A COST BENEFIT ANALYSIS OF A HOME CARE AIDE PROGRAM
Michelle White
A DNP project submitted to the faculty at the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Nursing Practice, (Nurse Executive) in the School of Nursing.
Chapel Hill 2017
Approved by:
Beverly Foster
Hugh Waters
ABSTRACT
Michelle White: A Cost Benefit Analysis of a Home Care Aide Program (Under the direction of Beverly Foster)
An exploratory, retrospective study capturing a two year time period was conducted at a
licensed home care agency to determine if services provided by Home Care Aides (HCAs)
positively impacted patient care outcomes and ultimately provided a cost savings to the health
care system. This program evaluation was conducted at a home care agency owned by a large,
private, not-for-profit health care system; and explored several interrelated concepts: patient
care outcomes, staff training and education, and employee engagement. These concepts
ultimately informed a financial evaluation: the Cost Benefit Analysis. Each of these areas shared
a common theme, the relationship to quality. Avedis Donabedian’s theory of quality
improvement was selected to guide this project. Donabedian’s theory allowed quality metrics to
be translated into a meaningful financial comparison outlined by structure, process and outcomes
(Donabedian, 1982). For the study period, 2014 to 2015, the agency demonstrated patient
satisfaction scores consistently in the 95th percentile and employee engagement scores in the 99th
percentile. These scores allowed for consideration that interpersonal relationships contribute to
the success of technical skill. Technical skill contributes to decreased acute care utilization and
improved patient care outcomes. The results of the evaluation demonstrated that while there is a
financial loss to the health care system due to low reimbursement rates and few payor sources for
federal government and other health insurers. More importantly, the study population receiving
HCA services demonstrated fewer hospitalizations and re-hospitalizations as compared to the
TABLE OF CONTENTS
LIST OF TABLES ...vii
LIST OF ABBREVIATIONS ...viii
CHAPTER 1: INTRODUCTION ...1
CHAPTER 2: APPLICATION OF QUALITY IMPROVEMENT THEORY ...5
CHAPTER 3: LITERATURE REVIEW ...7
DEMAND FOR THE HOME CARE AIDE...7
EDUCATION AND TRAINING...8
PATIENT CARE OUTCOMES AND FINANICAL IMPLICATIONS...10
LITERATURE LIMITATIONS...10
CHAPTER 4: PROJECT DESIGN ...12
CHAPTER 5: METHODOLOGY ...13
CHAPTER 6: CHRONIC CONDITIONS DEFINED ...14
CHAPTER 7: DATA ANALYSIS AND RESULTS ...15
CHAPTER 8: COST BENEFIT ANALYSIS ...21
CHAPTER 9: QUALITY IMPLICATIONS ...23
CHAPTER 10: EDUCATION AND TRAINING ...24
CHAPTER 11: LIMITATIONS OF THE STUDY ...26
CHAPTER 12: CONCLUSION ...27
APPENDIX II: NC BOARD OF NURSING NURSE AIDE TASKS ...29
APPENDIX III: SUBCHAPTER 13J – THE LICENSING OF HOME CARE AIDE
AGENCIES: IN-HOME AIDE SERVICES ...31
APPENDIX IV: APPLICATION OF DONABEDIAN THEORY OF QUALITY
IMPROVEMENT TO THE CBA OF THE HOME CARE AIDE PROGRAM ...32
APPENDIX V: COUNTY LEVEL MULTIPLE CHRONIC CONDITIONS (MCC):
PREVALENCE, MEDICARE UTILIZATION AND SPENDING METHODS ...33
LIST OF TABLES
TABLE 1 – PREVALENCE WITH 4-5 CHRONIC CONDITIONS 2015 ...16
TABLE 2 – PERCENT OF MEDICARE FFS BENEFICIARIES WITH 4-5
CHRONIC CONDITIONS WITH 1 OR MORE HOSPITAL ADMISSIONS ...17
TABLE 3 – POTENTIAL COST SAVINGS TO THE HEALTH CARE SYSTEM RELATED TO REDUCTIONS IN HOSPITALIZATIONS FOR PATIENTS
RECEIVING HOME CARE AIDE SERVICES...18
TABLE 4 – 30 DAY READMISSION RATE WITH 4-5 CHRONIC CONDITIONS ...19
TABLE 5 – MEDICARE SPENDING INCREASES WITH # CHRONIC
CONDITIONS IN 2014 ...20
TABLE 6 – AGENCY EXPENSE RELATED TO HOME CARE AIDE PROGRAM ...21
LIST OF ABBREVIATIONS
ADL Activity of daily living
BTBQ Building training, building quality
CBA Cost benefit analysis
CHF Congestive heart failure
CMS Centers for Medicare and Medicaid Services
COPD Chronic obstructive pulmonary disease
EHR Electronic health record
FFS Fee for service
HCA Home care aide
IADL Instrumental activity of daily living
NC DHSR North Carolina Division of Health Service Regulation
NNAS National nursing assistant survey
NNHS National nursing home survey
PCA Personal care aide
CHAPTER 1: INTRODUCTION
There is high value in providing care in the home because it can improve patient
outcomes in the least costly and patient preferred setting, the home (Alliance for Home Health
Quality and Innovation, 2014). As policy makers face the challenge of reducing health care
expense, the discussion often leads to a model that allows the patient to age at home and receive
efficient care without sacrificing effectiveness (Berta, 2013). Home Care Aides (HCAs) could be
essential in meeting the need for a low-cost, high quality care alternative for community
dwelling individuals who wish to remain home and who require assistance with activities of
daily living (ADLs) and instrumental activities of daily living (IADLs) (Luz & Hanson, 2015).
The HCA is a paraprofessional member of the home care team that assists the patient
with bathing, grooming, toileting, meal preparation, light housekeeping, reporting to the
professional staff changes in patient condition and medication reminders. The HCA has
commonly been referred to as an In Home Aide, Home Health Care Aide, Personal Care Aide,
Nursing Assistant, Homemaker or the Direct Care Worker in literature reviews. The Home Care
Aide practice is governed by the North Carolina Division of Health Service Regulation (NC
DHSR), Home Care Licensure section; and funded by many payer sources including federal and
state programs and the ever-growing private pay sector. However, there are problems in
capturing the financial value of HCA services. Financial value is often linked to outcomes,
scorecards and benchmarking within health care industries.
While data collection related to client outcomes is required by NC licensure, there is no
type of data to be collected; thus benchmarking patient care outcomes is difficult. NC licensure
requires an internal evaluation annually but does not require external reporting. The minimum
areas for evaluation include: census, number of hours of care, client outcomes and adequacy of
staff to meet client needs, rationale for non-acceptance of clients and reasons for discharge.
Licensure does not however provide a definition of “client outcomes” (The Licensing of Home
Care Agencies, 2017). Without this definition, agencies can collect any information they
determine to demonstrate “client outcomes” and therefore there is no structured, consistent
requirement for data collection. Without structured and consistent data collection, it is difficult
to benchmark outcomes and demonstrate improved patient outcomes based on care provided by
the HCA (Appendix I).
There is also the possibility of substantial inconsistency of the training and education of
the HCAs in the home. Licensure states that if the client requires extensive assistance than the
aide shall be listed on the Nurse Aide Registry. Listing on the Nurse Aide Registry demonstrates
that the individual has met both state and federal training and competency validation to perform
Nurse Aide I skills (NC Nurse Aide Registry, 2017) (Appendix II). If the client requires only
limited assistance there is no requirement for the aide to be listed on the Nurse Aide Registry
(The Licensing of Home Care Agencies, 2017). However, within licensure, there is no required
standardized training of the non-registered aide, allowing each agency to determine the elements
of training and competency validation for each of these employees (Appendix III).
Lack of required data collection related to patient outcomes and non-standardized
education and training are just a few of the challenges that prevent home care agencies from
maximizing and demonstrating the value of the HCA. Additionally, many of these programs are
dwindles. Medicare, the largest health insurer of those over the age of 65 is not a funder for these
services, limiting those patients who have access to HCA services. A retrospective, exploratory
study using internal home care organizational data to produce a cost benefit analysis was
conducted in an effort to describe potential costs and benefits for both the organization and the
recipients of care. The purpose of this project was to determine whether the care recipients of
community-based home care aide services had lower rates of hospitalizations and
re-hospitalizations 30 days after discharge as compared to a Medicare Fee for Service population
with like numbers of chronic conditions. It is important to note that since there is no requirement
for home care agencies to collect nor report acute care utilization, it was impossible to determine
if any of the participants in the general Medicare comparison group received HCA services.
The study site was a licensed home care agency owned by a large, multi-hospital health
care system. The clinical site employed over 140 HCAs and provided HCA services to 544
individuals aged 65 and older during the course of the study. All HCAs at this agency were listed
on the NC Nurse Aide Registry and received enhanced population health specific education by
nursing leadership in the home care agency. The education included certain chronic disease
processes such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD)
and diabetes. Content included a basic pathophysiology of each disease process, signs and
symptoms to observe and the role of the HCA in helping to maintain health and prevent acute
care utilization. The HCAs also received education regarding the aging process and caring for
those with general chronic health conditions. Elements of critical thinking were included in the
education provided to the HCAs. The HCAs were taught the “why” behind the task. For
instance, a HCA was taught the importance of daily weights and a low salt diet for a patient with
were caring for. The need for enhanced education was quickly identified and even verbalized by
the HCA staff and managers. According to the National Nursing Assistant Survey (NNAS),
inadequate training of this direct care workforce has far-reaching ramifications such as poor
quality of care, poor patient outcomes such as neglect and abuse, and is a predictor of job
dissatisfaction and job turnover (Sengupta, Ejaz, & Harris-Kojetin, 2012).
However, an additional and larger problem was discovered within the organization. Over
the past two years, the clinical site has consistently demonstrated a financial loss in the HCA
program. Despite efforts to reduce expenses, such as a reduction of mileage reimbursement, a
reduction of weekend differential, a substantial reduction of overtime and a reduced wage entry
rate, this program continued to demonstrate a negative income from the operations margin. An
observed hypothesis suggested the HCA improved quality and patient care outcomes, but also
provided a financial savings to the larger health care system through reduced acute care
utilization. A cost benefit analysis (CBA), guided by quality theory, informed the study.
The clinical questions were: (1.) Will older adults who receive care provided by HCAs
have fewer hospitalizations and re-hospitalizations? (2.) Will the larger health care system
CHAPTER 2: APPLICATION OF QUALITY IMPROVEMENT THEORY Understanding quality is essential in the attempt to translate quality data into financial
data. Quality of care has long appeared to be a mystery, illusive, difficult to define yet capable of
being perceived and appreciated but difficult to measure. The conceptual and operational
definition relies on many variables: performance of health care providers, contributions of
patients and overall performance of the health system. Essentially, quality is anything anyone
wants it to be (Donabedian, 1988). According to Donabedian, the process of healthcare itself can
be divided into two major components: technical care and interpersonal relationships. The
theory further informs the intervention by suggesting that interpersonal relationships are a
necessary vehicle for application of effective technical care (Donabedian, 1982). For example,
if the Home Care Aide (HCA) is consistently assigned to the same patient, develops a trusting
relationship and becomes knowledgeable of the patient’s baseline condition, then the HCA can
provide effective technical care that is individualized and meaningful. This theory will provide a
framework in which to illustrate Donabedian’s definitions of structure, process and outcomes
and conceptually operationalize the project (Appendix IV).
Donabedian defines structure as the environment in which services are provided, the
attributes of material and human resources. Process is defined as the service provided or the
patient’s role in seeking service. Outcomes are defined as the impact or effect on the patient’s
health status based on the process (Donabedian, 1988). When applied to this project, the
structure becomes the financial and human resources to provide care in the home including the
technical care provided by the HCA: assistance with activities of daily living, instrumental
activities of daily living, medication reminders, fall prevention strategies, reporting early changes
in the patient’s condition, transportation to physician appointments, meal preparation and
nutritional assistance and most importantly, consistent, long-term relationships that build trusting
inter-personal relationships. The outcome measure is the rate of hospitalizations,
re-hospitalization and cost associated with acute care utilization.
It has been demonstrated that those who receive HCA services will have lower rates of
hospitalizations and re-hospitalizations 30 days post hospital discharge. Cost and quality are
confounded as many believe that to increase quality, cost also must increase (Donabedian, 1988).
Conversely, this project demonstrates a positive correlation between structure, process and
CHAPTER 3: LITERATURE REVIEW
The literature review encompasses research into the various aspects that were considered
during the study’s planning phase: the HCA’s role, education and training, patient care
outcomes and the financial implications of home based services. The broader literature review
beyond nursing reveals disciplines that have identified the potential benefit of the HCA,
including: physical therapy, occupational therapy, speech therapy, family caregivers and various
funders.
Demand for the HCA
A staggering 24% of Nurse Aides work in home health/home care industry while 20%
work in nursing homes. It was estimated that there would be a 76% increase in the demand for
Home Care Aides by 2016 (Goodman, 2010). This prediction was realized in 2016 where
26,343 NC Nurse Aide I’s worked in Home Care compared to 17,348 in hospitals and 22,559
worked in Nursing Homes. Additionally, in 2016, there were 115,508 active nurse aides on the
registry and 339,438 inactive aides (Kathie Smith, personal communication February 27, 2017).
There is great variation in the terminology used to reference direct care workers in the home.
The clinical site for this study employs only Nurse Aide Is certified in NC. The minimum
federal curricular hourly requirements for Nurse Aide I training is 75 hours, the state approved
program average is 142 hours of education and training (Goodman, 2010). Many home care
agencies choose to employ personal care aides (PCAs). These employees are also often referred
to as the non-registered aides. There are no federal PCA competencies or training requirements
the agency. Thus, the concern is that while both workforces vary greatly in training, education
and competency, they both are ultimately assigned to care for the same acuity of patient in the
home. A frightening realization!
As the care paradigm shift moves towards community based models, home care agencies
prepare to meet the growing needs. As the need grows, so does the realization that this
workforce must be trained to provide safe, competent, quality care. However, an additional
problem exists: HCAs are hired for low paying jobs, with part-time hours, minimal benefits and
inadequate training. This leads to employee dissatisfaction, and high turnover rates (Luz &
Hanson, 2015). How, in this environment, do you ensure competent care and develop satisfied
employees that in turn may foster safe care to satisfied clients? The answer may lie partially in
the training.
Education and Training
The NNAS surveyed 3,377 HCAs from 2004 to 2007 as a supplement to the National
Nursing Home Survey (NNHS). A stratified, multistage probability design was utilized. The
study concluded the expected results: there was a direct relationship between initial training and
feeling prepared for the job (Sengupta, Ejaz, & Harris-Kojetin, 2012). In 2010, the Personal and
Home Care Aide State Training (PHCAST) demonstration project, mandated by the Affordable
Care Act and administered by the Health Resources and Services Administration, funded six
states to develop a range of curricula and test new training programs. As part of this project, the
Building Training, Building Quality (BTBQ) program in Michigan utilized a robust research
component using a prospective, mixed methods design with a randomized control group to
determine program impact and key elements of a “gold standard” PCA training program. The
knowledge, skills and attitudes and job status. According to the Bureau of Labor Statistics, the
mean wage for a HCA is $10.79/hour as compared to the mean wage of a textile factory worker
at $13.72/hour (Bureau of Labor Statistics, 2015). An unfortunate realization is that one can
make a higher wage making textiles than caring for our most vulnerable citizens as they strive to
stay safely at home. The problem is multi-faceted: creating a workforce that has the training and
skills to provide quality, competent care and exploring options to provide the training and retain
the workforce.
A long-term care and post-acute skilled facility located in Sylvania, Ohio, utilized a
longitudinal cohort study, which utilized pre and post-intervention surveys to assess the effects
of an advanced training program on job satisfaction. A 3-day advanced training for Nurse Aides
was designed including such topics as anatomy and physiology, infection control and exploration
into the aide’s role in the health care environment, fostering effective communication skills and
improving team functions. The students attended 2 classroom days and the third day was spent
with mastering skills in a lab setting. Job satisfaction did improve, turnover decreased and
clinical indicators were improved. As a result, communication between leadership and the Nurse
Aides improved and a mentorship program was born (Brown, Redfern, Bressler, Swicegood, &
Molnar, 2013).
Training, education and competency of the HCA is an important variable as it relates to
outcomes. The project clinical site only employs Nurse Aide Is and allows them to work to the
top of their legal scope of practice, offering additional education as the patient population
became more complex. Donabedian contends that care is often wasteful of resources and
costlier than it needs to be when administered ineffectively (Donabedian, 1980). The skills
think. If taught to critically think, educated about disease processes, the importance of
medication compliance, signs and symptoms to report, fall reduction strategies and the impact of
nutrition on overall health, the HCA could hypothetically reduce acute care utilization and
improve patient care outcomes.
Patient Care Outcomes and Financial Implications
According to Home Health Care Aides as Extenders of Therapy Services: A Managed
Care Pilot Program of four Kaiser Home Health Agencies in Northern California, HCAs received
specialized training to support the role of the physical therapist and reinforce exercises in the
home. The aide frequency of visits increased, allowing the physical therapy visits to decrease.
The result was improved patient outcomes and reduced organizational expense (Treml &
Schulman, 1998).
A similar exploratory research study occurred two years prior in northern California that
yielded similar results. Therapy (occupational, physical, speech) visits decreased from 11.2 to
7.5 and aide visits increased from 12 to 14 per patient. Cost of care was reduced by 15% by
allowing the aides to reinforce therapy instruction and assist with exercises taught by the
therapist (Swett, 1996).
Literature Limitations
The literature review did not reveal any studies of services provided solely by the HCA
where the outcomes were financially measurable. The literature review did not reveal research
that predicts cost savings to the health care system based on care provided by the HCA. This
type of research could validate the need to invest in training and education of this direct care
workforce and encourage reimbursement by new payor sources. The current problem is that the
improved patient care outcomes and therefore there is no demonstrated relationship to financial
savings.
While many studies exist surrounding the need for standardized training, little research
exists about the need for a consistent, comprehensive training program for HCAs that allows them
to work at the top of their skill set and that will permit them to transition from setting to setting.
Most research is site specific and thus the education is created specifically to benefit the
organization in which the research was conducted. According to the Oregon State Board of
Nursing, a stakeholder group comprised of Nursing Assistant, nurse administrators, nursing
assistant educator and regulators have met monthly to review the training curriculum and
authorized duties for the Nursing Assistant I and Nursing Assistant II. The proposed changes were
in response to the increasing acuity of patient needs across settings. These changes were initiated
to facilitate the transition from one setting to another (Buck, 2014). Quality of care and patient
care outcomes can be endangered without competent staff.
Of interest, at the time of launch of this study, Harvard Medical began a similar study titled
“The Intervention in Home Care to Improve Outcomes.” Harvard Medical, Right at Home, and
Clear Care have partnered together for this exciting research that is currently testing a large-scale,
randomized intervention aimed at preventing hospitalizations, improving health outcomes, and
lowering Medicare spending among private-pay home care recipients (Right at Home, 2015). The
CHAPTER 4: PROJECT DESIGN
The project design was a program evaluation of an existing service line falling under a
licensed home care agency with retrospective data spanning a two-year period, October 1, 2014
to September 30, 2016. The home care aide program provides a range of services to children,
those with behavioral health diagnoses, and to the frail elderly community dwelling individuals
who need assistance to stay safely in their homes. For the purposes of this proposed project,
only those who are 65 or older and living in their homes were included in the evaluation.
The information that was available includes the cost to provide the HCA services,
revenue, operational adjustments and the financial deficit related to this service line. The
organization has internal quality assurance data including ED visits, hospitalizations and
re-hospitalizations within 30 days post hospital discharge for the selected group. Additionally,
CHAPTER 5: METHODOLOGY
Prior to the initiation of the study, approval for the project was obtained by the clinical
site, IRB approval was obtained from the clinical site and IRB approval was obtained through the
university. The study methodology was a retrospective exploratory approach utilizing secondary
data captured within the organization. Inclusion criteria for data collection included patients of
the licensed home care agency who received HCA services who were aged 65 and older with
four or more chronic health conditions. Medicare is the United States Federal health insurance
program for those 65 years and older. The comparison consists of a number of chronic
conditions for traditional Medicare Fee for Service (FFS) beneficiaries. It is important to note
that was a limitation in the data collection process. As the study site transitioned from ICD-9 to
ICD-10 codes, some diagnoses were lost due to the translation. The impact could be that the
study sample actually had greater numbers of chronic health conditions than reported. The CBA
analyzed data for one year that included the total census of patients who met the inclusion
criteria, hours of care provided, payor source specific operational revenue, operational expense,
emergency department utilization, hospitalizations and re-hospitalizations less than 30 days of
hospital discharge. A comparison included the group of patients who received the HCA services
to a general Medicare FFS population in an effort to illustrate a statistical difference in the rate of
acute care utilization. Once that relationship was determined, expense savings were estimated.
CHAPTER 6: CHRONIC CONDITIONS DEFINED
The Office of Enterprise Data and Analytics, within the Centers for Medicare &
Medicaid Services (CMS), has outlined a set of chronic conditions to provide researchers and
policymakers with a better understanding of the burden of chronic conditions among
beneficiaries and the financial implications for health care systems. Statistics on prevalence, care
utilization, and Medicare spending for certain chronic conditions as well as multiple chronic
conditions demonstrates the overall financial burden and complexity of chronic conditions
among Medicare beneficiaries. The chronic conditions outlined by CMS were used in this study
when determining the number of chronic conditions per patient. These chronic conditions
include (CMS.GOV, 2016):
Alzheimers Disease and Related Dementia Heart Failure
Arthritis (Osteoarthritis and Rheumatoid) Hepatitis (Chronic Viral B & C)
Asthma HIV/AIDS
Atrial Fibrillation Hyperlipidemia (High cholesterol)
Autism Spectrum Disorders Hypertension (High blood pressure)
Cancer (Breast, Colorectal, Lung, and Prostate) Ischemic Heart Disease
Chronic Kidney Disease Osteoporosis
Chronic Obstructive Pulmonary Disease Schizophrenia and Other Psychotic Disorders
Depression Stroke
CHAPTER 7: DATA ANALYSIS AND RESULTS
There were a total of 277 patients who met the inclusion criteria for the timeframe
October 1, 2014 to September 30, 2015 and a total of 267 patients for the timeframe of October
1, 2015 to September 30, 2016. The inclusion criteria consisted of any patient 65 years or older
who received HCA services within the designated time period. There were a total of 544 patients
included in the study. The home care agency separates patients into three levels of care
depending on complexity of need and level of care required by the HCA. The variables to
determine level of care include nutrition, mobility, the need for assistance with bathing,
grooming, toileting and medication reminders. Patients in both Level I and Level II require
hands on assistance with two or more ADLs. Of the 544 patients studied, 93% required hands on
assistance with 2 or more ADLs.
HCA services are covered by various payor sources within the agency. These payor
sources include private pay, Medicaid Personal Care Services, Medicaid Community Alternatives
Program, Home and Community Care Block Grant, sub-contracts to other facilities and the
Department of Social Services. The largest base of HCA revenue is private pay and the
sub-contracts to other facilities. For the 2015 to 2016 time period, private pay accounted for 42% of
total revenue, Medicaid 20% and sub-contracts to other facilities 22%.
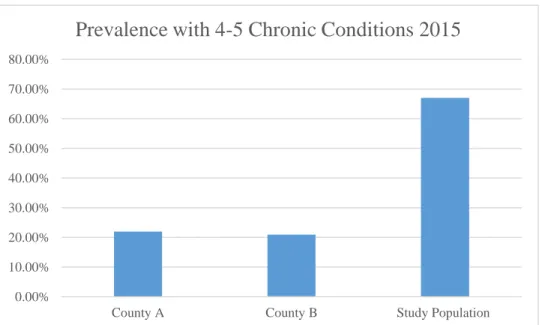
The home care agency serves 2 counties (county A and county B). According to CMS
data, county A’s prevalence rate for 4 or more chronic conditions among Medicare beneficiaries
is 21.94% (CMS.GOV, 2016). The prevalence in county B is 20.96%. Of the studied patients in
Medicare & Medicaid Services (CMS), much higher than the prevalence rate contained in the
individual counties. This was to be expected since only those individuals who require assistance
with ADLs and IADLs seek HCA services. Prevalence, Medicare utilization and spending were
determined by utilizing the County Level Multiple Chronic Conditions Table (CMS.GOV, 2016)
(Appendix V). An important limitation to discuss is that while all participants in both the general
Medicare population and the study population were aged 65 and older, there is no average age
from CMS to date and the average age in the clinical site for individuals who received HCA
services was 73. However, the average age in 2014 for county A was 70, the average age for
county B was 70 and the average age in the clinical site who received HCA services was 72.
Table 1. Prevalence with 4-5 Chronic Conditions 2015
0.00% 10.00% 20.00% 30.00% 40.00% 50.00% 60.00% 70.00% 80.00%
County A County B Study Population
County Prevalence of individuals with 4-5 chronic conditions Per Capita Spending per FFS Beneficiary ED Visits per 1000 Beneficiaries 30 Day Readmission Rate # in County A
2015 21.94% $11,008 759 11.20% 13,707
B
2015 20.96% $11,356 891 15.16% 40,869
Medicare beneficiaries with multiple chronic conditions have greater health care
utilization and higher health care cost. While the study population was heavily populated with
those patients with high chronicity, the hospitalization rate was far less than the average
Medicare FFS population with equal chronic health conditions (CMS, 2012).
Table 2. Percent of Medicare FFS Beneficiaries with 4-5 Chronic Conditions with One or More Hospital Admissions
It is evident that the individuals who received HCA services had substantially lower
rates of hospitalizations than the general Medicare FFS aggregate population. During the time
period October 1, 2014 to September 30, 2015 there were 30 unduplicated hospitalizations 0% 5% 10% 15% 20% 25% 30% 35%
% General Medicare FFS Beneficiaries
% Study Population That Receive HCA Services
2014-2015
% Study Population That Receive HCA Services
2015-2016
% of Medicare FFS Beneficiaries with 4-5
Chronic Conditions with One or More Hospital
(11%) and during the time period October 1, 2015 to September 30, 2016 there were 45
unduplicated hospitalizations (16%). According to the Agency for Healthcare Research and
Quality, in 2012, there were 36.5 million hospital stays in the United States, with an average
length of stay of 4.5 days and an average cost of $10,400 per stay (AHRQ, 2014). To quantify
the cost savings to the larger health care system, the difference in hospitalization rates from
those who received HCA services with one or more hospitalizations was compared to the
overall sample size. The difference in patient numbers from those hospitalized to the average
general Medicare FFS beneficiary grouping was determined. The difference was then
multiplied based on the AHRQ average rate per hospitalization at $10,400.
Table 3. Potential Cost Savings to the Health Care System Related to Reductions in Hospitalizations for Patients Receiving HCA Services
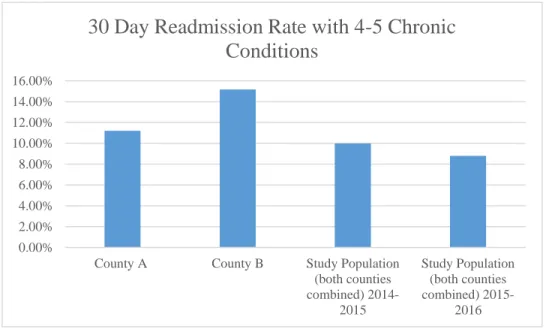
Medicare beneficiaries with multiple chronic conditions have a greater chance for a
hospital readmission within 30 days. A readmission is defined as an admission to an acute care
hospital for any cause within 30 days of discharge from an acute care hospital. The study $0
$100,000 $200,000 $300,000 $400,000 $500,000 $600,000
Cost Savings to Health Care System 2014-2015 ($551,200)
Cost Savings to Health Care System 2015-2016 ($364,000)
Potential Cost Savings to the Health Care System
population receiving the HCA services continues to have a lower re-hospitalization rate than the
general Medicare FFS population per county.
Table 4. 30 Day Readmission Rate with 4-5 Chronic Conditions
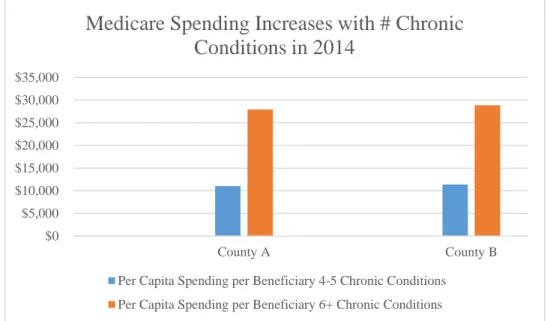
It is evident Medicare spending increases as the numbers of chronic health conditions
increase. Medicare spending includes total Medicare payments for all Medicare covered
services and is presented as total spending per beneficiary (per capita). CMS reports an annual
2014 Medicare spending of beneficiaries with 4-5 chronic health conditions to be
$85,998,126,413 and an annual spending of beneficiaries with 6+ chronic health conditions of
$141,772,441,945. 0.00%
2.00% 4.00% 6.00% 8.00% 10.00% 12.00% 14.00% 16.00%
County A County B Study Population
(both counties combined)
2014-2015
Study Population (both counties combined)
2015-2016
30 Day Readmission Rate with 4-5 Chronic
Table 5. Medicare Spending Increases with # Chronic Conditions in 2014
$0 $5,000 $10,000 $15,000 $20,000 $25,000 $30,000 $35,000
County A County B
Medicare Spending Increases with # Chronic
Conditions in 2014
Per Capita Spending per Beneficiary 4-5 Chronic Conditions
CHAPTER 8: COST BENEFIT ANALYSIS
In order to create a real time illustration of cost versus benefit, the financial cost data
analyzed spanned from October 1, 2015 to September 30, 2016.
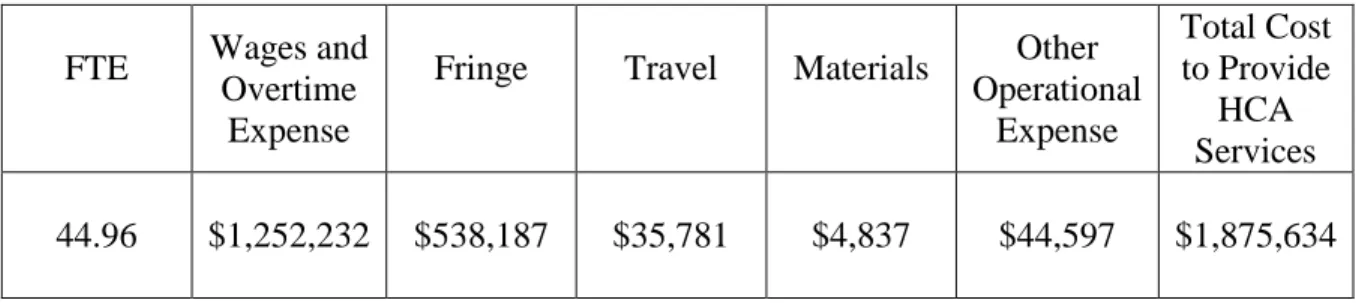
Table 6. Agency Expense Related to HCA Program
FTE Wages and Overtime
Expense
Fringe Travel Materials Other Operational
Expense
Total Cost to Provide
HCA Services
44.96 $1,252,232 $538,187 $35,781 $4,837 $44,597 $1,875,634
Total Agency Revenue Generated from HCA Program: $1,617,170
Total Organizational Loss from HCA Program / Expense from Operations ($258,464)
Table 7. Cost Benefit Analysis Snapshot 2015-2016
$0 $50,000 $100,000 $150,000 $200,000 $250,000 $300,000 $350,000 $400,000
Expense from Operations (Cost) $258,464
The average starting salary for the HCA is $9.75 per hour with a 28% fringe. Travel
is reimbursed at 0.36 per mile. The HCA is compensated for travel time between patients and
for mileage. This time and mileage is not reimbursable by any payor source. The living wage
for HCAs will increase to $12.00 per hour in the summer of 2017. This will further result in an
additional loss of $224,902.55 annually. Other operational expense included rent, utilities and
other fixed costs. Wages and overtime expense includes the HCA salaries and other fixed
salaries including Office Coordinators, Patient Accounting, Agency Director, RN Supervisor
and RN Educator.
It would be remiss not to mention the immeasurable benefits such as quality of life for
the patients and caregivers who receive HCA services. The HCA allows caregivers to continue
to work and can reduce caregiver burnout and strain. These services also could possibly
CHAPTER 9: QUALITY IMPLICATIONS
It is evident that while there is a financial loss to the healthcare system, there is a
greater savings to the larger health care system including private, state and federal insurers.
The question then becomes, “What is attributable to the success of this HCA program?”
Furthermore, one could ask if this HCA program provides unique outcomes or could these
outcomes be replicated in other HCA agencies. While there is no other data for benchmark
comparisons, one could argue that the quality of the HCA service provided by this agency lends
to the success. This project has three interrelated concepts: patient care outcomes (reduced
acute care utilization and reduction in Medicare spending), staff training and education, and
employee engagement. These concepts ultimately informed the financial evaluation: the cost
benefit analysis. Each of these areas share a common theme, the relationship to quality. More
importantly is the profound realization that the interpersonal relationships that the aides form
with the patients may in part, be the most determining factor of success (Donabedian, 1988).
For the study period, the agency demonstrated patient satisfaction scores consistently ranging
from 92-95th percentile and employee engagement scores in the ranging from the 95th to the 99th
percentile. These scores support Donabedian’s concept that interpersonal relationships
contribute to the success of patient satisfaction and enhanced training in technical skills
contribute to the success of employee engagement scores. Technical skill then drives the
outcomes of decreased acute care utilization (Donabedian, 1988). Using the framework of
structure, process and outcomes allowed for an analysis of the interrelatedness of each of these
CHAPTER 10: EDUCATION AND TRAINING
Training, education and competency of the HCA are important variables as they relate
to outcomes. For purposes of this project, all HCAs were at a minimum, Nursing Assistant Is
listed with the North Carolina Health Care Personnel Registry (Appendix 2). Donabedian
contends that care is often wasteful of resources and costlier than it needs to be when
administered ineffectively (Donabedian, 1980). One could contend that the HCA does not fully
practice within the allowable tasks for Nurse Aides defined by the North Carolina Board of
Nursing. The skills required of the HCA are not only ADL and IADL assistance but also the
need and ability to critically think. In 2013, the NC DHSR added a new module to the state
approved Nursing Assistant I training program: Critical Thinking. This module defines critical
thinking as safely providing resident care in a variety of situations based on facts learned and
bedside observations, or the ability to think on one’s feet (Module O - Critical Thinking, 2013).
The HCAs were taught and encouraged to critically think, educated about the most common
disease processes, the importance of medication compliance, signs and symptoms to report to
nursing supervisors, fall reduction strategies and the impact of nutrition on overall health. It is
proposed that this additional education contributed to the decreased acute care utilization
achieved by the home care agency, however since no benchmark data was available, this
remains a hypothetical variable.
An internal case study detailed the impact of the HCA services on a high-risk patient
bone was discharged to home from a recent admission with severe congestive heart failure
(CHF). Sixteen percent of all Medicare beneficiaries have CHF (2012). While hospitalized, he
was diagnosed and treated for bronchitis. A retrospective chart review revealed that the patient
was in acute heart failure and did not have bronchitis. At the time of discharge, the patient
weighed 30lbs over his dry, base weight. The Institute for Healthcare Improvement estimates
15 million incidents of patient harm that occurs in US hospitals annually (IHI, 2007).
Additional consideration could suggest that preventing hospitalizations, could also reduce the
risk of patient harm that could occur during one’s hospitalization. Once this patient returned
home, medication compliance, close monitoring and strict adherence to a low sodium diet was
of the most importance for success. A primary HCA was assigned to this case. The HCA
received individual education regarding CHF, the importance of restricting sodium in the diet,
signs and symptoms to report, how to perform correctly daily weights with parameters to report
and the importance of ensuring the patient took the medications that were pre-poured by family
in a timely manner. HCA services were increased to daily and the time spanned around
breakfast and lunch. The aide ensured daily weights, prepared low sodium, heart healthy meals
and reported any changes to the RN supervisor. Over a period of 2 months, the patient returned
to the original dry weight and the aide could clearly articulate the impact of sodium on weight
gain and the direct impact of the fluid gain on the exacerbation of the heart failure. While these
metrics are quantifiable, the quality of life returned to this patient is not. The plans for Hospice
CHAPTER 11: LIMITATIONS OF THE STUDY
An exhaustive review of the literature to locate like studies proved to be non-productive.
There were no like studies that researched the impact of HCA services on patient care outcomes.
Therefore, the need for exploratory research was confirmed.
A significant barrier to the project was the lack of precise comparative data available to
evaluate outcomes. Since many patients privately pay for HCA services, there was no
comparative to benchmark outcomes to, therefore the Medicare FFS population was chosen as a
general comparison. The lack of comparative data also prevented a correlation relationship
between advanced education of the HCA and improved patient outcomes.
Lastly and most detrimental to the Cost Benefit Analysis was the loss of numbers of
chronic conditions related to the transition from ICD-9 to ICD-10 codes. This was not an
automatic translation that occurred in the Electronic Health Record (EHR) within the site. It
required manual translation by clinicians. It is expected that some diagnoses were omitted, thus
creating a population with fewer chronic health conditions. Nonetheless, even with limited
diagnosis, it was evident that the agency did care for a large population with multiple chronic
health conditions. This limitation lead to an under estimation of total cost savings to the health
CHAPTER 12: CONCLUSION
Patients who received HCA services had lower hospitalization and re-hospitalization rates
than the general Medicare FFS population with equal amounts of chronic conditions. While the
agency demonstrates a financial loss, the cost saving may not be to the health care system that
owns the home care agency but may in fact be a savings to our health care system and insurance
companies. It is plausible to consider that if these services were covered by Medicare as a low
cost intervention for those wishing to remain home, then millions of federal dollars could be
APPENDIX I: SUBCHAPTER 13J – THE LICENSING OF HOME CARE AGENCIES: EVALUATION
(10A NCAC 13J 1004 EVALUATION)
(a) The agency's governing body or its designee shall, at least annually, conduct a comprehensive evaluation of the agency's total operation.
(b) The evaluation shall assure the appropriateness and quality of the agency's services with findings used to verify policy implementation, to identify problems, and to establish problem resolution and policy revision as necessary.
(c) The evaluation shall consist of an overall policy and administration review, including the scope of services offered, arrangements for services with other agencies or individuals, admission and discharge policies, supervision and plan of care, emergency care, service records, personnel qualifications and program evaluation. Data to be assessed shall include at a minimum the following:
(1) number of clients receiving each services; (2) number of visits or hours for each service; (3) client outcomes;
(4) adequacy of staff to meet client needs;
(5) numbers and reasons for nonacceptance of clients; and (6) reasons for discharge.
(d) An evaluation of the agency's client records shall be carried out at least quarterly by appropriate professionals representing the scope of the agency's program. The evaluation shall include a review of sample active and closed client records to ensure that agency policies are followed in providing services, both direct and under arrangement, and to assure that the quality of service is satisfactory and appropriate. The review shall consist of a representative sample of all home care services provided by the agency.
APPENDIX II: NC BOARD OF NURSING NURSE AIDE I TASKS I. PERSONAL CARE (ADL)
- Bathing (assist, bed bath, tub bath, shower, sitz)
- Mouth care - Skin care - Hair care - Nail care
- Bedmaking (modified) - Dressing and undressing
V. SAFETY
- Side rails/ call rails - Mitts and restraints - CPR/Heimlich Maneuver
- Infection control – Handwashing, Isolation technique, Standard precautions
II. BODY MECHANICS - Turn and position
- Transfer – chair and stretcher - Use of lifts
- Assist with ambulation - Range of motion exercises
VI. SPECIAL PROCEDURES
- Vital signs - Temp (oral, rectal, axillary) - Pulse (radial, apical)
- Respirations - BP
- Height and weight (stand-up scales/bed scales)
- Application of heat/cold
- Prevent and care for decubitus ulcers + - Surgical skin preps and scrubs - Clean dressing changes
- Apply ace bandages, TEDs and binders + - Apply and remove EKG monitor leads - Postmortem care
- Cough/deep breathing III. NUTRITION
- Prepare patient s for meal time - Feed patient s
- Intake and output - Force and restrict fluids IV. ELIMINATION - Bedpan/urinal
- Bowel/bladder retraining - Collect/test specimens - Perineal/catheter care - Apply condom caths + - Douches
- Enemas
+ - Insert rectal tubes/flatus bags - Empty drainage devices from body cavities/wounds
+ - Maintain gastric suction
Role of Nurse Aide I on Health Care Team*
*The licensed nurse maintains accountability and responsibility for the delivery of safe and competent care. Decisions regarding delegation of any of the above activities are made by the licensed nurse on a patient-by-patient basis. ALL of the following criteria must be met before delegation of any task may occur:
task is performed frequently in the daily care of a patient or group of patient s;
task is performed according to an established sequence of steps;
task involves little to no modification from one patient situation to another;
task may be performed with a predictable outcome;
task does not involve on-going assessment, interpretation or decision-making that cannot be logically separated from the task itself; and
As part of accountability, the registered nurse must validate the competencies of the NA I prior to delegating tasks. The licensed nurse (RN or LPN) must monitor the patient’s status and response to care provided on an on-going basis.
* Core tasks which the North Carolina Board of Nursing has determined are appropriate for inclusion in basic NAI education programs.
+ Common tasks which are appropriate for delegation to NAI following appropriate education and competency validation by a registered nurse but are not required to be taught in the
Division of Health Service Regulation approved 75 hour course.
The “Decision Tree for Delegation to UAP” (www.ncbon.com – Position Statements) is an additional tool to assist the RN and LPN in making appropriate decisions related to delegation of tasks to UAP.
APPENDIX III: SUBCHAPTER 13J – THE LICENSING OF HOME CARE AGENCIES: IN-HOME AIDE SERVICES
(10A NCAC 13J .1107 IN-HOME AIDE SERVICES)
(a) If an agency provides in-home aide services, the services shall be provided in accordance with the client's plan of care. Agencies participating in the Home and Community Care Block Grant or Social Services Block Grant through the Division of Aging and Adult Services shall comply, for those clients, with the in-home aide service level rules contained in 10A NCAC 06A and 10A NCAC 06X which are hereby incorporated by reference with all subsequent amendments. All other agencies providing in-home aide services shall comply with the provisions in Paragraphs (b) and (c) of this Rule.
(b) If the client's plan of care requires the in-home aide to provide extensive assistance as defined in Rule .0901(9) of this Subchapter the in-home aide shall be listed on the Nurse Aide Registry pursuant to G.S. 131E-255. However, if the client's plan of care requires the in-home aide to provide only limited assistance as defined in Rule .0901(18) of this Subchapter the in-home aide is not required to be listed on the Nurse Aide Registry.
(c) In-home aides shall follow instructions for client care written by the health care practitioner required for the services provided. In-home aide duties may include the following:
(1) help with prescribed exercises which the client and in-home aides have been taught by a health care practitioner licensed pursuant to G.S. 90;
(2) provide or assist with personal care (i.e., bathing, care of mouth, skin and hair); (3) assist with ambulation;
(4) assist client with self-administration of medications which are ordered by a physician or other person authorized by state law to prescribe;
(5) perform incidental household services which are essential to the client's care at home; and
APPENDIX IV: APPLICATION OF DONABEDIAN THEORY OF QUALITY IMPROVEMENT TO THE CBA OF THE HOME CARE AIDE PROGRAM
Donabedian Definition Structure:
The environment in which services are provided, the attributes of material resources and human resources
Process:
The service provided or the patient’s role in seeking service
Outcomes:
The impact or effect on the patient’s health status based on the process (Donabedian, 1988)
Application to DNP Project Structure:
Financial and human resources to provide care in the home: HCA, training and education of HCAs, hours of care provision, direct and indirect cost of service provision
(administration, RN supervision, office
coordinators, office lease, supplies)
Process:
Technical care provided by HCA: Assistance with ADLs, medication reminders, fall prevention strategies, reporting early changes in condition, transportation to physician appointments, meal preparation and nutritional assistance
Trusting and consistent interpersonal relationships
Outcomes:
Rate of hospitalization, re-hospitalization and cost
Comparison to Medicare data for like population with 4-5 chronic conditions
APPENDIX V: COUNTY LEVEL MULTIPLE CHRONIC CONDITIONS (MCC): PREVALENCE, MEDICARE UTILIZATION AND SPENDING METHODS
County Level Multiple Chronic Conditions (MCC): Prevalence, Medicare Utilization and Spending Methods
Data Source and Study Population: The data used in the chronic condition reports are based upon
CMS administrative enrollment and claims data for Medicare beneficiaries enrolled in the fee-for-service program. These data are available from the CMS Chronic Condition Data Warehouse (CCW), www.ccwdata.org. For all the chronic condition reports the Medicare beneficiary population is limited to fee-for-service beneficiaries. We exclude Medicare beneficiaries with any Medicare Advantage enrollment during the year since claims data are not available for these beneficiaries. Also, we exclude beneficiaries who were enrolled at any time in the year in Part A only or Part B only, since their utilization and spending cannot be compared directly to beneficiaries enrolled in both Part A and Part B. Beneficiaries who die during the year are included up to their date of death if they meet the other inclusion criteria.
Data Years: 2007-2015
Geographic Variables: U.S. counties
Chronic Condition Measures: The 19 chronic conditions are identified through Medicare
administrative claims. A Medicare beneficiary is considered to have a chronic condition if the CMS administrative data have a claim indicating that the beneficiary received a service or treatment for the specific condition. Beneficiaries may have more than one of the chronic conditions listed. On October 1, 2015 the conversion from the 9th version of the International Classification of Diseases (ICD-9-CM) to version 10 (ICD-10-CM) occurred. Regardless of when a claim was submitted for payment, services that occurred prior to October 1, 2015, use ICD-9 codes. Chronic conditions identified in 2015 are based upon ICD-9 codes for the first ¾ of the year (January-September) and ICD-10 codes for the last quarter of the year (October-December). Detailed information on the identification of chronic conditions in the CCW is available at http://www.ccwdata.org/chronic-conditions/index.htm. To classify MCC for each Medicare beneficiary, these conditions are counted and grouped into four categories (0-1, 2-3, 4-5 and 6 or more).
Socio-demographic Variables: A beneficiary’s sex is available from the CMS enrollment database and is
classified as Male/Female. All the chronic condition reports use the variable RTI_RACE_CD, which is available on the Master Beneficiary Files in the CCW. The race/ethnicity classifications are:
Measures: Prevalence estimates are calculated by taking the beneficiaries with a particular number of
conditions divided by the total number of beneficiaries in our fee-for-service population, expressed as a percentage. Prevalence estimates across MCC categories sum to 100%. Emergency department visits are presented as the number of visits per 1,000 beneficiaries and are presented within MCC categories. ED visits include visits where the beneficiary was released from the outpatient setting and where the beneficiary was admitted to an inpatient setting. Hospital readmissions are expressed as a percentage of all admissions and are presented within MCC categories. A 30-day readmission is defined as an admission to an acute care hospital for any cause within 30 days of discharge from an acute care hospital. Except when the patient died during the stay, each inpatient stay is classified as an index admission, a readmission, or both. Medicare spending includes total Medicare payments for all
Medicare covered services in Parts A and B and is presented per beneficiary (i.e. per capita) within MCC categories. Both total actual payments and total standardized payments are presented.
Data Suppression: An "*" indicates that the data have been suppressed because there are fewer than
11 Medicare beneficiaries in the cell or for necessary complimentary cell suppression.
Methodology Report: A complete description of the methodology for all the chronic condition reports
REFERENCES
Agency for Healthcare Research and Quality. (2014). Overview of Hospital Stays in the United States, 2014. Retrieved from:
http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.pdf
The Alliance for Home Health Quality & Innovation. (2014). The Future of Home Health Care Project. Retrieved from http://www.ahhqi.org/images/pdf/future-whitepaper.pdf.
Anderson, P. (2015). Theoretical Approaches to Quality Improvement. In J. B. Butts & K. L. Rich (Eds.), Philosophies and theories for advanced nursing practice (358-359). Burlington, MA: Jones & Bartlett.
Barbarotta, L. (2010). Direct care worker retention: Strategies for success. Retrieved from http: //www.leadingage.org/uploadedFiles/Content/About/Center_for_Applied_Research/Publicat ions_and_Products/Direct%20Care%20Workers%20Report%20%20FINAL%20(2).pdf.
Berta, W., Laporte, A., Deber, R., Baumann, A., & Gamble, B. (2013). The evolving role of health care aides in the long-term care and home and community care sectors in Canada. Human Resources for Health, 11(1), 25-25 1p. doi:10.1186/1478-4491-11-25.
Brown, M., Redfern, R. E., Bressler, K., Swicegood, T. M., & Molnar, M. (2013). Effects of an advanced nursing job satisfaction, turnover rate, assistant education program on and clinical outcomes. Journal of Gerontological Nursing, 39(10), 34-43 10p. doi:10.3928/00989134-20130612-02.
Bryan, R. L., Kreuter, M. W., & Brownson, R. C. (2009). Integrating adult learning principles into training for public health practice. Health Promotion Practice, 10(4), 557-563 7p. doi:10.1177/1524839907308117.
Buck, D., K. (2014). Patient need prompts changes to nursing assistant training curriculums and authorized duties. Oregon State Board of Nursing Sentinel, 33(3), 18-19. Retrieved from https://auth.lib.unc.edu/ezproxy_auth.php?url=http://search.ebscohost.com/login.aspx?direct =true&db=rzh&AN=2012763372&site=ehost-live&scope=site.
Bureau of labor statistics. (2015). Retrieved from http://www.bls.gov.
Butts, J. (2015). Components and Levels of Abstraction in Nursing Knowledge. In J. B. Butts & K. L. Rich (Eds.), Philosophies and theories for advanced nursing practice (100-101). Burlington, MA: Jones & Bartlett.
CMS.GOV. (2014). Medicare Chronic Conditions Dashboard: County Level. Retrieved from:
CMS. (2012). Chronic Conditions among Medicare Beneficiaries. Retrieved from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Chronic-Conditions/Downloads/2012Chartbook.pdf.
Donabedian, A. (1982). The criteria and standards of quality. Ann Arbor, Michigan: Health Administration Press.
Donabedian, A. (1980). The definition of quality and approaches to its assessment. Ann Arbor, Michigan: Health Administration Press.
Donabedian, A. (2005). Evaluating the quality of medical care. The Milbank Quarterly,
83(4). Retrieved from http://www.zzjzfbih.ba/wp-content/uploads/2012/11/ donabedian.pdf.
Donabedian, A. (1988). The quality of care, how can it be assessed?. Jama, 260(12).
Retrieved from http://www.nursingworld.org/DocumentVault/Care-Coordination-Panel-Docs/background-docs/Jun-4-Mtg-docs/The-Quality-of-CareHowCanIt BeAssessed-Donabedian1988.pdf.
Dreze, J., & Stern, N. (1987). The Theory of Cost-Benefit Analysis. In A.J. Auerbach & M. Feldstein (Eds.), The Handbook of Public Economics (909-989). North Holland: Elsevier Publishers.
Goodman, J. (2010). The North Carolina nurse aide. Retrieved from http://www.ncleg.net/ documentsites/committees/NCSCA/2009-10%20Interim%20Commission%20Meetings/2-25-10/Nurse%20Aide-Goodman.pdf.
Grabowski, D. C. (2006). The cost-effectiveness of noninstitutional long-term care services: Review and synthesis of the most recent evidence. Medical Care Research & Review, 63(1), 3-28 26p. Retrieved from https://auth.lib.unc.edu/ezproxy_auth.php?url=http://search.ebsco host.com/login.aspx?direct=true&db=rzh&AN=105951303&site=ehost-live&scope=site.
IHI estimates that 15 million incidents of patient harm occur in U.S. hospitals each year. (2007). Healthcare Purchasing News, 31(1), 6-6. Retrieved from
https://auth-lib-unc-edu.libproxy.lib.unc.edu/ezproxy_auth.php?url=http://search.ebscohost.com.libproxy.lib.unc .edu/login.aspx?direct=true&db=rzh&AN=106201064&site=ehost-live&scope=site.
Jones, T. L., & Yoder, L. (2010). Economic theory and nursing administration research -- is this a good combination? Nursing Forum, 45(1), 40-53 14p.
doi:10.1111/j.1744-6198.2009.00160.x.
Luz, C., & Hanson, K. (2015). Training the personal and home care aide workforce: Challenges and solutions. Home Health Care Management & Practice, 27(3), 150-153 4p.
doi:10.1177/1084822314566301.
Mitchell, T. (2014, June 3, 2014). NC Budget Magnifying Glass: Senate budget cuts in-home and community-based services funding for older adults. The Progressive Pulse. Retrieved from http://pulse.ncpolicywatch.org/2014/06/03/nc-budget-magnifying-glass-senate-budget-cuts-in-home-and-community-based-services-funding-for-older-adults/print/.
Module O - critical thinking. (2013). NC state-approved curriculum - Nurse aide I training program (pp. 1-4) North Carolina Department of Health and Human Services Division of Health Service Regulation.
Neuhauser, M.B. (2004). Avedis Donabedian: father of quality assurance and poet. Qual Saf Health Care, (13). Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/ PMC1743903/pdf/v013p00472.pdf.
NC Department of Health and Human Services. (2017). Nurse Aide I Registry. Retrieved from: https://www.ncnar.org/ncna.html.
NC Division of Health Service Regulation: Acute and Home Care Licensure and Certification Section. (2017). The Licensing of Home Care Agencies. Retrieved from:
https://www2.ncdhhs.gov/dhsr/ahc/rules.html.
QSEN institute. (2015). Retrieved from qsen.org.
Retooling for an aging America, IOM releases recommendations for rebuilding the healthcare workforce. (2008). American Geriatrics Society Newsletter, 39(2), 1-13 3p. Retrieved from https://auth.lib.unc.edu/ezproxy_auth.php?url=http://search.ebscohost.com/login.aspx?direct =true&db=rzh&AN=105772200&site=ehost-live&scope=site.
Rhee, Y., Degenholtz, H. B., Lo Sasso, A. T., & Emanuel, L. L. (2009). Estimating the quantity and economic value of family caregiving for community-dwelling older persons in the last year of life. Journal of the American Geriatrics Society, 57(9), 1654-1659 6p.
doi:10.1111/j.1532-5415.2009.02390.x.
Right at Home. (2015). Right at Home Partners with Harvard Medical School on In Home Care Study. Retrieved from: http://www.rightathome.net/oak-park-chicago/blog/right-at-home-partners-with-harvard-medical-school-on-in-home-care-study/.
Russell, D., Rosati, R. J., Peng, T. R., Barrón, Y., & Andreopoulos, E. (2013). Continuity in the provider of home health aide services and the likelihood of patient improvement in activities of daily living. Home Health Care Management & Practice, 25(1), 6-12 7p.
doi:10.1177/1084822312453046.
Swett, E. (1996). Rehab resource: Home care aides improve costs, outcomes, and satisfaction. Caring, 52-55 4p. Retrieved from https://auth.lib.unc.edu/ezproxy_auth.php
?url=http://search.ebscohost.com/login.aspx?directReferences.
Treml, L. A., & Schulman, C. C. (1998). Home health care aides as extenders of therapy services: A managed care pilot program. Home Health Care Management & Practice, 10(5), 16-29. Retrieved from https://auth.lib.unc.edu/ezproxy_auth.php? url=http:// search.ebsco host.com/login.aspx?direct=true&db=rzh&AN=1998060862&site=ehost-live&scope=site.