Implants Among Removable Prostheses Wearers
Ziad N. AL-Dwairi, BDS, PhD, FIADFE,1Bilal Mohammed El Masoud, BDS,2Sanaa A. AL-Afifi, BDS,3 Ali Borzabadi-Farahani, DDS, MScD, MOrth RCS(Ed),4,5 & Edward Lynch, BDentSci, PhD, FDSRCS(Ed)6 1Associate Professor, Faculty of Dentistry, Jordan University of Science and Technology, Irbid, Jordan
2Assistant Professor, Faculty of Dentistry, Jordan University of Science and Technology, Irbid, Jordan 3Postgraduate student, Faculty of Dentistry, Jordan University of Science and Technology, Irbid, Jordan
4Clinical Teaching Fellow, Orthodontics, Warwick Dentistry, Warwick Medical School, University of Warwick, Coventry, UK 5Former Research Scholar, Center for Craniofacial Molecular Biology, University of Southern California, Los Angeles, CA 6Head of Dentistry, Warwick Dentistry, Warwick Medical School, University of Warwick, Coventry, UK
Keywords
Complete denture; removable partial denture; awareness; expectations; dental implants.
Correspondence
Ziad N. AL-Dwairi, Associate Professor of Prosthodontics, Faculty of Dentistry, Jordan University of Science and Technology, PO Box 3030, Irbid 22110-Jordan. E-mail: [email protected].
This study was funded by the Department of Scientific Research at Jordan University of Science and Technology, Irbid, Jordan
The authors declare that they have no conflict of interest.
Accepted May 16, 2013
doi: 10.1111/jopr.12095
Abstract
Purpose:To assess removable denture patient awareness, expectations, and source of information about dental implants (DIs).
Materials and Methods: Three hundred patients [150 removable partial denture (RPD) wearers and 150 complete denture wearers (CDWs)] attended the removable prosthodontic clinic at Faculty of Dentistry, Jordan University of Science and Tech-nology. Patients were evaluated using a pilot-tested, 21-question questionnaire. Results:Ninety-six percent of participants were aware of DIs, with no difference be-tween CDWs and RPD wearers (p>0.05). The participants’ friends and relatives were the main source of information (63.4%), followed by dentists (32.4%). Improvement in function was the predominant reason (55.7%) for patients to consider DIs. Fear of unknown side effects was the major factor in preventing patients from choosing DIs (11.7%), followed by high cost (9.7%) and surgical risk (8.7%). Approximately 89% had no information or were poorly informed about DIs. Over two-thirds of patients did not know about the care (78.3%) of DIs, causes of DI failure (69.7%), or DI duration of service (80.7%). Only 24.7% knew that DIs would be anchored to the jaw-bone; however, 27.3% and 56.7% of CDWs and RPD wearers, respectively, preferred (p<0.05) to have their teeth replaced with DIs. High costs were considered the major disadvantage of DIs in 45% of participants, followed by fear of surgery (27.3%), and long treatment times (24.7%).
Conclusions:There was a high awareness about DIs among removable denture pa-tients; however, this awareness was associated with a low level of accurate information.
Today’s modern implant dentistry appeals to a wide popula-tion. Willingness to have implant treatment and its success depends on patient knowledge and expectations1as well as the care, skill, and judgment of clinicians. Since the introduction of dental implants (DIs), the efficacy of treatment has been confirmed by long-term clinical studies.2-6DIs were originally used for treating edentulous patients to improve denture re-tention, stability, functional efficiency, and quality of life.2-6 DIs are widely accepted for prosthetic treatment of completely or partially edentulous patients.7-10Implant-supported prosthe-ses have shown advantages such as increased masticatory ef-ficiency, maintenance of bone, improved function, phonetics, and esthetics.11,12
Information about patient awareness regarding DIs is impor-tant for planning health care services and marketing. Awareness
patient expectations with what can be achieved. Without access to current and accurate information, patients may face contra-dictory information supplied by media and industry, which does not always reflect evidence-based practice. Media, in particular, could be the main source of information in some countries,9,10 while in others, dentists were found to be the main source of information.1,11,18,19,22
Implants offer alternative treatment options to fully or par-tially edentulous patients. Elderly patients tend to tolerate func-tionally poor dentures better than younger edentulous patients do. They may favor using DIs for stabilizing their dentures and decline replacement of the existing conventional dentures.23,24 Currently, there is no information in the scientific literature about Jordanian patient awareness, knowledge, and expecta-tion toward DIs as treatment opexpecta-tions for replacement of teeth. Further, no data compare the awareness of DIs between partial denture wearers and complete denture wearers. The objective of the present study was to gather information on these subjects.
Materials and methods
After obtaining the necessary ethical approval, 300 patients at-tending the removable prosthodontic clinic at the Faculty of Dentistry, Jordan University of Science and Technology, for construction of new complete (n=150) and removable par-tial (n= 150) dentures, participated in this study. The data were collected through a structured interview in the form of a questionnaire gathering data about age, gender, income, edu-cation, occupation, frequency of dental visits, knowledge and awareness of DIs, level and sources of information regarding implants, as well as expectation and attitudes toward implant treatment. The pilot-tested questionnaire was based on a thor-ough review of literature on awareness of implants.1,10,18,21-24
Statistical analysis
Data were analyzed using SPSS software version 17.0 (SPSSR:
Inc., Chicago, IL). Frequency distribution and cross-tabulation were produced. In addition, the chi-square test was used for comparisons between removable partial and complete denture wearer groups. Further, multivariate logistic regression model analyses were performed to examine the differences between removable partial and complete denture wearers to determine the factors affecting awareness (difference between implant and other fixed prostheses among partial and complete denture wearers) and level of information about DIs. Adjusted odd ratios (OR) were generated for all significant variables. Significance was set atp<0.05.
Results
Characteristics of denture wearers
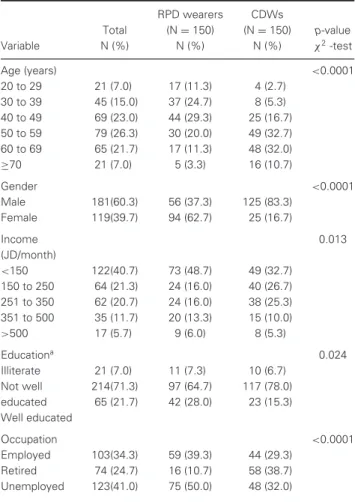
Approximately 26% of the participants (n=79) were between 50 and 59 years, 23% (n = 69) between 40 and 49 years. Sixty percent were male compared to 39.7% female (Table 1). The majority (83.3%) of CDWs were male, while the majority (62.7%) of RPD wearers were female (p<0.05). According to denture status, significantly more RPD wearers were be-tween 20 and 59 years compared to CDWs, where most were
Table 1 Distribution of the study population by prosthesis type accord-ing to age, gender, income, education, and occupation (150 RPD wear-ers; 150 CDWs)
RPD wearers CDWs
Total (N=150) (N=150) p-value
Variable N (%) N (%) N (%) χ2-test
Age (years) <0.0001
20 to 29 21 (7.0) 17 (11.3) 4 (2.7)
30 to 39 45 (15.0) 37 (24.7) 8 (5.3)
40 to 49 69 (23.0) 44 (29.3) 25 (16.7)
50 to 59 79 (26.3) 30 (20.0) 49 (32.7)
60 to 69 65 (21.7) 17 (11.3) 48 (32.0)
≥70 21 (7.0) 5 (3.3) 16 (10.7)
Gender <0.0001
Male 181(60.3) 56 (37.3) 125 (83.3)
Female 119(39.7) 94 (62.7) 25 (16.7)
Income 0.013
(JD/month)
<150 122(40.7) 73 (48.7) 49 (32.7)
150 to 250 64 (21.3) 24 (16.0) 40 (26.7)
251 to 350 62 (20.7) 24 (16.0) 38 (25.3)
351 to 500 35 (11.7) 20 (13.3) 15 (10.0)
>500 17 (5.7) 9 (6.0) 8 (5.3)
Educationa 0.024
Illiterate 21 (7.0) 11 (7.3) 10 (6.7)
Not well 214(71.3) 97 (64.7) 117 (78.0)
educated 65 (21.7) 42 (28.0) 23 (15.3)
Well educated
Occupation <0.0001
Employed 103(34.3) 59 (39.3) 44 (29.3)
Retired 74 (24.7) 16 (10.7) 58 (38.7)
Unemployed 123(41.0) 75 (50.0) 48 (32.0)
aAnswer to this item was recorded according to the following criteria:
Illiter-ate, not well educated (primary school, middle school, secondary school), well educated (university education).
between 40 and 69 years (p< 0.05). According to monthly income, 40.7% had an income less than 150 Jordanian Dinar (JD); this included 32% of CDWs, and 48.7% of RPD wear-ers. Only 5.7% reported to have a monthly income greater than 500 JD. Overall, there was a significant difference between CDWs and RPD wearers for the distribution of monthly income (p=0.013). About 71.3% were not well educated (p<0.05). As for occupation, 41% were unemployed, including 50% of the RPD wearers. Almost 60% reported they visited their den-tist once every 12 months or more (56.7% of RPD wearers and 64% of CDWs) (p<0.05).
Patient information and preferences about DIs
Table 2 Sources of patient information about dental implants (N=300)
RPD wearers CDWs
Total (N=150) (N=150) p-value
Variable N (%) N (%) N (%) χ2-test
1-How did you hear about dental implantsb From relatives and
friends
184(63.4) 84 (58.3) 100 (68.5) 0.072
From dentist 94 (32.4) 56 (38.9) 38 (26.0) 0.019
From media 54 (18.6) 24 (16.7) 30 (20.5) 0.396
From Internet 4 (1.4) 2 (1.4) 2 (1.4) 0.989
2-Level of information about implantsa
0.823
Very well 1 (0.3) 1 (0.7) 0 (0.0)
Well 2 (0.7) 1 (0.7) 1 (0.7)
Moderately well 30 (10.0) 15 (10.0) 15 (10.0)
Poorly 75 (25.0) 40 (26.7) 35 (23.3)
Not at all 192(64.0) 93 (62.0) 99 (66.0)
3-Awareness about the difference between implant and fixed prosthesis
176(58.7) 103(68.7) 73 (48.7) <0.0001
4-Like to have teeth replacedb With removable
appliance
90 (30.0) 22 (14.7) 68 (45.3) <0.0001
With fixed prosthesis 109(36.3) 98 (65.3) 11 (7.3) <0.0001 With implant 126(42.0) 41 (27.3) 85 (56.7) <0.0001
Not replaced at all 2 (0.7) 2 (1.3) 0 (0.0) 0.498
aAnswer to this question was recorded considering the answers provided by
patients for questions 3, 10 to 12, 14, and 16. The answers were numerically coded (scored) and according to the sum of scores, patients were placed in one
of the five categories.
bPercentages for questions 1 and 4 exceed 100%, as multiple answers were
allowed.
88% believed that nonremovable tooth replacements had more advantages relative to removable prostheses, but 11.7% pre-ferred removable prostheses. Only 0.3% felt very well informed about DIs, 64% claimed that they were not informed in any way, 58.7% were aware of differences between DIs and fixed prostheses (68.7% of RPD wearers, 48.7% of CDWs). Com-pared to CDWs, significantly more RPD wearers were aware of the differences between DIs and fixed prostheses (p<0.05). About 45.3% and 14.7% of CDWs and RPD wearers favored removable prosthetic options, respectively. By contrast, 65.3% of RPD wearers preferred to have fixed prostheses. Around 57% of CDWs favored their teeth to be replaced with DIs in comparison to 27.3% of RPD wearers (p<0.0001) (Table 2).
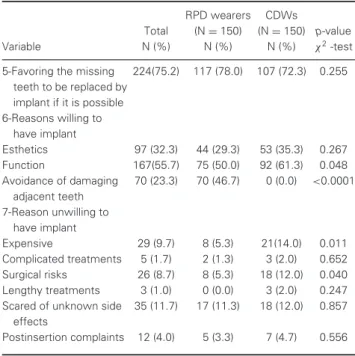
Approximately 75% preferred to replace missing teeth by implants if such treatment was possible, 32.3% for esthetic and 55.7% for functional reasons. Forty-seven percent of RPD wearers preferred having implants to avoid damaging adja-cent teeth, and nearly 25% did not favor implant therapy. Fear of unknown side effects was the major reason preventing pa-tients from choosing implants (11.7%), followed by high costs (9.7%), surgical risks (8.7%), postinsertion complaints (4%), complicated treatments (1.7%), and long treatment times (1%) (Table 3).
Table 3 Level of acceptance of dental implants as a treatment option (N=300)
RPD wearers CDWs
Total (N=150) (N=150) p-value
Variable N (%) N (%) N (%) χ2-test
5-Favoring the missing teeth to be replaced by implant if it is possible
224(75.2) 117 (78.0) 107 (72.3) 0.255
6-Reasons willing to have implant
Esthetics 97 (32.3) 44 (29.3) 53 (35.3) 0.267
Function 167(55.7) 75 (50.0) 92 (61.3) 0.048
Avoidance of damaging adjacent teeth
70 (23.3) 70 (46.7) 0 (0.0) <0.0001
7-Reason unwilling to have implant
Expensive 29 (9.7) 8 (5.3) 21(14.0) 0.011
Complicated treatments 5 (1.7) 2 (1.3) 3 (2.0) 0.652
Surgical risks 26 (8.7) 8 (5.3) 18 (12.0) 0.040
Lengthy treatments 3 (1.0) 0 (0.0) 3 (2.0) 0.247
Scared of unknown side effects
35 (11.7) 17 (11.3) 18 (12.0) 0.857
Postinsertion complaints 12 (4.0) 5 (3.3) 7 (4.7) 0.556
[Percentages for questions 5 to 7 do not equal 100%, because multiple answers were allowed (q6) or some patients chose not to answer (q5 and 7)].
Sixty-one percent reported that they did not know the cost of DI therapy. Eighty-four percent preferred to have implants if the cost of therapy could be covered by dental insurance, 63% were not prepared to pay any amount, with the majority being CDWs (p=0.001). Most participants (83%) were interested in receiving more information about DIs. Dentists were the pre-ferred source (67.7%). A significant difference existed between CDWs and RPD wearers (p<0.05).
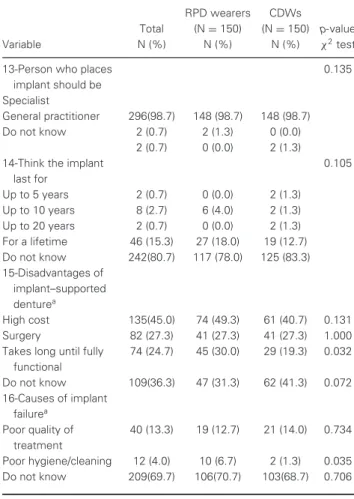
Approximately 78% were not aware if special care was needed for DIs, while only 9.3% thought that DIs required more care than natural teeth. Only 66% believed that patient systemic health was important when considering implant therapy, and 32.3% were not aware of such importance (Table 4). There was substantial agreement between participants that DIs should be provided by a specialist. Most participants (80.7%) had no idea about how long an implant would last, and only 15.3% thought that implants would last throughout a lifetime. High costs were the major reason for not considering DIs (45%), followed by the need for surgery (27.3%). The majority (69.7%) were not aware of any reason for implant failures, while 13.3% believed it was a consequence of poor quality treatment, and 4% related it to poor oral hygiene, with significantly more RPD wearers attributing implant failure to poor oral hygiene than CDWs did (p=0.035) (Table 5).
Sources of patient information
Table 4 Distribution of patients’ level of information about dental im-plants (N=300)
RPD wearers CDWs
Total (N=150) (N=150) p-value,
Variable N (%) N (%) N (%) χ2test
8-Like to know more about implanta
249(83.0) 131 (87.3) 118 (78.7) 0.046
9-If yes, source to get the informationa
Dentist 203(67.7) 110(73.3) 93 (62.0) 0.036
Friends and relatives 20 (6.7) 8 (5.3) 12 (8.0) 0.355 Periodicals, magazine,
etc
28 (9.3) 11 (7.3) 17 (11.3) 0.234
Others 26 (8.7) 13 (8.7) 13 (8.7) 1.000
10-Place of anchoring the implant
0.100
In the gum 34 (11.3) 18 (12.0) 16 (10.7)
In the jawbone 74 (24.7) 29 (19.3) 45 (30.0)
In/on neighboring teeth 0 (0.0) 0 (0.0) 0 (0.0)
Do not know 192(64.0) 103(68.7) 89 (59.3)
11-Ideal hygiene and care of implant
0.300
Cleaned like natural teeth 37 (12.3) 15 (10.0) 22 (14.7) More care than natural
teeth
28 (9.3) 12 (8.0) 16 (10.7)
Do not know 235(78.3) 123 (82.0) 112 (74.7)
12-Systemic health is important when considering implant therapy
0.140
Yes 200(66.7) 108 (72.0) 92 (61.3)
No 3 (1.0) 1 (0.7) 2 (1.3)
Do not know 97 (32.3) 41 (27.3) 56 (37.3)
aPercentages for questions 8 and 9 do not equate to 100%, because some patients
chose not to answer.
who heard about implants from friends were approximately three times more likely to be aware of the difference between the implant and fixed prosthesis compared with patients who did not (OR=3.17).
Participants with an income level of 351-500 JD/month, and more than 500 JD/month had a higher level of information about DIs (OR=13.2, 27.9, respectively). In addition, female participants were about four times more likely to have a higher level of such information (OR=3.7).
Discussion
Similar to Suprakash et al’s study,10the present study used a sample of patients with a wide age range enabling the authors to assess awareness of DIs in different age groups. Reviewing similar studies, one survey randomly approached potential par-ticipants in general public places; others included a representa-tive sample of the general population.9Tepper et al22selected the sample by prestratified multitiered cluster sampling of the general public; another survey was conducted on Indian urban dwellers.19Mgbeokwere et al20used a random sampling among health workers in health institutions, and Pommer et al23,24
in-Table 5 Distribution of patients’ expectations about dental implants (N=300)
RPD wearers CDWs
Total (N=150) (N=150) p-value
Variable N (%) N (%) N (%) χ2test
13-Person who places implant should be
0.135
Specialist
General practitioner 296(98.7) 148 (98.7) 148 (98.7)
Do not know 2 (0.7) 2 (1.3) 0 (0.0)
2 (0.7) 0 (0.0) 2 (1.3)
14-Think the implant last for
0.105
Up to 5 years 2 (0.7) 0 (0.0) 2 (1.3)
Up to 10 years 8 (2.7) 6 (4.0) 2 (1.3)
Up to 20 years 2 (0.7) 0 (0.0) 2 (1.3)
For a lifetime 46 (15.3) 27 (18.0) 19 (12.7)
Do not know 242(80.7) 117 (78.0) 125 (83.3)
15-Disadvantages of implant–supported denturea
High cost 135(45.0) 74 (49.3) 61 (40.7) 0.131
Surgery 82 (27.3) 41 (27.3) 41 (27.3) 1.000
Takes long until fully functional
74 (24.7) 45 (30.0) 29 (19.3) 0.032
Do not know 109(36.3) 47 (31.3) 62 (41.3) 0.072
16-Causes of implant failurea
Poor quality of treatment
40 (13.3) 19 (12.7) 21 (14.0) 0.734
Poor hygiene/cleaning 12 (4.0) 10 (6.7) 2 (1.3) 0.035
Do not know 209(69.7) 106(70.7) 103(68.7) 0.706
aAnswers to these questions to not equal 100%, as multiple answers were allowed
(both 15 and 16) or some patients chose not to answer (q16).
cluded a representative sample of the Austrian population. The definite need for replacement of missing teeth was reported by 98% of participants, similar to Tepper et al’s findings (97%).18 Most participants (>90%) were aware of different treatment options. Similar to earlier studies,21-23 patients showed a high preference for nonremovable replacement approaches (87.7%). This preference could be attributed to the fact that removable denture patients commonly reported dissatisfaction with re-movable dentures, and mostly preferred nonrere-movable pros-theses in replacing their missing teeth, regardless of the clinical situation.21
Reports from Austria showed that the implant awareness rate was 72% in 2003,18and increased to 79% in 2010.23As with the year-by-year increase in the prevalence of DIs and increased patient awareness,23,24 the awareness (96%) among removable denture patients about DIs was higher than that in previous studies.9,21,23,24 Other studies, however, found lower awareness levels (23.24%19and 38%11). In one study, 9.7% of health workers in hospitals were aware of DIs, which could be attributed to the lack of DI provision in those hospitals.20
most CDWs were between 50 and 69 years old, while most RPD wearers were between 40 and 59 years old. Some studies, as here, reported gender differences in patterns of edentulism, with more men becoming edentulous than women.26,27On the contrary, other studies observed no gender differences.29,30
Most study participants belonged to a lower educational sta-tus (71.3%), with a significantly higher educated population among RPD wearers than CDWs. Lower socioeconomic status was associated with a greater risk of oral diseases, more de-mand for prostheses,25,29 and less-regular requests for dental care, leading to more tooth loss and accelerated transition to a completely edentulous state.26,27 The demand for RPDs in-creased with an increase in education level and socioeconomic status.29Conversely, the need for complete dentures decreased with increasing levels of education, and the likelihood of re-taining teeth in the mouth also became higher.29
Berge reported that an age between 45 and 80 and edu-cation at the college level were the most powerful predic-tors of awareness.9 Despite the high awareness rate regard-ing DIs (96%), 64% considered themselves as not totally in-formed about implants, perhaps due to the lower educational status of participants, who were typically the least informed about advances in treatment options.19Higher income (>350 JD/month), similar to the Austrian study,22and female gender were the main factors underlying a higher level of information for this study. This may suggest women’s superior interest over men in health matters,20although a Norwegian study suggested that an age above 45 years and a high educational level were most strongly associated with a high level of information about implants.9
The main source of information about DIs was relatives and friends, followed by dentists. The contribution of media and the Internet to participants’ information was low (1.4%), reflecting limited Internet access and lower educational status. With the increase in Internet access in the future, its role may increase significantly.1The present distribution of information sources is similar to those reported by Berge9and Al-Johany et al.21 However, other studies1,11,19,22,23found dentists to be the main source of information. As suggested previously,21direct per-sonal communication appeared to be an important information source. Nevertheless, for nearly a third of participants, dentists were still the principal source. This source can have a variable influence; dentists who treat patients may not provide informa-tion about DIs if they do not practice implant dentistry.21The low contribution of media as a source of information could be due to the lower educational status of this source compared to that in the developed countries.11
Most patients preferred to have their missing teeth replaced by implants. This was most apparent in CDWs, possibly due to the impact on the quality of life.31-33Fear of unknown side effects was the primary reason for not considering implant treat-ment, followed by high cost and fear of surgery. A German study found that very old age was the most common reason for reject-ing implants,34as patients tended to accept age-related losses of masticatory function35and develop compensatory adaptive processes.36Some patients consider the placement of DIs as a major surgical procedure; this may explain the high fear of un-known side effects.21This reaffirms that dentists should explain
the surgical procedure carefully to their patients and address their worries.23
Overestimating the costs of implants without their prosthetic sets was reflected in the results of the present study. Indeed, most patients were not ready for an additional payment; how-ever, most were unaware of the actual cost of implants. Most preferred to be treated with DIs if they had insurance to pay for it, perhaps due to the poor socioeconomic status of patients, as they attended the Dental Teaching Clinics, seeking inexpen-sive therapy. These findings agree with the study of Pommer et al,23 but contradict the results of a German study, where most patients were prepared for an additional payment, with underestimation of implant costs.1
Most patients believed DIs should be inserted by special-ists, while other surveys reported lower percentages (60%, 44%).22,23 Similar to earlier studies,11,18,19,22 the cost of an implant-supported denture was considered the main disadvan-tage, which was held by 45% of the study population, followed by reluctance of surgery. Implant losses were blamed on the poor quality of treatment provided by 13.3%, similar to Al-Johany et al’s study,21 but contradicted other studies where 47% and 53% blamed dentists for such a failure.1,22Only 4% mentioned poor oral hygiene, while the majority had no idea about potential causes of implant failure.
Approximately 83% of patients were interested in having more information about implants, and about three-quarters pre-ferred to have dentists as the source of such information. This indicates the real need for dental education about implants.21 However, other studies found that interest for more informa-tion was lower than the present findings.22,23Dentists were the preferred source, while those younger than 50 years and living within urban areas turned to the media for more information.22 RPD wearers who wished to have their teeth replaced by DIs were 14.5 times more interested in having more information about DIs compared to CDWs. Tepper at al22 reported that variables such as urban residence, higher professional qualifi-cations, and age above 50 years were positively correlated with awareness about the correct site for implants. Whereas in the present study, income levels greater than 150 JD per month, hearing about implants from the media, and hearing about DIs from friends correlated strongly with knowledge about placing DIs among CDWs. RPD wearers with income more than 500 JD per month were found to be more likely to have such knowledge. Most participants (78.3%) were unaware of implant after-care. Previous studies found that 31% to 61.6% knew that DIs require more care than natural teeth,1,21-23 contradicting the present findings. Only 9.3% of the participants in the present study believed special oral hygiene was necessary for implants, indicating the need for more education on this subject.
Conclusions
References
1. Rustemeyer J, Bremerich A: Patients’ knowledge and expectations regarding dental implants: assessment by questionnaire. Int J Oral Maxillofac Surg 2007;36:814-817 2. Albrektsson T, Zarb G, Worthington P, et al: The long-term
efficacy of currently used dental implants: a review and proposed criteria of success. Int J Oral Maxillofac Implants 1986;1:11-25 3. Albrektsson T, Blomberg S, Branemark A, et al:
Edentulousness—an oral handicap. Patient reactions to treatment with jawbone-anchored prostheses. J Oral Rehabil 1987;14: 503-511
4. Lekholm U, Gunne J, Henry P, et al: Survival of the Br˚anemark implant in partially edentulous jaws: a 10-year prospective multicenter study. Int J Oral Maxillofac Implants 1999;14:639-645
5. Le BT, Follmar T, Borzabadi-Farahani A: Assessment of short dental implants restored with single-unit nonsplinted restorations. Implant Dent 2013; doi: 10.1097/ID.0b013e31829afaf2. 6. Esposito M, Grusovin MG, Polyzos IP, et al: Interventions for
replacing missing teeth: dental implants in fresh extraction sockets (immediate, immediate-delayed and delayed implants). Cochrane Database Syst Rev 2010;9:CD005968
7. Naert I, Koutsikakis G, Duyck J, et al: Biologic outcome of implant-supported restorations in the treatment of partial edentulism. Part I: a longitudinal clinical evaluation. Clin Oral Implants Res 2002;13:381-389
8. Naert I, Koutsikakis G, Quirynen M, et al: Biologic outcome of implant-supported restorations in the treatment of partial edentulism. Part 2: a longitudinal radiographic study. Clin Oral Implants Res 2002;13:390-395.
9. Berge TI: Public awareness, information sources and evaluation of oral implant treatment in Norway. Clin Oral Implants Res 2000;11:401-408
10. Suprakash B, Ahammed AY, Thareja A, et al: Knowledge and attitude of patients toward dental implants as an option for replacement of missing teeth. J Contemp Dent Pract 2013;14:115-118
11. Kaurani P, Kaurani M: Awareness of dental implants as a treatment modality amongst people residing in Jaipur (Rajasthan). J Clin Diagn Res 2010;4:3622-3626. 12. Lekholm U, Gr¨ondahl K, Jemt T: Outcome of oral implant
treatment in partially edentulous jaws followed 20 years in clinical function. Clin Implant Dent Relat Res 2006;8: 178-186
13. Allen PF, McMillan AS, Walshaw D: Patient expectations of oral implant-retained prostheses in a UK dental hospital. Br Dent J 1999;186:80-84
14. Blomberg S, Lindquist LW: Psychological reactions to edentulousness and treatment with jawbone-anchored bridges. Acta Psychiatr Scand 1983;68:251-262
15. Vermylen K, Collaert B, Linden U, et al: Patient satisfaction and quality of single-tooth restorations. Clin Oral Implants Res 2003;14:119-124
16. Annibali S, Vestri AR, Pilotto A, et al: Patient satisfaction with oral implant rehabilitation: evaluation of responses to a questionnaire. Ann Stomatol 2010;1:2-8
17. Babbush C: Post-treatment quantification of patient experiences with full-arch implant treatment using a modification of the OHIP 14 questionnaire. J Oral Implantol 2012;38:251-260
18. Tepper G, Haas R, Mailath G, et al: Representative marketing-oriented study on implants in the Austrian population. II. Implant acceptance, patient-perceived cost and patient satisfaction. Clin Oral Implants Res 2003;14:634-642
19. Chowdhary R, Mankani N, Chandraker NK: Awareness of dental implants as a treatment choice in urban Indian populations. Int J Oral Maxillofac Implants 2010;25:305-308
20. Mgbeokwere U, Okoye L, Ekwueme O: A survey of the knowledge of dental implants as a choice in treatment of edentulous jaws among health workers in government dental clinics in Enugu. Ann Med Health Sci Res 2011;1:91-96 21. Al-Johany S, Al Zoman HA, Al Juhaini M, et al: Dental patients’
awareness and knowledge in using dental implants as an option in replacing missing teeth: a survey in Riyadh, Saudi Arabia. Saudi Dent J 2010;22:183-188
22. Tepper G, Haas R, Mailath G, et al: Representative marketing-oriented study on implants in the Austrian population. I. Level of information, sources of information and need for patient information. Clin Oral Implants Res 2003;14:621-633 23. Pommer B, Zechner W, Watzak G, et al: Progress and trends in
patients’ mindset on dental implants. I: level of information, sources of information and need for patient information. Clin Oral Implants Res 2011;22:223-229
24. Pommer B, Zechner W, Watzak G, et al: Progress and trends in patients’ mindset on dental implants. II: implant acceptance, patient-perceived costs and patient satisfaction. Clin Oral Implants Res 2011;22:106-112
25. Adams C, Slack-Smith LM, Larson A, et al: Edentulism and associated factors in people 60 years and over from urban, rural and remote Western Australia. Aust Dent J 2003;48:10-14 26. Baran I, Ergun G, Semiz M: Socio-demographic and economic
factors affecting the acceptance of removable dentures. Eur J Dent 2007;1:104-110
27. Al-Dwairi ZN: Complete edentulism and socioeconomic factors in a Jordanian population. Int J Prosthodont 2010;23:541-543 28. Moreira Rda S, Nico LS, Tomita NE: Spatial risk and factors
associated with edentulism among elderly persons in Southeast Brazil. Cad Saude Publica 2011;27:2041-2054
29. Esan TA, Olusile AO, Akeredolu PA, et al: Socio-demographic factors and edentulism: the Nigerian experience. BMC Oral Health 2004;4:3
30. Shah N, Parkash H, Sunderam KR: Edentulousness, denture wear and denture needs of Indian elderly-a community-based study. J Oral Rehabil 2004;31:467-476
31. Locker D: Measuring oral health: a conceptual framework. Community Dent Health 1988;5:3-18
32. Reisine ST, Fertig J, Weber J, et al: Impact of dental conditions on patients’ quality of life. Community Dent Oral Epidemiol 1989;17:7-10
33. WHO: International Classification of Impairments, Disabilities and Handicaps. Geneva, World Health Organisation, 1980 34. Muller F, Wahl G, Fuhr K: Age-related satisfaction with
complete dentures, desire for improvement and attitudes to implant treatment. Gerodontology 1994;11:7-12
35. Borzabadi-Farahani A: Orthodontic considerations in restorative management of hypodontia patients with endosseous implants. J Oral Implantol 2012;38:779-791