Review Article
Hematologic adverse events (HAEs) of
Eribulin used in treating metastatic breast cancer
(MBC): a meta-analysis of randomized controlled trials
Chongxiang Chen
1, Jiaojiao Wang
2, Qingyu Zhao
11Department of Intensive Care Unit, Sun Yat-sen University Cancer Center; State Key Laboratory of Oncology in
South China; Collaborative Innovation Center for Cancer Medicine, Guangzhou 510060, Guangdong Province, China; 2Department of Tuberculosis, Pulmonary Hospital of Fuzhou of Fujian Province, Fuzhou, Fujian Province,
China
Received October 11, 2017; Accepted February 6, 2018; Epub June 15, 2018; Published June 30, 2018
Abstract: Objective: The objective was to conduct a systematic review and meta-analysis of MBC focusing on HAEs comparing eribulin monotherapy with other therapeutic regimens. Methods: PubMed and The Web of Science were searched for RCTs comparing eribulin monotherapy with other regimens for the treatment of metastatic breast cancer. Meta-analyses were used to estimate the odds ratios (OR) of adverse events (AEs), severe adverse events (SAEs), discontinuation of therapy due to adverse events (DAEs), and HAEs, such as neutropenia, anemia, leucope-nia, respectively. Results: We included in 3 RCTs of a total of 1968 patients with MBC and divided them into eribulin and comparator groups with 1114 patients and 854 patients, respectively. For AEs, the result comparing eribulin versus comparator (OR 4.09, 95% CI 3.33-5.01, I2=89%) was significantly different with high heterogeneity. For ei
-ther SAEs (OR 0.86, 0.68-1.08, I2=0%) or DAEs (OR 0.79, 0.58-1.06, I2=0%), the comparison was similar. For HAEs,
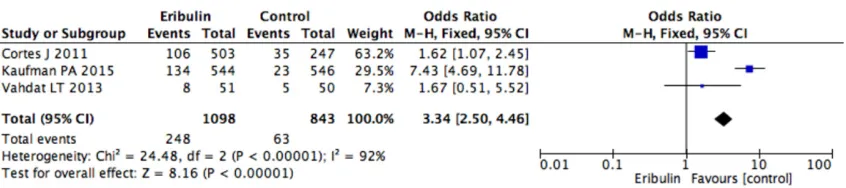
overall neutropenia (OR 4.09, 3.33-5.01, I2=89%), grade 3 neutropenia (OR 3.34 95% CI 2.50-4.46, I2=92), grade
4 neutropenia (OR 7.92, 95% CI 5.25-11.94, I2=90%), using MGF (OR 3.43, 95% CI 2.38-4.93, I2=54%), and febrile
neutropenia (OR 2.58, 95% CI 1.21-5.48, I2=0%) showed significant differences. Whereas for overall anemia (OR
0.99, 95% CI 0.78-1.24, I2=19%), grade 3 anemia (OR 1.06, 95% CI 0.78-1.24, I2=49%), grade 4 anemia (OR 0.41,
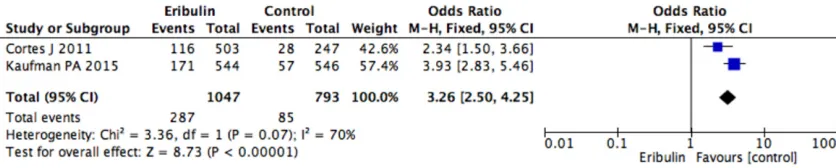
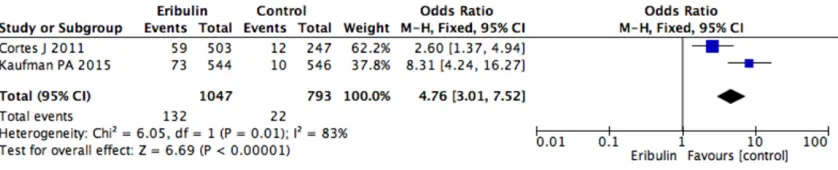
95% CI 0.05-3.27, I2=0%), overall leukopenia (OR 3.26, 95% CI 2.50-4.25, I2=70%), grade 3 leukopenia (OR 4.76,
95% CI 3.01-7.52, I2=83%), and grade 4 leukopenia (OR 4.49, 95% CI 1.35-14.97, I2=0%), the results were similar
in all groups. Conclusions: When treating patients with MBC that have previously been treated with more than two chemotherapy regimens, eribulin exerts more HAEs than others, and should be taken into consideration to treat with myeloid growth factor (MGF) support in all cycles if risk factors of febrile neutropenia are present.
Keywords: Eribulin, metastatic breast cancer, MBC
Introduction
Treatments based on anthracyclines or taxanes
are widely used in first-line of MBC [1], and
(neo) adjuvant stage. However, treatment
deci-sions in subsequent lines are difficult [2].
Eribulin, a non-taxane inhibitor of microtubule
dynamics of the halichondrin class of
antineo-plastic drugs, is a structurally modified synthet
-ic analogue of hal-ichondrin B, a natural product
isolated from the marine sponge Halichondria
okadai. Eribulin is different from other
tubulin-targeting agents [3-7] in action through inhibit
-ing the microtubule growth phase without
affecting the shortening phase, and causing
tubulin sequestration into non-productive ag-
gregates.
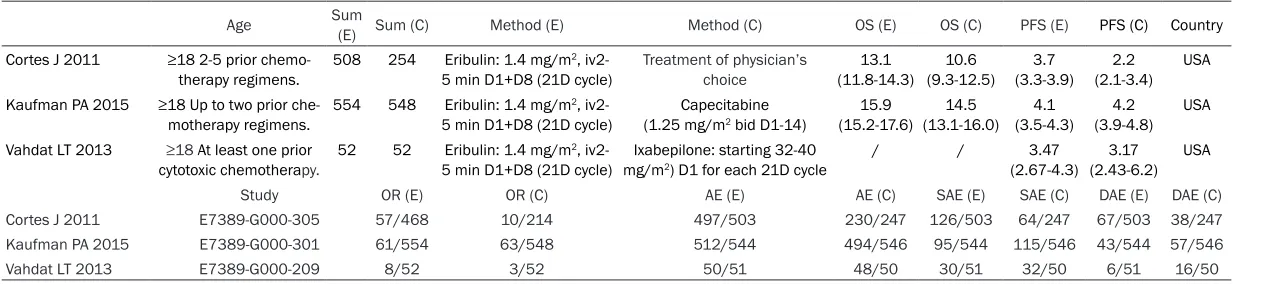
cytotoxic chemotherapy. 5 min D1+D8 (21D cycle) mg/m) D1 for each 21D cycle (2.67-4.3) (2.43-6.2)
Study OR (E) OR (C) AE (E) AE (C) SAE (E) SAE (C) DAE (E) DAE (C)
Cortes J 2011 E7389-G000-305 57/468 10/214 497/503 230/247 126/503 64/247 67/503 38/247
Kaufman PA 2015 E7389-G000-301 61/554 63/548 512/544 494/546 95/544 115/546 43/544 57/546
[image:2.792.89.722.84.226.2]Figure 1. Comparison of AEs between eribulin and comparator.
[image:3.612.94.522.473.566.2]Figure 2. Comparison of SAEs between eribulin and comparator.
[image:3.612.97.520.606.700.2]Figure 3. Comparison of DAEs between eribulin and comparator.
Figure 4. Comparison of neutropenia between eribulin and comparator.
studies and relevant papers were also
manual-ly searched and reviewed. A total of 510
arti-cles were found, and through reading the title
and abstract 501 articles were excluded,
leav-ing 3 articles [11-13] (
Table 1
).
Inclusion and exclusion
Inclusion: (1) Researched body, coincided with
MBC. (2) Two groups and one of them included
eribulin. (3) Outcome: including AEs, especially
HAEs.
Exclusion: (1) Breast cancer in situ or first regi
-men in MBC. (2) Review or retrospective
research. (3) insufficient data.
Data elected
Two authors extracted the data below: First
author, country, sum of patients et al. and the
baseline characteristics of these studies were
included.
Statistical analysis
RevMan 5.3 was performed to analyze the
clini-cal data for OR and with a 95% CI. Summary
statistics for each study were expressed as OR
with 95% CI for dichotomous outcomes (e.g.
AEs, SAEs, DAEs, HAEs, using MGF, febrile
neu-tropenia). Data were pooled and expressed
with this as an OR with a 95% CI.
Results
Our study comparing eribulin and comparator
groups demonstrated that eribulin, a new
che-motherapy agent in metastatic breast cancer,
exert more AEs than other monotherapeutic
regimens (OR 4.09, 95% CI 3.33-5.01, I
2=89%),
whereas either SAEs (OR 0.86, 95% CI
0.68-1.08, I
2=0%) or DAEs (OR 0.79, 95% CI
0.58-1.06, I
2=0%) were not different between the
groups (
Figures 1
-
3
).
For HAEs, the results comparing groups were
significantly different in neutropenia (OR 4.09,
3.33-5.01, I
2=89%), grade 3 neutropenia (OR
significant difference in groups (
Figures 7
-
9
).
The results for leukopenia (OR 3.26, 95% CI
2.50-4.25, I
2=70%), grade 3 leukopenia (OR-
4.76, 95% CI 3.01-7.52, I
2=83%), and grade 4
leukopenia (OR 4.49, 95% CI 1.35-14.97, I
2=
0%) showed a significant difference in groups
(
Figures 10
-
12
).
The results using MGF (OR 3.43, 95% CI
2.38-4.93, I
2=54%), and febrile neutropenia (OR
2.58, 95% CI 1.21-5.48, I
2=0%) showed a
sig-nificant difference in comparisons (
Figures 13
,
14
).
Discussion
Treatments based on anthracyclines or taxanes
are widely used as first-line therapy for MBC [1],
and (neo) adjuvant stages. However, decisions
of treatment in subsequent lines are hardly to
decide [2].
Eribulin, a nontaxane microbiotubule dynamics
inhibitor, belongs to the halichondrin class of
anticancer agents [14, 15]. It is different from
other tubulin-targeted agents in anticancer
through binding predominantly to a small
num-ber of high-affinity sites on the growing plus
ends of microtubules [16, 17]. This highly
focused end binding may likely decrease the
effects of eribulin on physiologic microtubule
functions in nonmalignant cells [18, 19]. The
ability of eribulin to block mitosis is irreversible
contrasting to other tubulin-targeted agents,
and intermittent drug exposure could result in
long-periods of loss of cell feasibility [20].
Figure 6. Comparison of grade 4 neutropenia between eribulin and comparator.
Figure 7. Comparison of anemia between eribulin and comparator.
Figure 8. Comparison of grade 3 anemia between eribulin and comparator.
Figure 9. Comparison of grade 4 anemia between eribulin and comparator.
[image:5.612.93.515.474.565.2] [image:5.612.95.513.609.693.2](95% CI 3.3-3.9) with eribulin and 2.2 months
(2.1-3.4) with TPC [11]. The results of Study
301 comparing eribulin with capecitabine for
advanced breast cancer or MBC demonstrated
an increased trend in eribulin with 15.9 months
(95% CI, 15.2-17.6) versus capecitabine with
14.5 months (95% CI, 13.1-16). As we can see,
Capecitabine is commonly used in the first-,
second-, and third-line settings for MBC and it
has also been the control arm in several trials
in MBC [21-24].
For the AEs, previously reported, manageable
[image:6.612.99.518.72.157.2] [image:6.612.96.511.197.281.2]nia, and peripheral neuropathy, have occurred
in patients using eribulin. Neutropenia was
managed with dose delays, reductions, and
MGF according to practice. In the EMBRACE
study 301 and study 209, the results of the
occurrence of all grades neutropenia were
52%, 54.2%, and 47.1%, respectively; for grade
3 neutropenia were 21%, 24.6%, and 15.7%,
respectively; for grade 4 neutropenia were
24%, 24.6%, 15.7%, respectively. Our analysis
comparing eribulin versus comparator showed
that overall neutropenia (OR 4.09, 3.33-5.01,
I
2=89%), grade 3 neutropenia (OR 3.34 95% CI
Figure 11. Comparison of grade 3 leukopenia between eribulin and comparator. [image:6.612.93.517.324.408.2]Figure 12. Comparison of grade 4 leukopenia between eribulin and comparator.
[image:6.612.95.518.450.534.2]Figure 13. Comparison of using MGF between eribulin and comparator.
7.92, 95% CI 5.25-11.94, I
2=90) was signifi
-cantly difference in comparisons [11-13].
The results with high heterogeneities in these
analyses because Ixabepilone, which is like
eribulin aiming at microtubule, is the
compara-tor of the Study 209. In Study 209, the overall
neutropenia (OR 2.29, 95% CI 1.00-5.22),
grade 3 neutropenia (OR 1.67, 95% CI
0.51-5.52), or grade 4 neutropenia (OR 1.67, 95% CI
0.51-5.52) did not show significantly difference,
but the results of the others (EMBRACE and
study 301) showed a significant difference.
In our analysis, using MGF (OR 3.43, 95% CI
2.38-4.93, I
2=54%), and febrile neutropenia
(OR 2.58, 95% CI 1.21-5.48, I
2=0%) showed
significantly differences. In the EMBRACE
st-udy, the rate of using MGF was 18% versus 8%
of eribulin and comparators, respectively, and
in study 301, the rate was 14.6% versus 3.6%.
The NCCN guideline version 2013 of MGF
sug-gested preventive using MGF when the
occur-rence rate of febrile neutropenia is higher than
20%, and considering to preventive use when
ranges from 10% to 20%. Although the
occur-rence rates of febrile neutropenia of eribulin
group were relatively low in the EMBRACE and
301 study with rates of 5% and 2%,
respective-ly [25].
One the one hand, according to the guidelines,
other high-risk factors (e.g. older patient >65
years , radiation therapy or chemotherapy ,
neutropenia or one marrow involvement with
tumor, neutropenia infection/open wounds, re-
cent surgery, poor renal function or liver
dys-function) must be taken into consideration in
febrile neutropenia. A low-risk regimen does
not necessarily preclude the use of CSFs in a
patient with high-risk factors [25].
Breast cancer is a neoplasm with
chemothera-peutic sensitivity and a high survival rate.
Patients with MBC, treated with eribulin and
second-lines regimens, are almost always at an
older age. In EMBRACE, median age of eribulin
group is 55 years, ranging from 28-85 with a
median age of the comparator group is 56
years, ranging from 27-81. In study 301, the
median age of eribulin is 54 years, ranging from
24-80 with a median age of comparator group
is 53 years, ranging from 26-80. MBC is often
found when metastasizing to bone, destroying
bone marrow, and influencing the function of
hematopoiesis. Liver or kidney metastasis of
MBC also carries a high risk of febrile
neutrope-nia because of poor liver or kidney function.
Above all, older age, destroying bone marrow,
and poor liver/kidney function are often
discov-ered as characteristic of patients with MBC
who have treated with more than two lines
regimens.
In the guideline, the regimens of breast cancer
of which the occurrence rates of febrile
neutro-penia are more than 20% [e.g. Docetaxel +
trastuzumab, Dose-dense AC (doxorubicin + cy-
clophosphamide) followed by T (Paclitaxel), TAC
(docetaxel + doxorubicin + cyclophosphamide)]
preventive treatment using MGF is required;
other frequent regimens [(e.g. Docetaxel every
21 days, CMF (cyclophosphamide +
methotrex-ate + fluorouracil), AC + sequential docetaxel,
AC + sequential docetaxel + trastuzumab, FEC
(fluorouracil + epirubicin + cyclophosphamide)
+ sequential docetaxel or Paclitaxel every 21
days)] are listed as 10-20% of the occurrence
rate of febrile neutropenia, which also should
consider preventive MGF treatment. According
to the guidelines, almost all regimens treating
patients with breast cancer are in the list of
intermittent or high occurrence rates of febrile
neutropenia. Patients with MBC that are
treat-ed with more than two regimens there are high
risks of febrile neutropenia because of
previ-ous chemotherapy, preexisting neutropenia,
and poor performance status, all of which are
accounted for as risk factors of febrile
neutro-penia and are characteristic of the relevant
treatments.
One the other hand, AC-T (cycling 3 weeks),
which in the guideline is listed as an
intermit-tent risk regimen, in some RCTs, of which the
occurrence rate of febrile neutropenia is less
than 5% in GEPARDUO study [26], and in a
study conducted by Burnell M et al. [27] was
4.8%, but these two studies didn’t use
preven-tive MGF in AC-T (cycling 3 weeks) group.
Another study conducted by Leone JP et al. [28]
showed that in a total of 126 patients treated
with FAC or CMF, only 2 patients had febrile
neutropenia. In the guidelines, these regimens
are all intermittent risk at 10-20%, so the data
of Clinical trials should take this into con-
sideration.
occur-into consideration to assess status of the
patients with MBC treated with eribulin of which
have been pre-treated with more than two lines
regimens. Because these patients, especially
older than >65 years old, having history of
neu-tropenia, and having metastasis to the liver or
kidney, are more likely to develop a need for
GCF for preventing neutropenia and febrile
neutropenia.
Disclosure of conflict of interest
None.
Address correspondence to: Qingyu Zhao, De- partment of Intensive Care Unit, Sun Yat-sen University Cancer Center; State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine, 651 Dongfeng East Road, Guangzhou 510060, Guangdong Province, China. E-mail: [email protected]
References
[1] Andreopoulou E, Sparano JA. Chemotherapy in patients with anthracycline- and taxane-pre-treated metastatic breast cancer: an overview. Curr Breast Cancer Rep 2013; 5: 42-50. [2] Moreno-Aspitia A, Perez EA. Treatment options
for breast cancer resistant to anthracycline and taxane. Mayo Clin Proc 2009; 84: 533-545.
[3] Towle MJ, Salvato KA, Budrow J, Wels BF, Kuznetsov G, Aalfs KK, Welsh S, Zheng W, Se-letsky BM, Palme MH, Habgood GJ, Singer LA, Dipietro LV, Wang Y, Chen JJ, Quincy DA, Davis A, Yoshimatsu K, Kishi Y, Yu MJ, Littlefield BA. In vitro and in vivo anticancer activities of syn-thetic macrocyclic ketone analogues of hali-chondrin B. Cancer Res 2001; 61: 1013-21. [4] Jordan MA, Kamath K, Manna T, Okouneva T,
Miller HP, Davis C, Littlefield BA, Wilson L. The primary antimitotic mechanism of action of the synthetic halichondrin E7389 is suppression of microtubule growth. Mol Cancer Ther 2005; 4: 1086-95.
[5] Kuznetsov G, Towle MJ, Cheng H, Kawamura T, TenDyke K, Liu D, Kishi Y, Yu MJ, Littlefield BA. Induction of morphological and biochemical
BM, Littlefield BA, Jordan MA. Eribulin binds at microtubule ends to a single site on tubulin to suppress dynamic instability. Biochemistry 2010; 49: 1331-37.
[8] Wozniak KM, Nomoto K, Lapidus RG, Wu Y, Carozzi V, Cavaletti G, Hayakawa K, Hosokawa S, Towle MJ, Littlefield BA, Slusher BS. Com -parison of neuropathy-inducing effects of erib-ulin versus paclitaxel in mice. Cancer Res 2011; 71: 3952-62.
[9] Kuznetsov G, TenDyke K, Yu MJ, Littlefield BA. Antiproliferative effects of halichondrin B ana-log eribulin mesylate (E7389) against paclitax-el-resistant human cancer cells in vitro. Proc Am Assoc Cancer Res 2007; 48: 275, abstr C58.
[10] National Comprehensive Cancer Network (2017). NCCN clinical practice guidelines in on-cology (NCCN Guidelines®). Breast cancer, version 2.
[11] Cortes J, O’Shaughnessy J, Loesch D, Blum JL, Vahdat LT, Petrakova K, Chollet P, Manikas A, Diéras V, Delozier T, Vladimirov V, Cardoso F, Koh H, Bougnoux P, Dutcus CE, Seegobin S, Mir D, Meneses N, Wanders J, Twelves C; EM-BRACE (Eisai Metastatic Breast Cancer Study Assessing Physician’s Choice Versus E7389) investigators. Eribulin monotherapy versus treatment of physician’s choice in patients with metastatic breast cancer (EMBRACE): a phase 3 open-label randomised study. Lancet 2011; 377: 914-23.
[12] Kaufman PA, Awada A, Twelves C, Yelle L, Per-ez EA, Velikova G, Olivo MS, He Y, Dutcus CE, Cortes J. Phase III open-label randomized study of eribulin mesylate versus capecitabine in patients with locally advanced or metastatic breast cancer previously treated with an an-thracycline and a taxane. J Clin Oncol 2015; 33: 594-601.
[13] Vahdat LT, Garcia AA, Vogel C, Pellegrino C, Lindquist DL, Iannotti N, Gopalakrishna P, Sparano JA. Eribulin mesylate versus ixabepi-lone in patients with metastatic breast cancer: a randomized Phase II study comparing the incidence of peripheral neuropathy. Breast Cancer Res Treat 2013; 140: 341-51.
apoptosis following prolonged mitotic blockage by halichondrin B macrocyclic ketone analog E7389. Cancer Res 2004; 64: 5760-5766. [15] Towle MJ, Salvato KA, Budrow J, Wels BF,
Kuznetsov G, Aalfs KK, Welsh S, Zheng W, Se-letsky BM, Palme MH, Habgood GJ, Singer LA, Dipietro LV, Wang Y, Chen JJ, Quincy DA, Davis A, Yoshimatsu K, Kishi Y, Yu MJ, Littlefield BA. In vitro and in vivo anticancer activities of syn-thetic macro-cyclic ketone analogues of hali-chondrin B. Cancer Res 2001; 61: 1013-1021. [16] Jordan MA, Kamath K, Manna T, Okouneva T,
Miller HP, Davis C, Littlefield BA, Wilson L. The primary antimitotic mechanism of action of the synthetic halichondrin E7389 is suppression of microtubule growth. Mol Cancer Ther 2005; 4: 1086-1095.
[17] Okouneva T, Azarenko O, Wilson L, Littlefield BA, Jordan MA. Inhibition of centromere dy-namics by eribulin (E7389) during mitotic metaphase. Mol Cancer Ther 2008; 7: 2003-2011.
[18] Smith JA, Wilson L, Azarenko O, Zhu X, Lewis BM, Littlefield BA, Jordan MA. Eribulin binds at microtubule ends to a single site on tubulin to suppress dynamic instability. Biochemistry 2010; 49: 1331-1337.
[19] Wozniak KM, Nomoto K, Lapidus RG, Wu Y, Carozzi V, Cavaletti G, Hayakawa K, Hosokawa S, Towle MJ, Littlefield BA, Slusher BS. Com -parison of neuropathy-inducing effects of erib-ulin mesylate, paclitaxel, and ixabepilone in mice. Cancer Res 2011; 71: 3952-3962. [20] Thadani-Mulero M, Nanus DM, Giannakakou P.
Androgen receptor on the move: boarding the microtubule expressway to the nucleus. Can-cer Res 2012; 72: 4611-4615.
[21] Geyer CE, Forster J, Lindquist D, Chan S, Ro-mieu CG, Pienkowski T, Jagiello-Gruszfeld A, Crown J, Chan A, Kaufman B, Skarlos D, Cam-pone M, Davidson N, Berger M, Oliva C, Rubin SD, Stein S, Cameron D. Lapatinib plus capecitabine for HER2-positive advanced breast cancer. N Engl J Med 2006; 355: 2733-2743.
[22] Hortobagyi GN, Gomez HL, Li RK, Chung HC, Fein LE, Chan VF, Jassem J, Lerzo GL, Pivot XB, Hurtado de Mendoza F, Xu B, Vahdat LT, Peck RA, Mukhopadhyay P, Roché HH. Analysis of overall survival from a phase III study of ixa-bepilone plus capecitabine versus capecita- bine in patients with MBC resistant to anthra-cyclines and taxanes. Breast Cancer Res Treat 2010; 122: 409-418.
[23] Miller KD, Chap LI, Holmes FA, Cobleigh MA, Marcom PK, Fehrenbacher L, Dickler M, Over-moyer BA, Reimann JD, Sing AP, Langmuir V, Rugo HS. Randomized phase III trial of ca- pecitabine compared with bevacizumab plus capecitabine in patients with previously treat-ed metastatic breast cancer. J Clin Oncol 2005; 23: 792-799.
[24] Thomas ES, Gomez HL, Li RK, Chung HC, Fein LE, Chan VF, Jassem J, Pivot XB, Klimovsky JV, de Mendoza FH, Xu B, Campone M, Lerzo GL, Peck RA, Mukhopadhyay P, Vahdat LT, Roché HH. Ixabepilone plus capecitabine for meta-static breast cancer progressing after anthra-cycline and taxane treatment. J Clin Oncol 2007; 25: 5210-5217.
[25] National Comprehensive Cancer Network (2013). NCCN clinical practice guidelines in oncology (NCCN Guidelines®). Myeloid Growth Factors.
[26] von Minckwitz G, Raab G, Caputo A, Schütte M, Hilfrich J, Blohmer JU, Gerber B, Costa SD, Merkle E, Eidtmann H, Lampe D, Jackisch C, du Bois A, Kaufmann M. Doxorubicin with cy-clophosphamide followed by docetaxel every 21 days compared with doxorubicin and docetaxel every 14 days as preoperative treat-ment in operable breast cancer: the GEPAR-DUO study of the German Breast Group. J Clin Oncol 2005; 23: 2676-85.
[27] Burnell M, Levine MN, Chapman JA, Bramwell V, Gelmon K, Walley B, Vandenberg T, Chalchal H, Albain KS, Perez EA, Rugo H, Pritchard K, O’Brien P, Shepherd LE. Cyclophosphamide, epirubicin, and Fluorouracil versus dose-dense epirubicin and cyclophosphamide followed by Paclitaxel versus Doxorubicin and cyclophos-phamide followed by Paclitaxel in node-posi-tive or high-risk node-neganode-posi-tive breast cancer. J Clin Oncol 2010; 28: 77-82.