The Search for Cryptogenic Stroke, A Case of
Marantic Endocarditis
Henry Chen
1, Timothy Fritz
1,2, Preeti Banga
1, David Wohns
1,2, Stephen Cohle
2, Sandeep Banga
2,3,*1Michigan State University College of Human Medicine 2Meijer Heart Center, Spectrum Health
3Department of Research, GRMEP
*Corresponding Author: [email protected]
Copyright © 2014 Horizon Research Publishing All rights reserved.
Abstract
Nonbacterial thrombotic endocarditis (NBTE) is rare and undoubtedly an under-recognized cause of cryptogenic stroke. Its diagnosis relies on a high index of clinical suspicion, particularly in patients with previous malignancy.We present a case of a young woman, with three neurologic events occurring in rapid succession over three weeks, ultimately resulting in her death. The echo imaging findings here appear relatively benign compared to the catastrophic consequences, and speaks of the aggressive fibrin and platelet deposition that can embolize widely in this condition, confirmed on the postmortem examination. We discuss the details of NBTE aiming to increase awareness while assessing patients with undetermined systemic embolization.Keywords
Cryptogenic Stroke, Marantic Endocarditis, Nonbacterial Thrombotic Endocarditis, Left Middle Cerebral Artery, Transesophageal Echocardiography1. Introduction
The search for an underlying cause of stroke remains a common clinical problem. If carotid disease is excluded, cryptogenic causes become the mainstay of further evaluation. This requires morphologic evaluation of the stroke substrate and questions culprit valvular lesions including infective endocarditis, intracardiac mass with attention to left atrial myxoma or left atrial thrombus, left ventricular thrombus, aortic atheroma or dissection, or shunting via an atrial or intrapulmonary defect. If no source is identified, frequently protracted monitoring for occult atrial fibrillation is recommended. NBTE is often not considered.It is rare and undoubtedly underdiagnosed.Since it was first described by Zeigler in 1888 [1] its variable presentations and causes have been discussed [2].Clinical factors considered in initiating the lesion development include immune complex disease, hypoxia, hypercoagulability, and precedent carcinomatosis.
2. Case
Report
A 52 year old woman with no previous cardiac history presented with expressive aphasia. The acute presentation was preceded by two days of not feeling well, with predominant occipital headache for which she took Aspirin 650mg every 6 hours. There were no constitutional symptoms, and no fever. The headache progressed and now was associated with nausea and vomiting. She presented to the emergency department when she was unable to find her words.
Past cardiac history was normal with no valvular disease and no arrhythmia. The patient had no family history of NBTE. Three years prior she was found to have breast cancer, and underwent mastectomy with adjuvant chemotherapy and radiation. Serial echocardiograms showed no treatment toxicity, with preservation of cardiac function. Initial examination demonstrated a nontoxic appearance.There was no fever. Cardiac examination was normal. Neurologic examination was largely normal except for a focal finding of “word salad”. There was no receptive component and no peripheral deficits.
appendage which demonstrated normal echogenicity (Figure 2a,2b,2c).Overall the valves were reported as normal. The aortic valve was mildly thickened but showed no stenosis or regurgitation by Doppler.
There is restricted diffusion involving the left middle
cerebral artery region consistent with acute ischemic infarction. There are additionally multiple isolated foci of restricted diffusion in a multi-arterial distribution in both cerebral hemispheres concerning for embolic-type phenomenon.
1a. 1b
Figure1. 1a, 1b. Axial T2 MRI without Contrast Diffuse Tensor Imaging of the Head [Last admission]
2a. Aortic valve without vegetations 2b.Left atrium, left ventricle, and left atrial appendage without thrombus
[image:2.595.201.411.561.734.2]2c. Intact interatrial septum
The patient recovered neurologically within 6 hours, was observed for three days with no arrhythmia, and ultimately discharged with a 30 day event monitor. Treatment consisted of Aspirin325 mg daily.
The day following discharge she again presented with acute receptive and expressive aphasia. The monitor showed no arrhythmia. Brain MRI showed no hemorrhage, but indicated a larger LMCA infarct. She was treated with recombinant tPA stroke protocol, and rapidly improved to normal neurologic function with no residual deficiet. An extensive repeat laboratory evaluation remained normal. She was observed, and ultimately discharged on oral anticoagulant-“Rivaroxaban”.
Seven days later, she again presented to our facility with a dense stroke manifesting as aphasia and dense right sided hemiparesis. Brain CT and MRI found more multiple focal infarcts and a dense LMCA infarct. Urgent TEE trying to identify a cause showed a small mobile echo density attached to the left ventricle side of the non-coronary cusp of the aortic valve measuring 0.3cm by 0.3cm (Figure 3a, 3b).There was also mild aortic regurgitation. She soon demonstrated recurrent seizures and rapid unresponsiveness with profound neurological decline, brain herniation and death.
3a. Vegetations on aortic valve
[image:3.595.328.535.107.310.2]3b. Off axis view of aortic valve. Vegetations on aortic surface of the aortic valve
Figure 3. Positive findings on last admission TEE
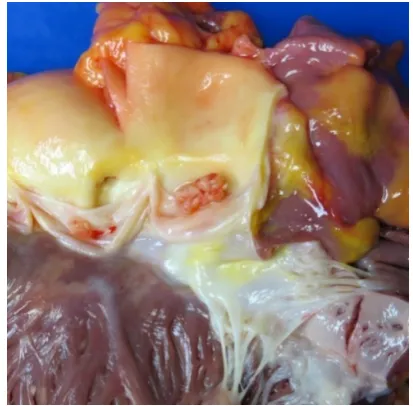
A postmortem examination was performed including histopathology (Figure 4a,4b, 4c).
4a. Gross picture of aortic valve with thrombus vegetations on the right coronary valve and the non-coronary valve
4b. Magnified gross view of thrombus vegetation on non-coronary valve.
4c. Photomicrograph of aortic valve (left) and thrombus (right). Thrombus composed of fibrin and platelets.
[image:3.595.323.542.346.523.2]3. Discussion
NBTE was first described by Zeigler in 1888 [1].In 1936, Gross and Friedberg coined the phrase “non-bacterial thrombotic endocarditis,” which is also described as marantic endocarditis [2].NBTE most commonly affects individuals from the fourth through the eighth decade of life [4].Approximately 1.2% of all autopsy patients have been found to have vegetations secondary to NBTE. It has been reported that the incidence of NBTE ranges from 0.3% to 9.3% [1].The sex distribution of NBTE is equal between males and females [4].The incidence of embolism varies from 14.1% to 90.9% [5].NBTE has been documented in many conditions including malignancy, tuberculosis, uremia, AIDS, connective tissue disorders, autoimmune, hypercoagulability states, SLE, and trauma [2].
The etiology and pathogenesis of NBTE is not fully understood. It is believed that endothelial damage results in the exposure of the subendothelium to circulating platelets. Vegetations of platelets and fibrin develop on cardiac valves, most commonly the mitral valve [2].Several initiating mechanisms have been proposed including, 1. immune complexes, 2. hypoxia, 3. hypercoagulability, and 4. carcinomatosis. In 1980, Williams described circulating immune complexes involved in the development of NBTE [6].It has since been shown through immunohistochemistry that immunoglobulin and complement deposits have been found at the base of NBTE vegetations [7].In regards to hypoxia induced tissue factor (TF) expression, it has been described that higher activity levels of tissue factor (TF) have been correlated with increased incidence of NBTE [8].Dutta et al. described a greater incidence of NBTE amongst smokers compared against non-smokers [9].Hypercoagulability and valvular degeneration were initially described as important precursors to the development of NBTE by MacDonald and Robbins [4].Finally cacinomatosis and NBTE has been extensively studied. Mucin adenocarcinoma of the gut and lung and disseminated intravascular coagulability (DIC) are commonly described in association with NBTE [10,11].The most common tumors associated with NBTE are from the gut and lung (48%) and then followed by hematologic malignancies [10].
The diagnosis of NBTE relies on high clinical suspicion than from family history. Currently there is not much literature discussing the relation of family history and NBTE. A family history of NBTE is suspected if there is occurrence of NBTE in the family together with disease known to initiate NBTE,which usually includes cancers and hypercoagulable diseases. There are no pathognomonic signs and symptoms [2].A clinical triad was described by Mckay and Wahler - 1. Known disease process associated with NBTE 2. Heart murmur 3. Signs of multiple systemic emboli [12].There are no bloodstream markers for diagnosis, but abnormal hematologic and coagulation parameters should raise suspicion for NBTE. In addition, blood cultures should be taken to rule out infectious endocarditis. Cardiac murmurs
are a poor sign for NBTE because they are frequently not present [1].However, inclusion of NBTE within a differential is essential when a murmur is discovered in the setting of malignancy, DIC, or known antiphospholipid syndrome. The hallmark feature of NBTE is recurrent emboli, which occurs in up to 50% of patients [1]. Vegetations within NBTE have little inflammatory reaction at the site of attachment. As a result, they can detach more frequently than infective endocarditis and result in multi-organ embolism. NBTE tends to embolize to the brain, kidney, spleen, mesenteric bed, or the extremities. Emboli to the brain typically occur in the middle cerebral artery (MCA) and subsequently presents with MCA stroke symptoms such as aphasia, agnosia, hemiparesis, and contralateral sensory loss [16].An uncommon clinical presentation can be valvular insufficiency from destruction of the valve leaflets or stenosis from the size of vegetations [13]. NBTE vegetations are usually small, <1cm in diameter, broad based and irregular in shape [14].Transoesophageal echo (TEE) is more sensitive (90%) for the diagnosis of vegetations than transthoracic echo (TTE), especially for the vegetation of <5mm.As a result of the small and irregular nature of NBTE vegetations, a TEE should be ordered over a TTE [2]. Edoute et al., a prospective TTE study of 200 cancer patients on the detection of cardiac valvular lesions with TTE found that 19% of the experimental group had valvular lesions compared with only 2% in the control group [15].Left sided heart valves were more commonly affected and the mitral valve was more commonly involved than the aortic.
When the TEE identifies apparently normal cardiac valves, a MRI may be useful in providing additional evidence supporting the diagnosis of NBTE .Diffusion-weighted MRI (DWI) may differentiate cardioembolic stroke from infectious endocarditis (IE) versus from NBTE.As seen within a study of 35 patients, stroke patterns were differentiated between NBTE and IE [16].NBTE exhibited pattern 4 (multiple small and medium or large disseminated lesions).IE exhibited pattern 1 (single lesion), pattern 2 (territorial infarction), pattern 3 (multiple punctuate disseminated), and pattern 4.The differences in stroke presentation may be secondary to NBTE lesions being more friable and the lack of inflammation at the site of vegetation attachment to cardiac valves with NBTE.
Histologically, NBTE vegetations are white or tan masses and are usually along the lines where the valve leaflets close. The vegetations typically present as degenerating platelets with interwoven strands of fibrin, which form a featureless, bland, and esoinophilic mass [2].
months [17].There are no guidelines for surgical intervention and therefore must also be tailored for each patient. Typically, surgical interventions occur in patients with acute congestive cardiac failure or recurrent thromboembolisms despite therapeutic anticoagulation [10].
NBTE remains an uncommon condition that is frequently underestimated because of the difficulty in diagnosis and the reliance on strong clinical suspicion.
A case was presented on an individual who presented with multi-organ embolic symptoms and demonstrated the difficulty in diagnosis with initially an apparently normal TEE and the lack of a cardiac murmur.The patient described had signs demonstrating commonly found features of NBTE including, MCA stroke symptoms, MRI demonstrating pattern 4 stroke presentation, and signs of recurrent embolism.
4. Conclusions
This case highlights the importance of including NBTE within a differential in individuals presenting with signs of systemic embolism and a history of having a disease associated with NBTE.
REFERENCES
[1] Lopez JA, Ross RS, Fishbein MC. Nonbacterial thrombotic endocarditis- A review, Am Heart J., Vol. 113,773—784,1987.
[2] Asopa S, Patel A, Khan OA, Sharma R, Ohri SK. Non-bacterial thrombotic endocarditis.Eur J CardiothoracSurg, Vol. 32,No.5, 696-701, Nov2007.
[3] Gross L, Friedberg CK. Nonbacterial thrombotic endocarditis. Classification and general description, Arch Intern Med., Vol. 58, 620—640, 1936.
[4] MacDonald RA, Robbins SL. The significance of nonbacterial thrombotic endocarditis, an autopsy and clinical study of 78 cases, Am Intern Med.,Vol. 46, 255—273,1957. [5] Angrist A, Marquiss J. The changing morphologic picture of
endocarditis since the advent of chemotherapy and antibiotic agents, Am J Pathol.,Vol. 30,39-63,1954.
[6] Williams Jr RC. Immune complexes in clinical and experimental medicine. 1st ed., Cambridge, Harvard
University press,p. 12,1980.
[7] Hojnik M, George J, Ziporen L, Schoenfeld Y. Heart valve involvement (Libman—Sacks endocarditis) in the antiphospholipid syndrome. Circulation,Vol.93,1579-1587,1 996.
[8] Nakanishi K, Tajima F, Nakata Y, Osada H, Ogata K, Kawai T, Torikata C, Suga T, Takishima K, Aurues T, Ikeda T. Tissue factor is associated with the nonbacterial thrombotic endocarditis induced by a hypobaric hypoxic environment in rats. Virchows Arch.,Vol.433,375-379,1998.
[9] Dutta T, Karas MG, Segal AZ, Kizer JR. Yield of transesophageal echocardiography for nonbacterial thrombotic endocarditis and other cardiac sources of embolism in cancer patients with cerebral ischemia. Am J Cardiol.,Vol.97(6),894-898,2006.
[10] Eiken PW, Edwards WD, Tazelaar HD, McBane RD, Zehr KJ. Surgical pathology of nonbacterial thrombotic endocarditis in 30 patients, 1985—2000. Mayo Clin Proc.,Vol.76,No.12,1204—1212,2001.
[11] Bedikian A, Valdiviesco M, Luna M, Bodey GP. Nonbacterial thrombotic endocarditis in cancer patients with or without concomitant disseminated intravascular coagulation. Med Pediatr Oncol.,Vol.4,149—157,1978. [12] Mckay DG, Wahler Jr GH. Disseminated thrombosis in colon
cancer. Cancer.Vol.8,970-978,1955.
[13] Kurdi M, Beanlands DS, Chan KL, Veinot JP. Nonbacterial thrombotic endocarditis presenting as aortic stenosis with suspected infective endocarditis,clinicopathological correlation. Can J Cardiol.,Vol.20,No.5, 549-552,2004.
[14] Otto CM. Nonbacterial thrombotic endocarditis. Valvular heart disease. W.B. Saunders,Philadelphia,pp. 445-450,1999. [15] Edoute Y, Haim N, Rinkevich D, Brenner B, Reisner SA.
Cardiac valvularvegetations in cancer patients, a prospective echocardiographic study of 200 patients, Am J Med, Vol. 102, 252—258, 1997.
[16] Singhal AB, Topcuoglu MA, Buonanno FS. Acute ischemic stroke patterns in infective and nonbacterial thrombotic endocarditis. A diffusion weighted magnetic resonance imaging study, Stroke, Vol. 33, 1267—1273, 2002.