Ebony, Lisa A. Cooper, Lloyd E. Ratner, Thomas A. LaVeist, and Neil R. Powe. 2003. “Race and Trust in the Health Care System.” Public Health Reports 118(4):358– 65.
Butler, Mary et al. 2016. Improving Cultural Competence to Reduce Health Disparities. Rockville (MD): Agency for Healthcare Research and Quality (US). Retrieved October 30, 2016 (http://www.ncbi.nlm.nih.gov/books/NBK361126/).
Cahill, Sean and Harvey Makadon. 2013. “Sexual Orientation and Gender Identity Data
Collection in Clinical Settings and in Electronic Health Records: A Key to Ending LGBT Health Disparities.” LGBT Health 1(1):34–41.
Crawford, Anne M. 1996. “Stigma Associated With AIDS: A Meta-Analysis1.” Journal of Applied Social Psychology 26(5):398–416.
Elliott, Marc N. et al. 2015. “Sexual Minorities in England Have Poorer Health and Worse Health Care Experiences: A National Survey.” Journal of General Internal Medicine 30(1):9–16.
Frankel, M. R. et al. 1999. “National Probability Samples in Studies of Low-Prevalence Diseases. Part II: Designing and Implementing the HIV Cost and Services Utilization Study Sample.” Health Services Research 34(5 Pt 1):969.
Gonser, Patricia A. 2000. “Culturally Competent Care for Members of Sexual Minorities.” Journal of Cultural Diversity 7(3):72–75.
Gonzales, Gilbert, Julia Przedworski, and Carrie Henning-Smith. 2016. “Comparison of Health and Health Risk Factors Between Lesbian, Gay, and Bisexual Adults and Heterosexual Adults in the United States: Results From the National Health Interview Survey.” JAMA Internal Medicine 176(9):1344–51.
Halbert, Chanita Hughes, Katrina Armstrong, Oscar H. Gandy, and Lee Shaker. 2006. “Racial Differences in Trust in Health Care Providers.” Archives of Internal Medicine
166(8):896–901.
Hicken, Margaret T., Hedwig Lee, Jeffrey Morenoff, James S. House, and David R. Williams. 2014. “Racial/Ethnic Disparities in Hypertension Prevalence: Reconsidering the Role of Chronic Stress.” American Journal of Public Health; Washington 104(1):117–23.
Hillman, Alan L. 1998. “Mediators of Patient Trust.” JAMA 280(19):1703–4.
Race/Ethnicity and Quality of Patient–Physician Communication During Medical Visits.” American Journal of Public Health 94(12):2084–90.
LaVeist, Thomas A. and Amani Nuru-Jeter. 2002. “Is Doctor-Patient Race Concordance
Associated with Greater Satisfaction with Care?” Journal of Health and Social Behavior 43(3):296–306.
Lee, Rachel S., Arlene Kochman, and Kathleen J. Sikkema. 2002. “Internalized Stigma Among People Living with HIV-AIDS.” AIDS and Behavior 6(4):309–19.
Lim, Fidelindo A., Donald V. Brown, and Sung Min Justin Kim. 2014. “CE: Addressing Health Care Disparities in the Lesbian, Gay, Bisexual, and Transgender Population.” AJN, American Journal of Nursing 114(6):24–34.
Mansh, Matthew, Gabriel Garcia, and Mitchell R. Lunn. 2015. “From Patients to Providers: Changing the Culture in Medicine Toward Sexual and Gender Minorities.” Academic Medicine 90(5):574–80.
Mayer, Kenneth H. et al. 2008. “Sexual and Gender Minority Health: What We Know and What Needs to Be Done.” American Journal of Public Health 98(6):989–995.
Mechanic, David and Mark Schlesinger. 1996. “The Impact of Managed Care on Patients’ Trust in Medical Care and Their Physicians.” JAMA 275(21):1693–97.
Meyer, Ilan H. 2003. “Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence.” Psychological Bulletin
Newcomer, Lee N. 1997. “Measures of Trust in Health Care.” Health Affairs; Chevy Chase 16(1):50–51.
Pearson, Steven D. and Lisa H. Raeke. 2000. “Patients’ Trust in Physicians: Many Theories, Few Measures, and Little Data.” Journal of General Internal Medicine 15(7):509–13.
Pescosolido, Bernice A., Steven A. Tuch, and Jack K. Martin. 2001. “The Profession of Medicine and the Public: Examining Americans’ Changing Confidence in Physician Authority from the Beginning of The’health Care Crisis’ to the Era of Health Care Reform.” Journal of Health and Social Behavior 1–16.
Poteat, Tonia, Danielle German, and Deanna Kerrigan. 2013. “Managing Uncertainty: A Grounded Theory of Stigma in Transgender Health Care Encounters.” Social Science & Medicine 84:22–29.
Roberts, Kathleen Johnston. 2002. “Physician-Patient Relationships, Patient Satisfaction, and Antiretroviral Medication Adherence among HIV-Infected Adults Attending a Public Health Clinic.” AIDS Patient Care and STDs 16(1):43–50.
van Ryn, M. 2002. “Research on the Provider Contribution to Race/Ethnicity Disparities in Medical Care.” Medical Care 40(1):140–51.
Sabin, Janice A., Rachel G. Riskind, and Brian A. Nosek. 2015. “Health Care Providers’ Implicit and Explicit Attitudes Toward Lesbian Women and Gay Men.” American Journal of Public Health 105(9):1831–41.
Physician and Patient Gender Concordance on Patient Satisfaction and Preventive Care Practices.” Journal of General Internal Medicine 15(11):761–69.
Shapiro, M. F. et al. 1999. “National Probability Samples in Studies of Low-Prevalence Diseases. Part I: Perspectives and Lessons from the HIV Cost and Services Utilization Study.” Health Services Research 34(5 Pt 1):951–68.
Street, R. L., K. J. O’Malley, L. A. Cooper, and P. Haidet. 2008. “Understanding Concordance in Patient-Physician Relationships: Personal and Ethnic Dimensions of Shared Identity.” The Annals of Family Medicine 6(3):198–205.
Valdiserri, Ronald O. 2002. HIV/AIDS Stigma: An Impediment to Public Health. American Public Health Association. Retrieved March 6, 2017
(http://ajph.aphapublications.org/doi/abs/10.2105/AJPH.92.3.341).
Vanable, Peter A., Michael P. Carey, Donald C. Blair, and Rae A. Littlewood. 2006. “Impact of Related Stigma on Health Behaviors and Psychological Adjustment among HIV-Positive Men and Women.” AIDS and Behavior 10(5):473–482.