Original Article
The relationship between angiotensin II type 1 receptor
gene A1166C polymorphism and cancer
risk: a meta-analysis
Zhiwei Liu, Mengwei Weng, Feng Dai, Ying Zhang, Shengjun Wu
Department of Clinical Laboratory, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou 310000, Zhejiang Province, People’s Republic of China
Received August 2, 2015; Accepted April 8, 2016; Epub June 15, 2016; Published June 30, 2016
Abstract: A number of studies have examined the association between angiotensin II type 1 receptor (AGTR1) gene A1166C polymorphism and risk of cancer but revealed in consistent results. The aim of this study was to clarify the association between AGTR1 gene A1166C polymorphism and risk of cancer. Databases including PubMed and
Embase databases were searched to find relevant studies. The odds ratio (OR) with corresponding 95% confidence intervals (CIs) was performed. A total of 7 case-control studies were finally identified. The results suggested that AGTR1 gene A1166C polymorphism was associated with a significantly decreased risk of cancer (Recessive model: OR=0.66, 95% CI 0.44-0.99). In stratified analysis by race, we also found that this polymorphism decreased cancer
risk in Caucasians and Breast cancer (BC). No publication bias was found in the present study. In conclusion, the
present meta-analysis suggests that the A1166C polymorphism in AGTR1 gene is associated with a significantly
decreased risk of cancer, especially in Caucasian population and BC. More studies with larger sample size, well controlled confounding factors are warranted to validate this association.
Keywords: Cancer, AGTR1 gene, genetic variant, meta-analysis
Introduction
The global burden of cancer continues to sig-nificantly increase with approximately 12.7 mil-lion cancer cases and 7.6 milmil-lion cancer deaths each year worldwide [1]. Despite considerable investigation, the causes are not yet fully under-stood. The classic risk factors include alcohol consumption, cigarette smoking, obesity, occu-pational exposures, family history of cancer and diet [2]. In addition, genetic factors also play important roles in the pathogenesis of can-cer [3]. Identification of a gene polymorphism that is associated with increased to risk of can-cer would greatly benefit the early prevention and cure for cancer.
The renin-angiotensin system (RAS) is a hor-monal signaling mechanism, which regulates is implicated in the regulation of blood pressure and cardiovascular homeostasis [4]. The pri-mary effector molecule of this system is angio-tensin II (ANG II) and is formed after two
cleav-converting enzyme Angiotensin Converting Enzyme (ACE). The physiological effects of ANG II are mediated mediates its physiological effects by two G protein-coupled receptors, namely the angiotensin Angiotensin II type 1 receptor Receptor (AGTR1) and the angiotensin Angiotensin II type 2 receptor Receptor (AGTR2) [5]. While AGTR1 is found in a wide variety of human normal tissues, its increased expres-sion is often found in the corresponding neo-plastic tissues, suggesting that its overexpres-sion is involved in carcinogenesis [6, 7]. Previous animal experiments in rat have shown that AGTR1 may play a role in the proliferation of tumor cells and vasculature development within the tumor tissue [8, 9]. In addition, sig-nificant attention has been paid to the block-ade of the RAS as a new approach to the treat-ment of cancer [10].
gene has been the most studied polymorphism of this gene, which consists of an AC nucleotide transversion at position 1166 (A1166C, rs51- 86). Previous meta-analyses demonstrated that the AGTR1 gene A1166C polymorphism was associated with susceptibility to coronary heart disease and hypertension [11, 12]. To date, several studies have investigated the relationship between AGTR1 gene A1166C polymorphism and cancer risk. But the results have been inconclusive, even conflictive. Meta-analysis can be a useful tool in detecting an association that could otherwise remain ma- sked in the sample size studies, especially in those evaluating rare allele frequency polymor-phisms [13]. To explore whether the AGTR1 gene A1166C polymorphism was associated with decreased risks of cancer, we performed a meta-analysis on the association between the AGTR1 gene A1166C polymorphism and cancer risk in the present study.
Materials and methods
Publication search
The search strategy for the association of AGTR1 AT1R gene A1166C polymorphism with
(c) the paper clearly described the sources of the cases and controls. Additionally, the follow-ing exclusion criteria were also used: (a) not case-control studies that evaluated the associ-ation between the AGTR1 gene A1166C poly-morphism and cancer risk; (b) case reports, let-ters, reviews, meta-analysis and editorial articles; (c) studies that were based on incom-plete raw data or no usable data reported and (d) duplicated publications.
Quality assessment
[image:2.612.91.350.83.376.2]The quality of these studies included in this analysis was also independently evaluated independently by the same two investigators according to the predefined quality assess-ment rules listed in Table 1. The criteria cover the representativeness of the cases, source of controls, ascertainment of ovarian cancer, total sample size, quality control of the genotyping methods, and Hardy-Weinberg equilibrium (HWE) in the control population. Disagreements were resolved by consensus. The total score ranged from 0 (worst) to 15 (best). Papers scor-ing <10 were classified as “low quality” and those scoring ≥10 as “high quality”.
Table 1. Scale for quality assessment
Criteria Score
Source of cases
Selected from population or cancer registry 3
Selected from hospital 2
Selected from pathology archives, but without description 1
Not described 0
Source of controls
Population-based 3
Blood donors or volunteers 2
Hospital-based (cancer-free patients) 1 1
Not described 0 0
Specimens of cases determining genotypes
White blood cells or normal tissues 3 Tumor tissues or exfoliated cells of tissue 0 Hardy-Weinberg equilibrium in controls
Hardy-Weinberg equilibrium 3
Hardy-Weinberg disequilibrium 0
Total sample size
≥1000 3
≥500 but <1000 2
≥200 but <500 1
>0 but <200 0
cancer risk was as follows. First, the relevant studies were sought in the electronic databases of PubMed and Embase databases on July 2015. The following key words were used as follows: (angiotensin II ty- pe-1 receptor) AND polymorphism AND (cancer) were entered into the aforementioned databases and the publication language was limited to the English language. If more than one article was published by the same author using the same case series, we selected the study where the most number of individuals were investigated.
Inclusion, exclusion criteria
Data extraction
Two investigators dependently reviewed the publications and obtained information accord-ing to a standard data form. For conflictaccord-ing eval-uations, an agreement was reached following a discussion. The following data were extracted from each study: first author, year of publica-tion, area, number of cases and controls, geno-type frequencies in cases and controls, and evidence of Hardy-Weinberg equilibrium (HWE) in controls.
Statistical analysis
The pooled OR with its corresponding 95% CI was calculated to assess the strength of the
association between AGTR1 gene A1166C polymorphism and cancer risk under a homozy-gote comparison (CC vs. AA), a heterozyhomozy-gote comparison (AC vs. AA), a dominant model (CC+AC vs. AA) and a recessive mode (CC vs. AC+AA) between groups. The variation pro-duced by heterogeneity was estimated by cal-culating the inconsistency index I2, with I2, 25%,
25-75% and 75% representing low, moderate or high degrees of inconsistency, respectively [14]. When the heterogeneity was absent I2<50%, the pooled OR estimates of each study
[image:3.612.93.522.75.525.2]were calculated using the fixed-effect model, specifically the Mantel-Haenszel method. Otherwise, a random-effect model, specifica- lly the Dersimonain and Laird method, was
Table 2. Characteristics of the included studies for meta-analysis Study Year Area Ethnicity Genotyping
methods of controlsource Cancer type ControlsCases/ Genotypes for cases for controlsGenotypes HWE test quality score AA AC CC AA AC CC
Alves Corrêa 2009 Brazil Caucasian PCR-RFLP PB BC 101/307 65 31 5 157 135 15 0.04 9
Sierra 2009 Mexico Caucasian PCR-RFLP PB PC 20/38 4 16 0 6 19 13 0.83 11
Mendizábal-Ruiz 2010 Mexico Caucasian PCR-RFLP PB BC 64/224 44 17 3 121 83 20 0.30 12
Namazi 2010 Iran Caucasian PCR-RFLP PB BC 444/329 40 30 0 38 28 4 0.69 13
Ouyang 2011 China Asian Taqman PB APA 148/192 96 43 9 102 73 17 0.45 12
Fishchuk 2013 Ukraine Caucasian PCR-RFLP PB BC 131/102 72 47 12 64 24 14 0.00 9
Ding 2014 China Asian PCR-RFLP HB BC 606/633 504 93 9 576 54 3 0.16 12
BC, Breast cancer; PC, Prostate cancer; APA, Aldosterone-producing adenoma; HWE, Hardy-Weinberg Equilibrium; HB, hospital based; PB, population based.
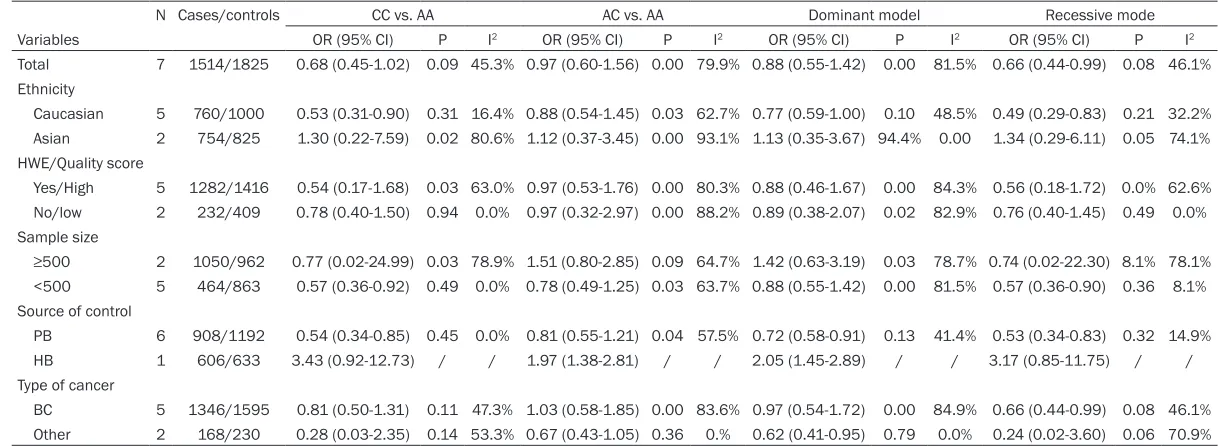
[image:4.612.84.526.232.691.2]Table 3. Summary of different comparative results
N Cases/controls CC vs. AA AC vs. AA Dominant model Recessive mode
Variables OR (95% CI) P I2 OR (95% CI) P I2 OR (95% CI) P I2 OR (95% CI) P I2
Total 7 1514/1825 0.68 (0.45-1.02) 0.09 45.3% 0.97 (0.60-1.56) 0.00 79.9% 0.88 (0.55-1.42) 0.00 81.5% 0.66 (0.44-0.99) 0.08 46.1%
Ethnicity
Caucasian 5 760/1000 0.53 (0.31-0.90) 0.31 16.4% 0.88 (0.54-1.45) 0.03 62.7% 0.77 (0.59-1.00) 0.10 48.5% 0.49 (0.29-0.83) 0.21 32.2%
Asian 2 754/825 1.30 (0.22-7.59) 0.02 80.6% 1.12 (0.37-3.45) 0.00 93.1% 1.13 (0.35-3.67) 94.4% 0.00 1.34 (0.29-6.11) 0.05 74.1%
HWE/Quality score
Yes/High 5 1282/1416 0.54 (0.17-1.68) 0.03 63.0% 0.97 (0.53-1.76) 0.00 80.3% 0.88 (0.46-1.67) 0.00 84.3% 0.56 (0.18-1.72) 0.0% 62.6%
No/low 2 232/409 0.78 (0.40-1.50) 0.94 0.0% 0.97 (0.32-2.97) 0.00 88.2% 0.89 (0.38-2.07) 0.02 82.9% 0.76 (0.40-1.45) 0.49 0.0%
Sample size
≥500 2 1050/962 0.77 (0.02-24.99) 0.03 78.9% 1.51 (0.80-2.85) 0.09 64.7% 1.42 (0.63-3.19) 0.03 78.7% 0.74 (0.02-22.30) 8.1% 78.1%
<500 5 464/863 0.57 (0.36-0.92) 0.49 0.0% 0.78 (0.49-1.25) 0.03 63.7% 0.88 (0.55-1.42) 0.00 81.5% 0.57 (0.36-0.90) 0.36 8.1%
Source of control
PB 6 908/1192 0.54 (0.34-0.85) 0.45 0.0% 0.81 (0.55-1.21) 0.04 57.5% 0.72 (0.58-0.91) 0.13 41.4% 0.53 (0.34-0.83) 0.32 14.9%
HB 1 606/633 3.43 (0.92-12.73) / / 1.97 (1.38-2.81) / / 2.05 (1.45-2.89) / / 3.17 (0.85-11.75) / / Type of cancer
BC 5 1346/1595 0.81 (0.50-1.31) 0.11 47.3% 1.03 (0.58-1.85) 0.00 83.6% 0.97 (0.54-1.72) 0.00 84.9% 0.66 (0.44-0.99) 0.08 46.1% Other 2 168/230 0.28 (0.03-2.35) 0.14 53.3% 0.67 (0.43-1.05) 0.36 0.% 0.62 (0.41-0.95) 0.79 0.0% 0.24 (0.02-3.60) 0.06 70.9%
applied. Subgroup analysis was also conducted according to ethnicity, quality score, sample size, source of control and cancer type. Sen- sitivity analysis was performed by removing the studies which were not in HWE. The funnel plot asymmetry was assessed by Begg’s test to estimate the potential publication bias (P<0.05 indicates statistical significance). The meta-analysis was performed using the STATA pack-age version 12.0 (Stata Corporation, College Station, TX, USA).
Results
Eligible studies
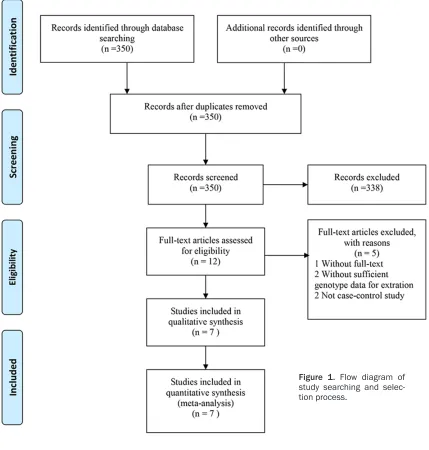
The study selection process is shown in Figure 1. A total of 7 case-control studies, including
[image:6.612.93.525.73.479.2]1514 cases and 1825 controls, were identified according to the inclusion and exclusion criteria [15-21]. The characteristics of the studies included in the current meta-analysis are pre-sented in Table 2. Among these studies, 5 were conducted for breast cancer (BC), 1 for pros-tate cancer (PC) and 1 for aldosterone-produc-ing adenoma (APA). The source of controls was mainly based on population-based studies except one study [21]. Regarding ethnicity, there were 5 studies on Caucasians and 2 stud-ies on of Asians. In all the studstud-ies, the control genotype distributions were in HWE except for those of Alves Corrêa et al. and Fishchuk et al. [15, 20]. Five studies were small sample size studies [15-17, 19, 20], while two were not [18, 21]. Additionally, 5 were conducted using the
PCR-RFLP method, 1 using the Taqman method [19]. The publication year of the included stud-ies ranged from 2009 to 2014. Five of the included studies were of high quality, as indi-cated by the quality score assessment which was higher than or equal to 10 points.
Meta-analysis results
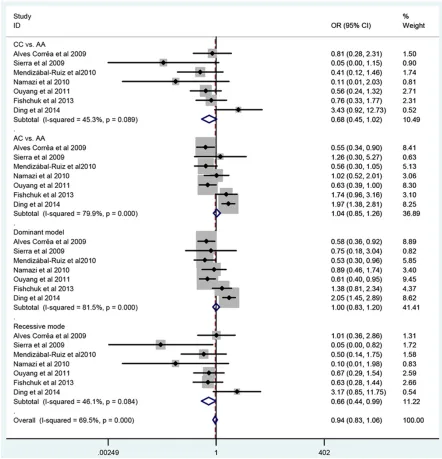
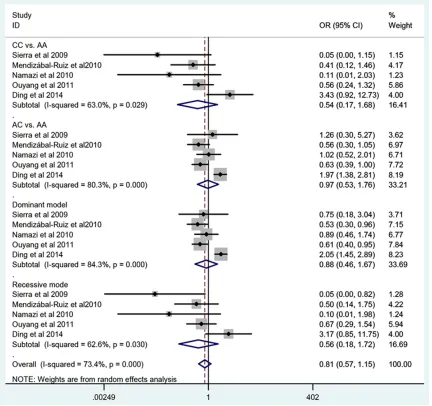
Summaries A summary of the meta-analysis findings on the association between AT1R gene A1166C polymorphism and cancer risk are is shown in Figure 2 and Table 3. Individuals with the CC genotype of AGTR1 gene A1166C poly-morphism were significantly associated with decreased risk of cancer (CC vs. AA: OR=0.68, 95% CI 0.45-1.02; AC vs. AA: OR=0.97, 95% CI 0.60-1.56; Dominant model: OR=0.88, 95% CI 0.55-1.42; Recessive model: OR=0.66, 95% CI 0.44-0.99). Considering the potential impact of the confounding factors on the overall results, we further performed subgroup analyses. When stratified according to ethnicity, we detected a significantly decreased cancer risk with the CC genotype in Caucasians (CC vs. AA: OR=0.53, 95% CI 0.31-0.90; AC vs. AA: OR=0.88, 95% CI 0.54-1.45; Dominant model: OR=0.77, 95% CI 0.59-1.00; Recessive model: OR=0.49, 95% CI 0.29-0.83), but not in Asians. In the stratified analysis by sample size, we detected no significant association for studies with >500 subjects. On the other hand, when limiting the analysis to the study sample size of <500, we detected significant association between the A1166C polymorphism and
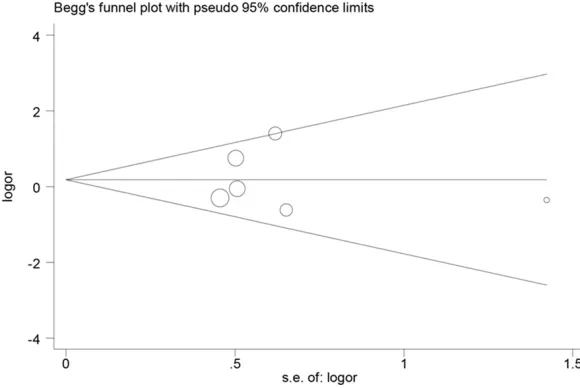
can-assess the publication bias of literatures. The results indicated that there was no evidence of publication bias in our study (Figure 4), implying that the publication bias was low in the present meta-analysis.
Discussion
[image:7.612.92.382.74.268.2]About 14.1 million cancer cases and 8.2 million cancer deaths were reported in the GLOBOCAN 2012 report, indicating that cancer has already become a global public health problem [22]. It is widely known to us that cancer is a disorder resulting from complex interrelationships be- tween environmental and genetic factors. The RAS has emerged as a prominent signaling pathway implicated in homeostasis, angiogen-esis and tumor metastasis [23]. Recent meta-analysis demonstrated that the ACE gene I allele might be a protective factor against gas-tric cancer [24]. Thus far, up to now, a number of studies have been conducted to evaluate the association between the AGTR1 gene A1166C polymorphism and the risk of different types of cancers. However, the results from the pub-lished studies have been inconclusive, even conflictive. In order to obtain a comprehensive and precise result, we performed this meta-analysis study to determine the association between this polymorphism and cancer risk. On the basis of the 7 case-control studies with a total of 1514 cancer cases and 1825 con-trols, our meta-analysis comprehensively eval-uated the association between the AGTR1 gene A1166C polymorphism and risk of cancer. Our
Figure 4. Begg’s funnel plot for publication bias test.
cer. Further subgroup anal-ysis using the source of control, we detected signifi-cant association with popu-lation-based studies and hospital based studies. In addition, when stratified according to cancer type, the A1166C polymorphism was associated with BC.
Sensitivity analysis and publication bias
results show that the AGTR1 gene A1166C polymorphism is associated with decreased cancer risk when all the qualified studies were poo- led into the meta-analysis. In term of stratified analyses by ethnic groups, our findings indicat-ed that the AGTR1 gene A1166C polymorphism had an significant association with cancer risk in Caucasians, but not in Asians. These differ-ences may be result from different genetic backgro- unds and environmental exposures. In the sub-group analysis based on cancer type, a signifi-cantly decreased cancer risks was observed in BC. When stratifying by sample size (<500), this meta-analysis detects significant association, suggesting a possibility of publication bias by in smaller studies. In addition, we also conducted a sensitivity analysis. Specifically, after remov-ing non-HWE studies, the significant associa-tion between the AGTR1 gene A1166C poly-morphism and cancer risk became null, which suggests that the HWE violation was a signifi-cant source of the heterogeneity in the meta-analysis. And the observed associations be- tween the AGTR1 gene A1166C polymorphism and decreased cancer risk may reflect chance observations rather than true associations. Therefore, the results should be interpreted with caution, further large and well-designed studies are needed to confirm these findings. Several limitations of our study should be noted. First, our systematic review was based on unadjusted data, because the genotype information stratified for the main confounding variables was not available in the original papers and also the confounding factors addressed across the different studies were variable. Second, the effect of potential gene-gene and gene-gene-environment interactions could not be addressed as well in this meta-analysis. Third, a meta-analysis is a retrospective re- search that is subject to methodological limi- tations.
In conclusion, the present meta-analysis indi-cated that the A1166C polymorphism in AGTR1 gene is associated with a significantly de- creased risk of cancer, especially in Caucasian population and in particular BC. Admittedly, fur-ther studies estimating the effect of gene-gene and gene-environment interactions may even-tually provide a better, comprehensive under-standing of such association.
Disclosure of conflict of interest None.
Address correspondence to: Shengjun Wu, De- partment of Clinical Laboratory, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, No. 3, Qingchun East Road, Hangzhou 310000, Zhejiang Province, People’s Republic of China. Tel: +86 0571 86002066; E-mail: wushengjun001@126. com
References
[1] Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90.
[2] Marron M, Boffetta P, Zhang ZF, Zaridze D, Wünsch-Filho V, Winn DM, Wei Q, Talamini R, Szeszenia-Dabrowska N, Sturgis EM, Smith E,
Schwartz SM, Rudnai P, Purdue MP, Olshan AF,
Eluf-Neto J, Muscat J, Morgenstern H, Menez-es A, McClean M, Matos E, MatMenez-es IN, Lissows-ka J, Levi F, Lazarus P, La Vecchia C, Koifman S, Kelsey K, Herrero R, Hayes RB, Franceschi S, Fernandez L, Fabianova E, Daudt AW, Dal Maso L, Curado MP, Cadoni G, Chen C, Castell-sague X, Boccia S, Benhamou S, Ferro G, Berthiller J, Brennan P, Møller H, Hashibe M. Cessation of alcohol drinking, tobacco smok-ing and the reversal of head and neck cancer risk. Int J Epidemiol 2010; 39: 182-196. [3] Zaridze DG. Molecular epidemiology of cancer.
Biochemistry 2008; 73: 532-542.
[4] Harrison-Bernard LM. The renal renin-angio-tensin system. Adv Physiol Educ 2009; 33: 270-274.
[5] Mehta PK, Griendling KK. Angiotensin II cell signaling: physiological and pathological ef-fects in the cardiovascular system. Am J Physi-ol Cell PhysiPhysi-ol 2007; 292: C82-97.
[6] Okamoto K, Tajima H, Ohta T, Nakanuma S, Hayashi H, Nakagawara H, Onishi I, Takamura
H, Ninomiya I, Kitagawa H, Fushida S, Tani T, Fujimura T, Kayahara M, Harada S, Wakayama T, Iseki S. Angiotensin II induces tumor
pro-gression and fibrosis in intrahepatic cholangio -carcinoma through an interaction with hepatic
stellate cells. Int J Oncol 2010; 37: 1251-1259.
[7] Du N, Feng J, Hu LJ, Sun X, Sun HB, Zhao Y, Yang YP, Ren H. Angiotensin II receptor type 1 blockers suppress the cell proliferation effects of angiotensin II in breast cancer cells by
inhib-iting AT1R signaling. Oncol Rep 2012; 27:
1893-1903.
[8] Tybitanclova K, Macejova D, Liska J, Brtko J, Zorad S. AT1 receptor and ACE mRNA are in-creased in chemically induced carcinoma of rat mammary gland. Mol Cell Endocrinol 2005; 244: 42-46.
[10] Huang W, Yu LF, Zhong J, Qiao MM, Jiang FX, Du F, Tian XL, Wu YL. Angiotensin II type 1 re-ceptor expression in human gastric cancer and induces MMP2 and MMP9 expression in MKN-28 cells. Dig Dis Sci 2008; 53: 163-168. [11] Xu M, Sham P, Ye Z, Lindpaintner K, He L.
A1166C genetic variation of the angiotensin II type I receptor gene and susceptibility to coro-nary heart disease: collaborative of 53 studies with 20,435 cases and 23,674 controls. Ath-erosclerosis 2010; 213: 191-199.
[12] Niu W, Qi Y. Association of the angiotensin II type I receptor gene +1166 A>C polymor-phism with hypertension risk: evidence from a meta-analysis of 16474 subjects. Hypertens Res 2010; 33: 1137-1143.
[13] Attia J, Thakkinstian A, D’Este C. Meta-analy-ses of molecular association studies: method-ologic lessons for genetic epidemiology. J Clin Epidemiol 2003; 56: 297-303.
[14] Higgins JP, Thompson SG. Quantifying hetero-geneity in a meta-analysis. Stat Med 2002; 21: 1539-1558.
[15] Alves Corrêa SA, Ribeiro de Noronha SM, Nogueira-de-Souza NC, Valleta de Carvalho C, Massad Costa AM, Juvenal Linhares J, Vieira Gomes MT, Guerreiro da Silva ID. Association between the angiotensin-converting enzyme (insertion/deletion) and angiotensin II type 1 receptor (A1166C) polymorphisms and breast cancer among Brazilian women. J Renin Angio-tensin Aldosterone Syst 2009; 10: 51-58. [16] Sierra Díaz E, Sánchez Corona J, Rosales
Gó-mez RC, Gutierrez Rubio SA, Vázquez Cama-cho JG, Solano Moreno H, Morán Moguel MC. Angiotensin-converting enzyme insertion/dele-tion and angiotensin type 1 receptor A1166C polymorphisms as genetic risk factors in be-nign prostatic hyperplasia and prostate cancer. J Renin Angiotensin Aldosterone Syst 2009; 10: 241-246.
[17] Mendizábal-Ruiz AP, Morales J, Castro Marti-nez X, Gutierrez Rubio SA, Valdez L, Vásquez-Camacho JG, Sanchez Corona J, Moran Mo-guel MC. RAS polymorphisms in cancerous and benign breast tissue. J Renin Angiotensin Aldosterone Syst 2011; 12: 85-92.
[18] Namazi S, Monabati A, Ardeshir-Rouhani-Fard S, Azarpira N. Association of angiotensin I con-verting enzyme (insertion/deletion) and angio-tensin II type 1 receptor (A1166C) polymor-phisms with breast cancer prognostic factors in Iranian population. Mol Carcinog 2010; 49: 1022-1030.
[19] Ouyang J, Wu Z, Xing J, Yan Y, Zhang G, Wang B,
Li H, Ma X, Zhang X. Association of polymor-phisms in angiotensin II receptor genes with aldosterone-producing adenoma. J Huazhong Univ Sci Technolog Med Sci 2011; 31: 301-305.
[20] Fishchuk LE, Gorovenko NG. Genetic polymor-phisms of the renin-angiotensin system in
breast cancer patients. Exp Oncol 2013; 35:
101-104.
[21] Ding P, Yang Y, Ding S, Sun B. Synergistic as-sociation of six well-characterized polymor-phisms in three genes of the renin-angiotensin system with breast cancer among Han Chinese women. J Renin Angiotensin Aldosterone Syst 2015; 16: 1232-9.
[22] Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieu-lent J, Jemal A.Global cancer statistics, 2012. CA Cancer J Clin 2015; 65: 87-108.
[23] Egami K, Murohara T, Shimada T, Sasaki K, Shintani S, Sugaya T, Ishii M, Akagi T, Ikeda H, Matsuishi T, Imaizumi T. Role of host angioten-sin II type 1 receptor in tumor angiogenesis and growth. J Clin Invest 2003; 112: 67-75. [24] Yang H, Cai C, Ye L, Rao Y, Wang Q, Hu D,