Regenerating Life: Exploring the Potential for Stem Cell
Therapy in Traumatic Brain Injury.
Codie Wiley
Abstract
Introduction
Traumatic brain injury (TBI) accounted for 2.8 million emergency room visits in 2013 across the United States.1 Of those that experience TBI and survive, many are left with lifelong disabilities that result in major socioeconomic burden. In 2000, the economic impact of TBI in the United States was estimated to be $9.2 billion in lifetime medical costs and $51.2 billion in productivity losses.3
Survivors of TBI are often left disabled, with long-term side effects from the initial injury. The negative impact on patients is substantial and seen in every aspect of their lives. They often experience cognitive, psychiatric, physical, emotional, and behavioral changes.1 Moderate to severe TBI can be devastating to patients. 50% of survivors die during the first five years after injury and 57% of the remaining patients will be moderately to severely disabled indefinitely.1
Research exploring the potential utilization of stem cell for any number of medical conditions is both controversial and exciting. While there have been several recent trials involving the
treatment of TBI in rats with stem cells there are few studies involving human patients. As research grows and new evidence emerges there has been increasing interest in the possibility that human neurons can be regenerated or produced by stem cell therapies.
This paper sets out to address the clinical question: Can Mesenchymal stem cell implantation in patients who have suffered traumatic brain injuries regenerate or renew neuronal cells to improve cognitive and physical outcomes?
TBI is most commonly divided into stages in order to direct treatment; primary and secondary. Primary TBI is a result of external mechanical forces being transferred to intracranial contents.1 These external mechanical forces are most commonly the result of direct impact, rapid
acceleration or deceleration, a penetrating injury, or blast waves.1 What results from these initial
blows can be devastating. Hematomas, contusions, and shearing forces leading to diffuse axonal
injury all occur in this primary stage of brain injury. Loss of function, coma, and even death are
common in the first few hours of a severe brain injury.1 In motor vehicle collisions, focal cerebral contusions are the most commonly seen in the frontal and temporal areas from the
extreme acceleration/deceleration caused by the impact.1 It is during this stage that physical
damage is inflicted on neurons, glial cells, nerve fibers, and the blood brain barrier.2
Following the initial insult, disruption in the BBB can lead to passage of immune cells into the
central nervous system.2 The BBB stands between the brain extracellular fluid and the circulating peripheral blood keeping toxins at bay and regulating ion concentrations.2 Disruption in this system draws Astrocytes to the area creating a “glial scar” that creates a type of barricade
keeping macrophages from the site of injury. Macrophages are cells that are important in the
removal of damaged myelin.2 Without an influx of macrophages to the injured area the brain’s
ability to recover is hindered.2 This so called “glial scar” is an important factor in protecting viable neurons in the surrounding area from damage occurring from the disruption of the BBB.2 While preventing astrocytes from forming this scar would help macrophages enter the area to
clear debris and aid in recovery, it could possibly open the door to more neuronal cell damage.
The astrocytes also secrete essential metabolites to neurons that encourage neuronal survival.2
One possible way stem cell treatments could improve outcomes in TBI is to immediately repair
Secondary TBI is what occurs following the primary insult; it is best described as a cascade of
molecular injuries that leads to neuronal cell death.4 This path of destruction leads to neurotransmitter-mediated excitotoxicity causing glutamate, free-radical injury to cell membranes, electrolyte imbalances, mitochondrial dysfunction, inflammatory responses, apoptosis, secondary ischemia from vasospasm, focal microvascular occlusion, and vascular injury.1 The secondary insults that occur during this process are what medical experts are working to alleviate with treatments during the acute setting.
These pathological changes in the brain can lead to neurological deficits ranging from mild to severe. Symptoms of TBI are vast and associated with the amount and location of the neuronal damage. Patients often report nausea, vomiting, vertigo, photophobia, fatigue, and visual
disturbances.16 Headaches are the most commonly reported symptom associated with mild TBI.14 They can also suffer from psychological symptoms including irritability, anxiety, depression, and sleep disturbances.16 Cognitive impairments can include slowed or difficulty thinking, loss of memory, and disrupted thought patterns among others. 16 Speech and language can be affected as well.6 Expressive and receptive aphasia problems combined with problems reading and writing can lead to significant impairment in independence. Patients often lose hearing, smell, taste, and often report changes in vision.6 Paralysis and spasticity are two other devastating symptoms that
Epidemiology of TBI
The Centers for Disease Control reports that 538.2 out of 100,000 people experienced a TBI in
the United States in 2003.1 That number rose drastically in 2010 to an alarming 823.7 per
100,000.17 Injuries resulting in TBI or combined with TBI were responsible for 56,000 deaths and 30% of injury related mortality.14
The entire population is at risk of suffering from TBI during their lifetime. However, there are
subsets of the population that are at higher risk for occurrence. Those at highest risk overall
include the very young (0-4) and elderly (75+), many of which have suffered falls.14 The countries aging population has seen a 17.9% increase in falls resulting in TBI.17 These
individuals are at a much higher risk of TBI sequelae and face long recovery times. Their
likelihood of comorbidities, anti-coagulant use, and increased hospitalization are all likely
factors in the increased incidence of mortality among these patients.17
Falls are the leading cause of TBI-related emergency room visits in pediatric patients (0-4 years)
but the leading cause of TBI mortality in this population is due to assault/homicide (42.9%),
blunt trauma to the head, or violent shaking.17 Of those that survive, pediatric patients, for the most part, have the benefit of their youth to aid in their recovery. Sports related injury accounts
dependent on family members or facilities for full time care costing millions of dollars. 29% more males were involved in TBI-related medical care or died from their injuries in 2010 than females.1 Lower socioeconomic status, substance abuse, and underlying psychiatric disorder are all risk factors for TBI.1
In 2013 motor vehicle crashes (MVC) were the leading cause of TBI-related death in 5-24 years
of age, while intentional self-harm was number one for individuals 25-64 years of age.1
Fortunately, for individuals 45 years of age, TBI related mortality is declining, in large part due
to advances in motor vehicle safety, updated treatment guidelines, and increased access to
healthcare. However, with the number of TBI related deaths decreasing every year the number of
survivors with TBI related disabilities in this population are rising.17
There are other subsets of the population that are more likely to suffer from TBI. The United
States involvement in Middle Eastern conflict has given rise to a disproportionate increase in
TBI in military personal verses their civilian counterpart. Over the past decade an increasing
number of military related TBIs have been reported. An estimated 15.2% to 22.8% of service
members return home from war with mild TBI (mTBI); an estimated 320,000 military
underlying co-existing mental health conditions could be to blame for the disparity.13
It is estimated that 1-2% of the United States population has a long-term disability secondary to
the brain injury.1 That is 3.2 to 5.3 million Americans suffering every day with life altering
disabilities and the numbers continue to grow. There is also a substantial economic toll on
society; an estimated $76.5 billion dollars was spent on moderate to severe TBI-related medical costs in 2010 alone.16 These symptoms can be life-long, affecting not only their daily lives but also shortening overall life expectancy rates by 9 years.1 They are also at increased risk for seizures, accidental drug poisoning, and infections are 9 times more likely.1
Current Treatment
Primary Phase Management
Standard of care for traumatic brain injuries includes immediate attention to oxygen saturation
and blood pressure in the pre-hospital setting. Patients are closely monitored with provision of
early interventions such as supplemental oxygen or intravenous fluids in order to ensure
adequate oxygenation to the brain and perfusion to vital organs.4
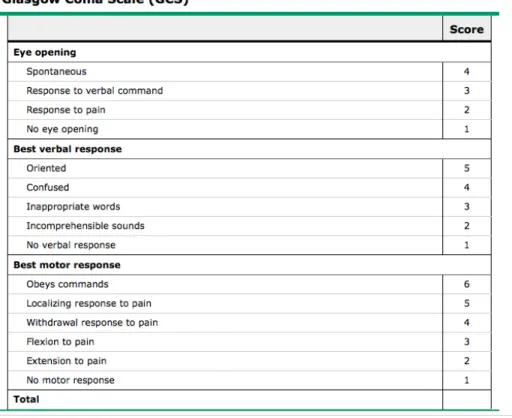
The Glasgow coma scale (GCS) is used to direct care and aid in making decisions regarding
treatment of TBI patients. table 1 The scale can be utilized to predict mortality rates and prognosis.
TBI is rated on this scale by mild disability given 13-15 points, Moderate disability (9-12),
Severe disability (3-8), and Vegetative state.16 Patients with Glasgow coma scales of <8 are
Table one –Uptodate
In the acute evaluation and management of TBI, patients are monitored for stability of vital
organs. They undergo evaluation by CT imaging, and are treated with neurosurgical procedures,
such as evacuation of hematoma, if indicated. Intracranial pressure is also monitored; if an
increase over 20 mmHg is detected, cerebral spinal fluid (CSF) drainage is initiated.4
Hyperventilation of patients in an induced coma is also used to decrease intracranial pressure in
the days following injury.1 Other treatment options include sedation, antiepileptic drugs, glucose
management, and various pharmacologic agents. Medical professionals are in disagreement over
many of the available treatment options for TBI however the current mainstay is the treatment of
hypoxemia and hypotension.5 Advances have been made but there is not a huge body of evidence
to strongly suggest that most of these treatment options have significant effect on outcomes.
The Secondary phase of TBI can prove the most challenging for survivors. The weeks, months,
and years following a brain injury can be devastating to an individual and their families. Patients
participate in many different medical therapies to improve cognitive and physical function.
Occupational and Physical therapists work with patients to improve function in every day tasks
and gain independence. Speech Language Pathologists work to rehabilitate speech patterns and
the ability to communicate. Psychotherapy is also important for both the patient and their
caregivers in order to educate and support their overall well-being.14 Medications are used in this phase to treat symptoms commonly associated with TBI. Depakote, NSAIDS, and Triptans are
prescribed for headaches, SSRI’s for depression, and anticonvulsants for seizures, as well as a
myriad of other pharmacologic treatments to reduce irritability, agitation, and cognitive loss
commonly experienced.14
Stem Cell Research and Applications
Stem cells are no longer a far-off, futuristic idea set aside for future generations to explore. In fact, they are already being studied in many areas of medicine today. In 1981 researchers were able to extract the first embryonic stem cells from mouse embryos. This research paved the way for researchers to extract and culture the first human embryonic stem cells in 1998.23 Stem cells were first discovered in the brain in the 1960’s but was not widely accepted until the 1990’s when published research showed proof of both the existence of stem cells within the brain and their ability to differentiate into astrocytes, oligodendrytes, and nerve cells.23
They are undifferentiated by definition but once stimulated are able to differentiate into a multitude of cells including neurons, cardiac, and muscle cells.16 As these cells divide they become either replicas of themselves, undifferentiated stem cells or they become a specialized cell that will become part of the body’s tissue.16 Research is being done determine how these
cells decide what to become and the exact moment they are stimulated to do so. With this knowledge stem cells could be directed to an area within the body and stimulated to regenerate or repair specific organs or cells. At the moment it remains unclear the mechanism that begins each individual cell’s journey to proliferation and what directs the path to an end product. Researchers have theorized that stem cells may produce soluble factors that regulate the trauma such as cytokines, mitochondria, and growth factors by protecting cells and reducing
inflammation.21 Stem cells may also regulate brain injury by replacing damaged cells to repoair tissue or stimulating other cells to repair the damaged area.21
Researchers are currently studying new ways to use stem cells in diseases such as Parkinson’s, Multiple Sclerosis, Autism, and diabetes. The clinical question at hand, however, explores the use of stem cells as a therapy for TBI.
cells (hUC-MSCs) are isolated from discarded extra-embryonic tissue after birth.11 Previously it was believed that the only source of coveted mesenchymal stem cells were unborn fetuses. However further research has shown these cells exist in abundance in both the umbilical cord and placenta.9 The cells are readily available and the process is painless to the mother and fetus.9
Of special interest to TBI, these cells have shown the ability to differentiate into neurons, astrocytes, and oligodendrocytes among others that consist of three germ layers.9 These same stem cells are being used in treatments for neuromylitis optica10 Bone Marrow mesenchymal stem cells (BMMSC) are being harvested from patients and injected back to study their ability to differentiate into other cells like neurons.8 In the past it was believe that adult stem cells could
only differentiate into the organ they originated in however new and exciting research is working to disprove this theory. Many studies are taking autologous BMMSCs and injecting them back into the site of injury in hopes that they will differentiate in to the cell type that has suffered damage.8 They have the potential to reverse the damage in TBI by differentiating into neurons and regenerating function.
Methods
To answer the clinical question PubMed, EMBASE, and Google Scholar were queried with the following search terms; “Neuronal stem cells”, “Stem Cells AND Central Nervous System”, “Stem Cell AND Traumatic Brain Injury”, “Stem Cell therapy AND injection”, “Traumatic
brain injury AND human neurons”, and “Stem Cell regeneration”. A search on
Brain Injury Pathophysiology”, “Stem Cells”, “Military TBI”, “Epidemiology in TBI” and
“Traumatic Brain Injury”.
Included in this paper were patient populations with mild to severe traumatic brain injury resulting from physical trauma, human subjects, studies within the last 10 years, English
language, and studies that used with Mescenchymal stem cells only. Animal and other laboratory vectors were excluded as well as studies involving patient groups with serious co-morbidities, cancer, or previous TBI.
The Cochrane review was used in the evaluation of each study in order to determine the validity
of results.
Results
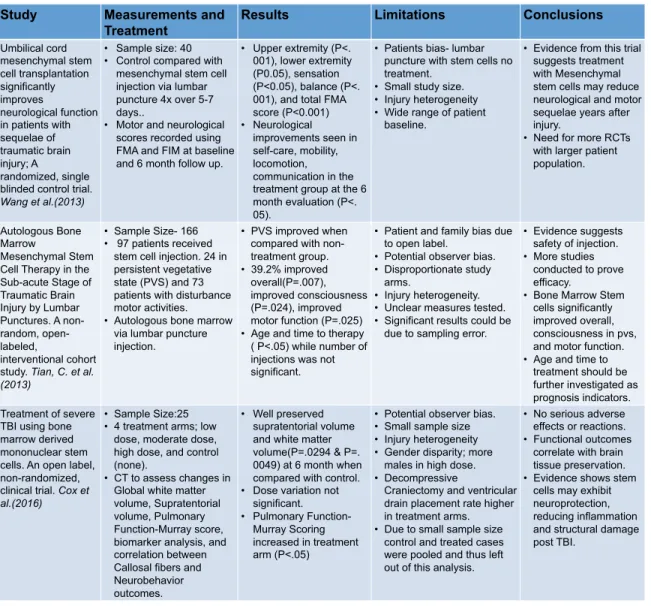
The search strategy yielded 600 studies, of those, 3 met inclusion criteria. Each will be overviewed here and are outlined in table 2.
Wang et al. studied the use of umbilical cord Mesenchymal stem cells in patients with sequelae of traumatic brain injury. Researchers conducted a randomized, single blinded controlled clinical
study. To be included in the study patients had to consent to treatment, could not undergo other
treatments or surgeries three months prior to or during the study, have diagnosis of TBI with
sequelae based on clinical manifestations as well as head CTs and MRIs, and have some degree
of central nervous system dysfunction. Patients were excluded if they presented with signs of
inherited metabolic diseases of the CNS, allergies, autoimmune diseases, history of tumors or
blood disease, positive serologic AIDS, hepatitis, or syphilis, or showed dysfunction of vital
organs. 40 patients were recruited for the study. Differences in age, gender, and severity of
injury were not statistically significant. 20 patients were given 4 treatments with umbilical stem cells injected via lumbar puncture while 20 patients were in the control group. All 40 patients were present at the conclusion of the study. Patients were given a function independence measurement test that tested an 18 item rating scale that assessed self-care, bowel and bladder management, mobility, communication, cognition, and psychosocial adjustment. Patients in both groups were evaluated both at baseline and 6 months after treatment. The patients who received
umbilical stem cells had statistically significant improvement in almost all areas tested. Upper
extremity (P<.001), lower extremity (P0.05), sensation (P<0.05), balance (P<.001), and total
FMA score (P<0.001) were all improved 6 months after treatment while the control group did
not show statistically significant improvement in any of the categories. Neurological
improvements were also seen in self-care, mobility, locomotion, and communication in the stem
cell group at the six month evaluation (P<.05). Improvements in sphincter tone and social cognition were slight but not significant. The control group did not experience any significant improvement in any of the functional groups tested. In all groups except sphincter control, communication, and social cognition there were statistically significant improvements seen in the stem cell patient group when compared with the control.
marrow mesenchymal stem cells were harvested and injected via lumbar puncture. Those in PVS showed improvement with consciousness (P=.024). Those with motor disturbances had
improvments in motor function (P.025) and both groups combined improved by 39.2% overall. Patient age and time from injury to therapy were statistically significant (P<.05) but the number of stem cell injections did not have a significant effect. Limitations are listed in table 2.
Cox et al. conducted an open label, non-randomized, single center clinical trial to further investigate the treatment of severe TBI using bone marrow derived mononuclear stem cells (BMMNC). Patients were screened in the emergency room and admitted to the trial if between the ages of 18 and 55 years, had a post-resuscitation GCS score of 5-8, less than 24 hours from initial injury, and English speaking. To ensure patients did not already suffer from irreversible brain injury patients were excluded if there were any known pre-existing serious medical co-morbidity or psychiatric disorder, seizure disorder, or any previous moderate to severe TBI. Patients were also excluded if they were thermodynamically unstable at time of consent, suffered open pelvic fracture, spinal cord injury, opening intracranial pressure >40 mmHg, had evidence of hypoxic-ischemic insult, uncorrected coagulopathy, greater than a grade III solid or hollow visceral injury of the abdomen or pelvis as rated by the American Association for the Surgery of Trauma, pregnancy, weight >300 lbs (MRI limitations), concurrent participation in an
interventional study, and unwillingness to return for follow up visits.
The study consisted of 25 patients between the ages of 18 and 55 years. BMMNCs were
(low), 9 x 106 BMMNC/kg (medium), 12 x 106 BMMNC/kg(high) while the control group did not receive any stem cells. Blood pressure, heart rate, oxygen saturation, and intracranial pressure were measured at timed intervals until the 12 hour mark in all treatment arms. These measures were also observed and recorded post stem cell harvest to evaluate safety of the procedure. MRI was performed at 1 and 6 months to follow changes in neuroinflammation in patient’s Corpus callosum and corticospinal tract. In patients that received stem cell treatment white matter was preserved when compared with control as well as Supratentorial volume. These patients also scored higher in neurocognitive function tests.
Table 2. Stem Cell Therapy Trial Summary
Study Measurements and
Treatment
Results Limitations Conclusions
Umbilical cord mesenchymal stem cell transplantation significantly improves neurological function in patients with sequelae of traumatic brain injury; A
randomized, single blinded control trial.
Wang et al.(2013)
• Sample size: 40 • Control compared with
mesenchymal stem cell injection via lumbar puncture 4x over 5-7 days..
• Motor and neurological scores recorded using FMA and FIM at baseline and 6 month follow up.
• Upper extremity (P<. 001), lower extremity (P0.05), sensation (P<0.05), balance (P<. 001), and total FMA score (P<0.001) • Neurological
improvements seen in self-care, mobility, locomotion, communication in the treatment group at the 6 month evaluation (P<. 05).
• Patients bias- lumbar puncture with stem cells no treatment.
• Small study size. • Injury heterogeneity • Wide range of patient
baseline.
• Evidence from this trial suggests treatment with Mesenchymal stem cells may reduce neurological and motor sequelae years after injury.
• Need for more RCTs with larger patient population.
Autologous Bone Marrow
Mesenchymal Stem Cell Therapy in the Sub-acute Stage of Traumatic Brain Injury by Lumbar Punctures. A non-random, open-labeled,
interventional cohort study. Tian, C. et al. (2013)
• Sample Size- 166 • 97 patients received
stem cell injection. 24 in persistent vegetative state (PVS) and 73 patients with disturbance motor activities. • Autologous bone marrow
via lumbar puncture injection.
• PVS improved when compared with non-treatment group. • 39.2% improved overall(P=.007), improved consciousness (P=.024), improved motor function (P=.025) • Age and time to therapy ( P<.05) while number of injections was not significant.
• Patient and family bias due to open label.
• Potential observer bias. • Disproportionate study
arms.
• Injury heterogeneity. • Unclear measures tested. • Significant results could be
due to sampling error.
• Evidence suggests safety of injection. • More studies
conducted to prove efficacy. • Bone Marrow Stem
cells significantly improved overall, consciousness in pvs, and motor function. • Age and time to
treatment should be further investigated as prognosis indicators. Treatment of severe
TBI using bone marrow derived mononuclear stem cells. An open label, non-randomized, clinical trial. Cox et al.(2016)
• Sample Size:25 • 4 treatment arms; low
dose, moderate dose, high dose, and control (none).
• CT to assess changes in Global white matter volume, Supratentorial volume, Pulmonary Function-Murray score, biomarker analysis, and correlation between Callosal fibers and Neurobehavior outcomes.
• Well preserved supratentorial volume and white matter volume(P=.0294 & P=. 0049) at 6 month when compared with control. • Dose variation not
significant. • Pulmonary
Function-Murray Scoring increased in treatment arm (P<.05)
• Potential observer bias. • Small sample size • Injury heterogeneity • Gender disparity; more
males in high dose. • Decompressive
Craniectomy and ventricular drain placement rate higher in treatment arms. • Due to small sample size
control and treated cases were pooled and thus left out of this analysis.
• No serious adverse effects or reactions. • Functional outcomes
correlate with brain tissue preservation. • Evidence shows stem
Discussion
In the past it was thought that neurons were unable to regenerate or renew after injury. However evidence has shown the presence of stem cells with in the brain that are able to differentiate in to oligodendrocytes, astrocytes, and nerve cells. With this in mind, current treatments aim to reduce factors that lead to secondary TBI like hypoxia, hypotension, increased intracranial pressure, and hypoglycemia. However new research points to the possibility that stem cells can infiltrate the brain and encourage regeneration in patients’ existing neurons and stimulate new neurons to differentiate. This could lead to vast improvements in function, memory, physical abilities, and quality of life.
In the clinical trial conducted by Wang et al. significant improvements with stem cell injections in neurocognitive function tests as well as motor scores were seen in almost every treatment group when compared with control. Cox et al. showed evidence of correlation between stem cell therapy and preservation of white matter within the brain and supratentorial volume. With less brain volume loss patients were able to preform at higher levels on neurocognitive function tests. The mechanism behind this is unknown and should be further investigated. Whether this
Stem cell therapy could affect outcomes both in the acute setting and in the recovery process. It is thought that damage to neurons is a result of inflammation that leads to hypoxic conditions and cell death throughout the neuronal environment. If researchers can find a way to intervene in this process they could greatly reduce poor prognosis. The ability to regenerate neurons and stimulate self-renewal could slow and even eliminate the cascade of events primary brain injury sets in to motion.
Many of the current interventions are aimed at treatment during the primary phase of injury however with the secondary phase lasting up to several months there is a great opportunity to affect long term outcomes during this time. Further research in reducing symptoms of TBI in the months and years after the initial insult should be conducted as there is limited evidence in this area. Wang et el. sought to do this by treating patients at least 1 year after initial injury. Results were promising with TBI-related sequelae significantly reduced in the treatment arm however due to multiple limitations of the study should be further investigated with a randomized, double blinded control trial.
The current studies in stem cell implantation have followed many successful animal trials demonstrating promising outcomes for humans. The limitations placed on how stem cells can be collected and used stands as a major barrier to the advancement of stem cell research. New collection methods that pose little ethical issue could increase the number of clinical trials and become more widely accepted.
conducted in order to increase efficacy of stem cell transplant to regenerate neuronal cells. Another drawback to stem cell therapy with MSC’s may be their suppression of patient’s
antitumor response as Djouad et al. reported.2 Very few adverse effects have been seen in clinical trials to date but there is a possibility that with more research a link between increased tumors and stem cell therapy may be found.
TBI’s can be reduced and lives can be saved with more attention to education surrounding fall risks, safety equipment, motor vehicle safety, etc. However, not all TBI’s can be prevented. Neuronal regeneration and renewal through stem cell treatment could allow scientists to prevent primary TBIs from causing secondary injuries that result in life long disabilities and eliminate debilitating sequelae. This could reduce the overall impact of their medical care costs to the healthcare system by billions of dollars each year and improve the lives of millions of TBI survivors around the world.
1.Centers for disease control and Prevention; National center for injury prevention and control. Traumatic Brain Injury and Discussion. (2017). Retrieved November 12, 2017. https://www.cdc.gov/traumaticbraininjury/get_the_facts.html
2.Mesenchymal stem cells in the treatment of traumatic brain injury. (2017). Front Neurology. 8;28. Retrieved from Ncbi.nlm.nih.gov
3.Hemphill, J. Claude, III,MD,MAS. (2016). Traumatic brain injury: Epidemiology, classification, and pathophysiology. UptoDate. Retrieved from
https://www.uptodate.com/contents/traumatic-brain-injury-epidemiology-classification-and-pathophysiology
4.Hemphill, C., Phan, N., (2017). Management of acute severe traumatic brain injury; Uptodate.
5.Buki A, Koizumi H, Povlishock JT. (1999) Moderate posttraumatic hypothermia decreases early calpain-mediated proteolysis and concomitant cytoskeletal compromise in traumatic axonal injury. Experimental Neurology.159;1 319-328.
6.Heather H. Ross, Fabrisia Ambrosio, Randy D. Trumbower, Paul J. Reier, Andrea L. Behrman, Steven L. Wolf; Neural Stem Cell Therapy and Rehabilitation in the Central Nervous System: Emerging Partnerships, Physical Therapy, Volume 96, Issue 5, 1 May 2016, Pages 734–742, https://doi.org/10.2522/ptj.20150063
7.Ilie G, Boak A, Adlaf EM, Asbridge M, Cusimano MD, (2016). Prevalence and correlates of traumatic brain injuries among adolescents. JAMA. 2013;309(24):2550.
8.Ji-Yao Jiang, Guo-Yi Gao, Wei-Ping Li, Ming-Kun Yu, and Cheng Zhu. Journal of Neurotrauma.(2004) Early Indicators of Prognosis in 846 Cases of Severe Traumatic Brain Injury.19(7): 869-874.
http://doiorg.libproxy.lib.unc.edu/10.1089/08977150260190456
9.Fan, C.-G., Zhang, Q., Zhou, J. (2011). Therapeutic Potentials of Mesenchymal Stem Cells Derived from Human Umbilical Cord. Stem Cell Reviews and Reports. 7(1), 195-207. 10.Lu, Z., Ye, D., Qian, L. Zhu, L., Wang, C. Guan, D., Zhang, X., Xu, Y. (2012) Human
umbilical cord mesenchymal stem cell therapy on neuromyelitis optica. Department of Neurology, Affiliated Drum Tower Hospital. 9(4);250-255.
11.Mckee, A.C., Robinson, M.E., (2014). Military- related traumatic brain injury and neurodegeneration. Alzheimer’s & Dementia. The Journal of the Alzheimer’s Association. 10;3. S242-S253. http://doi.org?10.1016?j.jalz.2014.04.003
12.Chapman, J., Diaz-Arrastia, R.(2014). Military traumatic brain injury: A Review. Alzheimer’s & Dementia. The journal of the Alzheimer’s Association, 10(3), S97-S104.http://doi.org/10.1016/j.jalz.2014.04.012
13.Georges, A., Dulebohn, S., (2017). Traumatic Brain Injury. NCBI Bookshelf. Retrieved from ncbi.nlm.nih.gov.
14.Wang, S., Cheng, H.,Dai, G.,Wang, X., Hua, R., Liu, X., Wang, P.,Chen, G.,Yue and An, Y.(2013) Umbilical cord mesenchymal stem cell transplantation significantly improves neurological function in patients with sequelae of traumatic brain injury. Brain Research.
1532, 76-84.
15.Rutland-Brown, W., Langlois, JA., Thomas, KE.(2006) Incidence of traumatic brain injury in the United States, 2003. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Injury Response. 21(6):544. 16.Taylor CA, Bell JM, Breiding MJ, Xu L. (2017). Traumatic Brain Injury-related
MMWR;66(No. SS-9):1–16. DOI:http://dx.doi.org/10.15585/mmwr.ss6609a1
17.Tian, C., Wang X, Wang X, Wang L, Wang X, Wu S, Wan Z. (2013) Autologous bone marrow mesenchymal stem cell therapy in the subacute stage of traumatic brain injury by lumbar puncture. Institute of Neurology, the First College of Clinical Medical Science. 11(2):176-181. Doi; 10.6002/ect.2012.0053
18.Cox, C., Hetz, R., Liao, G., Aertker, B., Ewing-Cobs, L., Juranek, J.,Savitz, S., Jackson, M., Romanowska-Pawliczek, A., Triolo, F, Dash, P., Pedroza, C., Lee, D., Worth, L., Aisiku, I., Choi, H., Holcomb, J., Kitawaga, R.(2016) Treatment of Severe Adult Traumatic Brain Injury Using Bone Marrow Mononuclear Cells. Stem Cells Journal.
35;4(1065-1079)
19.Hsuan, Y. C.-Y., Lin, C.-H., Chang, C.-P. and Lin, M.-T. (2016), Mesenchymal stem cell-based treatments for stroke, neural trauma, and heat stroke. Brain and Behavior, 6: 1–11. e00526, doi: 10.1002/brb3.526
20.Shen, W., Plachez, C., Tsymbalyuk, O., Tsymbalyuk, N., Xu, S., Smith, A., Michel., Yarnell, D., Mullins, R., Gullapalli, R., Puche, A., Simard, JM., Fishman, P., Yarowsky, P. Cell-Based Therapy in TBI: Magnetic Retention of Neural Stem Cells In Vivo.
21.Pati, S., Rasmussen, T. (2017)Cellular therapies in trauma and critical care medicine: Looking towards the future. PLOS medicine.
https://doi.org/10.1371/journal.pmed.1002343
22.Cox CS Jr, Baumgartner, JE., Harting MT. 2011. Autologous bone marrow mononuclear cell therapy for severe traumatic brain injury in children. Neurosurgery. 2011;68(3):588-600.
23.U.S. Department of Health and Human Services; National Institutes of Health. (2016).
Stem Cell Basics. Retrieved from https://stemcells.nih.gov/info/basics/4.htm
24.Cox, C., Hetz, R., Liao, G., Aertker, B., Ewing-Cobs, L., Juranek, J.,Savitz, S., Jackson, M., Romanowska-Pawliczek, A., Triolo, F, Dash, P., Pedroza, C., Lee, D., Worth, L., Aisiku, I., Choi, H., Holcomb, J., Kitawaga, R.(2016) Treatment of Severe Adult Traumatic Brain Injury Using Bone Marrow Mononuclear Cells. Stem Cells Journal.
35;4(1065-1079)
25.American Association of Neurological Surgeons. 2017. Sports Related Head Injury. http://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Sports-related-Head-Injury
26. Reis, C., Wang, Y., Akyol, O., Ho, W. M., Applegate II, R., Stier, G., Zhang, J. H. (2015). What’s New in Traumatic Brain Injury: Update on Tracking, Monitoring and Treatment. International Journal of Molecular Sciences. 16(6), 11903–11965. http://doi.org/10.3390/ijms160611903
27.Kobeissy FH. NCBI Bookshelf. (2015) Implications for Repair and Regeneration of Injured Brain in Experimental TBI Models. Stem Cell Therapy in Brain Trauma. CH 42. 28.Zehtabchi S, Soghoian S, Liu Y, et al. The association of coagulopathy and traumatic
brain injury in patients with isolated head injury. Resuscitation. 2008; 76:52.