TO CAP OR NOT TO CAP: CUSPAL COVERAGE INDICATIONS WITH CAD/CAM LITHIUM DISILICATE RESTORATIONS
Elizabeth Griffis
A thesis submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the Department of
Restorative Sciences in the Adams School of Dentistry.
Chapel Hill 2019
Approved by: Taiseer Sulaiman Terry Donovan
ABSTRACT
Elizabeth Griffis: To cap or not to cap: cuspal coverage indications with CAD/CAM lithium disilicate restorations
(Under the direction of Taiseer Sulaiman)
This study was conducted to examine the in vitro fracture resistance of restored
premolars with varying preserved cusp widths, and to determine if functional and nonfunctional cusps have different cuspal coverage indications.
Human maxillary premolars were prepared for IPS e.max CAD onlays. Groups 1-4 preserved a varying amount of the functional or nonfunctional cusp, Group 5 reduced both cusps and Group 6 preserved the functional cusp and included added retentive features. The samples were exposed to simultaneous thermocycling and mechanical loading, and
were examined visually to determine mode of failure.
The difference in percent failure between the functional cusp groups and
nonfunctional cusp groups was statistically significant. No cusp or restoration fractures were observed; all failures were due to debonding of the restoration.
To Matt, my husband. My barista, my cheerleader, my therapist, my everything. Your strengths overshadow my weaknesses. Because of your sacrifice, constant encouragement
and unconditional support, I may chase my dreams.
ACKNOWLEDGEMENTS
I wish to express my deepest gratitude to my thesis committee chair, Dr. Taiseer Sulaiman. Your endless positivity and enthusiasm for innovative dental research was a constant source of motivation throughout the last three years. Without your laboratory
support, literature knowledge and willingness to answer text messages or e-mails at any time, this project would not have been possible. Thank you for empowering me with tools and structure, while still giving me the space to take risks and be intellectually creative in designing and completing this thesis.
I would also like to thank Drs. Terry Donovan, Lee Boushell and Dennis Fasbinder. Your participation on my thesis committee was invaluable. Thank you for challenging my
ideas, sharing your infinite professional wisdom and providing me the space to work through the inevitable complications that arose.
Lastly, I give much appreciation to my close friend Dr. Islam Abd Alraheam. I have truly cherished your partnership in this project and throughout the last three years. Thank you for being a constant voice of reason and logic, and for your dedication and hard work
TABLE OF CONTENTS
LIST OF FIGURES ... viii
LIST OF TABLES ... ix
CHAPTER 1: REVIEW OF THE LITERATURE ... 1
1.1 Introduction ... 1
1.2 The rationale for conservation of tooth structure ... 3
1.3 Tooth colored dental material options for inlays/onlay and relative longevity ... 6
1.4 Lithium disilicate: onlay material of choice ... 12
1.5 CAD/CAM and CEREC for onlay fabrication ... 16
1.6 Onlay preparation design ... 20
1.7 Fatiguing of ceramics ... 26
CHAPTER 2: RESEARCH STUDY ... 29
2.1 Specific aims of this research study ... 29
2.2 The null hypotheses ... 29
2.3 Materials and methods ... 29
2.3.2 Fatigue testing ... 36
2.3.3 Evaluating failure ... 37
2.4 Statistical analysis ... 38
2.5 Results ... 38
2.6 Discussion ... 40
2.7 Limitations of the study ... 46
2.8 Conclusions ... 48
LIST OF FIGURES
Figure 1.1 – Microscopic structure of IPS e.max ... 17
Figure 1.2 – Pascal Magne’s onlay preparation design ... 23
Figure 2.1 – Group preparation designs ... 33
Figure 2.2 – CEREC onlay fabrication sequence ... 35
Figure 2.3 – Mechanical loading pattern of stainless-steel antagonist ... 37
Figure 2.4 – Test specimen mechanical cycles survived ... 39
Figure 2.5 – Group 1 test specimen ... 45
LIST OF TABLES
Table 2.1 – Ivoclar Vivadent Variolink Esthetic DC information ... 36
Table 2.2 – Test group failure rates ... 38
CHAPTER 1: REVIEW OF THE LITERATURE
1.1 Introduction
Modern operative dentistry has experienced a dramatic rise in minimally invasive restorations. Clinicians routinely challenge traditional guidelines that detail the indications
for preparation/restoration design with the goal of conserving as much tooth structure as possible. Further, the development of reliable enamel and dentin adhesive techniques and ceramic materials with improved physical properties has led to a significant increase in the utilization of ceramic restorations.1
For the last fifty to one hundred years, porcelain-fused-to-metal (PFM) or all metal restorations have been the dominant treatment options when large restorations were
needed. Further, PFM restorations have historically been the most common type of esthetic indirect restoration used in dentistry.1 In addition to the rising cost of noble metal alloys, the development of posterior adhesive restorations has been fueled by the growing demand of patients for esthetic and metal-free restorations and the desire of clinicians to
use tissue-preserving materials. These motives led to the “biomimetic principal”, which is based on maximum dental tissue preservation and sound biomechanics. The goal of this treatment philosophy is to use “tooth-like” restorative materials, such as composite and ceramic, in combination with hard tissue bonding to enamel and dentin to replace only the
The heavily debated theory that a tooth is strengthened from a bonded restoration, and the reduced need for dental hard tooth preparation have even fueled a shift in many dental school curricula away from dental amalgam and traditional “G.V. Black” preparation principals to adhesive dentistry which utilizes composite resin and ceramic.3
In alignment with this clinical philosophy, ceramic onlays are now considered viable
alternatives to complete coverage crowns, with greater than 90% success at 10 years.4 Traditional onlay preparation guidelines suggest to “cap a cusp if the extension is two-thirds or greater than the distance from any primary groove to the cusp tip”.5 Another conventional onlay preparation guideline advises cuspal capping “if the tooth preparation involves more than two-thirds of the intercuspal distance”.6 These protocols were
supported with the 1981 classic research study by Larson et al. which concluded that restorations that encompass just one-third of the intercuspal distance reduce the tooth’s resistance to fracture by more than one half.7 Restorative materials that utilize adhesive dentistry, in particular fracture resistant ceramics, have greatly improved since 1981.
However, cuspal coverage guidelines, even when considering modern restoratives, have remained the same.
A recent etchable glass ceramic, a lithium disilicate glass ceramic material (IPS e.max) was introduced by Ivoclar Vivadent and was recommended for use as anterior or posterior crowns, implant crowns, inlays, onlays and veneers.8 IPS e.max CAD blocks
retrospective clinical research study by Fabbri et al. reported cumulative survival rates of lithium disilicate onlays ranging from 97.86% to 100% over an observational period of 12-57 months.10 Lithium disilicate may therefore be a reliable material for
ceramic onlays. However, the manufacturers fail to provide guidelines as to
when onlay cuspal coverage is indicated.11
Research studies focusing on cuspal coverage indications using modern restorative materials are sparse. The few published research studies that evaluated the effect of remaining cusp thickness on fracture rates did not use lithium disilicate ceramic onlays. Additionally, these research studies did not compare possible differences in preparation design of the functional versus nonfunctional cusps.12-13 Therefore, the overall objective
of the proposed study was to examine the in vitro fracture resistance of restored premolars with varying preserved cusp widths, and to determine if functional and nonfunctional cusps have different cuspal coverage indications.
1.2 The rationale for conservation of tooth structure
Conservation of remaining tooth structure may be essential to the vitality, function
and esthetics of a tooth. The enamel and dentin help to protect the pulp from injury. Therefore, loss of either due to caries or mechanical means may pose a threat to the pulp and ultimately the vitality of the tooth. The use of rotary diamond and carbide cutting instruments exposes the pulp to heat generation, mechanical vibration, desiccation and loss of dentinal tubule fluid. Odontoblast processes that extend into dentin tubules may also be
is only slight or moderate, the pulpal response is protective and localized. Conversely, a pulpal necrosis may occur in cases of severe injury or destruction.5
During tooth preparation, the enamel and dentin act as good thermal insulators and, along with heat dissipation properties of pulpal vascularity, help to limit temperature rise and afford protection to the pulp. This thermal insulating capacity is dependent on the
remaining hard tissue thickness. The remaining tissue is effective in protecting the pulp in proportion to the square of its thickness.5 The longer the time of cutting and the higher the local temperature produced, the greater the potential for thermal trauma. A more extensive tooth preparation, such as a traditional full coverage crown, may require a longer cutting time and therefore a higher local temperature is potentially produced. In a research study
by Zach and Cohen, the pulps of 15% of primate teeth subjected to intrapulpal temperature increases of 10°F failed to recover and suffered necrosis, and a rise of 17°Fresulted in 60% pulpal necrosis. 14 A similar canine study also found teeth exposed to excessive heat
showed marked odontoblastic cell body aspiration into the adjacent dentinal tubules as
well as thermal coagulation (denaturing) of odontoblasts and adjacent tissue. The amount of pulpal injury correlated to the thickness of remaining dentin; i.e. the thicker the
remaining dentin, the less the likelihood of pathologic changes (as assessed by histology) that occurred in the pulp.15 Extensive tooth preparation involves a greater number of
In addition to the threat of overheating the pulp, crown preparation subjects the pulp to the risk of vascular stasis, thrombosis, reduced blood flow and internal bleeding.18 Exposed dentinal tubules communicate directly with the pulp. Deep dentin has increased permeability, which makes it particularly vulnerable to chemical, physical and microbial
irritants.14 The more dentinal tubules that are exposed, the higher the microbial threat is that is presented by the oral flora. These threats can illicit irreversible inflammatory changes that may result in progressive pulpal necrosis.19 It may be expected that these reactions would be more severe in tooth preparations where higher numbers of dentinal tubules are exposed, hence the potential pulpal advantage of more conservative onlay preparations that preserve enamel-covered dentin.
A full 360° crown preparation, infamously known as “the circle of death”, is often the culmination of a long history of restorative procedures and associated insults to a tooth. It is uncertain how many teeth lose vitality as a direct result of crown preparation due to the multitude of other variables a tooth is exposed to. Bergenholtz and Nyman’s study
suggested 9% of crowned teeth lost vitality during long-term review.20 In a review, Felton et al. found 13.3% of teeth restored with full coverage crowns lost vitality in the long term compared to 0.5% of unrestored controls.21 In a Scottish subpopulation, Saunders and Saunders found that 63% of adult patients had at least one tooth with a full coverage
The desire to “do no harm” and to avoid patient pain, swelling and suffering, which often accompanies pulpal pathology, should be sufficient justification to try to preserve healthy pulp tissue. However, maintaining intact tooth structure offers additional benefits. A conservative onlay preparation that retains any remaining cusps not only aims to sustain
a healthy pulp, but also to preserve a tooth’s natural hues and shades. For example, a much more esthetic result can be achieved by leaving the natural buccal cusp intact. Additionally, if portions of the cusps are preserved, they can be used as a guide for the final restoration to uphold the intracoronal geometry and location of the tooth in the arch. Smaller tooth preparations result in restorations that have less effect on intra-arch and inter-arch
relationships and esthetics.5 Preserving healthy tooth structure can serve as a blueprint for
replicating tooth shade, anatomy and occlusal function. Ultimately, a conservative onlay may prolong the lifespan, and be more likely to reproduce the natural function and esthetics of a restored tooth.
1.3 Tooth colored dental material options for inlays/onlays and relative longevity
Indirect tooth-colored restorations may be considered for large class I and II restorations that have undermined the strength of the remaining cusps.5 Preliminary in vitro studies supported the idea that use of an adhesive restoration may offer increased strength to the remaining tooth structure. Several of these studies have examined the so-called “cusp reinforcement” ability of a restoration when enamel and dentin bonding are
cusp under occlusal forces in restorations bonded by the acid-etch technique showed significantly less hysteresis and strain compared to non-bonded restorations.24 Similarly, the use of bonded restorations has produced higher fracture resistance in premolars restored with MOD restorations compared to non-bonded restorations.25-26 Further, in
Camacho et al.’s experiment on the fracture strength of restored premolars, MOD cavity preparations restored with ceramic restorations presented the highest values for fracture strength and were similar to the unprepared control group. Teeth restored with bonded composite restorations showed fracture strengths inferior to the ceramic restorations but still significantly higher than fracture strength of non-bonded amalgam restorations.27 It is important to note that none of the aforementioned studies subjected their samples to
artificial aging or fatiguing. Additionally, there is no clinical evidence available that
indicates that a tooth is strengthened due to adhesive bonding of a restoration. Over time, mechanical and chemical deterioration occurs which may compromise the longevity of the dentin bond due to enzymatic degradation of the exposed collagen fibrils and hydrolytic plasticization of the polymer matrix.28-29 However, a restoration that utilizes enamel
bonding in addition to dentin adhesion may be less subject to time dependent degradation of the hybrid layer. In Friedman’s 15-year review of porcelain veneer failure, over 3,500 restorations were evaluated. Overall, the success rate was an impressive 93% with ceramic veneers, which rely on bonding alone for retention. In examining the failures, microleakage and debonding of a ceramic veneer was common when the preparation was devoid of
reasonable to expect an inlay or onlay will have a successful outcome in terms of retention and resistance to microleakage. Therefore, it may be unnecessary to extend a preparation for the sole purpose of G.V. Black’s retention form, and a more conservative preparation may be sufficient.
Glass-ceramic, as opposed to composite resin, is recommended when excessively
worn, non-vital or fractured teeth present.27 Composite resin may be chosen for small to moderate sized restorations, however larger restorations including onlays should be restored with ceramic. Ceramic restorations have shown to have better marginal
adaptation, color match, wear resistance, anatomic form and survival probability compared to composite resin.31 Several clinical studies have shown that indirect glass-ceramic
restorations perform better than indirectly fabricated composite resin restorations as well. In a three-year clinical evaluation of composite resin and leucite reinforced ceramic inlays, 100% of the ceramic inlays and 89% of the composite resin inlays were assessed to be clinically excellent or acceptable. In this study, ceramic inlays revealed significantly better
“anatomic form of the surface” and “integrity of the restoration”.32 The higher wear
resistance and strength of ceramic inlays can explain this clinical finding.33-34 In Mangani et al.’s systematic review on the clinical success of indirect restorations in posterior teeth, a combined total of 5,858 indirect glass-ceramic and composite resin restorations were
longitudinal, controlled clinical studies and retrospective cross-sectional studies were evaluated, it was found that indirect restorations exhibited a significantly lower annual failure rate than direct techniques, and that indirect ceramic restorations performed better than indirect composite resin restorations.36 This clinical evidence is in support of the use
of ceramic materials for large esthetic indirect restorations.
Etchable dental ceramics consist of a composite structure of a crystalline phase or phases within a glassy matrix. The initial use of conventional dental ceramics, such as feldspathic porcelain, revealed several mechanical and physical property shortcomings of the available materials of the time. Although dental ceramics have high compressive strength, they exhibit low tensile strength, do not resist crack propagation, demonstrate
increased brittleness, have increased bulk fractures of the restorations and lead to
excessive wear of opposing teeth.37-40 Over the past three decades, several newer ceramics have been developed to address these deficiencies through improvement of the durability of these dental materials in the oral environment.
Ceramic inlays and onlays have become increasingly popular for several reasons. Aside from patients’ increased esthetic demands, increased use has resulted from improvements in the following: 1) material properties, 2) fabrication techniques, 3) adhesives, and 4) resin-based cements. Glass-ceramics may be etched with hydrofluoric acid and salinized to achieve a strong and durable bond via composite resin cement to
porcelain, leucite reinforced, and lithium disilicate ceramic materials are available for use with either chairside or laboratory CAD/CAM systems.5 Overall, the most common clinical failure modes for ceramic restorations, regardless of the manufacture system used, appears to be bulk fracture and marginal deterioration.41
Traditional feldspathic porcelain inlays and onlays are less popular today than in
the past, despite having a low start-up cost for dental laboratories. Historically, fabricating these restorations was technique sensitive and involved firing the porcelain on refractory dies. They required gentle handling during try-in and bonding to avoid fracture. In
addition, feldspathic porcelain restorations were relatively weak potentially resulting in a high incidence of fracture.42 Smales and Etemadi followed patients with feldspathic
porcelain onlays over a 6-year period. Over this time, 26.9% of the onlays failed primarily due to bulk fracture.43 In another clinical 6-year follow up, van Dijken et al. found that 12% of feldspathic porcelain ceramic inlays luted with dual-cured resin composite failed and 26% of inlays cemented with conventional glass ionomer cement (GIC) failed. The main
reason for failure was partial fracture or loss of the inlay. This study illustrated a relatively high and increasing failure rate over 6-years. Additionally, because the failure rate was higher in the GIC group, it may be concluded that ceramic restorations are more successful when supported a resin cement bond to the supporting tooth structure.44 Finally, Hayashi
et al. examined the clinical performance of feldspathic porcelain inlays after eight years. Eighty percent of the restorations survived after eight years, although it was 92% at six years. The authors noted that 77% of the restorations suffered from marginal
Pressed glass-ceramics have demonstrated improved clinical durability compared to feldspathic porcelain inlays made on refractory dies.36,45-46 These ceramics are modified with nucleating agents that, when treated with heat, develop organized leucite crystalline structure with increased resistance to fracture propagation. IPS Empress (Ivoclar
Vivadent) is a leucite-reinforced ceramic restoration fabrication system that has been available since 1990. In this system, molten ingots of leucite reinforced glass ceramic are pressed into refractory molds, fabricated using the lost-wax method, in order to create well-fitting ceramic inlays, onlays and crowns. Several clinical trials have examined the clinical longevity of IPS Empress inlays and onlays. One of the longest controlled clinical trials using leucite reinforced glass ceramic was conducted by Frankenberger et al. IPS
Empress inlays and onlays bonded with either light-cured or dual-cured resin cement were followed for 12 years. The failure rate was 12% at 12 years, mostly due to bulk fracture. Significantly more bulk fractures were found when light-curing composite resin was used for luting. Interestingly, 15% of the restorations had proximal margins located below the CEJ in dentin, however none of these restorations developed recurrent caries or failed.47
Van Dijken and Hasselrot conducted a 15-year evaluation of extensive dentin-enamel bonded IPS Empress partial and complete coverage restorations. In this clinical trial, the authors included 2 groups of patients with onlay restorations. Preparation Group 1 had no shoulder preparation and preserved a thin remaining cusp wall, even if the clinician believed it was at risk for fracture. Preparation Group 2 also preserved a thin remaining
failure. Interestingly, most failures were due to restoration loss or fracture. Only 1 tooth in the entire study experienced a cuspal fracture. Overall, the cumulative failure for all the groups was 24% after 15 years.48
Although pressed leucite reinforced ceramic inlays and onlays appear to have a lower failure rate compared to feldspathic porcelain inlays and onlays, ceramic fracture
continues to be the leading cause of failure.51 Ceramic inlays/onlays continue to suffer from some material related shortcomings. However, their success rivals the longevity of
traditional porcelain-fused-metal full coverage crowns, which meta-analysis has shown between 69%49and 74%50 survival rates at 15 years.
1.4. Lithium disilicate: onlay material of choice
Given that the most common reason for ceramic restoration failure is bulk fracture, dental materials manufacturers have continued to develop newer ceramic formulations with improved mechanical properties. In 1988, Ivoclar Vivadent first introduced lithium disilicate (2SiO2-Li2O) dental ceramics for use as a heat pressed core material. This material was named IPS Empress 2 and was a particle filled glass ceramic that contained
approximately 70% crystalline lithium disilicate filler. The lithium disilicate crystals functioned to minimize microcrack propagation. This material used a pressure casting procedure that resulted in a material with less defects (voids) and more uniform crystal distribution.52 The resultant flexural strength and fracture toughness of IPS Empress 2 (lithium disilicate) was improved by a factor of more than three in comparison with IPS
CAD/CAM use. Quartz, lithium dioxide, phosphor oxide and other components are included in IPS lithium disilicate. The low thermal expansion that occurs during processing of this formulation results in a glass ceramic that is thermal shock resistant. The pressable form of lithium disilicate is sold as ingots that are optimally manufactured to prevent defects
through simultaneous nucleation of two different crystals. The ingots are heat pressed in a porcelain furnace to mold the ceramic material into the desired shape. This technique has been shown to improve mechanical stability by reducing processing errors associated with conventional sintering.54 The final microstructure consists of 70% needle-like lithium disilicate crystals embedded in a glassy matrix. The crystals are approximately 3.0-6.0 μm in length.55
These lithium disilicate materials are marketed for use as either monolithic restorations or core materials to be veneered.56 Typically, monolithic restorations are stronger than layered restorations, but the layered lithium disilicate may provide more esthetic restorative outcomes. Therefore, the layered restorations are indicated for
anterior teeth, while monolithic lithium disilicate is better suited for posterior units.46
Lithium disilicate crowns may be luted in a traditional manner with a retentive preparation or may be etched and adhesively bonded with contemporary conservative non-retentive preparations such as for onlays or partial veneer preparations.46 For adhesively bonded lithium disilicate restorations, the intaglio surface is typically etched
compared to conventional cementation with glass-ionomer cement.57-58 Further, when compared to leucite-reinforced ceramic, lithium disilicate ceramic has been shown to have significantly higher microtensile bond strengths to composite resin with the same surface treatments.59
Monolithic lithium disilicate materials demonstrate a flexural strength of around
400Mpa while layered lithium disilicate is slightly weaker.60 This is a significant
improvement from feldspathic porcelain, which shows a flexural strength of approximately 90Mpa and leucite-reinforced ceramic’s flexural strength of 140Mpa.46 From this data, it can be concluded that monolithic IPS e.max restorations may be roughly five times
stronger than those made from traditional feldspathic porcelains, which may contribute to
extremely low clinical fracture rates.55
Due to increasing costs of precious metals (gold, platinum, palladium) the primary driver for contemporary ceramic materials is cost savings. The laboratory costs for contemporary ceramic restorations are substantially lower than for metal-ceramic
restorations. According to Glidewell (Glidewell Laboratories, Newport Beach CA, USA), a major dental laboratory, in 1997 72% of restorations produced were porcelain fused to metal. In 2010, this number dropped to 45%, while 50% of the restorations were all ceramic or resin-based composite restorations (including 12% lithium disilicate
restorations).61 Of considerable concern is the fact that most of these systems have been
brought to market with very limited independent clinical testing.46
three-unit fixed partial denture in the anterior, premolar and posterior region.62 A systematic review by Pieger et al. examined the clinical performance of lithium disilicate single crowns and fixed partial dentures. The 2-year cumulative survival rate for single crowns was 100%, and the 5-year cumulative survival rate was 97.8%. One study that
included 10-year data found the survival rate for single crowns was 96.7%. Unfortunately, the 2, 5 and 10-year cumulative survival rate for fixed dental prosthesis was only 83.3%, 78.1% and 70.9% respectively.63 Fabbri et al. published a clinical evaluation of 860 lithium disilicate restorations including crowns, veneers and onlays with an observations period of 3-6 years. The cumulative survival rates for all lithium disilicate restorations ranged from 95-100%. Sixty-two onlays were included in the study, reporting 99% cumulative survival
rate through a follow-up range of 12-57 months.64 Valenti and Valenti’s retrospective clinical analysis of 261 lithium disilicate crowns found an overall survival rate of 95.5% after 10 years, with chipping and ceramic fracture leading to all failures.65 Finally, a
retrospective clinical study examining 43 partial and complete crowns found a cumulative survival rate of 97.7% for up to 81 months. The two failures were due to fracture and
chipping of the ceramic.66
Long-term randomized, controlled clinical trials are lacking that evaluate lithium disilicate’s use for onlay restorations. In an effort to evaluate the clinical performance of
remained with their original practice and that bulk fractures were not deemed therapeutically inconsequential) that in the medium-term, IPS e.max onlays do not experience a high rate of catastrophic failure. Therefore, in alignment with the prevailing philosophy of minimally invasive dentistry, it is clear that many teeth may be effectively
restored with partial coverage e.max restorations. This treatment alternative is now a viable alternative to traditional full coverage crowns for teeth in need of indirect restorations.
1.5. CAD/CAM and CEREC for onlay fabrication
Over the last two decades, the use of computer-aided design computer-aided
manufacturing (CAD/CAM) systems in dentistry has increased dramatically. The CAD/CAM approach may provide a solution to the numerous subjective errors the traditional way of manufacturing restorations is prone to. Despite the advantages of conventional laboratory manipulation and precise shaping, there are inherent drawbacks related to thermal
sensitivity (the high coefficient of thermal expansion of the wax), time consuming and
technique sensitivities of the lost wax-method.68 CAD/CAM technologies may provide a precise, efficient and accurate means by which to produce high-quality dental restorations.
Mormann and Brandestini developed the first commercially available CAD/CAM system in 1985 known as the CEREC (CEramic REConstruction) 1. This chairside system enables single visit appointments by allowing the dentist to independently design and machine indirect dental restorations in a matter of hours.69 The success rate of feldspathic
Presently, the Charlotte, N.C. based Dentsply Sirona CEREC system is one of the most popular chairside CAD/CAM systems currently available. Modern technologies have vastly improved the system performance as compared with the original CEREC 1. Currently its restorative capabilities include but are not limited to inlays, onlays, crowns, fixed denture
prostheses, custom implant abutments and restorations, implant surgical guides, etc. With a clinically relevant variety of milling materials and sophisticated milling machines
available, the dental in-office applications for CEREC are constantly expanding.
Several categories of restorative materials are available for use with the CEREC system. Solid block glass-ceramics available include feldspathic porcelain,
leucite-reinforced and lithium disilicate. These glass-ceramics allow the restoration to be etched
and adhesively bonded for retention to the tooth. Composite resin materials are also available, however ceramic blocks are the primary material used for chairside CAD/CAM restorations.71
Figure 1.1. IPS e.max Press (left) and IPS e.max CAD containing lithium disilicate crystals of 3.0-6.0μm and 0.8-3.0-μm, respectively56
360-400MPa, higher than any other chairside CAD/CAM material available at the time. IPS e.max CAD comes initially prepared in its so called “blue state” which contains
approximately 40% crystals by volume, consisting of 0.2-μm to 1-μm lithium meta-silicate (Li2SiO3) crystals in a glassy phase along with lithium disilicate nuclei. This partially
crystallized form of the ceramic offers high edge stability and is easier to mill, resulting in lower bur wear of the milling machine.72 The final lithium disilicate restoration is formed after the milling process in completed and the material is glazed and heat-treated in one step. The material fully crystallizes after being tempered at 850°C for 20-25minutes under a vacuum. The manufacturer literature states that fully crystallized IPS e.max CAD
produces a microstructure of 70% fine grain lithium disilicate crystals, ranging in size from
0.8-μm to 3.0-μm (Fig 1.1).56 It has been reported that there is a level of uniform porosity in the final ceramic.73 Size, volume fraction and distribution of the crystalline structure are known to play a significant role in the mechanical and chemical properties of any ceramic material. This unclear relationship continues to be studied for lithium disilicate as the exact correlation between microstructure and mechanical properties has yet to be determined.
Notably, the manufacturer reports that IPS e.max press demonstrates a slightly higher biaxial flexural strength and fractures toughness compared to IPS e.max CAD.56 However, the use of a chairside CAD/CAM system with e.max CAD allows the dentist to avoid multiple appointments and the use of provisional cements (which may compromise dentine
adhesion).75 Nonetheless, IPS e.max CAD has seen increased use over several years due to
its esthetic nature, impressive strength and ease of use.62
showed 100% survival and did not find any indication of crown fracture, surface chipping, poor marginal adaptation or recurrent caries.75 One 10-year study showed 83.5% survival rate of monolithic single unit crowns, although only 26 crowns were available for
examination after this time period.76 Finally, laboratory clinical data was examined in one
systematic study to determine projected survival rates of various CAD/CAM all ceramic restorations. Of significance was the finding that IPS e.max CAD restorations showed a trend of decreasing survival with increasing restoration size. That is, IPS e.max CAD crowns performed statistically significantly worse than both onlays and inlays (P = 0.0313 and P = 0.0002, respectively). Additionally, for both onlays and inlays, e.max CAD showed higher survival rates than Empress CAD (leucite-reinforced ceramic). In total, 48 fractures
occurred out of 6,743 e.max CAD onlay restorations over the short-term study period of 3.5 years, equating to a total failure rate of 0.7%.77
Marginal fit is an important factor in the success of dental restorations. Marginal gap is defined as the vertical distance from the internal surface of the restoration to the finish
line of the preparation.78 There is no evidence-based consensus regarding what specific marginal gap may be clinically acceptable. Some authors suggest that a marginal fit of <120μm is clinically acceptable.79 In the 1960’s, the American Dental Association suggested an ideal marginal fit between 25 and 40μm was the clinical goal80, however achieving these
levels is clinically difficult.81 Critics claim that restorations produced with CAD/CAM
statistically significantly smaller marginal gaps than those fabricated with the CAD technique. However, the restorations across all groups achieved marginal gaps within a clinically acceptable range.82 A study comparing the marginal fit of pressed vs. CAD/CAM lithium disilicate crowns found that while the pressed crowns had significantly smaller
marginal gaps, both groups were in the clinically acceptable range, which was considered less than 50 μm.83 Another study examined the internal fit of lithium disilicate crowns. The results suggested that pressed or milled IPS e.max crowns fabricated from a digital
impression demonstrated better internal fit compared to those fabricated from polyvinyl siloxane (PVS) impressions.84 An alternate view, concluded by one author, is that
preparation quality has a major impact on the marginal gap of crowns fabricated with a
CAD/CAM system. The mean marginal gap was 38.5μm for crowns fabricated from ideal preparations, while preparations categorized as poor averaged a marginal gap of 90.1μm.85 The marginal fit of a milled restoration is therefore highly dependent on the mill’s ability to replicate the irregularities of the preparation margin.
In light of these considerations, the number of CEREC users continues to grow year by year. The accuracy in the acquisition and milling process has been steadily improved through continuous research and development in both hardware and software. With over 40,000 users worldwide, many dentists are considering this system a viable alternative to
traditional procedures.69
1.6. Onlay preparation design
preparation may remove up to 75% of dental tissue, while an inlay or onlay preparation may remove as little as 20%.86 The strength of the remaining tooth structure decreases as the width and depth of the tooth preparation increases, increasing the risk of fracture of the tooth.87
Two main factors may predispose teeth to fractures or cracks. First, there are
anatomical features such as the limited dentinal support of the non-functional cusps of posterior teeth and the steep cusp/fossa of maxillary premolars that increase fracture risk during clenching or bruxism. Secondly, loss of dentinal support of the cusps through caries lesion development along with subsequent extensive cavity preparations may increase the risk of tooth fracture. For example, a large mesial-occlusal-distal preparation may
jeopardize the integrity of the tooth by decreasing the amount of sound dentin structure joining the facial and lingual cusps, especially if the tooth is subject to excessive occlusal stresses.88
In a report on overall incidence of complete cusp fractures by Bader et al., it was
revealed that complete fracture rates were 8.0 posterior teeth per 100 adults per year. Molar cusps fractured with higher frequency than premolar cusps. In mandibular teeth, the lingual cusps fractured twice as frequently as the facial cusps, while the opposite was true for the maxillary teeth.89 This survey supports the conclusion that the nonfunctional cusps fracture with higher frequency than functional cusps. Cuspal anatomy may contribute to
excursive movements and closure forces. In an examination of stress distribution in posterior teeth, Magne et al. found that during working and nonworking micromotions, functional cusps were generally well protected and subjected to compressive stresses, while nonfunctional cusps tend to exhibit more tensile stresses.90
More conservative bonded restorations have been advocated to treat fractured
teeth as opposed to a full crown restoration. As previously referenced, various studies favor bonded restorations to increase the strength of a prepared tooth by adhesively stabilizing the remaining tooth structure. Thus, the use of esthetic partial coverage
restorations such as inlays or onlays, have increased because they provide a conservative and esthetic option that requires minimal tooth preparation, and therefore helps to
preserve the tooth’s remaining structural integrity.4,91 The common clinical dilemma regarding inlay and onlay restorations relates to cavity design. Specifically, there is
confusion amongst dentists regarding occlusal isthmus width and remaining cusp thickness and especially with regard to the clinical decision to reduce and overlap the cusp with the
Figure 1.2. Pascal Magne recommends at least 2mm at the base of any remaining cusp.
The extent of the caries, demineralization of adjacent enamel and discoloration of tooth structure that may negatively affect the esthetics and geometry of the final
restoration may initially guide the inlay or onlay outline form.One of the biggest advocates
of the “biomimetic principal”, Dr. Pascal Magne, suggests, “thin, isolated remaining cusps (<2mm at the base or when the occlusal margin is located at the cusp tip) should be covered to ensure a 2mm overlap of restorative material” (Figure 1.2). Any proximal or occlusal extensions should be kept as minimal as possible and may be placed in contact areas.2 However, this assertion is not based on any in vivo, clinical evidence.
A few laboratory studies have attempted to analyze contemporary onlay
preparation designs with regards to when cuspal reduction and coverage is indicated. Yoon et al. prepared two widths of occlusal isthmus (75%, 100% of intercuspal distance) and three designs of cuspal coverage (none, palatal, complete) on maxillary premolars. The inlay/onlay preparations were restored with milled lithium disilicate and statically loaded
showed no statistically significant difference depending on designs of cuspal coverage.93 This study’s major shortcoming was that there was no attempt to fatigue the test
specimens in a wet environment, which may contribute to the development and growth of cracks in ceramic and lead to their failure, therefore its results must be interpreted with
caution.94-95 Shibata et al. studied the influence of surrounding wall thickness on the fatigue resistance of molars restored with feldspathic porcelain inlays. Groups of 2.0mm, 1.5mm, 1.0mm and 05.mm buccal and lingual wall thicknesses were preserved, and after being restored with feldspathic porcelain inlays, were subject to increasing forces in a staircase-aging technique, with up to 185,000 mechanical cycles in a chewing simulator. All
specimens survived the fatiguing protocol, leading the authors to conclude that remaining
tooth wall thickness does not influence the fatigue resistance of molars restored with CAD/CAM ceramic inlays.96 However, this study also displayed a few shortcomings. For example, the fatiguing protocol exposed specimens to a constant water temperature of 37°C. The use of fluctuating water temperatures may accelerate the aging process and also represents clinical conditions more accuracy. Also, 185,000 cycles represent less than a
year of clinical use, which is an extremely short time period used to accurately evaluate the longevity of ceramic restorations.97 Lastly, lithium disilicate, in comparison to feldspathic or leucite reinforced porcelain displays the highest fracture resistance among the glass ceramic systems used for onlay restorations.91
compressive force only and is not representative of the clinical environment.90 All ceramic restorations are clinically subjected to complex intraoral forces. Magne et al.’s study on premolar cuspal flexure as a function of restorative material and occlusal contact location used software to conduct finite element analysis so as to observe if occlusal loading in
either enamel, at the restoration margin, or in the restorative material caused more cuspal widening. The research study found occlusal contact on the restoration demonstrated the least amount of cuspal deformation and occlusal contact at the restoration margin
demonstrated the most cuspal deformation. Cuspal deformation of composite resin inlays and ceramic inlays were also compared. It was concluded that the ceramic inlays provided a cusp stabilizing effect when compared to the composite resin inlays.98
Patient occlusal pathology, tooth morphology, remaining cusp width, final occlusal margin location and material selection may all be important factors to consider when designing ceramic partial coverage restorations. Nonetheless, the need for classic means of retention, with respect to taper, height of the preparation, and circumferential margins,
may be dramatically reduced for restorations bonded to tooth structure. Dentin and
enamel bonded ceramic restorations may be expected to have a major advantage in clinical circumstances of minimal or no retention. Traditional crown preparation techniques will in these cases occasionally involve extensive preparation and/or prescriptive endodontic
treatment, in combination with a post or pin(s) and core placement in order to obtain retention. The minimal preparation for the bonded ceramic restoration is less traumatic for the tooth, which ultimately may help maintain pulp vitality. There are currently no
1.7. Fatiguing of ceramics
The best method to determine the clinical performance of ceramic material or
preparation design is to conduct a randomized controlled clinical trial. However, it is costly, involves ethical approvals and the process from study inception to article publication of a five-year clinical trial may take up to ten years.46 In vitro dynamic fatigue testing of ceramic
materials under water may be the best laboratory substitute for in vivo testing. However, there is no conclusive guidance on the testing parameters and standardization of such testing has yet to be determined in the literature94.
Clinically, all-ceramic restorations are subjected to complex intraoral forces. They
are loaded repeatedly in the presence of water with sub-critical masticatory loads for an average of 500,000cycles/ year109. An aqueous environment may reduce the number of cycles to produce fatigue failure in glass ceramics by causing microstructural degradation in highly crystalline materials at relatively low temperatures100. Periodic tension and compression that occur at leading edge of a ceramic fracture, as a result of thermocycling,
further escalates the level of damage. The combination of cyclic loading in fluctuating chemical and thermal conditions results in a reduction of the mechanical properties of ceramic101. Damage accumulates from repetitive contacts between maxillary and
mandibular teeth and, ultimately, the survival probability and lifetime of the restoration(s) is reduced.
In vitro studies that utilize static loading and one-cycle load-to-failure tests, known
this testing may provide information on material strength, or be useful as a means to compare different materials, it is inadequate to predict the long-term performance of dental materials during clinical service. On the contrary, dynamic fatigue studies may represent a more clinically relevant approach to analyze the mechanism of failure of
ceramics.94 Clinically, mechanical failure of ceramic restorations occurs after many years in service, which indicates fatigue failure not acute overload.102 Laboratory testing should attempt to mimic different aspects of the oral environment so as to produce failure modes similar to those seen clinically.94 Unfortunately, long-term fatigue studies require expensive and technologically advanced machinery, and may be time intensive.
A variety of testing parameters are involved in fatigue testing machines. For
example, there are a wide range of loading forces, number of cycles, loading frequency, antagonist material, periodontal ligament simulation, wet/dry fatigue, thermocycling, abutment material and vertical and lateral movement.100 Variation in all of these parameters has the ability to drastically affect the results of an experiment.
Loading force is an important parameter that can have an impact on the mechanical behavior of a loaded object in fatigue. The position of a restoration in the oral cavity
determines the load it may receive during service.103 During normal masticatory function, an occlusal load between 10 and 120N is considered within normal range and adequate for chewing.104 The force range used in laboratory fatigue and mechanical chewing simulation
Chewing rates in humans is consistently reported in the literature as below 2Hz.110 In Nawafleh et al.’s systematic review on lithium disilicate fatigue testing parameters, sixteen of the nineteen studies reviewed applied a cycling rate between 1 and 2 Hz.100
The 3D motion of the teeth during chewing can be simulated in the chewing device by controlling the vertical and lateral movement of the antagonist. However, most
laboratory fatigue studies involving premolar restorations use a simple vertical motion contacting the central fossa of the test sample and perpendicular to the occlusal surface, with no horizontal movement.105-108 However, previous research has shown the
deteriorating effect of lateral movements on a restoration, especially in wet conditions. Therefore, it is recommended that any laboratory simulation intended to establish the
longevity of an all-ceramic restoration include lateral movements to more closely resemble clinical oral conditions.111-112
A natural tooth antagonist used during testing may be the most representative of a clinical scenario. However, natural teeth vary in size, form and shape making it very
difficult to standardize antagonist parameters across all test specimens, especially if the test sample is a restoration on a natural tooth. Therefore, ceramic and stainless-steel indenters are the most commonly used antagonists.100
The amount of heterogeneity in testing parameters across fatigue studies makes it difficult to compare results between experiments. Specific international standardization for fatigue testing of dental materials is needed to more accurately predict and compare
CHAPTER 2: RESEARCH STUDY
2.1Specific aims of this research study:
Specific aim 1) To evaluate the in vitro fracture resistance of restored premolars with varying preserved cusp buccal-lingual widths during simultaneous thermal and mechanical
fatigue cycling.
Specific aim 2) To evaluate the in vitro fatigue resistance of restored premolars that preserve either the functional or nonfunctional cusps during simultaneous thermal and mechanical fatigue cycling.
Specific aim 3) To evaluate the in vitro fatigue resistance of CAD/CAM generated lithium
disilicate onlays during simultaneous thermal and mechanical fatigue cycling.
2.2 The null hypotheses:
1) The buccal-lingual width of preserved cusps will not influence the fracture resistance of restored maxillary premolars.
2) There is no difference in the fatigue resistance of restored maxillary premolars which
preserve either the functional or nonfunctional cusp.
2.3. Materials and methods:
48 freshly extracted human maxillary premolars free of caries, cracks, endodontic treatment or restorations, were selected. This research study was deemed by the UNC Institutional Review Board to be exempt (IRB #17-1775). Calculus and soft tissue deposits coating these teeth were removed with a hand scaler. Teeth were stored in 0.05% thymol
solution @ 25°C for 1-2 months prior to use. Teeth were randomly divided into six groups of eight specimens each. Two calibrated operators (E.G. and I.A.) prepared teeth for one group at a time. Preparations were performed with 330MWV, 846KR.31.016M and
8846KR.31.016F diamond modified flat-end taper burs (Brassler, Savannah, GA) in a high-speed handpiece with copious air and water-cooling.
Each test group was prepared for an onlay restoration design that replaced one cusp
and a varying buccal-lingual width of the remaining cusp (Figure 2.1). Preserved cusp buccal-lingual width was verified with a digital caliper (63731, Pittsburgh, PA, USA) at the base of the remaining cusp. Remaining preparation measurements were verified with a periodontal probe. Preparations were designed to simulate the clinical presentation of a
fractured cusp with a previous MOD restoration. Standardized tooth preparations were completed as follows:
• Group 1: Preparation of each maxillary premolar was initiated by a 2.0mm depth cut mesiodistally through the central groove. The preparation was extended laterally to the facial to completely and flatly reduce the nonfunctional cusp, and preserve
the cementoenamel junction (CEJ) surrounding the completely reduced nonfunctional cusp.
• Group 2: Preparation of each maxillary premolar initiated by a 2.0mm depth cut mesiodistally through the central groove. The preparation was extended laterally to the facial to completely and flatly reduce the nonfunctional cusp, and
preserve 2.0mm of the buccal-lingual width of the functional cusp. This created an approximate 3.0mm pulpal depth from the occlusal cavosurface margin of the functional cusp. A 1.0mm wide rounded shoulder margin was placed 1.0mm above the CEJ surrounding the completely reduced nonfunctional cusp.
• Group 3: Preparation of each maxillary premolar was initiated by a 2.0mm depth cut mesiodistally through the central groove. The preparation was extended laterally to the lingual to completely and flatly reduce the functional cusp, and preserve 3.0mm of the buccal-lingual width of the nonfunctional cusp. This created an approximate 3.0mm pulpal depth from the occlusal cavosurface margin of the nonfunctional cusp.
A 1.0mm wide rounded shoulder margin was placed 1.0mm above the CEJ surrounding the completely reduced functional cusp.
• Group 4: Preparation of each maxillary premolar was initiated by a 2.0mm depth cut mesiodistally through the central groove. The preparation was extended laterally to the lingual to completely and flatly reduce the functional cusp, and preserve 2.0mm of the buccal-lingual width of the nonfunctional cusp. This created an approximate
A 1.0mm wide rounded shoulder margin was placed 1.0mm above the CEJ surrounding the completely reduced functional cusp.
• Group 5 (control): Complete cuspal coverage. Preparation of each maxillary premolar was initiated by a 2.0mm depth cut through the central groove. The preparation was extended laterally to completely reduce both the functional and
nonfunctional cusps. A 1.0mm wide rounded shoulder margin was placed 1.0mm above the CEJ.
• Group 6: Premolar preparation was initially identical to Group 1 and, subsequently, two 1.5x2.0mm boxes were placed 1.0mm above the CEJ on the mesial and distal
A. B.
C. D.
E. F.
CAD/CAM blocks of lithium disilicate (IPS e.max CAD A2 LT, Ivoclar Vivadent, Schaan, Liechtenstein) were used in conjunction with CEREC BlueCam (Dentsply Sirona, Charlotte, NC, USA) using software version 4.4.4 CAD/CAM system to fabricate test sample onlays. The software “biogeneric copy” function was utilized to replicate the original
anatomy of the tooth in the onlay restoration (Figure 2.2). Therefore, because of the standardized tooth preparations, minimal occlusal thickness of the onlays was 2.0mm and minimal axial thickness was 1.0-1.5mm. Onlays were crystallized according to the
manufacturer’s instructions using Object Fix putty (Ivoclar Vivadent, Schaan,
Liechtenstein) and the Programat CS2 oven (Ivoclar Vivadent, Schaan, Liechtenstein). IPS e.max CAD Crystall Glaze Spray was applied prior to crystallization according to
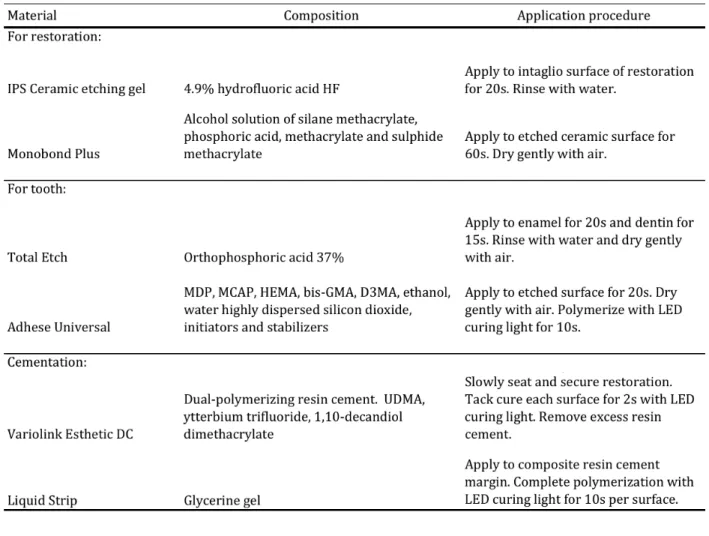
manufacturer’s instructions. Onlays were bonded with Variolink Esthetic DC (Ivoclar Vivadent, Schaan, Liechtenstein) resin cement following adhesive conditioning of the dental tissues and ceramic restoration according to the manufacturer’s instructions (Table 2.1). Excess luting material was removed and glycerin gel was applied to the resin cement margin prior to final curing. Onlays were light cured for 10s per surface (Demetron A.2 LED
A. B.
C. D.
E.
Figure 2.2. CEREC BlueCam 4.4.4 biogeneric copy design sequence for restoration fabrication. A, Initial scan of unprepared tooth. B, Scan of tooth preparation with the unprepared tooth scan superimposed. C, Selected area of the unprepared tooth scan that
Table 2.1 Ivoclar Vivadent Variolink Esthetic DC resin cement adhesive system components, composition and application procedures according to the manufacturer.
2.3.2 Fatigue testing
Test samples were mounted and prepared for fatiguing in a chewing simulator (SD Mechatronik, Feldkirchen-Westerham, Germany). Specimens were oriented parallel to the long axis of the tooth and embedded in acrylic resin (VariDur 200, Buehler, Lake Bluff, IL,
USA) from the root to 1.0mm below the CEJ in the cylinder specimen holders of the chewing simulator.
accomplish fatiguing. This protocol represented approximately five years of clinical simulation109.
A 4.0mm diameter stainless steel stop was used to represent an opposing cusp. In an effort to replicate cusp-to-fossa contacting relationship, during each mechanical loading cycle the stainless-steel stop made contact with the functional cusp, then moved laterally
2.0mm to contact the central fossa (Figure 2.3). A 1.0mm vertical indentation threshold facilitated constant contact during this motion.
Figure 2.3. Mechanical loading pattern of stainless-steel antagonist.
2.3.3 Evaluating failure
Each sample was monitored by a wear detector mounted in each chamber of the
Failure was determined by visual examination with 2.5x magnification loupes. Onlay debonding or fracture, cusp fracture or a combination of tooth and onlay fracture was classified as a failure.
2.4 Statistical analysis:
The failure rate for each group was determined by visual inspection of each test sample after testing. The influence of cusp type was analyzed with a test of proportions by comparing the cumulative percent failure of the functional cusp groups (G1+G2) with the cumulative percent failure of the nonfunctional cusp groups (G3+G4) at a 4% significance level.
2.5 Results:
The group failure rates were as follows: 75.0% (G1), 0.0% (G2), 12.5% (G3), 0.0% (G4), 0.0% (G5) and 0.0% (G6) (Table 2.2).
Table 2.2. Test group failure rates.
The wear detectors mounted in each chamber in the chewing simulator detected
2.4). No other sample failures were detected by the wear detectors or after visual inspection with loupes.
Table 2.3. Mechanical cycles survived (or detected failure cycle) for each test specimen.
Figure 2.4 Mechanical cycles survived (or detected failure cycle) for each test specimen.
The cumulative failure rate for the functional cusp groups (G1+G2) was 37.5%. The
cumulative failure rate for the nonfunctional cusp groups (G2+G3) was 6.3%. The
groups was statistically significant (p=.04; 95%CI:2.11-55.66). Groups 2, 4 and 5
experienced no sample failures. Group 6, which was identical to Group 1 with the addition of retentive mesial and distal boxes, also experienced no failures.
Overall, no cusp or restoration fractures were observed. After visual inspection, all failures were determined to be solely from debonding of the IPS e.max CAD onlay from the
tooth.
2.6 Discussion:
Bulk fracture and loss of restoration have historically been reported to be the main reasons for clinical failures of inlays and onlays41, 47-48, 91. Lithium disilicate ceramic
however, with its improved mechanical durability compared to other glass ceramics, may
offer increased clinical longevity for partial coverage restorations53, 55, 59.
The use of bonded ceramics may be advantageous in clinical scenarios where traditional mechanical retention form is limited, and may allow for more conservative tooth preparations compared to mechanically retained restoration preparations. In these
cases, the need for conventional means of retention such as ideal taper and axial height of the preparation, is reduced due to the bonding potential of ceramic to dentin and enamel with composite resin cement. Alternately, the success of these partial coverage ceramic restorations is, to a high degree, dependent on sufficient support and an optimal adhesive
approaches may, in these cases, involve extensive preparation and/or endodontic treatment, in combination with a post or pin(s) and core placement in order to achieve retention. Rather, the minimal preparation for the bonded ceramic partial coverage restoration is less traumatic for the tooth, and pulp vitality may be preserved.
The clinical performance of adhesively bonded all ceramic restorations has mostly
been studied in the short- and medium-term. There are few studies with extended
observation periods of 10 years or more. Frankenberger et al. found the failure rate for IPS Empress (leucite-reinforced feldspathic porcelain) inlays and onlays of 12% at 12 years, mostly due to bulk fracture47. Van Dijken and Hasselrot conducted a 15-year evaluation of extensive dentin-enamel bonded IPS Empress partial and complete coverage restorations.
In the clinical trial, the authors included onlays that preserved very thin portions of buccal or lingual cusps. Overall, the cumulative failure rate was 24% after 15 years. Most of the failures were due to restoration loss or fracture, with only 1 tooth in the entire study experiencing a cusp fracture48.
Long term, randomized controlled clinical trials are lacking that evaluate lithium disilicate’s use for onlay restorations. In an effort to evaluate the clinical performance of IPS e.max, there have been two studies that sought to indirectly gain insight into
restoration longevity by analyzing dental laboratory data from dentists making remake requests. One study showed 0.99% of e.max onlays were requested to be remade due to
the medium-term, IPS e.max onlays do not experience a high rate of catastrophic failure. However, these studies may tend to under report negative outcomes since the only restorations counted are the ones that were remade by the original laboratory and the patient by the same dentist. Furthermore, patients, who had received the IPS e.max
onlay(s), who had moved to other regions where not included. It can be reasonably said that if there had been large numbers of these restorations failing that this would have surfaced through these indirect studies.
Ideal preparation design standards for dentin-enamel-bonded crowns or partial coverage restorations are lacking. A common clinical dilemma regarding inlay and onlay restorations relates to cavity design. Specifically, there is confusion amongst dentists
regarding occlusal isthmus width, remaining cusp thickness and when cuspal coverage is indicated. The traditional principals of cavity preparation with respect to cuspal coverage are based on cast metal or amalgam restorations that do not adhere to the dental tissue5-7,
92.
Several in vitro studies have shown that the use of adhesive techniques may provide cuspal reinforcement and enhance fracture resistance of nontraditional onlay preparation designs93,96,113. The present study also demonstrated the high fracture resistance of
adhesively bonded onlay restorations. Additionally, unlike the previous mentioned studies, this experiment sought to more thoroughly mimic clinical conditions by exposing samples
teeth during chewing was simulated with both vertical and lateral movements of the stainless-steel antagonist. In all test groups, an effort was made to replicate the typical cusp-to-fossa contacting relationship. During each mechanical loading cycle the stainless-steel stop made contact with the functional cusp, then moved laterally 2.0mm to contact
the central fossa. The use of lateral movements on restorations has a deteriorating effect, especially in wet environments. Therefore, it is recommended that any laboratory
simulation intended to establish the longevity of an all-ceramic restoration include lateral movements to more closely resemble clinical oral conditions111-112.
In the present study, there was no association found between the fracture resistance of premolars restored with CAD/CAM lithium disilicate onlays and the preserved
buccal-lingual wall width of the remaining cusps. Therefore, the null hypothesis that surrounding wall thickness does not affect the fracture resistance of the tooth-restoration complex was accepted. Notably the nonfunctional cusps, which were exposed to a degree of lateral forces when the stainless-steel stop rotated to the central fossa, did not experience any fractures.
There was a significant difference in the failure rates between the groups that preserved the functional cusp and the groups that preserved the nonfunctional cusp. Therefore, the null hypothesis that functional or nonfunctional cusp preservation does not affect the fatigue resistance of a tooth-restoration complex was rejected.
Group 1 displayed the highest failure rate of 75.0%. It was noted after visual
contact location. It was found that antagonist contact with the restoration margin
demonstrated the most amount of cuspal deformation98. In the present study, antagonist forces directly contacting the restoration margin on the functional cusp in Group 1 may have caused cuspal deflection, stressed the adhesive bond of the ceramic onlay to the tooth
and led to a high rate of onlay debonding. Group 6 preparation design was identical to Group 1, with added mesial and distal boxes for retention. Remarkably, this group demonstrated a 0.0% failure rate. Although the antagonist also made contact with the restoration margin in this group, the added retentive boxes may have minimized potential flex or movement of the onlay away from the cusps, thus preventing the onlays from debonding. In addition, the presence of retentive boxes likely limited the ability of shear
forces to overcome the adhesive interface. Therefore, a clinician may want to consider added retentive features to an onlay preparation design if the opposing occlusion will be on the restoration margin. In Group 2, a 2.0mm buccal-lingual width of the functional cusp was preserved in each sample. This design allowed for the antagonist to make majority contact with the onlay restoration, and not the onlay margin or remaining cusp (Figure 2.6). This
Figure 2.5. An occlusal view of a test specimen from group 1 after simultaneous thermocycling and mechanical loading. The wear pattern of the antagonist demonstrates
initial mechanical loading primarily on the tooth and restoration margin.
Figure 2.6. An occlusal view of a test specimen from group 2 after simultaneous thermocycling and mechanical loading. The wear pattern of the antagonist demonstrates
initial mechanical loading primarily on the ceramic restoration.
There was a statistically significant difference in the cumulative failure rates
functional cusps are generally well protected and subject to more compressive forces while nonfunctional cusps tend to receive more tensile stresses90, it is important to note that none of the failures in this study were due to cusp fracture. The mechanism of failure in the functional cusp group may be more related to the margin location in relation to antagonist
occlusion, as previously discussed. Although thin cusps were preserved in groups 2, 3 and 4, the antagonist occlusion was not directly on the restoration margin and they experienced only one debonded restoration and no cusp or restoration fractures.
The tooth structure saving preparation designs used in this study may minimize the risk of pulpal complications in vital teeth. In addition, other advantages may include
preserving a tooth’s natural hues and shades, intracoronal geometry and position in the
arch. The use of adhesively retained lithium disilicate ceramics, that demonstrate improved biomechanical properties, for partial coverage restorations may be a viable alternative to full coverage restorations, and may challenge the once widely accepted principals related to preparation resistance and retention form.
2.7 Limitations of the study
Randomized, controlled clinical trials are the best option for evaluating clinical procedures and/or dental materials. However, they are costly, involve ethical approvals and the process from study inception to article publication may take up to ten years to produce a five-year clinical trial46. In vitro dynamic fatigue testing of ceramic materials under water may be the best laboratory substitute for in vivo testing. However, there is no
The primary limitation of this study was the inability to precisely reproduce clinical intraoral conditions. A natural tooth antagonist used during testing may be the most representative of a clinical scenario. However, natural teeth vary is size, form and shape making it very difficult to standardize antagonist parameters across all test specimens. This
becomes increasingly difficult when the test sample is a restoration on a natural tooth, as was in the present study. Evident in Figures 2.5 and 2.6, the stainless-steel antagonists used generated aggressive wear patterns that are unlike what is typically seen clinically.
Additionally, the chewing simulator is also limited to simple chewing patterns. An effort was made in the present study to replicate a cusp-to-fossa occlusal relationship and to include both vertical and lateral movements from the antagonist. Clinically, teeth
experience varied directional application of loads from working, nonworking and closure, which induce both compressive and tensile stresses. These in vitro differences in force generation produced by the chewing simulator may not be completely analogous to forces commonly experienced by teeth intraorally.
A second limitation of the study was the simple failure criteria. This research study defined the success of a test specimen by considering what would be considered a clinical success. Ideally, survival and success would be differentiated with clearly defined criteria. For example, success rates may be determined by comparison of crack formation in the